Embed Size (px)
Citation preview
© Royal College of Obstetricians and Gynaecologists
LAPAROSCOPIC ENTRY
GREEN-TOP GUIDELINE, 2008
SOGC CLINICAL PRACTICE GUIDELINE, 2013
Aboubakr Elnashar
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
CONTENTS
1. POSITION OF PATIENT
2. PRIMARY PORT CLOSED ENTRY
3. SECONDARY PORT ENTRY
4. PRIMARY PORT ALTERNATIVES
5. EXIT TECHNIQUES
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
1. POSITION
Prone
Stirrups/Lloyd Davis
Non slip mattress
Trendelenberg after ports
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
The operating table should be horizontal
(not in the Trendelenberg tilt) at the start of
the procedure
The abdomen should be palpated to check
for any masses before insertion of the
Veress needle
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
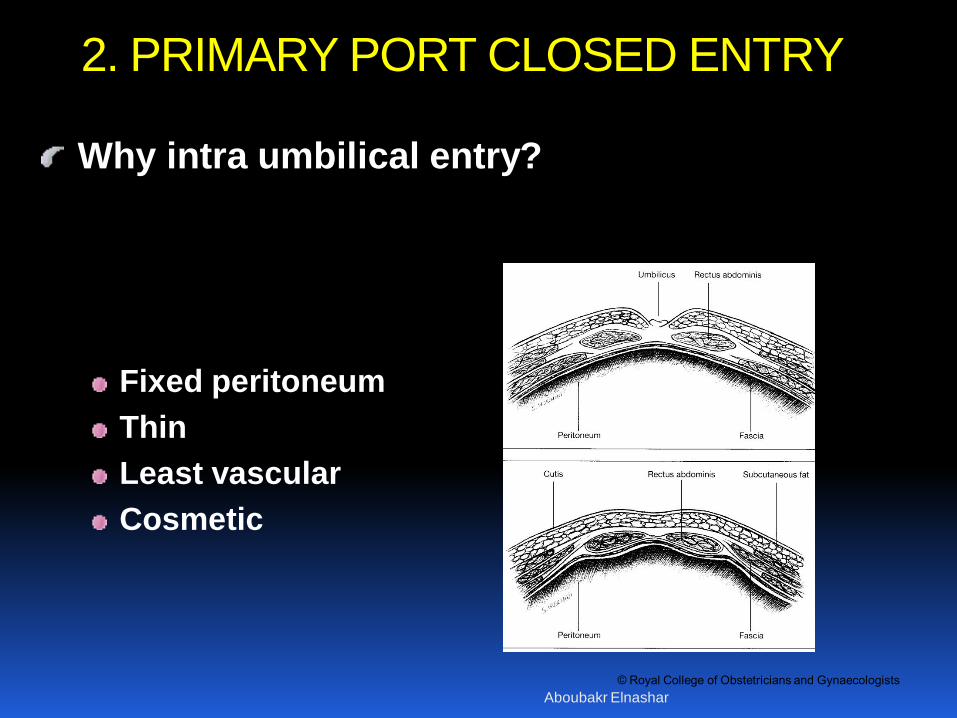
Why intra umbilical entry?
Fixed peritoneum
Thin
Least vascular
Cosmetic
2. PRIMARY PORT CLOSED ENTRY
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
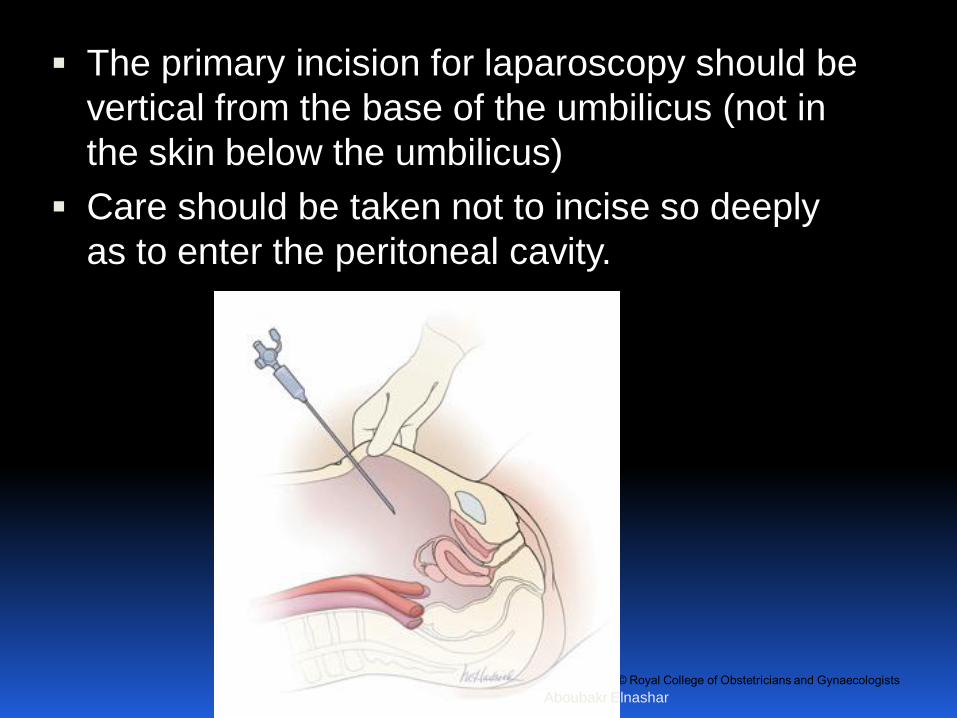
The primary incision for laparoscopy should be
vertical from the base of the umbilicus (not in
the skin below the umbilicus)
Care should be taken not to incise so deeply
as to enter the peritoneal cavity.
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
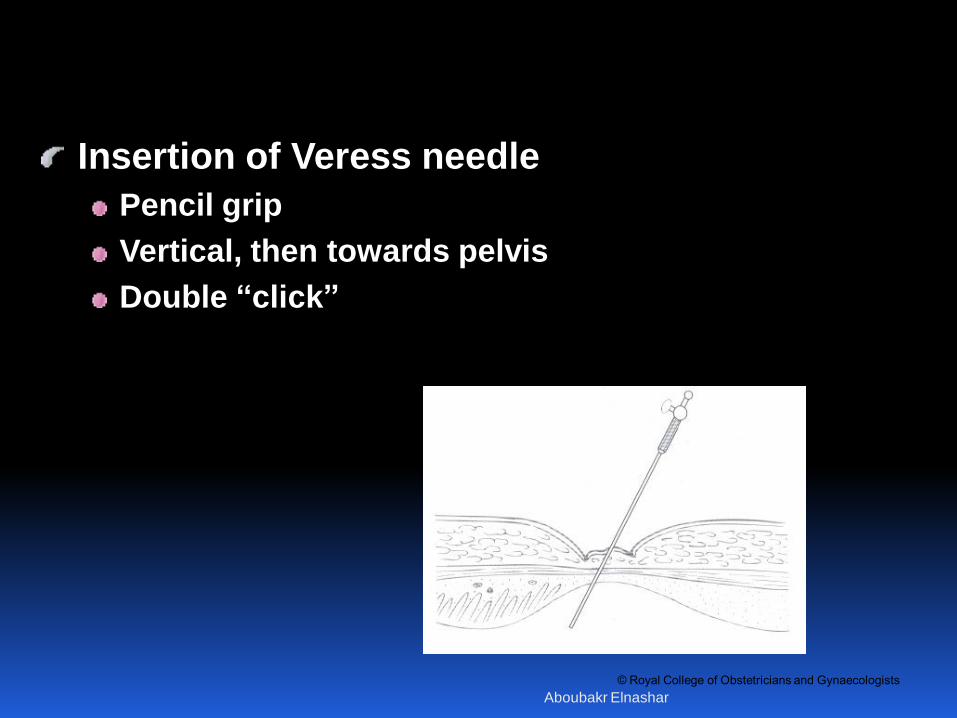
Insertion of Veress needle
Pencil grip
Vertical, then towards pelvis
Double “click”
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
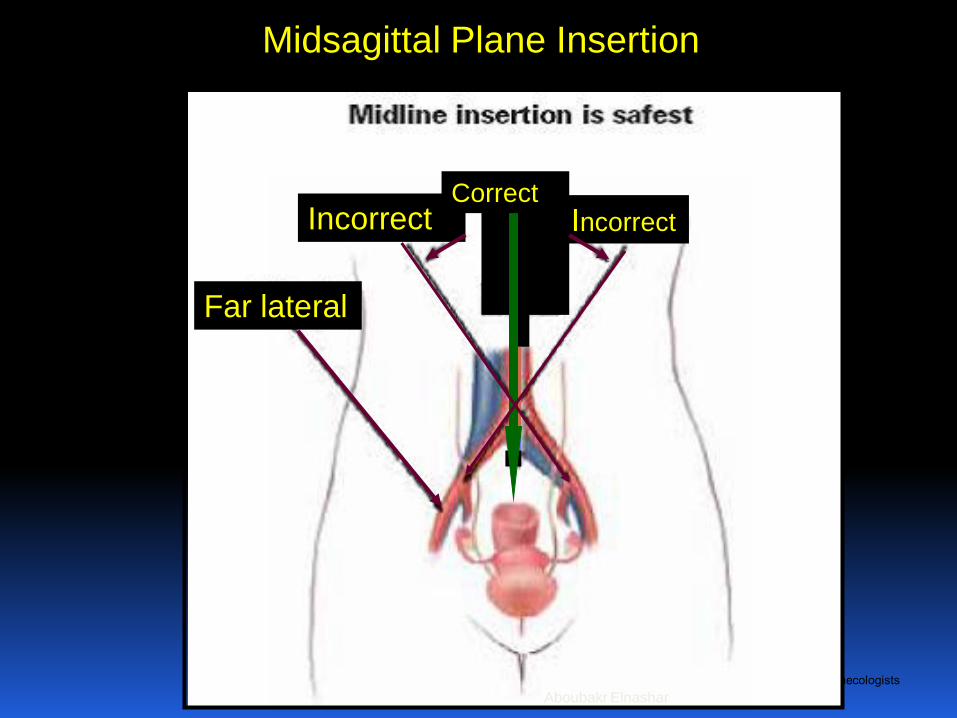
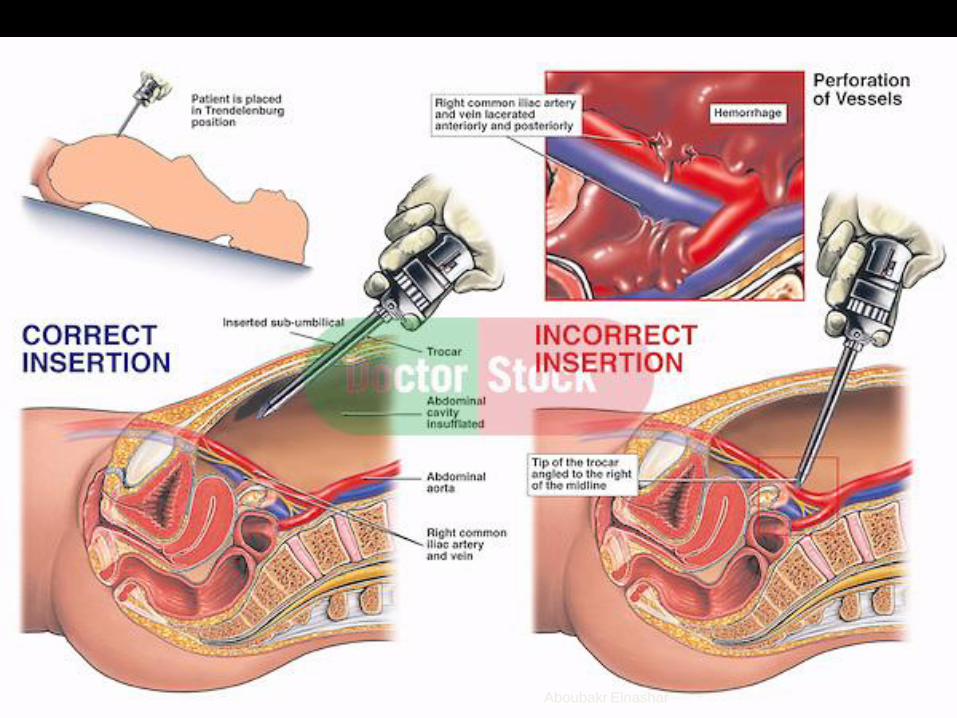
Far lateral
Incorrect Incorrect Correct
Midsagittal Plane Insertion
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
• The Veress needle should be sharp, with a good and tested
spring action. A disposable needle is recommended
• The lower abdominal wall should be stabilised in such a way
that the Veress needle can be inserted at right angles to the
skin
• Elevation of the anterior abdominal wall at the time of Veress
or primary trocar insertion is not routinely recommended, as it
does not avoid visceral or vessel injury. (II-2 B)
• The angle of the Veress needle insertion should vary
according to the BMI of the patient from 45 in non-obese
women to 90 in obese women. (II-2 B)
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
• Two audible clicks are usually heard as the layers of
the umbilicus are penetrated.
• Excessive lateral movement of the needle should be
avoided. This may convert a small needle point
injury in the wall of the bowel or vessel into a
complex tear
• Waggling of the Veress needle from side to side
must be avoided, as this can enlarge a 1.6 mm
puncture injury to an injury of up to 1 cm in viscera
or blood vessels. (II-1 A)
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
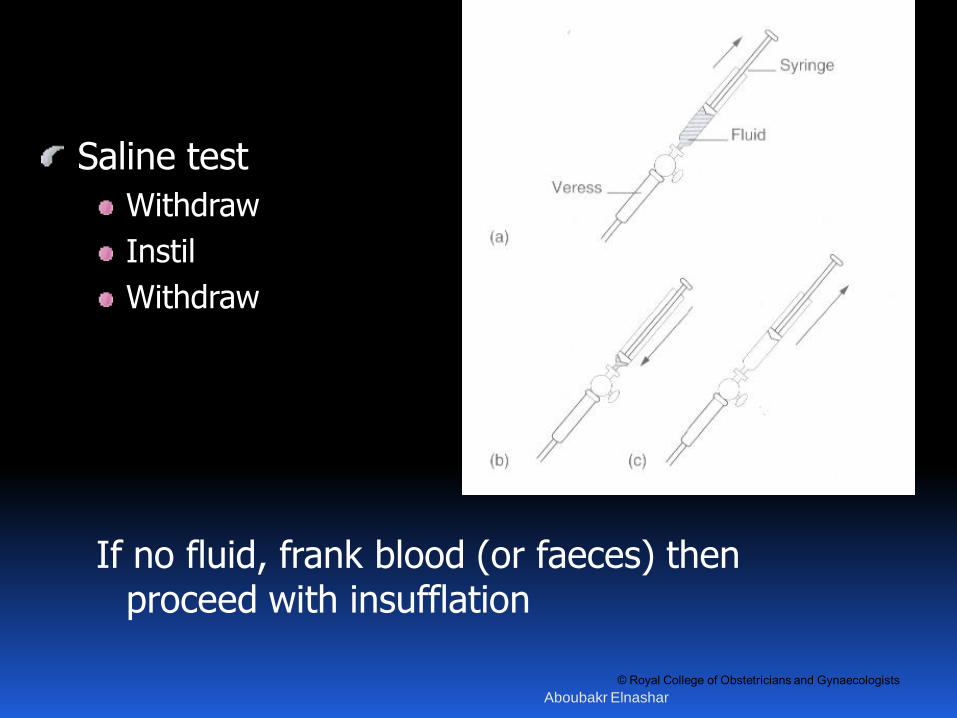
Saline test
Withdraw
Instil
Withdraw
If no fluid, frank blood (or faeces) then proceed with insufflation
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
• The saline test not 100% accurate
• The various Veress needle safety tests or checks
provide very little useful information on the placement
of the Veress needle. It is therefore not necessary to
perform various safety checks on inserting the Veress
needle
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
The most valuable test of correct placement of the
Veress needle is to observe that the initial insufflation
pressure is relatively low (less than 8mmHg) and is
flowing freely
• The Veress intraperitoneal (VIP-pressure 10mmHg) is
a reliable indicator of correct intraperitoneal placement
of the Veress needle; therefore, it is appropriate to
attach the CO2 source to the Veress needle on entry.
(II-1 A)
• After 2 failed attempts to insert the Veress needle,
either the open Hasson technique or Palmer’s point
entry should be used.
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
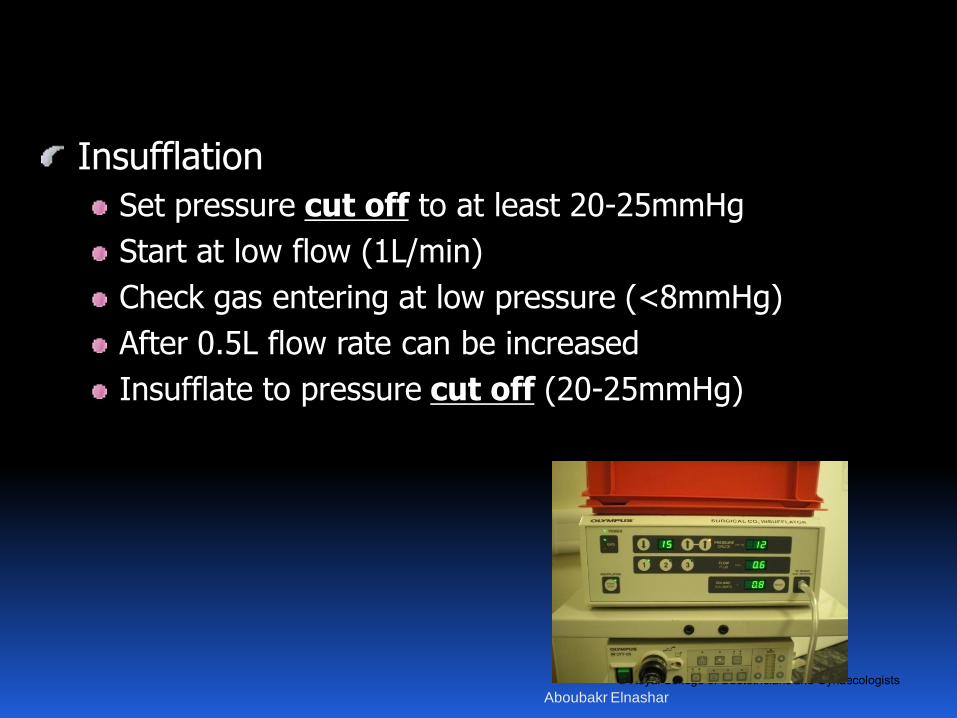
Insufflation
Set pressure cut off to at least 20-25mmHg
Start at low flow (1L/min)
Check gas entering at low pressure (<8mmHg)
After 0.5L flow rate can be increased
Insufflate to pressure cut off (20-25mmHg)
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
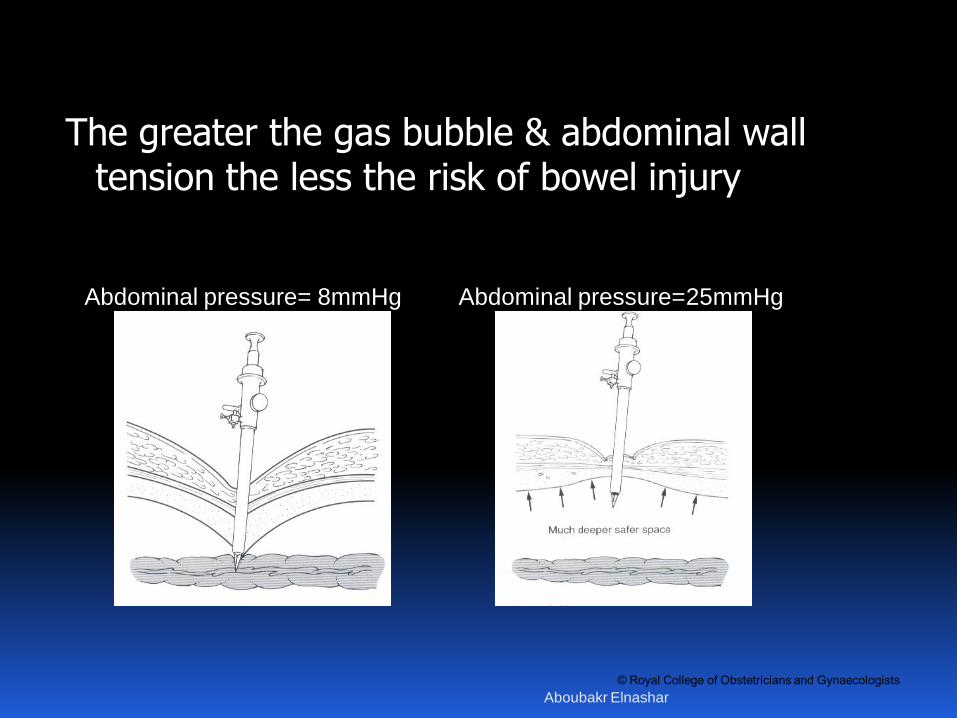
The greater the gas bubble & abdominal wall tension the less the risk of bowel injury
Abdominal pressure= 8mmHg Abdominal pressure=25mmHg
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
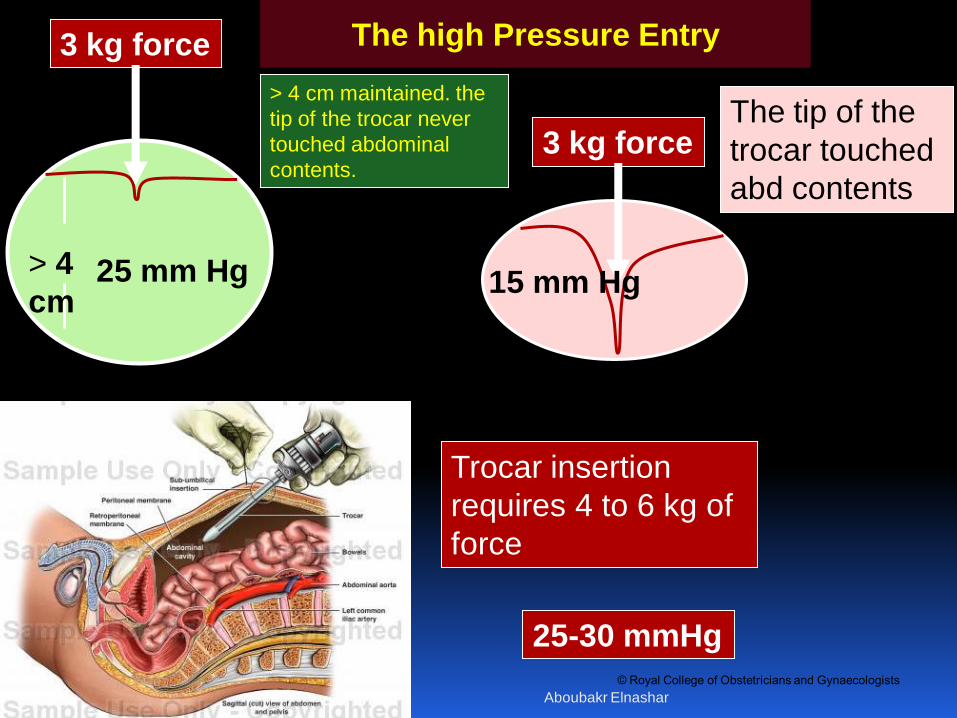
3 kg force
3 kg force
25 mm Hg 15 mm Hg
The tip of the
trocar touched
abd contents
> 4 cm maintained. the
tip of the trocar never
touched abdominal
contents.
Trocar insertion
requires 4 to 6 kg of
force
> 4
cm
The high Pressure Entry
25-30 mmHg
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
• An intra-abdominal pressure of 20–25 mmHg
should be achieved before inserting the primary
trocar
• The volume of CO2 inserted with the Veress
needle should depend on the intra-
abdominal pressure.
• Adequate pneumoperitoneum should be
determined by a pressure of 20 to 30 mm Hg
and not by predetermined CO 2 volume. (II-1
A)
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
The distension pressure should be reduced to
12–15 mmHg once the insertion of the trocars
is complete
In the Veress needle method of entry, the
abdominal pressure may be increased
immediately prior to insertion of the first
trocar. The high intraperitoneal (HIP-
pressure) laparoscopic entry technique does
not adversely affect cardiopulmonary
function in healthy women. (II-1 A)
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
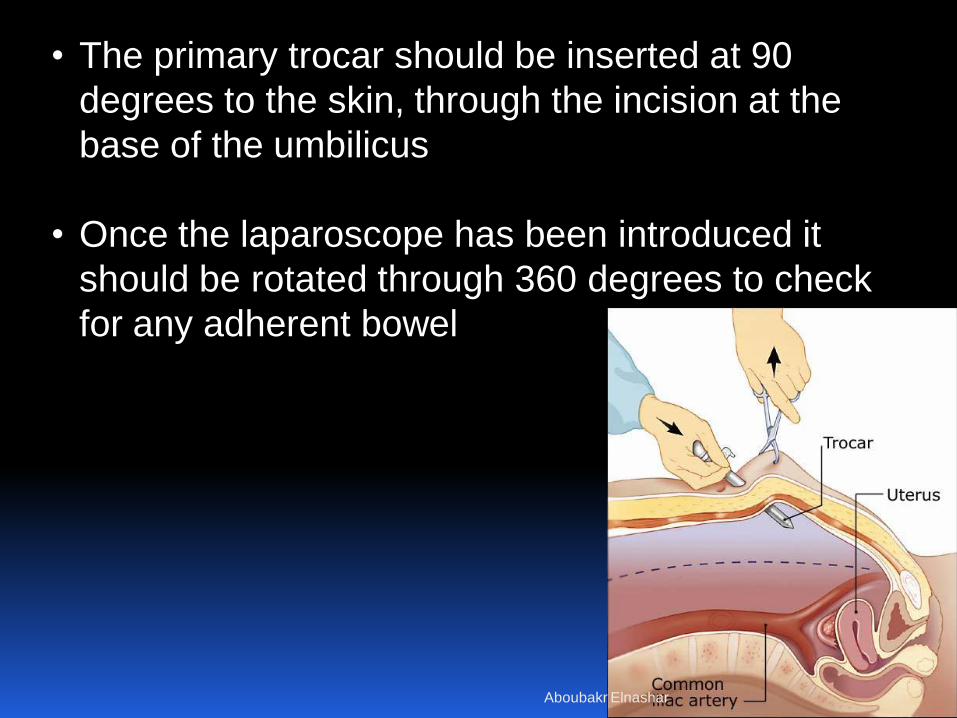
• The primary trocar should be inserted at 90
degrees to the skin, through the incision at the
base of the umbilicus
• Once the laparoscope has been introduced it
should be rotated through 360 degrees to check
for any adherent bowel
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
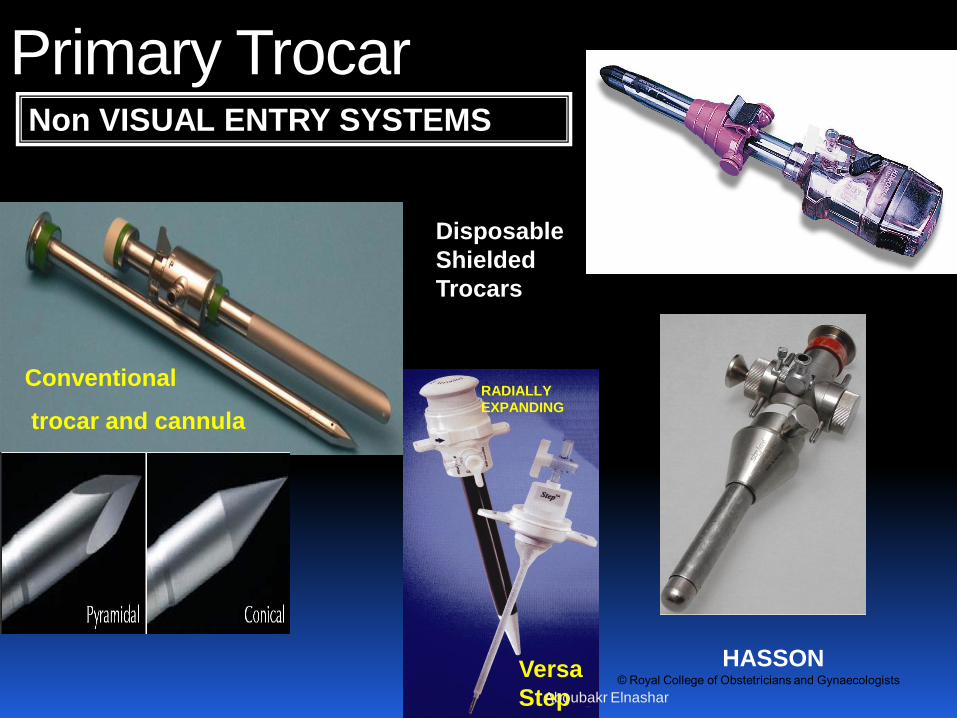
Primary Trocar Non VISUAL ENTRY SYSTEMS
Conventional
trocar and cannula
HASSON Versa
Step
RADIALLY
EXPANDING
Disposable
Shielded
Trocars
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
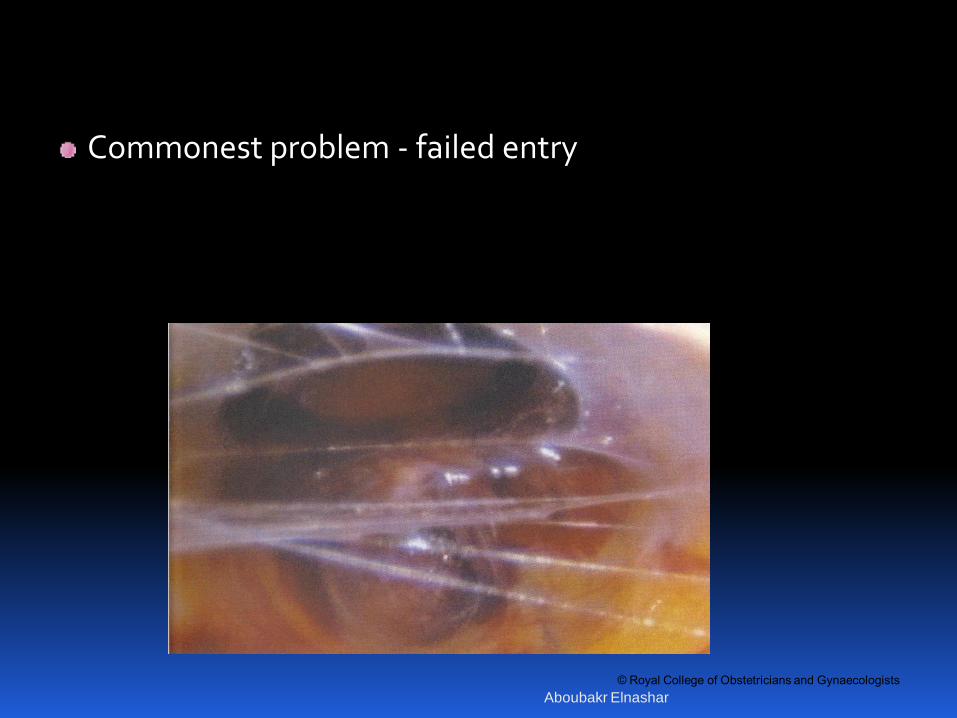
Commonest problem - failed entry
Insertion of subumbilical Veress needle
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
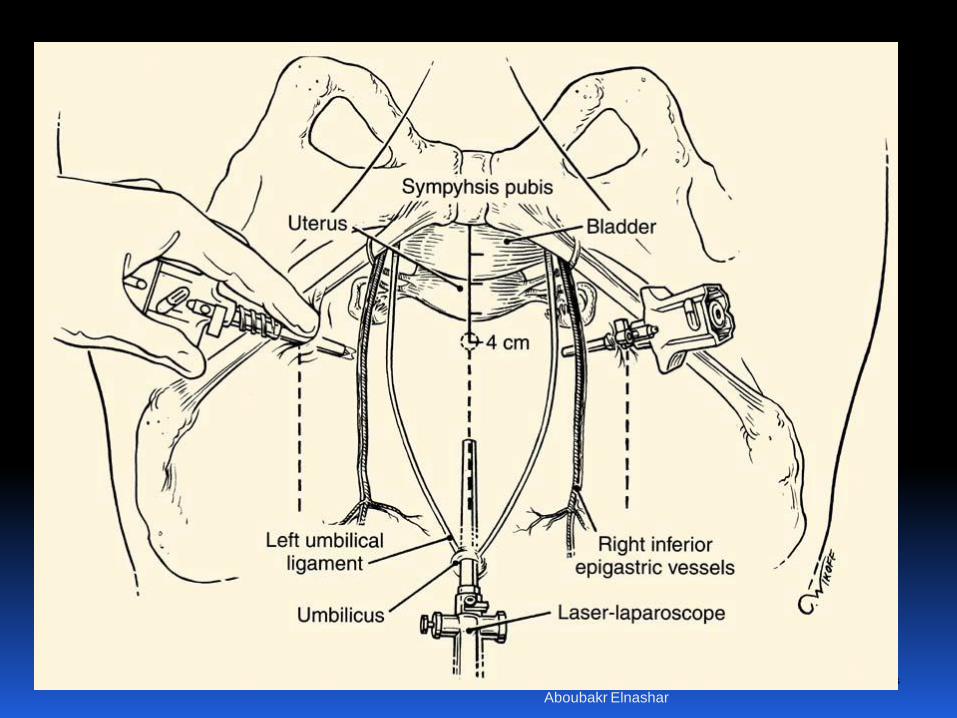
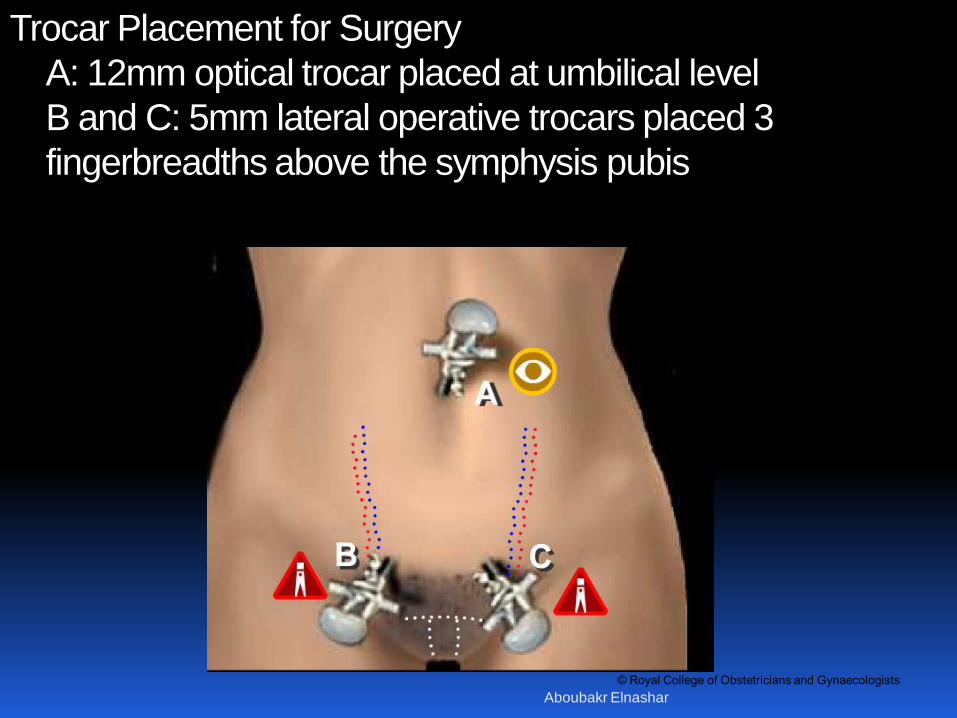
Trocar Placement for Surgery
A: 12mm optical trocar placed at umbilical level
B and C: 5mm lateral operative trocars placed 3
fingerbreadths above the symphysis pubis
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
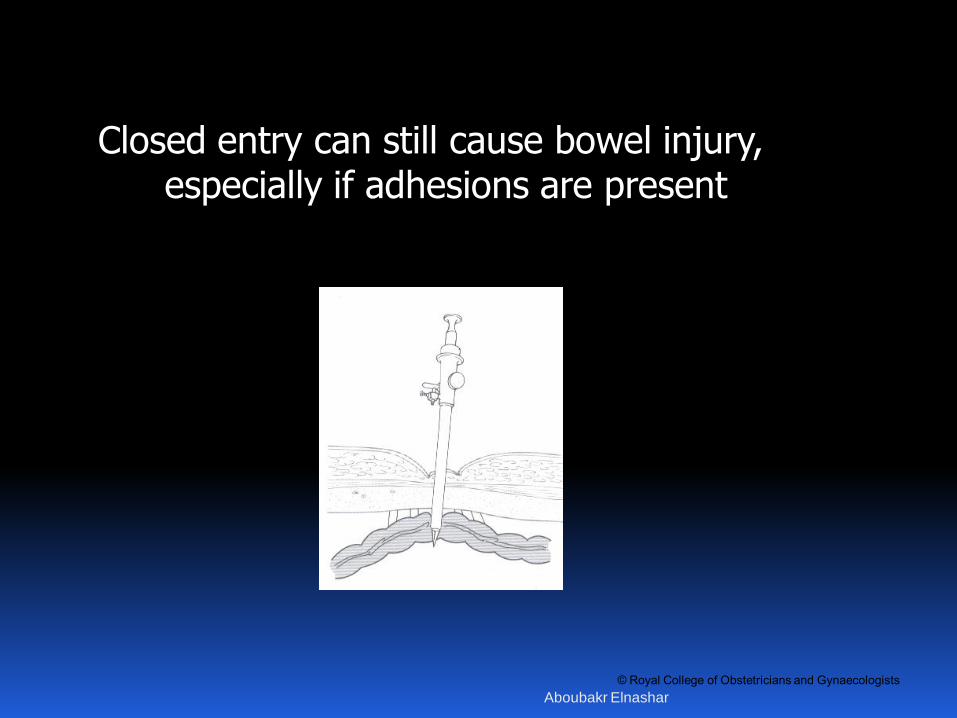
Closed entry can still cause bowel injury, especially if adhesions are present
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
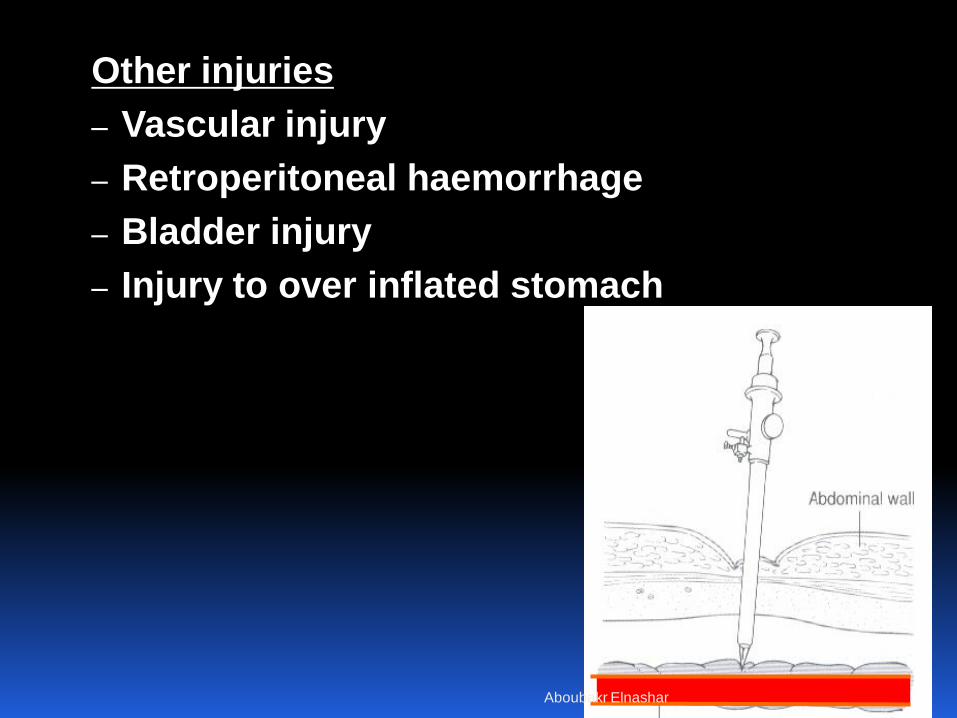
Other injuries
– Vascular injury
– Retroperitoneal haemorrhage
– Bladder injury
– Injury to over inflated stomach
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
Secondary ports are inserted under direct
vision - an inadvertent injury from a
secondary port could be considered
negligent”
Principles
Avoid inferior epigastric vessels
Avoid bowel/vascular injury
Minimise hernia risk
3. SECONDARY PORTS
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
• Secondary ports inserted under direct vision at
right angles to the skin at 20–25 mmHg
pneumoperitoneum
• Inferior epigastric vessels should be visualised
laparoscopically prior to secondary port placement
• Once the trocar has pierced the peritoneum it
should be angled towards the anterior pelvis
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
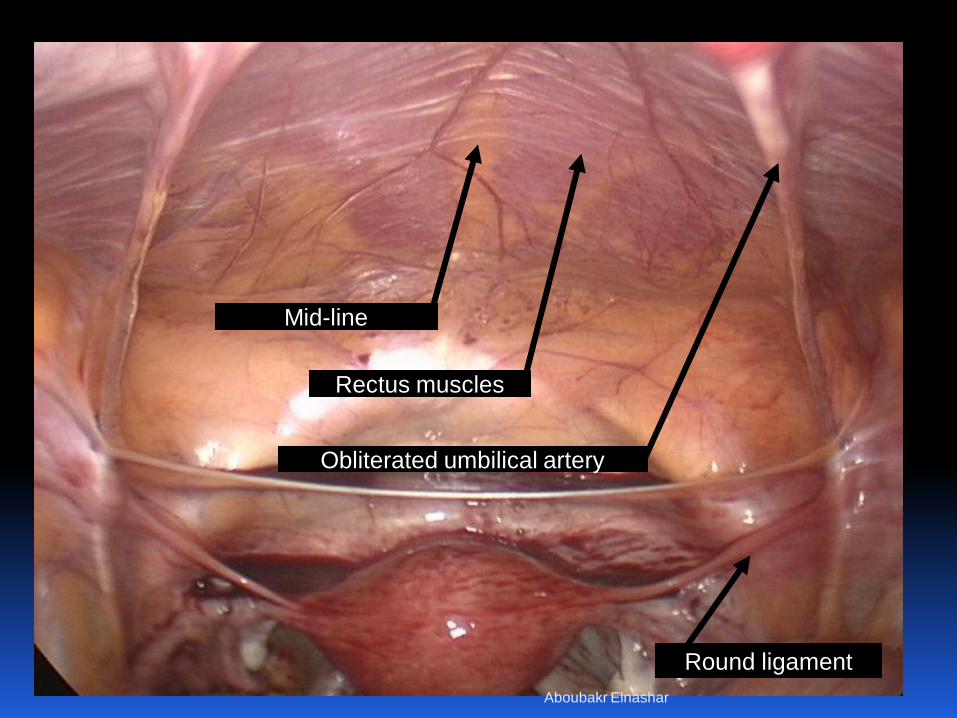
Round ligament
Obliterated umbilical artery
Rectus muscles
Mid-line
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
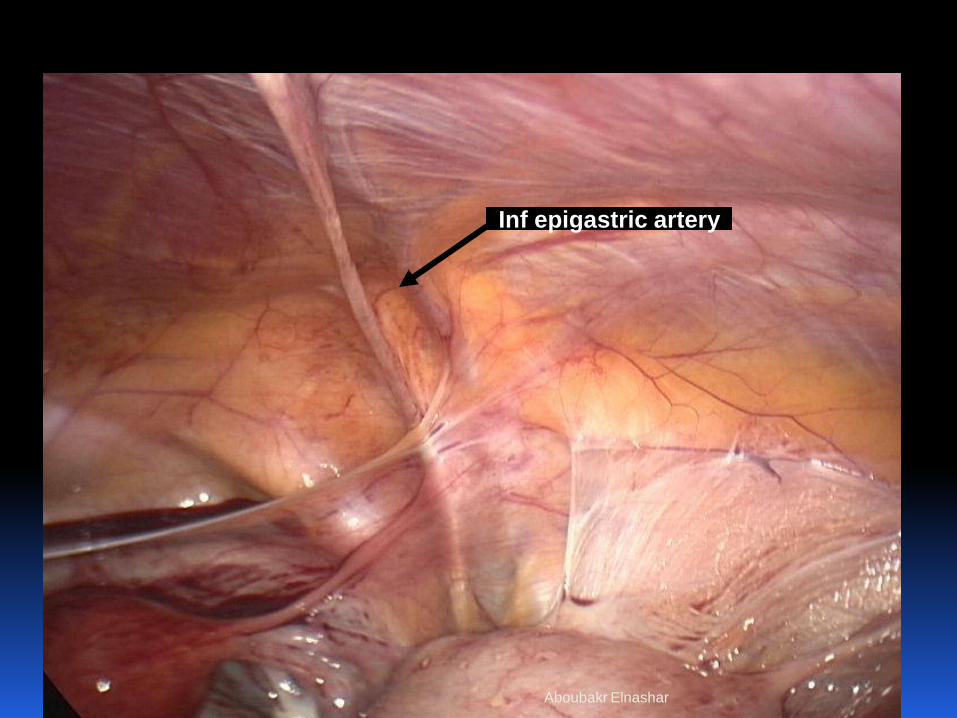
Inf epigastric artery
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
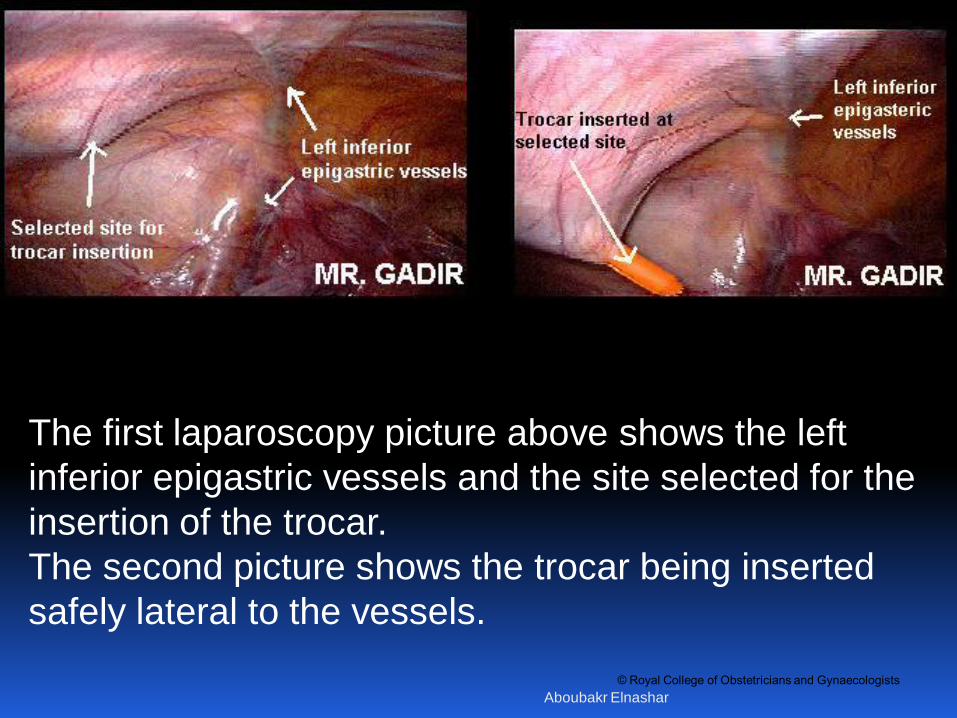
The first laparoscopy picture above shows the left
inferior epigastric vessels and the site selected for the
insertion of the trocar.
The second picture shows the trocar being inserted
safely lateral to the vessels.
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
Alternatives to closed umbilical entry
considered:
If there is risk of umbilical adhesions - previous
(midline) laparotomy
In very slim or morbidly obese women
Failed saline test or Veress insertion x2
Unsatisfactory closed Veress insufflation
Alternatives include:
Open entry – variations of Hassan technique
Palmer’s point closed entry
4. PRIMARY PORT –ALTERNATIVES
Aboubakr Elnashar

© Royal College of Obstetricians and Gynaecologists
Aboubakr Elnashar

© Royal College of Obstetricians and Gynaecologists
Palmer’s point is the preferred alternative trocar
insertion site, except in cases of previous surgery
in this area or splenomegaly.
Left upper quadrant (LUQ, Palmer’s) laparoscopic
entry should be considered in patients with suspected
or known periumbilical adhesions or history or
presence of umbilical hernia, or after three failed
insufflation attempts at the umbilicus. (II-2 A)
Other sites of insertion, such as transuterine Veress
CO2 insufflation, may be considered if the umbilical
and LUQ insertions have failed or have been
considered and are not an option. (I-A)
Aboubakr Elnashar
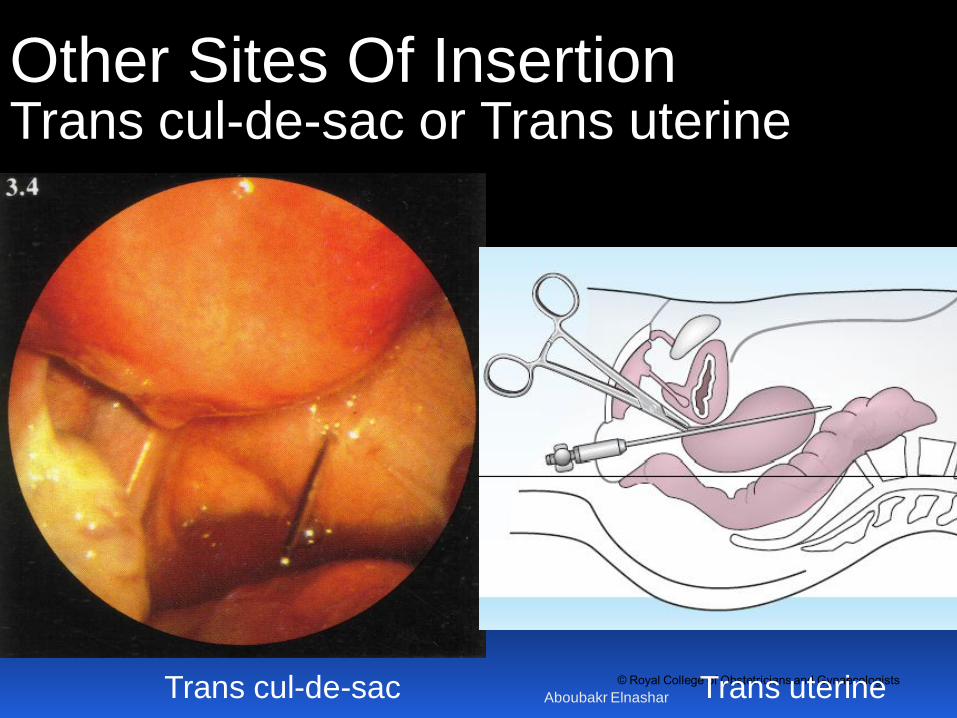
© Royal College of Obstetricians and Gynaecologists Trans cul-de-sac Trans uterine
Other Sites Of Insertion Trans cul-de-sac or Trans uterine
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
When Hasson open laparoscopic entry is employed,
confirm that the peritoneum has been opened by
visualising bowel or omentum
The open entry technique may be utilized as an
alternative to the Veress needle technique, although
the majority of gynaecologists prefer the Veress
entry. There is no evidence that the open entry
technique is superior to or inferior to the other entry
techniques currently available. (II-2 C)
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
Direct insertion of the trocar without prior
pneumoperitoneum may be considered as a safe
alternative to Veress needle technique. (II-2)
Direct insertion of the trocar is associated with less
insufflation-related complications such as gas
embolism, and it is a faster technique than the
Veress needle technique. (I)
Shielded trocars may be used in an effort to
decrease entry injuries. There is no evidence that
they result in fewer visceral and vascular injuries
during laparoscopic access. (II-B)
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
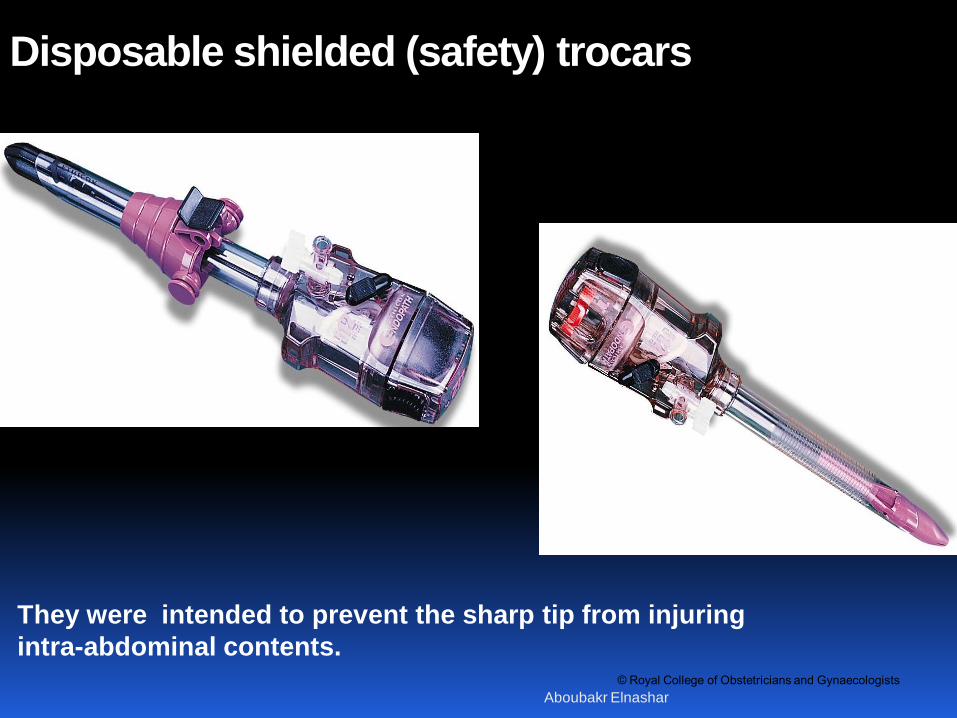
Disposable shielded (safety) trocars
They were intended to prevent the sharp tip from injuring
intra-abdominal contents.
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
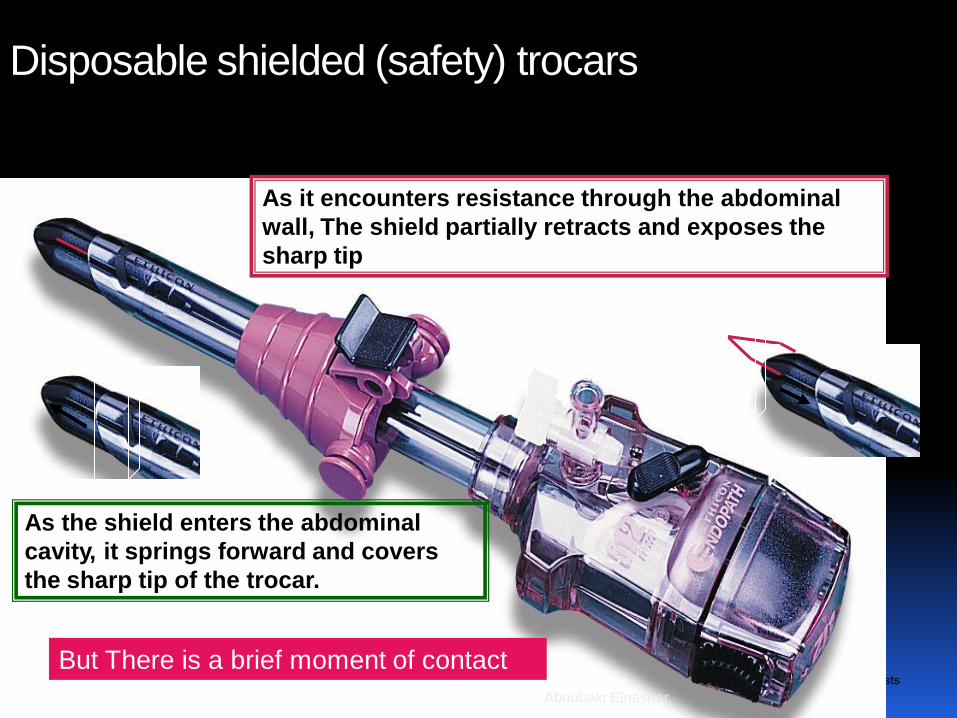
Disposable shielded (safety) trocars
As it encounters resistance through the abdominal
wall, The shield partially retracts and exposes the
sharp tip
As the shield enters the abdominal
cavity, it springs forward and covers
the sharp tip of the trocar.
But There is a brief moment of contact
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
Radially expanding trocars are not recommended
as being superior to the traditional trocars. They do
have blunt tips that may provide some protection
from injuries, but the force required for entry is
significantly greater than with disposable trocars. (I-
A)
The visual entry cannula system may represent
an advantage over traditional trocars, as it allows a
clear optical entry, but this advantage has not been
fully explored. The visual entry cannula trocars have
the advantage of minimizing the size of the entry
wound and reducing the force necessary for
insertion. Visual entry trocars are non-superior to
other trocars since they do not avoid visceral and
vascular injury. (2 B) Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
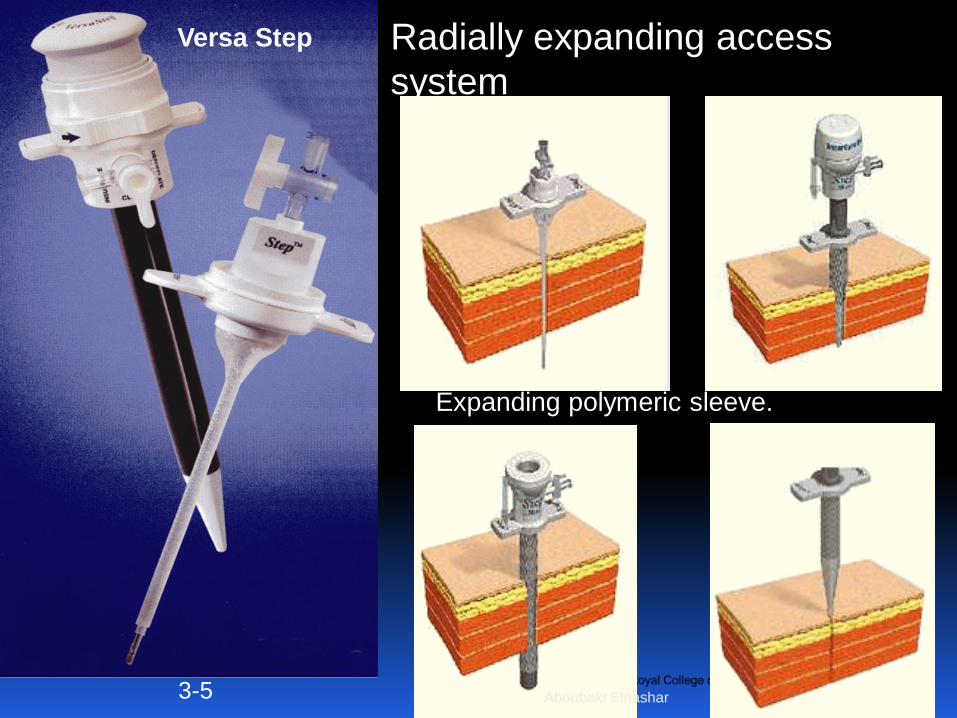
Versa Step
3-5
Radially expanding access
system
Expanding polymeric sleeve.
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
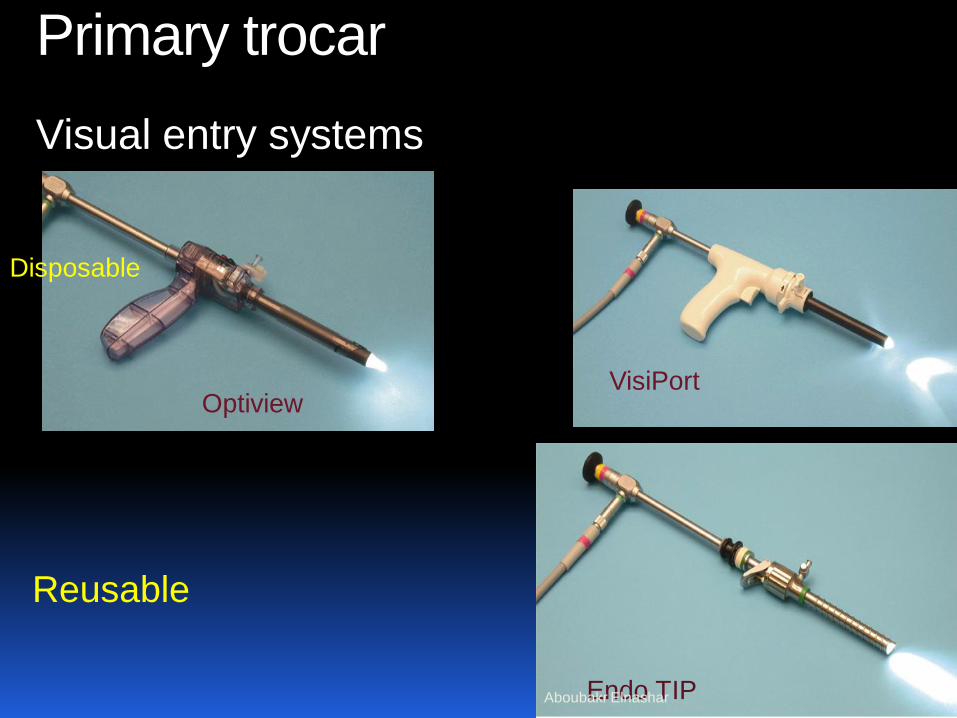
Primary trocar
Visual entry systems
Endo TIP
VisiPort Optiview
Disposable
Reusable
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
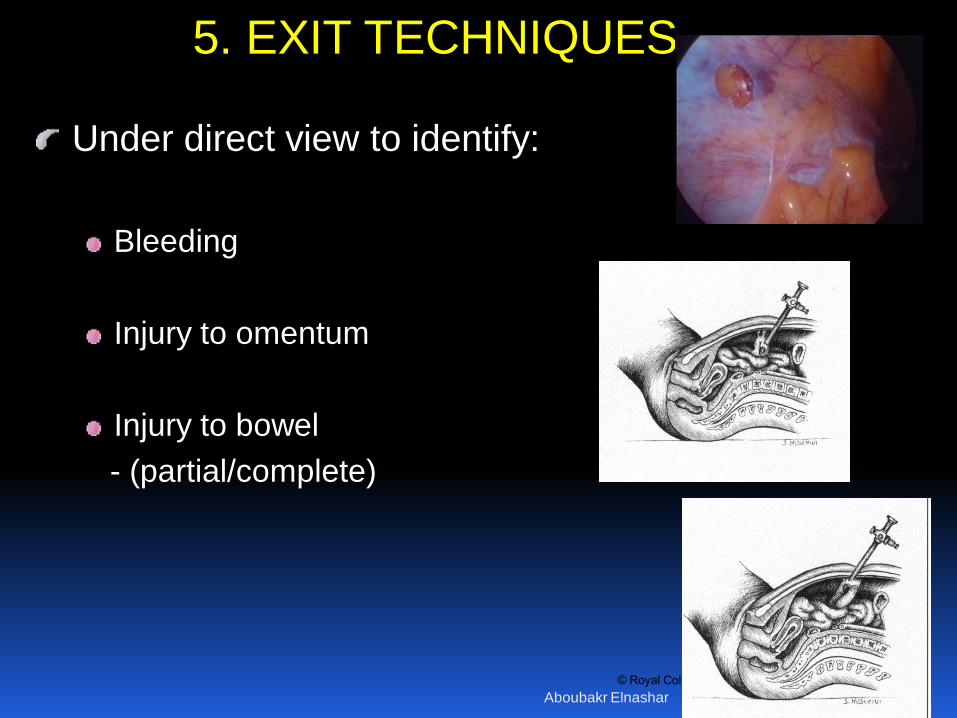
Under direct view to identify:
Bleeding
Injury to omentum
Injury to bowel
- (partial/complete)
5. EXIT TECHNIQUES
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
• On removal of a laparoscope. Check by direct
visualisation that there has not been a through-
and-through injury of bowel adherent under the
umbilicus
• Secondary ports must be removed under direct
vision to ensure that any haemorrhage can be
observed and treated, if present.
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
Wound closure:
Proper closure of fascia within umbilical port site to prevent wound dehiscence or hernia
Avoid hernia risk by closing sheath:
- Midline port sites > 7mm
- Lateral port sites > 5 mm
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
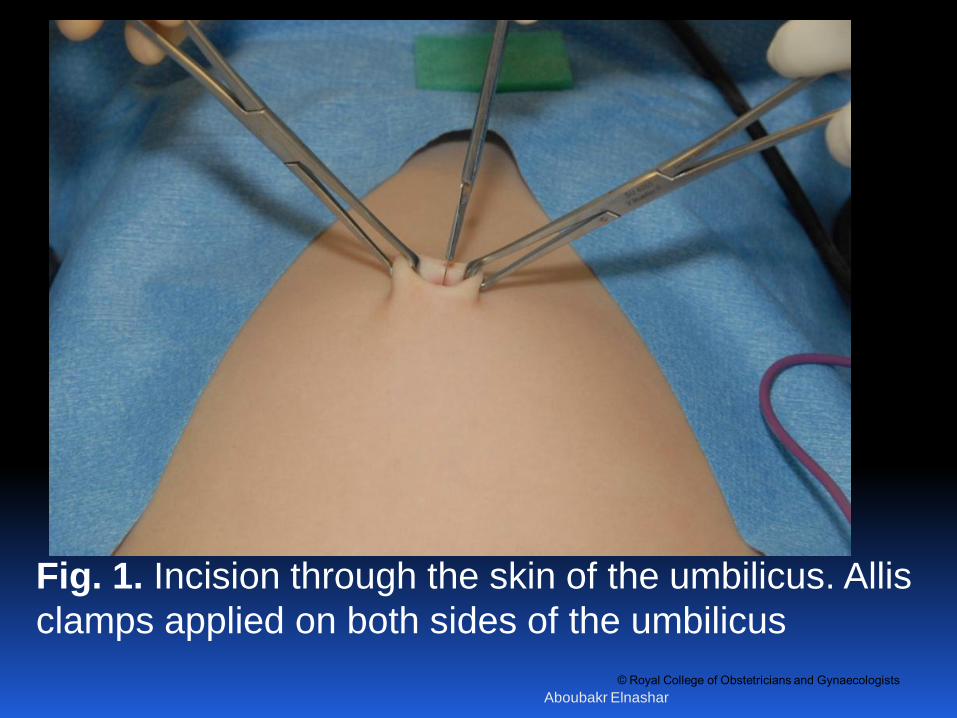
Fig. 1. Incision through the skin of the umbilicus. Allis
clamps applied on both sides of the umbilicus
Aboubakr Elnashar

© Royal College of Obstetricians and Gynaecologists
Fig. 2. Incision through the fascia and peritoneum.
Kocher clamps applied on the fascia
Aboubakr Elnashar

© Royal College of Obstetricians and Gynaecologists
Fig. 3. Metzembaum scissors in the abdominal cavity
to confirm successful entry Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
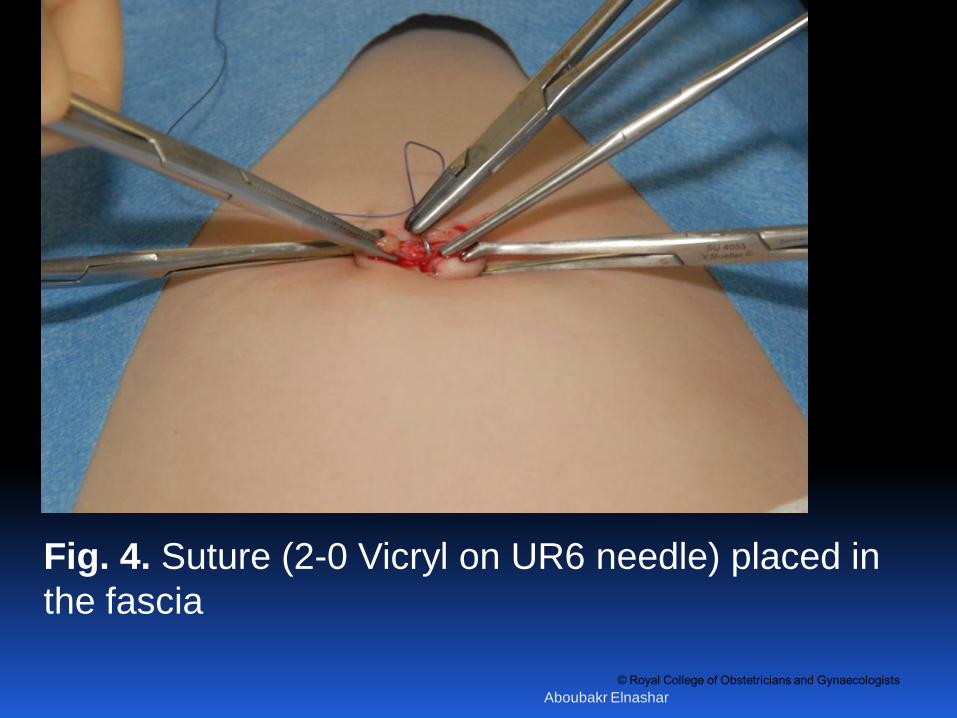
Fig. 4. Suture (2-0 Vicryl on UR6 needle) placed in
the fascia
Aboubakr Elnashar

© Royal College of Obstetricians and Gynaecologists
Fig. 5. Hasson port (Ethicon Xcel) placed in the
abdomen
Aboubakr Elnashar
© Royal College of Obstetricians and Gynaecologists
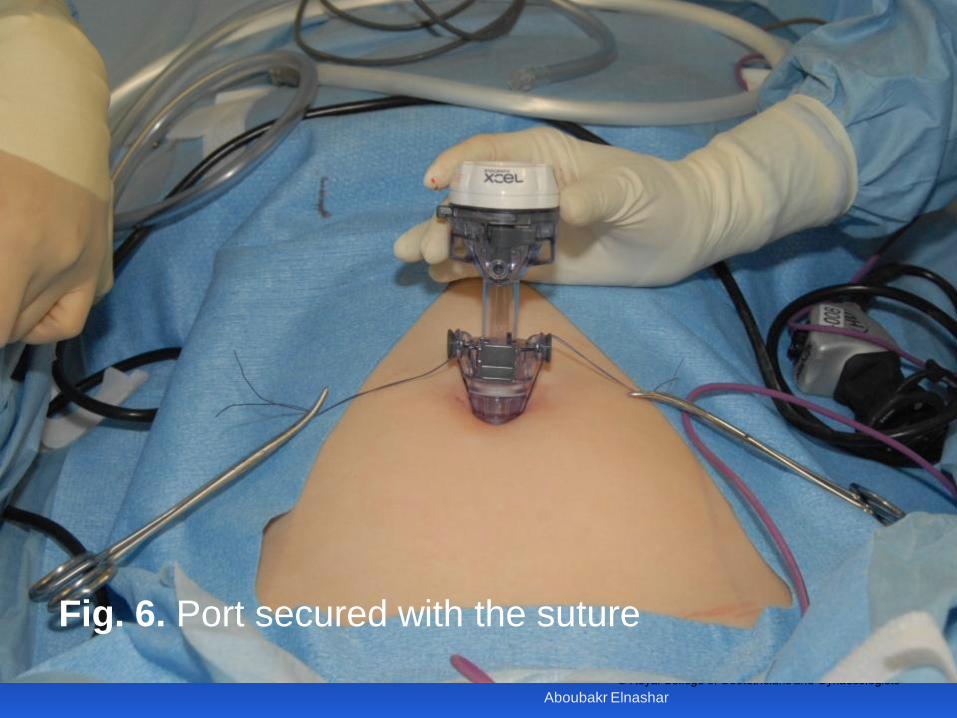
Fig. 6. Port secured with the suture
Aboubakr Elnashar

© Royal College of Obstetricians and Gynaecologists
Aboubakr Elnashar





























