Embed Size (px)
DESCRIPTION
Clinical Chemistry 1
Citation preview

LIPIDS & DYSLIPOPROTEINEMIA
Merlyn A. Baraclan, RN, RMT

TOPIC OUTLINE Overview on Lipids Lipoproteins,
Apoliporoteins & Related Proteins
Lipid Transport & Lipoprotein Metabolism
Lipid & Lipoprotein Measurement
The NCEP Guidelines Lipids, Lipoproteins &
Disease References

LIPIDS are biological
compounds which are soluble in nonpolar organic solvents but relatively insoluble in polar solvents.

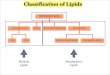
MAJOR BODY LIPIDS
Triglycerides / TAG / TG Cholesterol / C Phospholipids
Glycolipids

BIOLOGIC ROLES OF LIPIDS
Primary source of fuel Components of cell membranes &
many cell structures Provide stability to cell membranes Means of transmembrane transport

LIPOPROTEINS
The function of lipoprotein particle is to transport lipids around the body in the blood.
Contain cholesterol in 2 forms: _ free cholesterol_ cholesterol ester
Lipoproteins have a micellar structure.

LIPOPROTEINS The transport proteins of lipids
having a micellar structure composed of two parts as follows:
Central corecontains TAG and cholesterol ester
nonpolar moiety
Surface coatcontains PL, free cholesterol, and apolipoproteins

4 MAJOR LIPOPROTEIN CLASSES
- Chylomicrons (CM) - very low density lipoproteins
(VLDL)
- low density lipoproteins (LDL)
- high density lipoproteins (HDL)

LIPOPROTEINSCLASS DENSITY
(g/ml)MEAN
DIAMETER
(mm)
source Principal function
Electropho
retic mobility
CM < 0.95 500 intestine Transport ofExogenous
TAG
Remains at Origin
VLDL 0.96 -1.006
43 liver Transport of Endogenous
TAG
Pre β
IDL 1.007-1.019
27 Catabolism of VLDL
Precursor of LDL
“broad β”
LDL 1.020-1.063
22 Catabolism of VLDL via IDL
CholesterolTransport
β
HDL 1.064-1.210
8 Liver,intestine,catabolism of CM & VLDL
“reversecholesteroltransport”
α

CHEMICAL COMPOSITION OF MAJOR CLASSES OF PLASMA PROTEINS
CLASS PROTEIN%
TAG%
CHOLESTEROL%
PHOSPHO LIPID
%
Chylomicron/ CM
1-2 85 - 95 3 -5 5 -10
VLDL 10 60 -70 10 -15 10 – 15
LDL 15 -25 5 - 10 45 20 -30
HDL 50 Verylittle
20 30



LIPOPROTEINS , APOLIPOPROTEINS & RELATED PROTEINS
MAJOR LIPOPROTEINS
1. CHYLOMICRONS / CM- Produced by the intestine- Transport lipids of dietary origin- Poor in free cholesterol- Has a “very high lipid/protein ratio- “milky plasma”- “Floating creamy layer”- Removed by the liver

MAJOR LIPOPROTEINS
2. VERY LOW DENSITY LIPOPROTEINS / VLDL
- Produced by the liver- Supplies the body w/ TAG of
endogenous origin & also cholesterol- “ turbid plasma”

MAJOR LIPOPROTEINS
3. LOW DENSITY LIPOPROTEINS / LDL
- Produced by the metabolism of VLDL- The particles do not scatter light- Removed by the liver & macrophages

MAJOR LIPOPROTEINS 4. HIGH DENSITY LIPOPROTEIN /
HDL
- Consists mostly of proteins- Produced by the liver- “reverse cholesterol transport”- Cardioprotective

MINOR & ABNORMAL LIPOPROTEINS
1. Lipoprotein (a) / Lp (a)- Similar to LDL - Synthesized in the liver- “lipid staining pre β band”- Has atherogenic properties- 2. LPX Lipoprotein- Seen in patients with obstructive biliary
disease, & with LCAT deficiency- 3. β – VLDL - “Floating β lipoprotein”

EXOGENOUS (DIETARY) LIPID PATHWAYFood intestinal absorption
CM High TAG,Low Chol, Apo B48
TAG in adipose tissue
Muscle & FFA
chylomicron remnants taken by the liver

ENDOGENOUS LIPID PATHWAY FFA TAG synthesis in liver, intestine VLDL
High TAG
Low Chol
FFA Apo B100
LPL Apo E
IDL
Apo E Binds onto hepatocytes through Apo E
LDL LDL binds to the receptors in liver (70%)
& other tissues (30%)

HDL PATHWAYliver secretes Apo A1 + other Apos + PLs Nascent
HDL
Cholesterol from tissues
HDL 3
Esterification of Cholestrol by LCAT
LDL
uptake by liver
Cholesterol transfer to VLDL
excretion into bile

C.1 BLOOD SAMPLING & STORAGE
BIOLOGIC VARIATION FASTING POSTURE
VENOUS VS. CAPILLARY
PLASMA VS. SERUM STORAGE

BLOOD SAMPLING & STORAGE
BIOLOGIC VARIATION- Cholesterol level rises w/ age - Women have lower levels than
men (except in childhood & after the early 50’s)
- Age related variation is the basis of NCEP recommendation that cholesterol screening be repeated every 5 years.

BLOOD SAMPLING & STORAGE FASTING- 12 hours before venipuncture- Chylomicrons are completely cleared
w/in 6 – 9 hours - NCEP Adult Treatment Panel III( ATP III),
has recommended that patients fast for at least 9 hours before blood specimens are taken for lipid & lipoprotein analysis
POSTURE- Current NCEP guidelines recommend
that patients be seated for 5 minutes prior to sampling.

BLOOD SAMPLING & STORAGE VENOUS VS. CAPILLARY SAMPLES- Measurements in capillary blood samples
are lower than venous samples & tend to be more variable.
PLASMA VS. SERUM- Either plasma or serum can be used when
only TAG, cholesterol & HDL are measured, & LDL – C is calculated from these three measurements.
- Plasma is preferred when lipoproteins are measured by ultracentrifugal or electrophoretic methods

BLOOD SAMPLING & STORAGE PLASMA VS. SERUM Cont.- EDTA is the preferred anticoagulant - ♥- Heparin – X- Citrate – X STORAGE- When serum or plasma must be stored
for long periods it should be maintained at a temperature of -70⁰C.
- For short term storage, the samples can be kept at – 20⁰C.

LIPID & LIPOPROTEIN MEASUREMENT A. TAG measurementChemical Nonenzymatic MethodsGeneral Steps1. Extraction- To remove TAG from LP’s- Accomplished by using MeOH, EtOH,
isopropyl alcohol, Folch’s rgt & diethyl ether
- - removal of interferences by zeolite

A. TAG MEASUREMENT
2. Hydrolysis of TAG into FFA & Glycerol- By saponification w/ alcoholic KOH
3. Measurement of Glycerol- The glycerol liberated is oxidized by
periodate to HCHO & quantified by using any of the ff:
- Eegrine reaction- Schryver’s reaction- Pay’s reaction- Hantzsch reaction (method of choice)

A. TAG MEASUREMENT Enzymatic Methods- Based on the hydrolysis of TAG & the
measurement of glycerol that is released in the reaction:
LPS- TAG + 3H2O glycerol + fatty acid- Methods:- Boculo David - Megraw - Winartasaputra- Nagele - Trinder

B. CHOLESTEROL MEASUREMENT Chemical Nonenzymatic Methods4 General Steps1. Extraction- Using Bloor’s rgt (3:1 EtOH – ether) or
zeolite extraction2. Saponification- Using KOH3. Purification- Using digitonin4. Color development- May proceed w/ the Leibermann-
Burchardt reaction or Salkowski reaction

B. CHOLESTEROL MEASUREMENT
Leibermann - Burchardt reaction- Uses sulfuric acid & acetic anhydride to
produce an unstable green cholestadienyl monosulfonic acid; color stabilized by sodium sulfate
Zak or Salkowski reaction- Uses sulfuric acid & ferric ions to
produce a stable red to red – violet cholestadienyl disulfonic acid

CHOLESTEROL MEASUREMENT NONENZYMATIC 1 Step Methods- Zlatkis – Zak Boyle method- Ferro – Ham method- Pearson – Stern – MacGavack- Wybenga et al 2 Step Methods- Carr – Drekter 3 Step Methods- Abell – Kendall method (Standard reference
method) 4 Step Methods- Schoenheimer – Sperry - Parek – Jung- Sperry - webb

CHOLESTEROL MEASUREMENT: ENZYMATIC (CHOD – PAP) cholesterol ester
Cholesterol ester + H2O cholesterol + FFA
hydrolase
cholesterol
Cholesterol + O2 cholest – 4 – en – 3 – one + H2O2
oxidase
peroxidase
H2O2 + phenol + 4 aminoantipyrine quinoneimine dye
+ 2 H2O

LIPOPROTEIN MEASUREMENT 1. HDL Measurement- Polyanion precipitation- Electrophoresis – spectrophotometric
det’n- Ultracentrifugation ( reference method) 2. Chylomicrons / CM- Standing Plasma Test 3. Lipid Profile- Use of the Friedewald equation


THE NCEP GUIDELINES Testing & TreatmentCholesterol Goals:ATP III recommends a complete
lipoprotein profile as the initial test for evaluating blood cholesterol.
Testing should be performed on all adults aged 20 & older & should be repeated once every 5 years.
The need for a therapeutic lifestyle change & drug therapy

ATP III CLASIFICATION FOR LIPID VALUES
For Cholesterol: conversion factor to convert mg/dL to mM is 0.02586For triglyceride : conversion factor to convert mg / dL to mM is 0.011 LDL
CholesterolHDL
Cholesterol
Total Cholesterol
Triglyceride
<100 optimal < 40
low < 200
desirable < 150
normal
100-129
Near optimal / above optimal
≥ 90 high 200-239
Borderline
high
150 -199
Borderline high
130-159
Borderline
high
≥ 240 high 200 -499
high
160 -189
High ≥ 500 Very high
≥190 Very high

HYPERLIPIDEMIA DRUGS
Drug Class Mechanism of Action Example
Statins Lowers LDL cholesterol Lovastatin , simvastatin,Pravastatin, fluvastatin
Fibric acid derivatives
Lowers TAG Gemfibrosil, Fenofibrate
Bile acid resins
Lowers LDL cholesterol Colestipol, cholestyramine
Niacin (nicotinic acid)
Lowers TAG niacin

E. LIPIDS, LIPOPROTEINS & DISEASE
CHD (coronary heart
disease) Atherosclerosis

RISK FACTORS OF CHDPositive
Age: Male 45 yrs and above, Females 55 yrs and above or premature menopause without estrogen therapyFamily history of premature CHDCurrent cigarette smokingHypertension (equal or more than 140/90 mmHg or on antihypertensive therapy)Low HDL-Chol (<35 mg/dl)Diabetes mellitus
NegativeHigh HDL-Cholesterol (equal to or above 60 mg/dl)

HIGH CHOLESTEROL WITH HIGH LDL - CHOLESTEROL
hyperbetalipoproteine-
mia Elevated LDL – C Normal TAG High cardiac risk Commonly
encountered
SPECIFIC DISEASES- Polygenic (Nonfamilial)
Hypercholesterolemia- Familial
hypercholesterolemia/FH
- Familial Defective Apo B
- Sitosterolemia

HIGH TAG WITH NORMAL CHOLESTEROL
Due to the elevation of TAG rich particles
Hyperprebetalipo – proteinemia
secondary to excess alcohol & high carbohydrate intake
SPECIFIC DISEASES- Diabetic dyslipidemia- Familial
hypertriglyceridemia- Lipoprotein lipase
deficiency- Apo C II deficiency- Apo C III excess

LIPIDOSES
A group of inherited disorders characterized by the accumulation of lipids in tissues especially the “brain” due to a deficiency in a particular sphingolipid catabolic enzyme

LIPIDOSES: Niemann – Pick disease- Deficiency in sphingomyelinase & accumulation of
sphingomyelin Gaucher’s disease- Deficiency in β – D glucosidase & the
accumulation of glucocerebroside Krabbe’s disease- Deficiency in β – D galactosidase & the
accumulation of galactocerebrosides Fabry’s disease- Deficiency in α – D galactosidase & the
accumulation of ceramide trihexoside Tay – Sach’s disease- Deficiency in β – D hexaminidase & the
accumulation of β - sulfogalactocerebroside

KEY POINT SUMMARY Ultracentrifugation & electrophoretic techniques
are of historical significance, MOST useful lipid & lipoprotein testing are now enzymatic.
LDL – cholesterol can be measured directly , but is usually calculated using the Friedewald formula.
LDL – C is now considered the MOST important value in assessing cardiac risk & directing therapy.
The profile for initial adult screening aged 20 & above, includes TC, TAG, HDL – C & LDL – C & should be repeated every 5 years.

F. REFERENCES INTERNET SOURCES Bhagavan NV (2002).
Medical Biochemistry. San Diego: Harcourt/Academic Press. ISBN 0-12-095440-0. http://books.google.com/?id=vT9YttFTPi0C&printsec=frontcover.
http://biology.clc.uc.edu/courses/bio104/lipids.htm
BOOK SOURCES Clinical Diagnosis and
Management by Laboratory Methods / John Bernard Henry.
20th ed. 224 – 248
Henry’s Clinical Diagnosis and Management by Laboratory
Methods / Richard McPherson & Mathhew Pincus. 21st ed. 200 –
219 Clinical Chemistry: Principles,
Procedures & Correlations / Michael Bishop, Janet Engelkirk
& Edward Fody. 4th ed. 232 – 259 Southwestern University
College of Medical Technology Clinical Internship Manual / 2005
ed. Southwestern University College of
Medical Technology: Lecture Handbook in Routine Clinical
Chemistry/ Julius Mario. 2008 ed. 44 -54
Danny Donor ♥

THANKS FORLISTENING…
learn to love
the things you
hate
You're on the road to success when you realize that failure is only a detour.