Embed Size (px)
Citation preview

An Overview of Epidemiology, Etiology and
Classification of Lung Cancer
Presented byDr.Shah Ashiqur Rahman Ashiq
Choudhury Phase-A Resident,
Pulmonology,BSMMU

Background Lung cancer was once a very rare disease, so rare that
doctors took special notice when confronted with a case, thinking it a once-in-a-lifetime oddity.
Cigarettes were recognized as the cause of the epidemic in the 1940s and 1950s, with the confluence of studies from epidemiology, animal experiments, cellular pathology and chemical analytics.
As late as 1960 only one-third of all US doctors believed that the link of lung cancer with cigarettes had been established.

Sir Richard DollSir Richard Doll
• 1950 study linking 1950 study linking smoking to lung cancersmoking to lung cancer
• 1954: Doll and Hill 1954: Doll and Hill published “The Mortality published “The Mortality of Doctors and Their of Doctors and Their Smoking Habits” in BMJ Smoking Habits” in BMJ (lead to most M.D. giving (lead to most M.D. giving up smoking)up smoking)



Epidemiology: Global Scenario


Lung cancer is the most common visceral malignancy,
accounting for roughly one-third of all cancer deaths.
It is the most common cause of cancer-related death in both men and women.
More than 225,000 individuals was diagnosed with lung cancer and over 150,000 individuals died from the disease in the United States in 2013.
The incidence of lung cancer peaked among men in the late 1980s and has plateaued in women.


In the 40 countries comprising Europe, lung cancer accounts for 12 % of approximately 3.2 million new cancer cases and 19.9 % ( 342,000) of cancer related deaths.
Lung cancer is rapidly emerging as a major cause of mortality in the Middle East, Africa, and Asia as well.
Approximately 70,000 annual cancer-related deaths are currently attributed to lung cancer in Japan. More than 130,000 lung cancer deaths occur annually in China.

• The incidence of lung cancer varies considerably among different ethnic populations throughout the world.
• Among men, African Americans had the highest incidence of lung cancer risk ( approximately 7.5 % ) , where as Swedes had the lowest cumulative risk (approximately 2 % ) .
• Among women, cumulative lung cancer risk was highest
in African Americans (approximately 3 .5 % ) , whereas French and Korean women had very low cumulative risks (approximately 1% ) .

Epidemiology: Bangladesh Scenario

Bangladesh is still lacking a national cancer registry.
Cancer is the sixth leading cause of death in Bangladesh (BBS, 2008).
According to the cancer registry report of National Institute of Cancer Research Hospital (NICRH) with the collaboration of WHO and Bangladesh Government, Lung cancer is the most common cause of cancer in male and 4th common cause of cancer in female.
A recent WHO study has been estimated that there are 196,000 lung cancer cases in Bangladesh among those aged 30 years or above.

Etiology


Smoking

Smoking About 80% of lung cancer occur in smokers or those who
stopped recently.
The risk becomes 60 times greater among habitual heavy smokers compared with non smokers.
Although cessation of smoking decreases the lung cancer risk over time but it may never return to the baseline levels.
Passive smoking increases the risk of lung cancer development approximately twice than that of non-smokers.


Not all person exposed to tobacco smoke develop lung cancer and this is because the mutagenic effect of carcinogens in smoke is modified by genetic variants.
Specific and highly polymorphic p-450 monooxygenase
enzyme has an increased capacity to activate the procarcinogens in smoke.
Similarly, smokers whose peripheral blood lymphocyte show more numerous chromosomal breakage after exposure to tobacco related carcinogens have 10 fold higher risk of developing lung cancer than others.

Basal cell hyperplasiaǁ
Squamous metaplasiaǁ
Squamous dysplasiaǁ
Carcinoma in situǁ
Invasive carcinoma

Second hand smoke or environmental tobacco smoke contains numerous human carcinogens for which there is no safety level.
It is estimated that about 3000 non-smoking adults die of lung cancer as a result of breathing second hand smoke
Cigars and pipe smoking also increase the risk but much less than smoking cigarettes.

Environmental Carcinogens
Asbestos
Radon
Radon is a naturally occurring, radioactive gas.
It is odourless and tasteless.
Formed from the radioactive decay of uranium.
Underground miners.

Arsenic (naturally)
inorganicorganic (carcinogen)
Insecticides, weed killers, rat poison, Fungicides,
wood preservatives, Paints, leather industry.
Chromium
• Natural element, odourless and tasteless.
• Chromium (VI) or hexavalent chromium is
carcinogenic.
• Chrome plating, Stainless steel welding

Nickel
Polycyclic Aromatic Hydrocarbons (PAHs)
A group of over 100 different chemicals that are formed during the incomplete burning of coal,oil, gas, garbage.
Diesel fuel exhaust is a prevalent source of PAHs.
Some PAHs are used to make medicines, dyes, plastics, and pesticides.

Other Environmental Lung Carcinogens
bis(chloromethyl)ether,chloromethyl methyl ether, ionizing radiation (x-rays), gamma radiation, mustard gas, tars, mineral oils,vinyl chloride.
Suspected lung carcinogens include acrylonitrile,
cadmium, beryllium,
lead,ferric oxide dust.

Lung cancer itself is a risk factor for a 2nd lung cancer.
Other Lung diseases like scars( due to TB, fibrosis; specially idiopathic pulmonary fibrosis) and Chronic Obstructive Pulmonary Disease can increase the risk of lung cancer

Genetic Predisposition “Driver” mutation plays a key role in neoplastic
transformation of pulmonary epithelial cells.
Some of these genetic changes associated with cancer can be found in the “benign” bronchial epithelium of smokers without lung cancers.
This suggests that large areas of respiratory mucosa are mutagenized by exposure to the carcinogens of tobacco.
This phenomenon is called “field effect”

Genetic Predisposition
• Oncogenes:• activation of oncogenes or inactivation
of tumor suppressor genes.–Proto-oncogenes are believed to turn
into oncogenes when exposed to particular carcinogens.
–Mutations in the K-ras proto-oncogene are responsible for 10–30% of lung adenocarcinoma.

• Chromosomal damage:– Chromosomal damage can lead to loss of
heterozygosity– This can cause inactivation of tumor suppressor
genes.– Damage to chromosomes 3p, 5q, 13q, and 17p
are particularly common in small-cell lung carcinoma.
– The p53 tumor suppressor gene, located on chromosome 17p, is affected in 60-75% of cases.

• Epidermal Growth Factor Receptor (EGFR)
– EGFR regulates cell proliferation, apoptosis, angiogenesis, and tumor invasion
– Mutations and amplification of EGFR can lead to cancerous growth, esp. non-small-cell lung cancer (basis for the treatment with EGFR-Inhibitors)

• Genetic polymorphisms
– People with genetic polymorphisms are more likely to develop lung cancer after exposure to carcinogens.
– These include polymorphisms in genes coding for» interleukin-1, » cytochrome P450, » apoptosis promoters such as caspase-8,and » DNA repair molecules such as XRCC1


Molecular genetic features of some distinctive Lung
carcinomas

Squamous Cell Carcinoma

Squamous Cell Carcinoma Highly associated with smoking and harbors diverse
genetic aberrations including chromosomal deletions involving the tumour suppressor loci.
Chromosomal deletions in 3p,9p(site of CDKN2A gene) and 17p( site of the TP53 gene) are the early events in tumour evolution.
Squamous cell carcinoma shows highest frequency of
TP53 mutations of all histologic types of lung carcinoma.

Squamous Cell Carcinoma (contd.)
Loss of expression of Retinoblastoma(RB) tumour suppressor gene is identified by immunohistochemistry in 15% of squamous cell carcinoma.
The CDKN2A is inactivated and its protein product p16,is
lost in 65% of tumours.
It has been recently recognized that many squamous cell carcinomas have amplifications of FGFR1, a gene encoding the fibroblast growth factor receptor tyrosine kinase.

Small Cell Carcinoma

Small Cell Carcinoma Small cell carcinoma has the strongest association with
smoking and despite its diverse histological features shares many molecular features with squamous cell carcinoma.
Most common genetic aberrations include loss of function of TP53( 75%-90% of tumours), RB( close to 100% of the tumours) and chromosome 3p deletions.
Also common in amplification of MYC gene family.

Adenocarcinoma

Adenocarcinoma Adenocarcinoma is marked by oncogenic gain-of-
function mutations involving the components of growth factor rececptor signalling pathways.
These include gain-of-function mutations in multiple genes encoding receptor tyrosine kinase such as: EGFR,ALK,ROS,MET and RET which are all also mutated in the other forms of cancer.
Tumours without tyrosine kinase gene mutations often have mutations in the KRAS gene.


Lung Cancers in Never Smokers
The WHO estimates that 25% of lung cancer worldwide occurs in never smokers.
This cancer commonly occurs in women and mostly are adenocarcinomas.
Cancers in non-smokers are more likely to have EGFR mutations and almost never have KRAS mutations.
TP53 mutations are not uncommon but occur less frequently than in smoking related cases.

Classification of Malignant Lung Tumours

Classification of Malignant Lung Tumours
Importance of Classification: Consistency in patient treatment
Provision of basis for epidemiologic and biological studies.
On the basis of origin, lung carcinoma can be divided into:
A. Primary Lung Tumour: Arises from lung itself B. Secondary Lung Tumour: Arises from elsewhere.

Histologic Classification of Lung Carcinoma in Resected Specimens 1) Pre-invasive leisonsa) squamous dysplasia b) atypical adenomatous
hyperplasia c) adenocarcinoma in situ d) diffuse idiopathic pulmonary neuro-endocrine cell hyperplasia
2) Squamous cell carcinomaa) Papillary b) small cell c) clear cell d) basaloid3) Small cell carcinoma Combined small cell carcinoma

4) Adenocarcinomaa) minimally invasive b) invasive adenocarcinoma5) Large cell carcinomaa) large cell neuro-endocrine carcinoma b)
basaloid c) lympho-epithelioma like carcinoma d) clear cell
e) large cell carcinoma with rhabdoid prototype6) Adenosquamous carcinoma

7) Sarcomatoid Carcinomasa) Pleomorphic b) spindle cell c) giant cell
d) carcinosarcoma e) plumonary blastoma
8) Carcinoid Tumours9)Carcinoma of Salivary gland typesa) Mucoepidermoid b) adenoid cystic c)
epimyothelial carcinoma

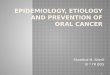
The relative proportions of major histopathological categories
0%5%
10%15%20%25%30%35%40%
1stQtr
AdenocarcinomaSquamous cellcarcinomaSmall cellcarcinomaLarge cellcarcinomaOthers




THANK YOU