Embed Size (px)
Citation preview
By
Ahmad Saber Soliman
Ass. Lecturer of gynecology and obstetrics
Management of Endometrial Hyperplasia
Endometrial hyperplasia is :
1. proliferation of endometrial glands that may progress to or coexist with endometrial cancer.
2. Results from chronic estrogen stimulation unopposed by progesterone.
3. Treated with hysterectomy or progestin therapy.
4. Treatment is guided by risk of endometrial carcinoma.
The classification system that is used most commonly is
W H O.
CLASSIFICATION
Simple without atypia
Complex without atypia
Simple with atypia
Complex with atypia
The terms simple or complex refer to the glandular/stromal architectural pattern. Atypia refers to nuclear atypia.
The endometrial intraepithelial system is another classification system.
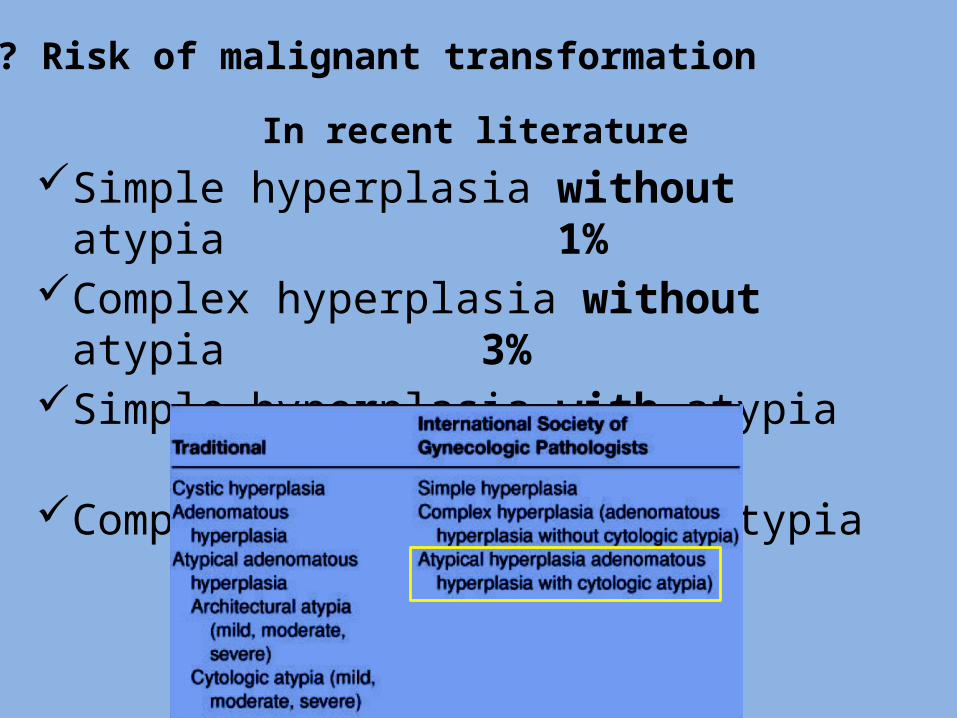
In recent literature Simple hyperplasia without atypia 1%Complex hyperplasia without atypia 3%Simple hyperplasia with atypia 8%Complex hyperplasia with atypia 40%
Risk of malignant transformation ???
Management of hyperplasia with atypia
Hysterectomy is the treatment of choice for women with endometrial hyperplasia with atypia who are not planning future pregnancy.
Progestin therapy is an option for women who wish to preserve fertility or who cannot tolerate surgery.
high risk endometrial cancer more than 40 % . concurrent foci of endometrial cancer (17 to 52
percent) how to exclude
based upon data from a literature review of six studies that included 511 women.
Why hysterctomy ?
The best type is total extrafascial hysterectomy.
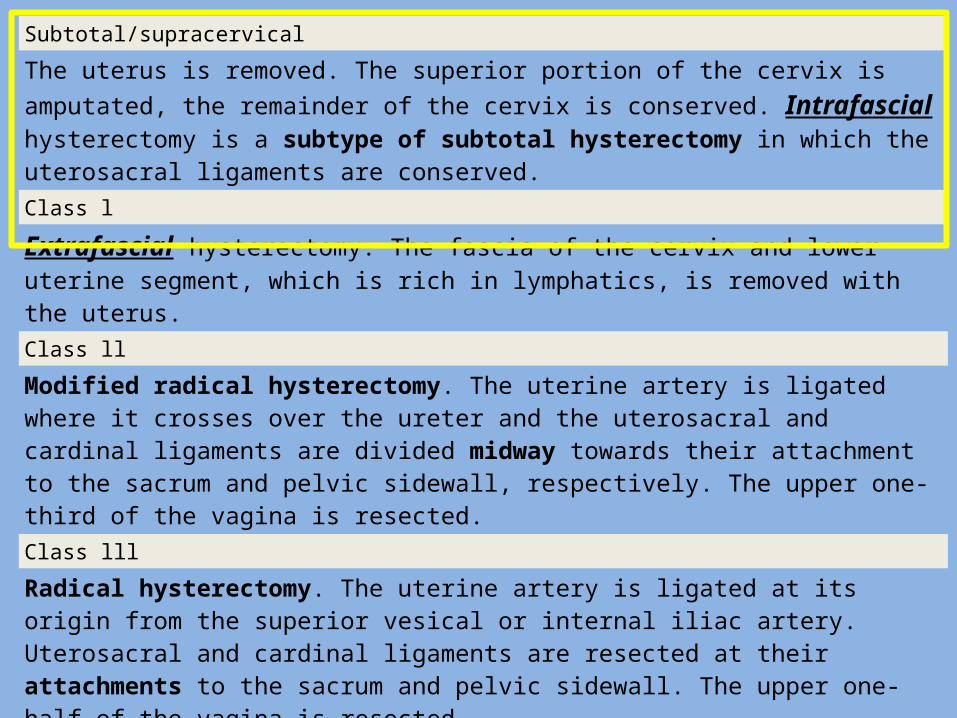
Subtotal/supracervical
The uterus is removed. The superior portion of the cervix is amputated, the remainder of the cervix is conserved. Intrafascial hysterectomy is a subtype of subtotal hysterectomy in which the uterosacral ligaments are conserved.
Class l
Extrafascial hysterectomy. The fascia of the cervix and lower uterine segment, which is rich in lymphatics, is removed with the uterus. Class ll
Modified radical hysterectomy. The uterine artery is ligated where it crosses over the ureter and the uterosacral and cardinal ligaments are divided midway towards their attachment to the sacrum and pelvic sidewall, respectively. The upper one-third of the vagina is resected.
Class lll
Radical hysterectomy. The uterine artery is ligated at its origin from the superior vesical or internal iliac artery. Uterosacral and cardinal ligaments are resected at their attachments to the sacrum and pelvic sidewall. The upper one-half of the vagina is resected.
Class lV
Radical hysterectomy.The ureter is completely dissected from the vesicouterine ligament, the superior vesical artery is sacrificed, and three-fourths of the vagina is resected.
Class V
Radical hysterectomy. There is additional resection of a portion of the bladder or distal ureter with ureteral reimplantation into the bladder.
What about subtotal hysterectomy??Supracervical hysterectomy is not a valid option for these patients, since the potential for local extension of the endometrial neoplasia into the cervix outweighs any benefits of this surgical approach.
systematic review : total versus subtotal hysterectomy for benign conditions
1. no difference in the rates of incontinence, constipation or measures of sexual function (sexual satisfaction, dyspareunia).
2. Length of surgery and amount of blood lost during surgery were significantly reduced during subtotal hysterectomy compared with total hysterectomy, but there was no difference in the likelihood of transfusion.
3. Febrile morbidity was less likely in total hystectomy and cyclical vaginal bleeding one year after surgery was more likely after subtotal hysterectomy.
4. There was no difference in the rates of other complications, recovery from surgery, or readmission rates.
Can we exclude endometrial carcinoma intraoperative?
Unfortunately, there is no reliable method of excluding endometrial malignancy
intraoperatively.
Gross examination and frozen section of the uterus should be performed, but these often fail
to detect endometrial cancer foci .
What about risk reducing hysterectomy?
Cases of lynch syndrome MLH MSH genes mutations or cowden syndrome PTEN mutation
What is the fate of the ovary?
RCOG recommends BSO ≥45 years
Disadvantage of routinely performing BSO in women with atypical hyperplasia is that the procedure will be unnecessary in about 50 to 80 percent of women who do not have endometrial cancer.
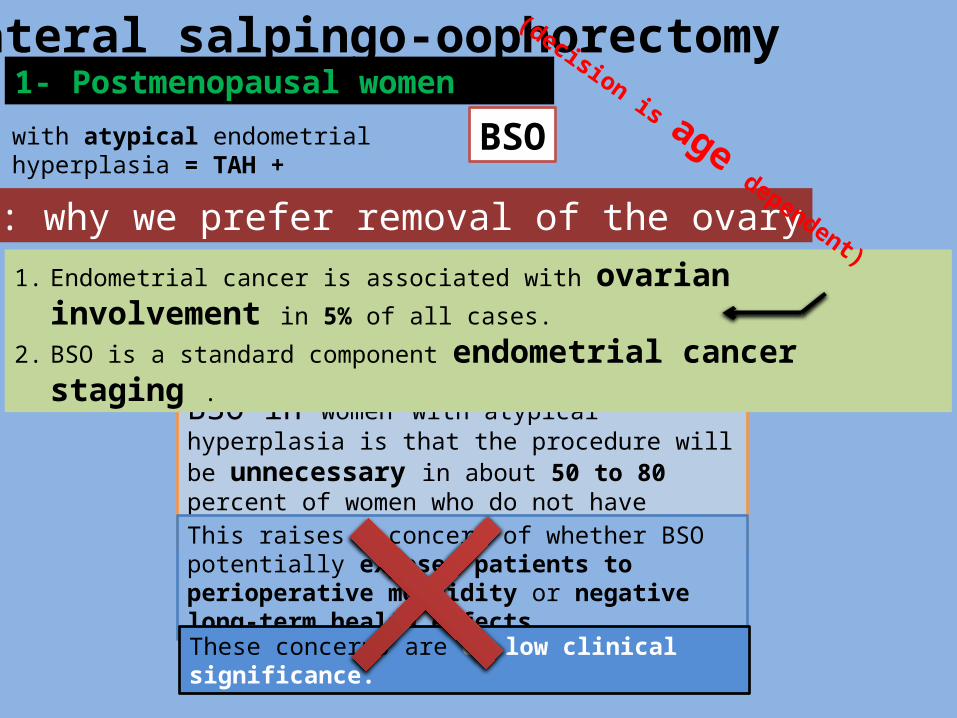
Bilateral salpingo-oophorectomy1- Postmenopausal women
with atypical endometrial hyperplasia = TAH +
Q: why we prefer removal of the ovary? 1. Endometrial cancer is associated with ovarian involvement in 5%
of all cases.
2. BSO is a standard component endometrial cancer staging .
This raises a concern of whether BSO potentially exposes patients to perioperative morbidity or negative long-term health effects. These concerns are of low clinical significance.
(
decision is age dependent
)
BSO
What evidence says in BSO???
There are no standard recommendations regarding conserving or removing ovaries when a hysterectomy is performed for treatment of atypical endometrial hyperplasia.
Observational studies
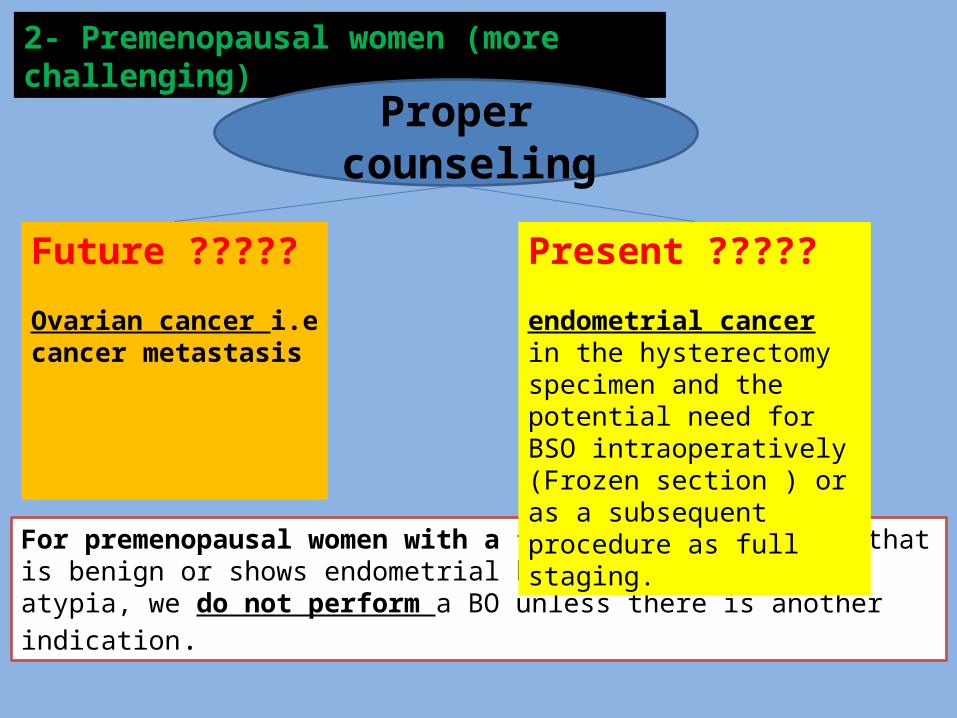
2- Premenopausal women (more challenging)
For premenopausal women with a frozen section result that is benign or shows endometrial hyperplasia without atypia, we do not perform a BO unless there is another indication.
Proper counseling
Future ?????
Ovarian cancer i.ecancer metastasis
Present ?????
endometrial cancer in the hysterectomy specimen and the potential need for BSO intraoperatively (Frozen section ) or as a subsequent procedure as full staging.
Compared with postmenopausal women, the risk of a synchronous primary or metastatic disease involving the ovary in premenopausal patients with endometrial cancer is significantly higher (25 percent) . Walsh et al; Obstet Gynecol 2005
Remove Do not Remove
No further surveillance related to endometrial hyperplasia is necessary after hysterectomy.
HRT, if there are no contraindications.
This is based upon findings that post-treatment estrogen therapy is not associated with recurrence in women with endometrial cancer.
Outcome and follow-up
What about cytology screening for atypical cells ( cancer cervix
screening) programs?
Hormonal treatment
Treatment with other agents or conservative surgery is not standard clinical practice.
Women who wish to preserve fertility
Women who are not surgical candidates

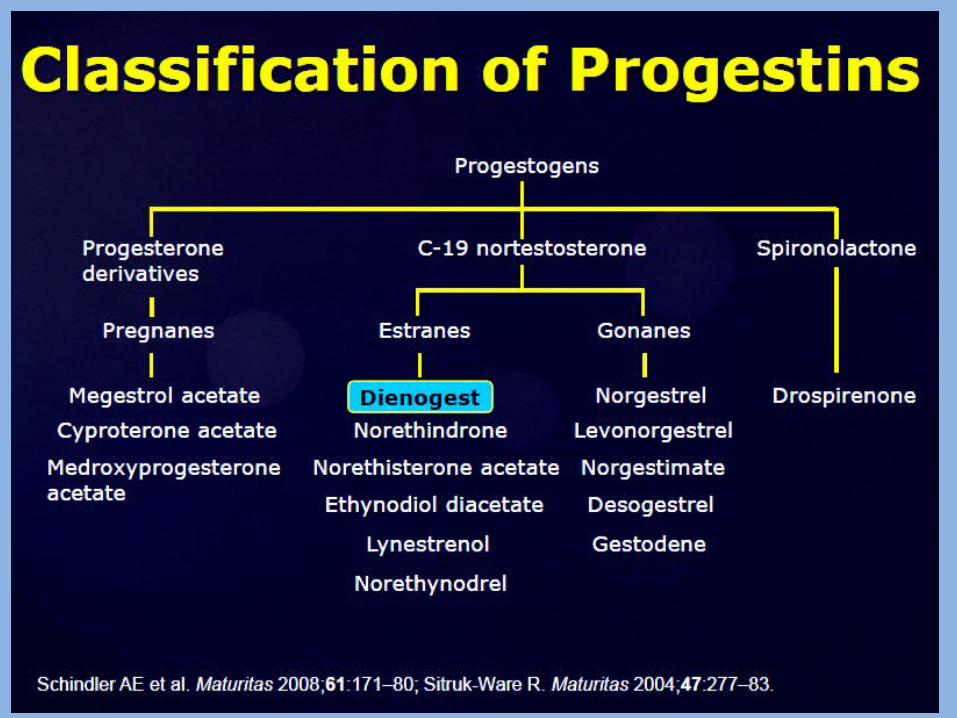
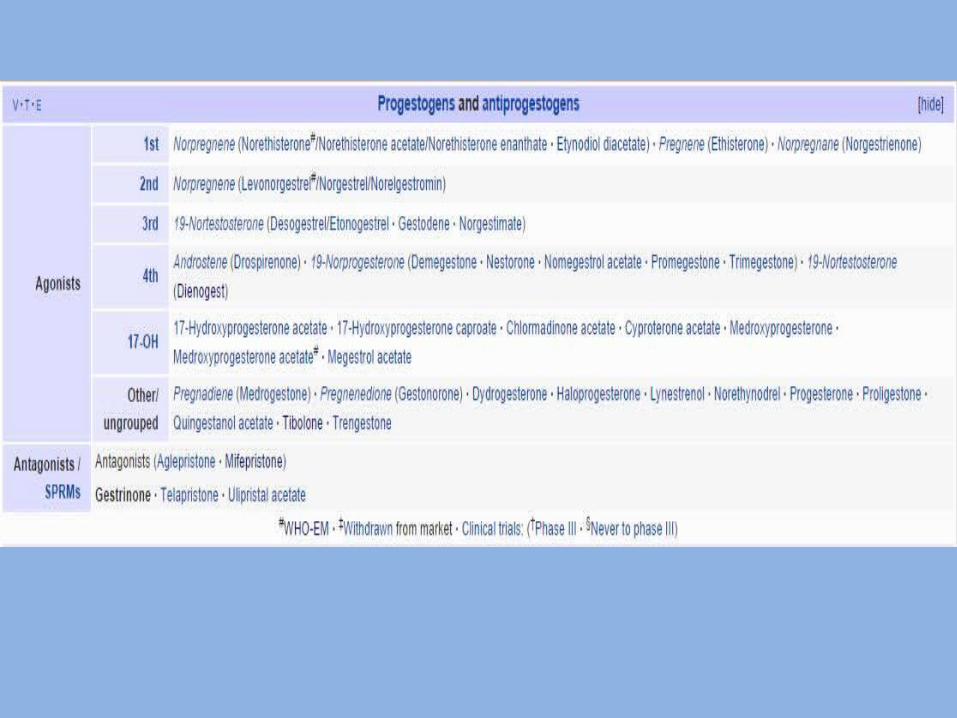
Progestin therapy
Clinical pearls before initiating progestin therapy
The type of progestin, dose, and duration of treatment for endometrial hyperplasia varies widely.
treatment options depending upon the presence or absence of atypia and desire for fertility.
Unlike atypia, whether the hyperplasia is described as
having simple or complex architecture does not play a role in management
If regression is achieved on progestins, recurrences can be prevented by administering preventive therapy. ?????? progestin
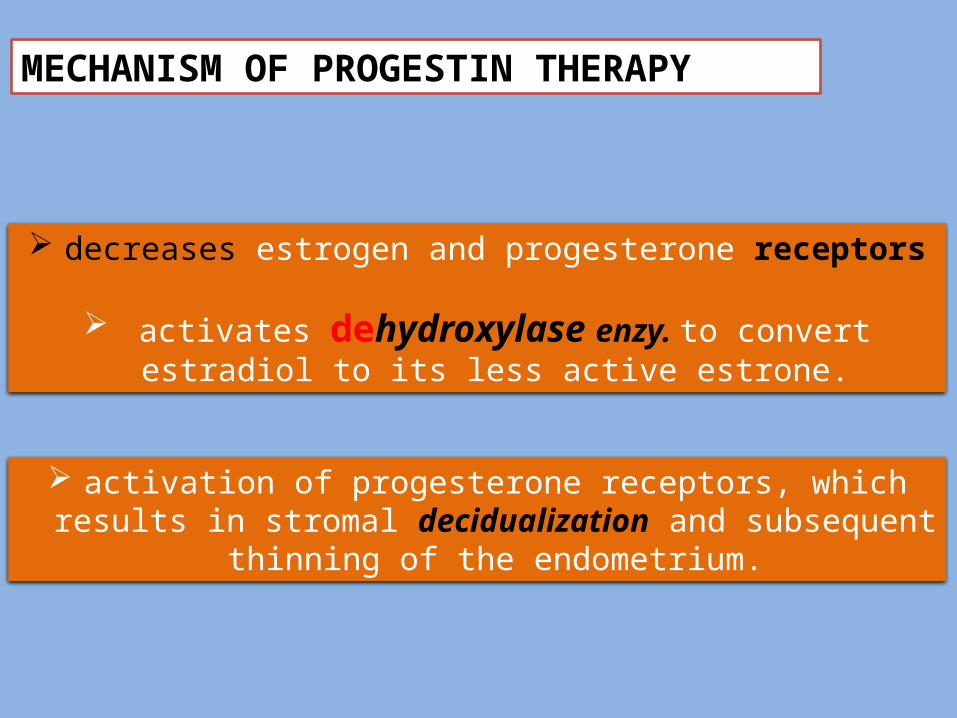
MECHANISM OF PROGESTIN THERAPY
activation of progesterone receptors, which results in stromal decidualization and subsequent thinning of
the endometrium.
decreases estrogen and progesterone receptors
activates dehydroxylase enzy. to convert estradiol to its less active estrone.
Other options for progestin therapy include: MPA (oral) 10 to 20 mg daily OR cyclic 12 to 14 days/month Depot medroxyprogesterone (intramuscular) 150 mg every three
months Micronized progesterone (vaginal) 100 to 200 mg daily or
cyclic 12 to 14 days per month Levonorgestrel -intrauterine device, duration of use one to five
years
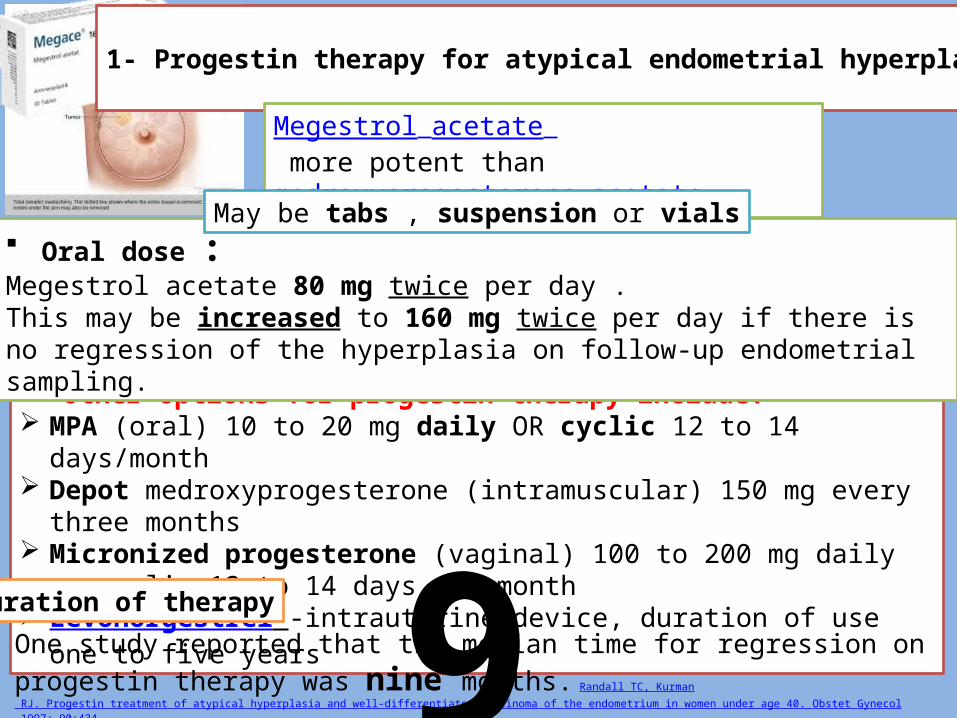
1- Progestin therapy for atypical endometrial hyperplasia
Megestrol acetate more potent than medroxyprogesterone acetate .
Oral dose :Megestrol acetate 80 mg twice per day . This may be increased to 160 mg twice per day if there is no regression of the hyperplasia on follow-up endometrial sampling.
May be tabs , suspension or vials
One study reported that the median time for regression on progestin therapy was nine months. Randall TC, Kurman
RJ. Progestin treatment of atypical hyperplasia and well-differentiated carcinoma of the endometrium in women under age 40. Obstet Gynecol 1997; 90:434.
Duration of therapy 9
Can hormonal treatment succeed in regressing atypical hyperplastic
cells??
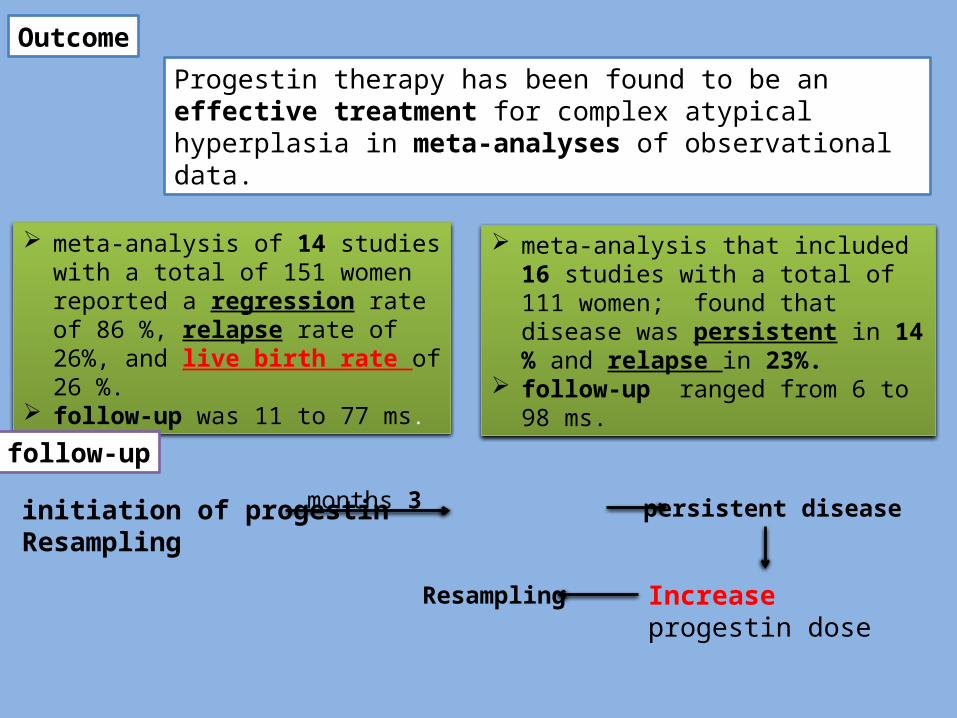
meta-analysis of 14 studies with a total of 151 women reported a regression rate of 86 %, relapse rate of 26%, and live birth rate of 26 %.
follow-up was 11 to 77 ms.
Outcome
follow-up
initiation of progestin Resampling
Progestin therapy has been found to be an effective treatment for complex atypical hyperplasia in meta-analyses of observational data.
meta-analysis that included 16 studies with a total of 111 women; found that disease was persistent in 14 % and relapse in 23%.
follow-up ranged from 6 to 98 ms.
3 months persistent disease
Increase progestin dose
Resampling
When to do endometrial sampling ??
Wait for withdrawal bleeding or not
Some experts advise waiting for a withdrawal bleed before sampling, while others sample the endometrium while the patient is on progestin
therapy
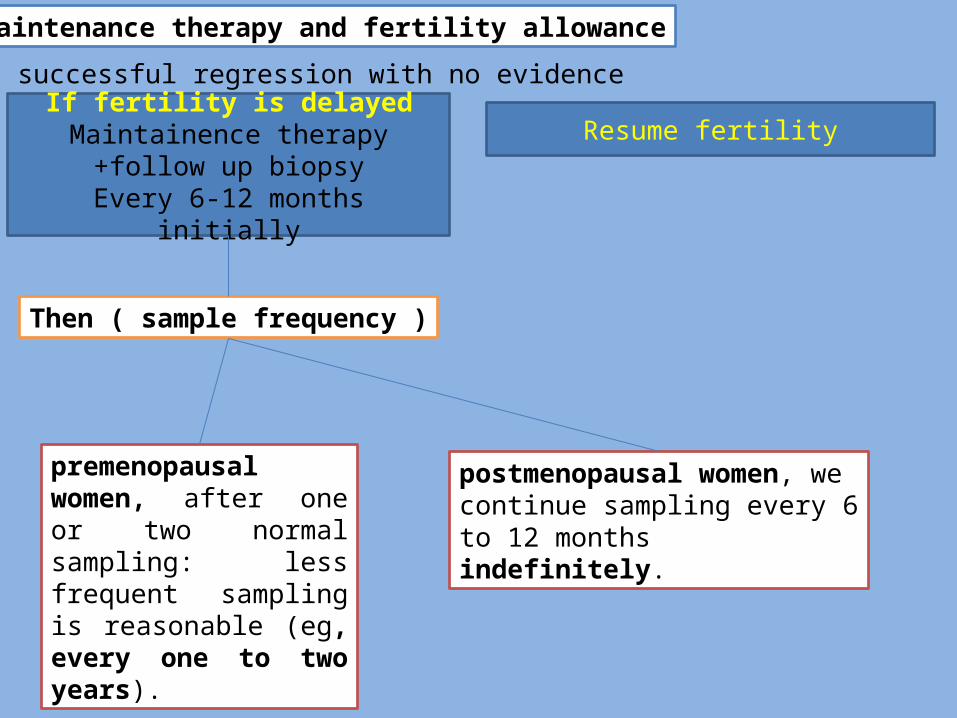
successful regression with no evidence of hyperplasia,
Maintenance therapy and fertility allowance :
postmenopausal women, we continue sampling every 6 to 12 months indefinitely.
Resume fertilityIf fertility is delayedMaintainence therapy +follow
up biopsyEvery 6-12 months initially
premenopausal women, after one or two normal sampling: less frequent sampling is reasonable (eg, every one to two years).
Then ( sample frequency )
persistent disease after nine months was predictive of treatment
failure .
When to say .. FAILED HORMONAL TREATMENT
Hysterectomy
2- HYPERPLASIA WITHOUT ATYPIA • low risk of malignant transformation (1 to 3 percent)
Goal of treatment
Prevent progression to
cancer
Control abnormal uterine
bleeding• Endometrial hyperplasia without atypia is usually treated with progestin therapy.
Medroxyprogesterone acetate (MPA) is the progestin that is typically usedDose : 10 mg daily
Duration: 3-6 months.
Regimen used: continuous dosing schedule more acceptable than a cyclic regimen because they do not have cyclic vaginal bleeding during treatmentcyclic regimen of MPA (eg, 10 mg daily for 12 to 14 days each month).
Micronized progesterone (100 to 200 mg)
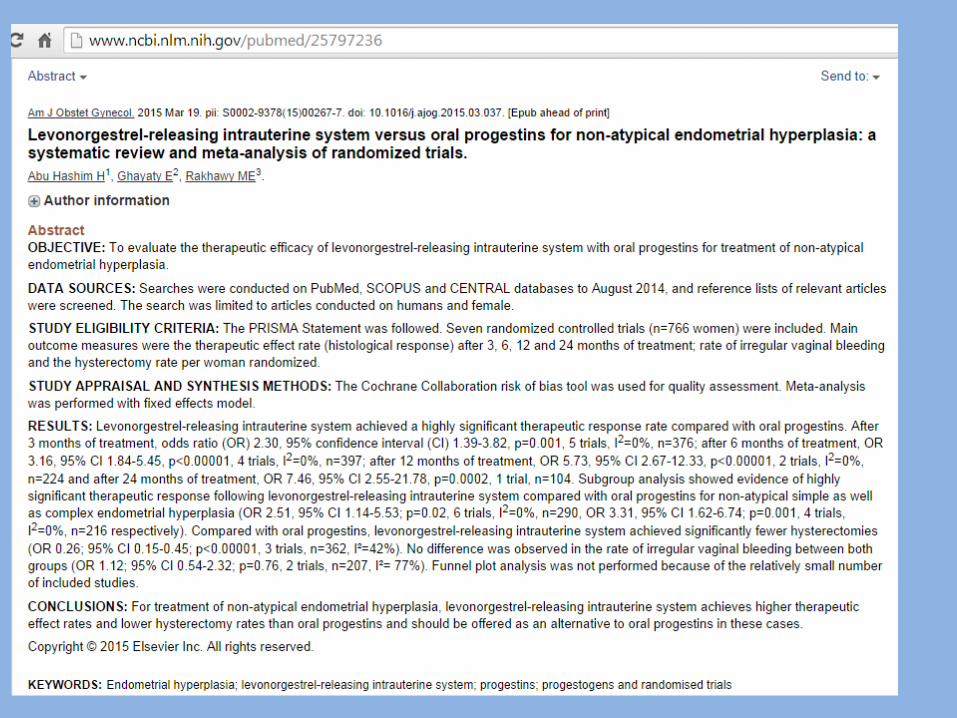
Levonorgestrel -releasing intrauterine device (LNG-IUD) –
Endometrial biopsy can be performed with an intrauterine device in place.
Estrogen-progestin contraceptives –
Ovulation induction – In reproductive-age women, this approach will result in formation of a corpus luteum and exposure to progestins.
This may be a good option for women with endometrial hyperplasia without atypia who desire pregnancy.
Regression was noted in up to 80% of cases simple hyperplasia without atypia . & up to 71% in cases of complex hyperplasia without atypia
After treatment, we suggest initiating preventive treatment if the patient has not resumed normal cyclic menstrual function. We rebiopsy if abnormal uterine bleeding recurs.
endometrial sampling : every three to six months. • If no regression the progestin dose may be increased or a
combination of a systemic progestin and the LNG-IUD may be used.
• If atypical hyperplasia or endometrial carcinoma develops, the patient should be treated as appropriate.
Outcome
Follow-up
preventive treatment
Alternative treatments for primary endometrial protection in women who cannot or prefer not to take an estrogen-progestin contraceptive include intermittent or continuous progestins. Intermittent therapy should be continued as long as chronic anovulation is present: Medroxyprogesterone acetate (5 to 10 mg) daily for 12 to 14 days
per month Norethindrone acetate (5 to 15 mg) daily for 12 to 14 days per
month Micronized progesterone in a vaginal cream (200 mg) daily for 12
to 14 days per month Depot medroxyprogesterone acetate (150 mg intramuscularly)
every three months LNG-IUD, which releases 15 to 20 mcg of levonorgestrel daily
Preventive therapy
There are no strong data supporting the use of one of these regimens over another. Choice of regimen therefore depends upon patient preference, based upon factors such as cost, convenience, and side effects.
Idea :.For women with chronic anovulation, such as with polycystic ovary syndrome, an estrogen-progestin contraceptive is often the best choice.
RCOG guide lines
• Management depends on many variables age, desire for fertility, symptoms
• Exclude : exogenous esrogen .and tumours• Ttt : continous progestin therapy for 3-6
months• Dose : premenopausal 5mg perimenopausal 10 mg Postmenopausal 20 mg or mirena• Rebiopsy only if AUB
Obese women should be encouraged to lose weight
reduction of estradiol and estrone production by adipocytes.
Other approaches under investigation
Hysteroscopic resection of endometrial hyperplasia was reported to be effective in 68 of 73 treated women, but the long term consequence of this treatment remains to be determined .
Danazol has also been used successfully but has significant side effects . In a series of postmenopausal women, danazol (400 mg per day for six months) caused complete regression in only 83 percent of patients, with 8 percent relapse within four months of discontinuing therapy .
Gonadotropin-releasing hormone (GnRH) agonists or antagonists may be given to produce a pseudomenopausal state. In one report, approximately 86 percent of women (mean age 46 years) had regression of hyperplasia without atypia to normal endometrium after six months of GnRH agonist treatment; however, this regimen was not effective in the three women with atypia .
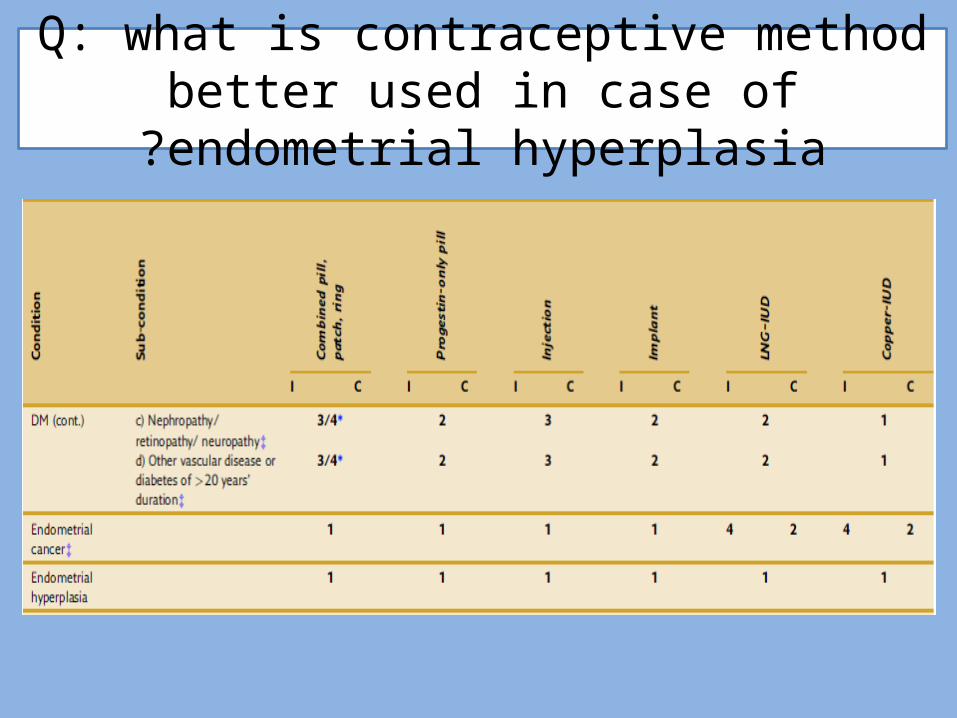
Q: what is contraceptive method better used in case of endometrial hyperplasia?
RECOMMENDATIONS • Hysterectomy is the treatment of choice for women with endometrial hyperplasia with
atypia who are not planning future pregnancy.
• For postmenopausal women with atypical hyperplasia, we suggest hysterectomy with concomitant bilateral salpingo-oophorectomy (BSO) rather than hysterectomy alone ( Grade 2C ). For premenopausal women undergoing treatment with hysterectomy, BSO is reasonable for those who value avoiding re-operation (in the event the final evaluation shows endometrial cancer) more than retaining their ovaries.
• Progestin therapy is an option for women with atypical endometrial hyperplasia who wish to preserve fertility or who cannot tolerate surgery. We treat these women with oral megestrol acetate 80 mg twice per day every day. This may be increased to 160 mg twice per day if there is no regression of the hyperplasia on follow-up endometrial sampling. Other progestin preparations may also be used.
• We suggest progestins rather than surgery for treatment of endometrial hyperplasia without atypia ( Grade 2C ). We treat these patients with medroxyprogesterone acetate 10 mg daily for at least 12 to 14 days each month for three to six months. Other progestin preparations may also be used.
thyroid dysfunction or mellitus diabetes and/or insulin resistance

Thanks
















![Endometrium presentation - Dr Wright[1] · Endometrial Hyperplasia Simple hyperplasia Complex hyperplasia (adenomatous) Simple atypical hyperplasia ... Progression of Hyperplasia](https://img.pdfslide.net/doc/110x75/5b8a421e7f8b9a50388bc13d/endometrium-presentation-dr-wright1-endometrial-hyperplasia-simple-hyperplasia.jpg)