Embed Size (px)
Citation preview
Marc Bourlière, MDGraham R. Foster, FRCP, PhD
Managing Cirrhotic HCV Patients: Whom to Treat, How to Treat
This program is supported by an educational grant from
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
About These Slides
Users are encouraged to use these slides in their own noncommercial presentations, but we ask that content and attribution not be changed. Users are asked to honor this intent
These slides may not be published or posted online without permission from Clinical Care Options (email [email protected])
DisclaimerThe materials published on the Clinical Care Options Web site reflect the views of the authors of the CCO material, not those of Clinical Care Options, LLC, the CME providers, or the companies providing educational grants. The materials may discuss uses and dosages for therapeutic products that have not been approved by the United States Food and Drug Administration. A qualified healthcare professional should be consulted before using any therapeutic product discussed. Readers should verify all information and data before treating patients or using any therapies described in these materials.
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
Disclosures
Marc Bourlière, MD, has disclosed that he has received consulting fees from Boehringer Ingelheim, Bristol-Myers Squibb, Gilead Sciences, Janssen, Merck, GlaxoSmithKline, and Roche.
Graham R. Foster, FRCP, PhD, has disclosed that he has received funds for research support from Idenix and Spring Bank; consulting fees from AbbVie, Boehringer Ingelheim, Bristol-Myers Squibb, Gilead Sciences, Idenix, Janssen, Merck, Novartis, and Roche; and fees for non-CME/CE services received directly from a commercial interest or their agents (eg, speaker bureaus) from AbbVie, Boehringer Ingelheim, Bristol-Myers Squibb, Gilead Sciences, Janssen, Merck, Novartis, and Roche
The following planners and managers, Laura Excell, ND, NP, MS, MA, LPC, NCC; Trace Hutchison, PharmD; Samantha Mattiucci, PharmD, CCMEP; Jan Schultz, RN, MSN, CCMEP; Patricia Staples, MSN, NP-C, CCRN; and Eric D. Peterson, EdM, FACEHP, hereby state that they or their spouse/life partner do not have any financial relationships or relationships to products or devices with any commercial interest related to the content of this activity of any amount during the past 12 months.
Which Cirrhotic Patients Should be Treated?
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
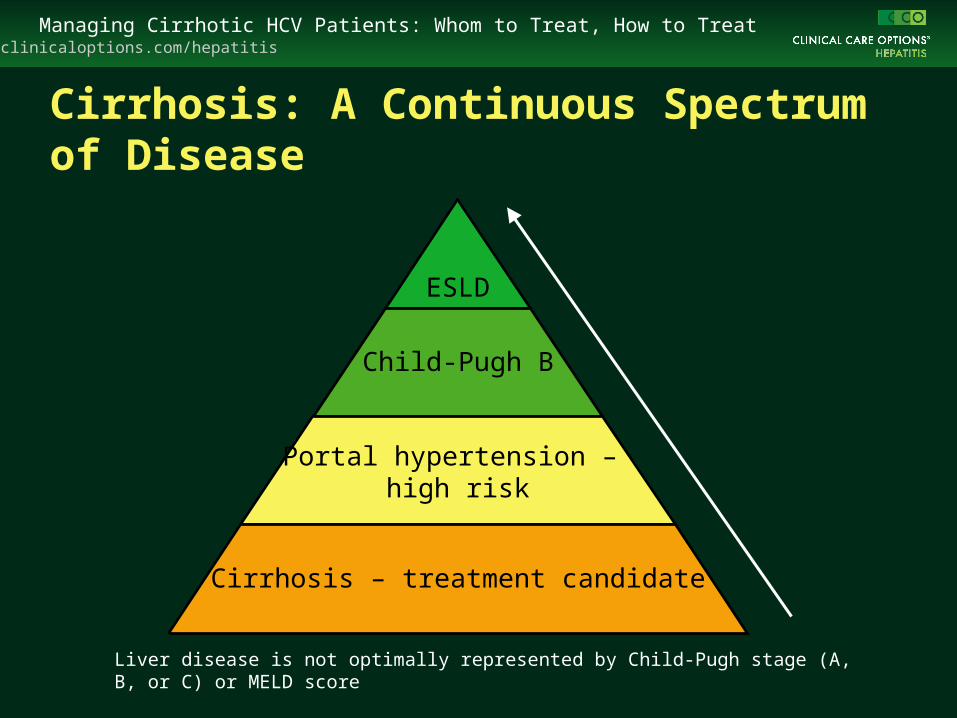
Cirrhosis: A Continuous Spectrum of Disease
ESLD
Child-Pugh B
Portal hypertension – high risk
Cirrhosis – treatment candidate
Liver disease is not optimally represented by Child-Pugh stage (A, B, or C) or MELD score
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
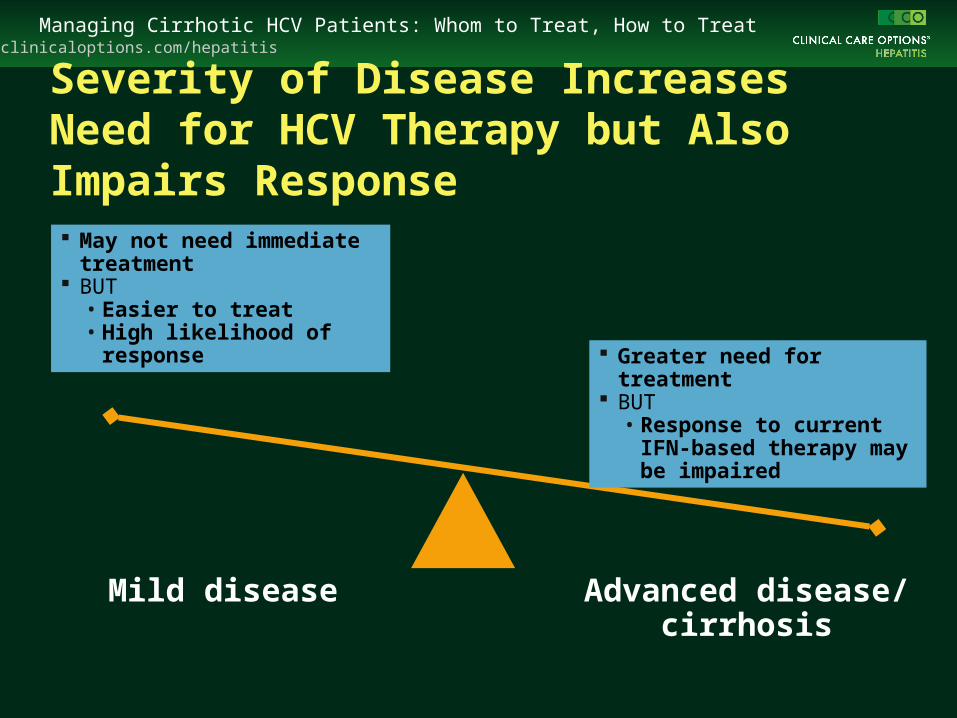
Severity of Disease Increases Need for HCV Therapy but Also Impairs Response
May not need immediate treatment
BUT • Easier to treat• High likelihood of response
Advanced disease/ cirrhosis
Mild disease
Greater need for treatment BUT
• Response to current IFN-based therapy may be impaired
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
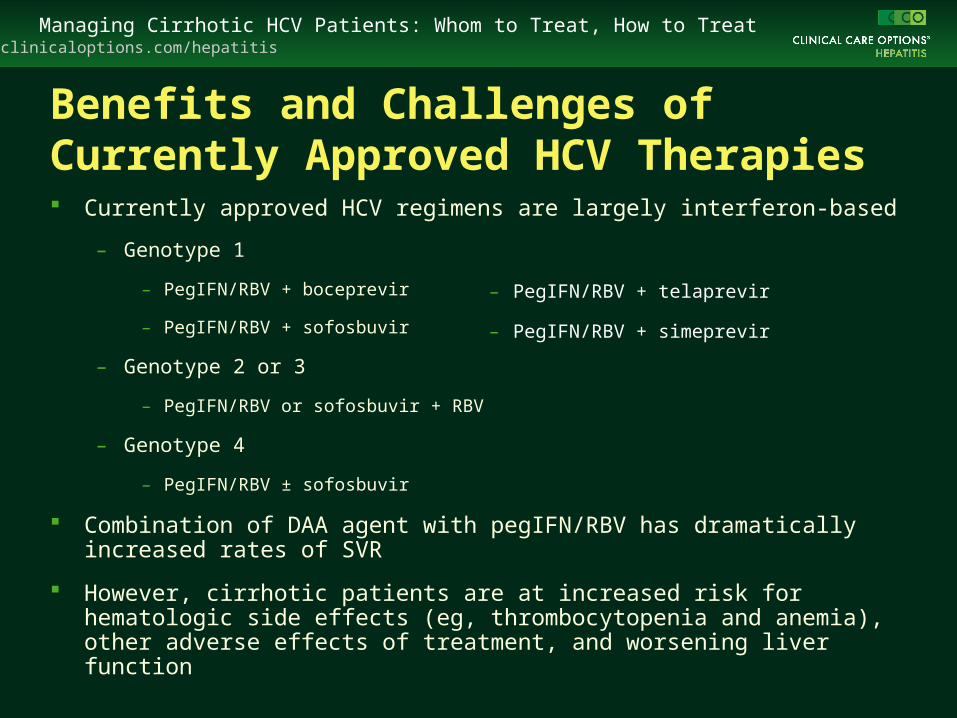
Benefits and Challenges of Currently Approved HCV Therapies Currently approved HCV regimens are largely interferon-based
– Genotype 1
– PegIFN/RBV + boceprevir
– PegIFN/RBV + sofosbuvir
– Genotype 2 or 3
– PegIFN/RBV or sofosbuvir + RBV
– Genotype 4
– PegIFN/RBV ± sofosbuvir
Combination of DAA agent with pegIFN/RBV has dramatically increased rates of SVR
However, cirrhotic patients are at increased risk for hematologic side effects (eg, thrombocytopenia and anemia), other adverse effects of treatment, and worsening liver function
– PegIFN/RBV + telaprevir
– PegIFN/RBV + simeprevir
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
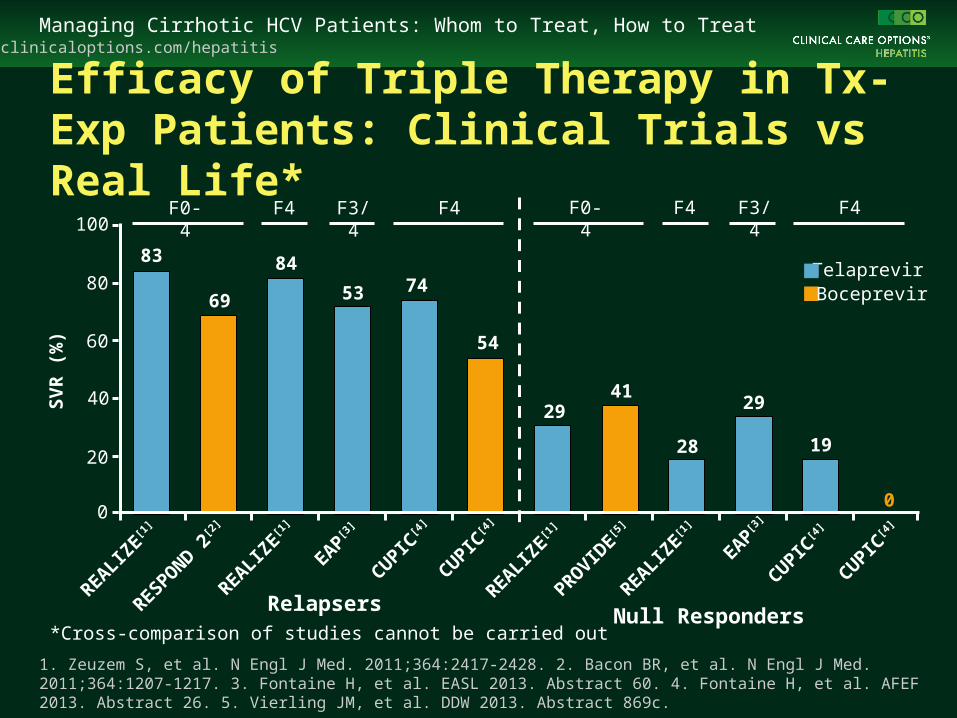
Efficacy of Triple Therapy in Tx-Exp Patients: Clinical Trials vs Real Life*
1. Zeuzem S, et al. N Engl J Med. 2011;364:2417-2428. 2. Bacon BR, et al. N Engl J Med. 2011;364:1207-1217. 3. Fontaine H, et al. EASL 2013. Abstract 60. 4. Fontaine H, et al. AFEF 2013. Abstract 26. 5. Vierling JM, et al. DDW 2013. Abstract 869c.
RelapsersREALIZ
E[1
]
EAP[3
]
REALIZE[1
]
CUPIC[4
]
CUPIC[4
]
RESPOND 2[2
]
Null RespondersREALIZ
E[1
]
EAP[3
]
REALIZE[1
]
CUPIC[4
]
CUPIC[4
]
PROVIDE[5
]
SV
R (
%)
Telaprevir
F0-4 F4 F3/4 F4 F0-4 F4 F3/4 F4
*Cross-comparison of studies cannot be carried out
100
80
60
40
20
0
Boceprevir
83
69
84
54
7453
2941
28
29
19
0
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
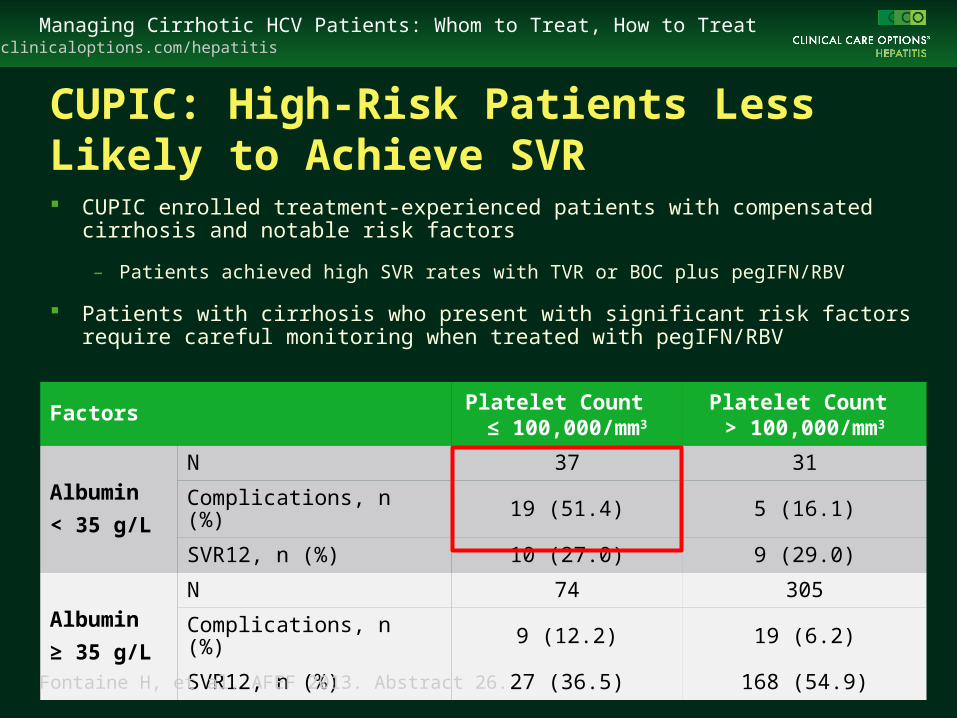
CUPIC: High-Risk Patients Less Likely to Achieve SVR CUPIC enrolled treatment-experienced patients with compensated cirrhosis
and notable risk factors
– Patients achieved high SVR rates with TVR or BOC plus pegIFN/RBV
Patients with cirrhosis who present with significant risk factors require careful monitoring when treated with pegIFN/RBV
Factors Platelet Count ≤ 100,000/mm3
Platelet Count > 100,000/mm3
Albumin
< 35 g/L
N 37 31
Complications, n (%) 19 (51.4) 5 (16.1)
SVR12, n (%) 10 (27.0) 9 (29.0)
Albumin
≥ 35 g/L
N 74 305
Complications, n (%) 9 (12.2) 19 (6.2)
SVR12, n (%) 27 (36.5) 168 (54.9)
Fontaine H, et al. AFEF 2013. Abstract 26.
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
HCV Decompensated Cirrhosis: Treatment With PegIFN/RBV Most in need of treatment (5-yr survival rate: 50%)
SVR rates ranged:
– 7% to 16% in genotypes 1-4[1,2]
– 44% to 57% in genotypes 2/3 [1,2]
Treatment limitation
– Higher risk of infection and deaths related to infection[1]
– More frequent adverse effects in Child-Pugh C (MELD > 18)[3]
Treatment benefit
– Lower rate of decompensation during follow-up[1,4]
– Reduced mortality in responders[1,4]
1. Iacobellis A, et al. J Hepatol. 2007;46:206-212. 2. Iacobellis A, et al. Aliment Pharmacol Ther. 2009;27:1081-1085. 3. Forns X, et al. J Hepatol. 2003;39:389-396. 4. Fattovich G, et al. Gastroenterology. 1997;112:463-472.
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
100
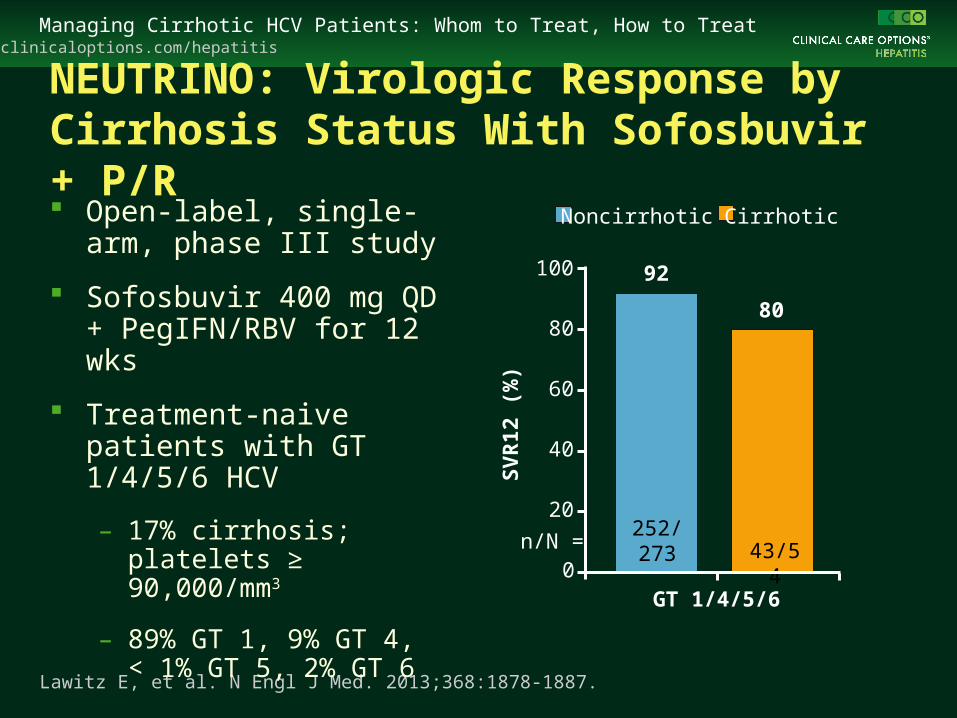
NEUTRINO: Virologic Response by Cirrhosis Status With Sofosbuvir + P/R
Lawitz E, et al. N Engl J Med. 2013;368:1878-1887.
Open-label, single-arm, phase III study
Sofosbuvir 400 mg QD + PegIFN/RBV for 12 wks
Treatment-naive patients with GT 1/4/5/6 HCV
– 17% cirrhosis; platelets ≥ 90,000/mm3
– 89% GT 1, 9% GT 4, < 1% GT 5, 2% GT 6
SV
R12
(%
)
92
80
252/273 43/54
80
60
40
20
0n/N =
GT 1/4/5/6
CirrhoticNoncirrhotic
clinicaloptions.com/hepatitisHCV Phase III Studies and Approved Agents
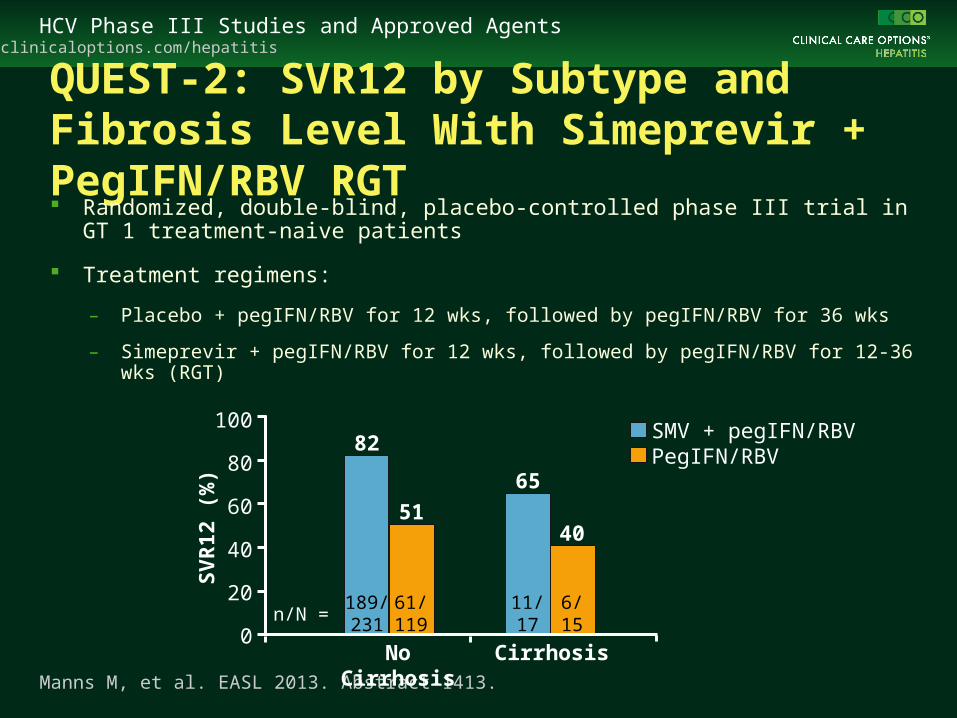
QUEST-2: SVR12 by Subtype and Fibrosis Level With Simeprevir + PegIFN/RBV RGT Randomized, double-blind, placebo-controlled phase III trial in GT 1 treatment-
naive patients
Treatment regimens:
– Placebo + pegIFN/RBV for 12 wks, followed by pegIFN/RBV for 36 wks
– Simeprevir + pegIFN/RBV for 12 wks, followed by pegIFN/RBV for 12-36 wks (RGT)
Manns M, et al. EASL 2013. Abstract 1413.
No Cirrhosis Cirrhosis
SMV + pegIFN/RBVPegIFN/RBV
189/231
61/119
11/17
6/15
n/N =
100
80
60
40
20
0
SV
R12
(%
)
82
65
5140
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
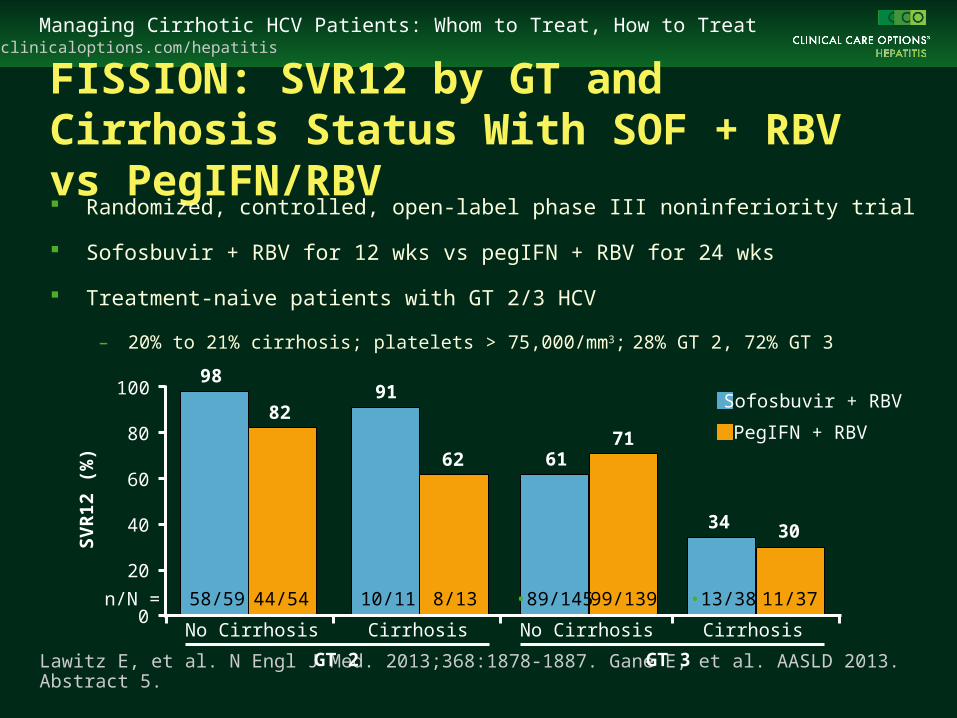
FISSION: SVR12 by GT and Cirrhosis Status With SOF + RBV vs PegIFN/RBV Randomized, controlled, open-label phase III noninferiority trial
Sofosbuvir + RBV for 12 wks vs pegIFN + RBV for 24 wks
Treatment-naive patients with GT 2/3 HCV
– 20% to 21% cirrhosis; platelets > 75,000/mm3; 28% GT 2, 72% GT 3
Lawitz E, et al. N Engl J Med. 2013;368:1878-1887. Gane E, et al. AASLD 2013. Abstract 5. GT 2 GT 3
SV
R12
(%
)
No Cirrhosis No CirrhosisCirrhosis Cirrhosis
58/59 44/54 10/11 8/13 •89/145 99/139 •13/38 11/37n/N =
100
80
60
40
20
0
98
8291
62 6171
34 30
Sofosbuvir + RBV
PegIFN + RBV
clinicaloptions.com/hepatitisAASLD 2013: HCV Investigational Agents
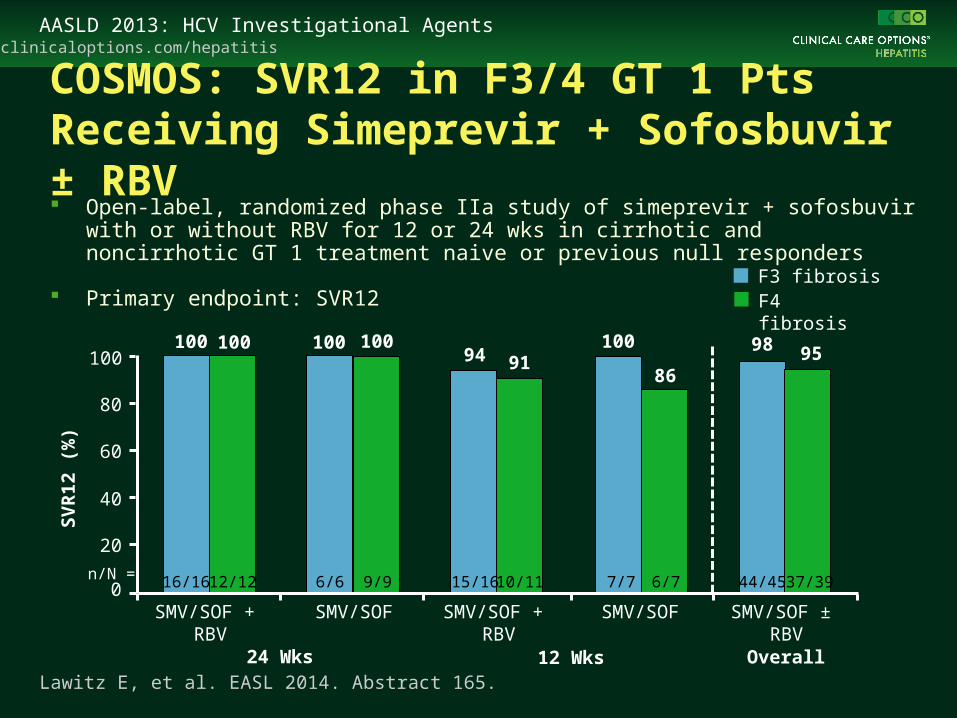
COSMOS: SVR12 in F3/4 GT 1 Pts Receiving Simeprevir + Sofosbuvir ± RBV
Lawitz E, et al. EASL 2014. Abstract 165.
Open-label, randomized phase IIa study of simeprevir + sofosbuvir with or without RBV for 12 or 24 wks in cirrhotic and noncirrhotic GT 1 treatment naive or previous null responders
Primary endpoint: SVR12
SMV/SOF ± RBV
SMV/SOF + RBV
SMV/SOF + RBV
SMV/SOF SMV/SOF
24 Wks 12 Wks Overall
16/16 12/12 6/6 9/9 15/16 10/11 7/7 6/7 44/45 37/39
F3 fibrosisF4 fibrosis
SV
R12
(%
)
100
80
60
40
20
0
100 100 100 100 10094 91
98
8695
n/N =

clinicaloptions.com/hepatitisAASLD 2013: HCV Investigational Agents
Promising IFN-Free Regimens in Genotype 1 Cirrhotic Patients
RegimenSVR12, %
Tx Naive Tx Exp PI Failure
Sofosbuvir + ledipasvir[1,2] --- 70 (N = 10) 91 (N = 11)
Sofosbuvir + ledipasvir + RBV[1,2] --- 100 (N = 25) 100 (N = 11)
Sofosbuvir + ledipasvir + GS-9669[1] --- 100 (N = 26) ---
Daclatasvir + asunaprevir[3]* 90 (N = 203)† 82 (N = 205)† ---
Daclatasvir + asunaprevir + BMS-791325 75 mg[4] 94 (N = 16) --- ---
Daclatasvir + asunaprevir + BMS-791325 150 mg[4] 89 (N = 18) --- ---
ABT-450/ritonavir/ombitasvir + dasabuvir + RBV[5] 94 (N = 86) 87-97 (N = 122) ---
ABT-450/ritonavir/ombitasvir + dasabuvir + RBV[5]* 95 (N = 74) 95-100 (N = 98) ---
1. Gane EJ, et al. AASLD 2013. Abstract 73. 2. Lawitz. E et al. AASLD 2013, Abstract 215. 3. Manns M, et al. EASL 2014. Abstract 166. 4. Everson GT, et al. Gastroenterol. 2014;146:420-429. 5. Poordad F, et al. N Engl J Med. 2014;[Epub ahead of print].
*Treatment duration: 24 weeks; all others 12 weeks.†Genotype 1b HCV-infected patients only
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
Take Home Points
Cirrhotic patients are the most in need for HCV treatment
Child-Pugh A patients should be strongly advised to undergo therapy
More advanced cirrhosis should be treated with caution on a case-by-case basis
Newest DAA + pegIFN/RBV combinations increase SVR in cirrhotic patients
IFN-free DAA regimens demonstrate significant potency in cirrhotic patients
Ensuring Informed Decision-Making When Treating or Deferring in
Cirrhotic Patients
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
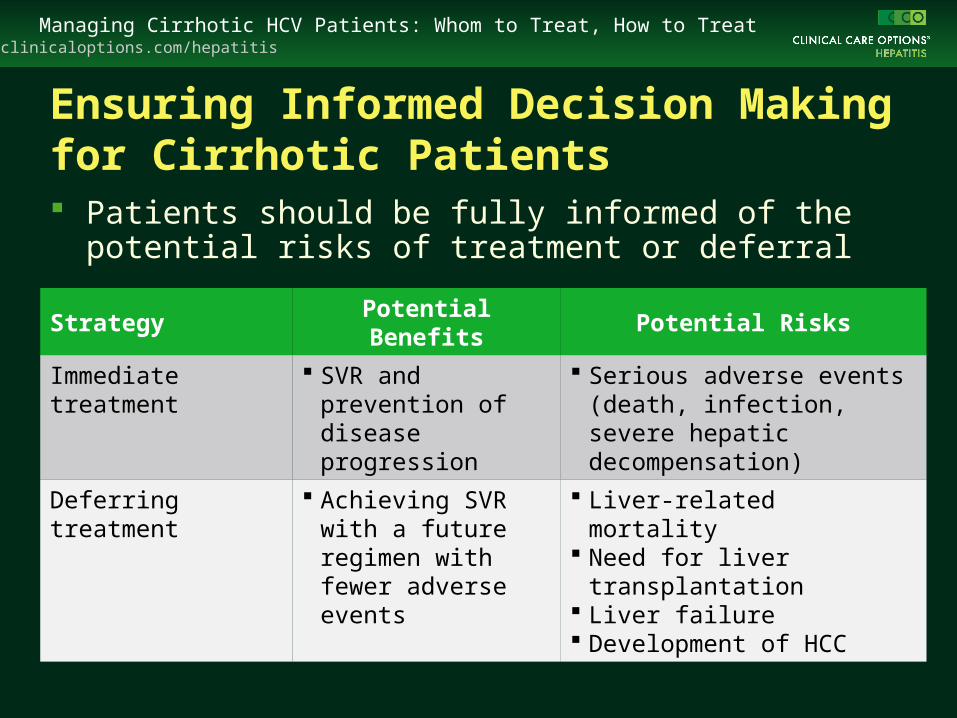
Ensuring Informed Decision Making for Cirrhotic Patients Patients should be fully informed of the potential risks of
treatment or deferral
Strategy Potential Benefits Potential Risks
Immediate treatment SVR and prevention of disease progression
Serious adverse events (death, infection, severe hepatic decompensation)
Deferring treatment Achieving SVR with a future regimen with fewer adverse events
Liver-related mortality Need for liver transplantation Liver failure Development of HCC
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
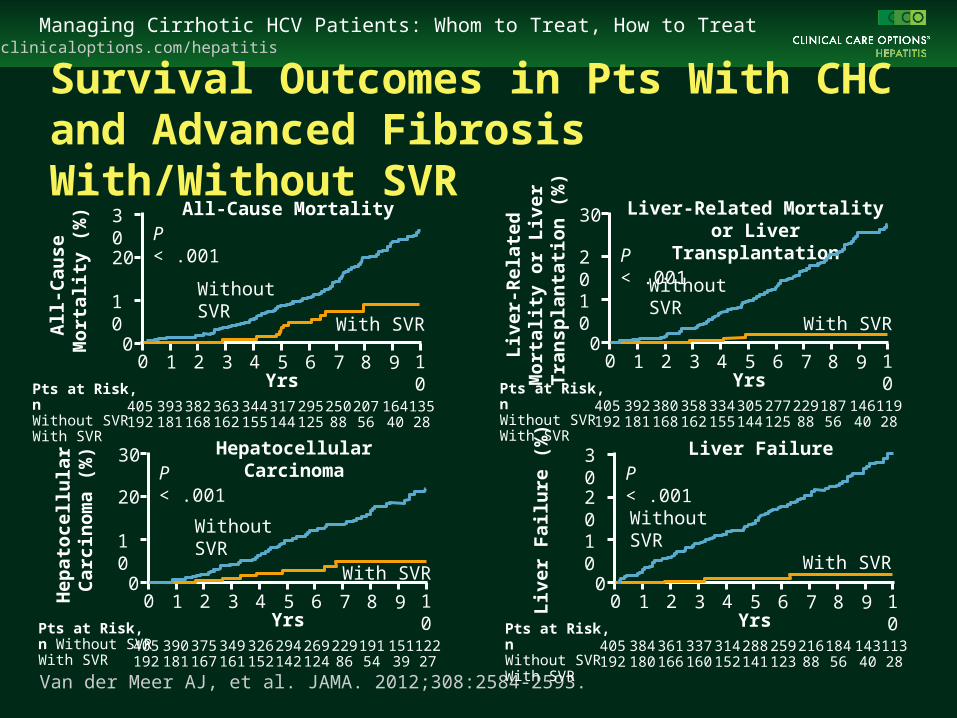
Survival Outcomes in Pts With CHC and Advanced Fibrosis With/Without SVR
Van der Meer AJ, et al. JAMA. 2012;308:2584-2593.
30
20
10
00
All
-Cau
se
Mo
rtal
ity
(%)
1 2 3 4 5 6 7 8 9 10Yrs
All-Cause MortalityP < .001
Without SVR
With SVR
Pts at Risk, nWithout SVRWith SVR
405192
393181
382168
363162
344155
317144
295125
25088
20756
16440
13528
30
20
10
00
Liv
er-
Rel
ated
M
ort
alit
y o
r L
iver
T
ran
spla
nta
tio
n (
%)
1 2 3 4 5 6 7 8 9 10Yrs
Liver-Related Mortality or Liver Transplantation
P < .001
Without SVR
With SVR
Pts at Risk, n Without SVRWith SVR
405192
392181
380168
358162
334155
305144
277125
22988
18756
14640
11928
30
20
10
00
Hep
ato
cell
ula
r C
arci
no
ma
(%)
1 2 3 4 5 6 7 8 9 10Yrs
Hepatocellular CarcinomaP < .001
Without SVR
With SVR
Pts at Risk, n Without SVRWith SVR
405192
390181
375167
349161
326152
294142
269124
22986
19154
15139
12227
30
20
10
00
Liv
er
Fai
lure
(%
)
1 2 3 4 5 6 7 8 9 10Yrs
Liver FailureP < .001
Without SVR
With SVR
Pts at Risk, n Without SVRWith SVR
405192
384180
361166
337160
314152
288141
259123
21688
18456
14340
11328
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
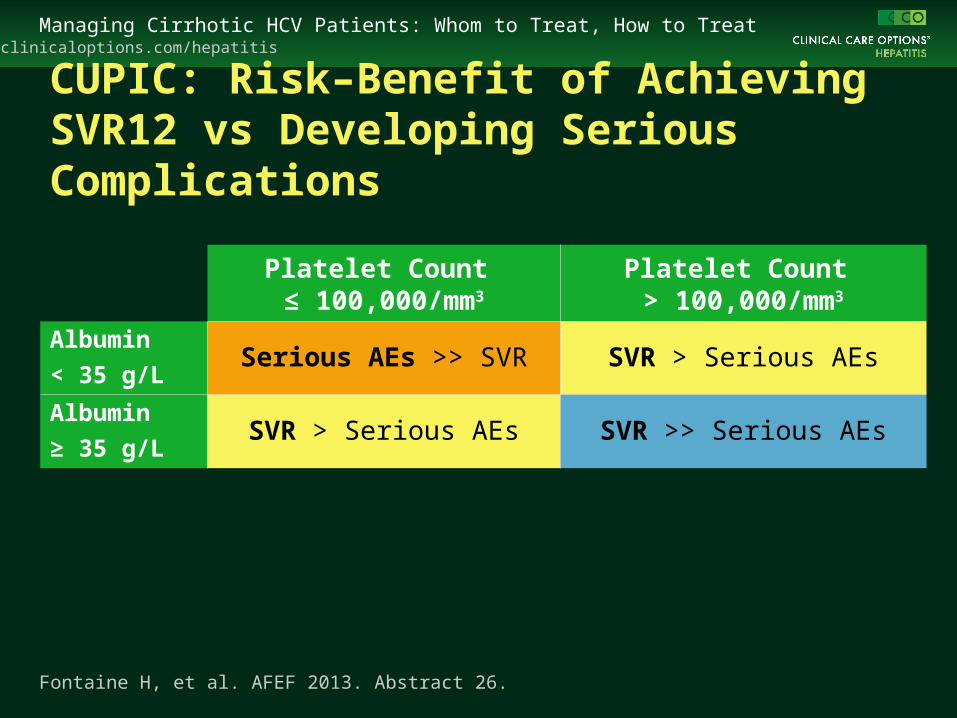
CUPIC: Risk–Benefit of Achieving SVR12 vs Developing Serious Complications
Platelet Count ≤ 100,000/mm3
Platelet Count > 100,000/mm3
Albumin
< 35 g/LSerious AEs >> SVR SVR > Serious AEs
Albumin
≥ 35 g/LSVR > Serious AEs SVR >> Serious AEs
Fontaine H, et al. AFEF 2013. Abstract 26.
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
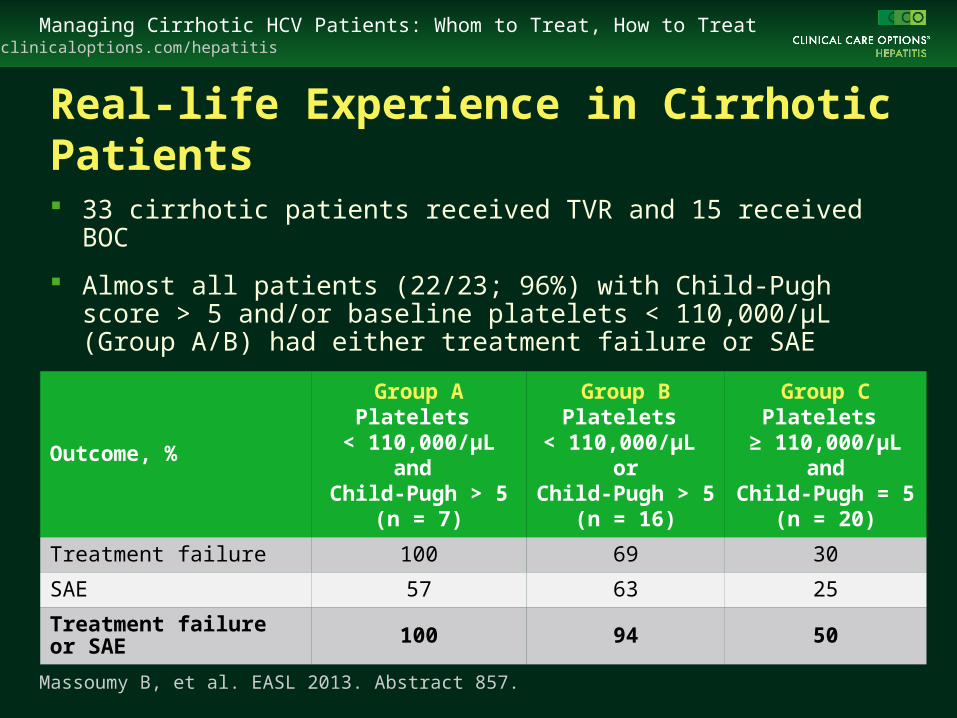
Real-life Experience in Cirrhotic Patients
33 cirrhotic patients received TVR and 15 received BOC
Almost all patients (22/23; 96%) with Child-Pugh score > 5 and/or baseline platelets < 110,000/µL (Group A/B) had either treatment failure or SAE
Outcome, %
Group APlatelets
< 110,000/µLand
Child-Pugh > 5(n = 7)
Group BPlatelets
< 110,000/µL or
Child-Pugh > 5(n = 16)
Group CPlatelets
≥ 110,000/µLand
Child-Pugh = 5(n = 20)
Treatment failure 100 69 30
SAE 57 63 25
Treatment failure or SAE 100 94 50
Massoumy B, et al. EASL 2013. Abstract 857.
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
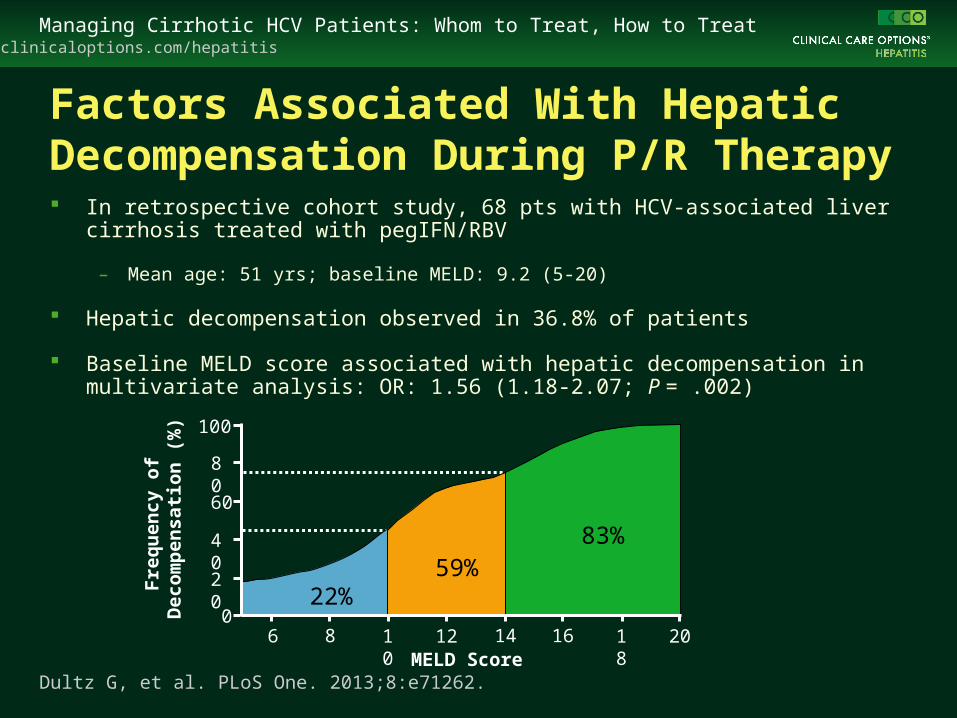
Factors Associated With Hepatic Decompensation During P/R Therapy In retrospective cohort study, 68 pts with HCV-associated liver cirrhosis treated with
pegIFN/RBV
– Mean age: 51 yrs; baseline MELD: 9.2 (5-20)
Hepatic decompensation observed in 36.8% of patients
Baseline MELD score associated with hepatic decompensation in multivariate analysis: OR: 1.56 (1.18-2.07; P = .002)
Dultz G, et al. PLoS One. 2013;8:e71262.
100
80
60
06
Fre
qu
enc
y o
f D
eco
mp
en
sati
on
(%
)
40
20
8 10 12 14 16 18 20MELD Score
22%59%
83%
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
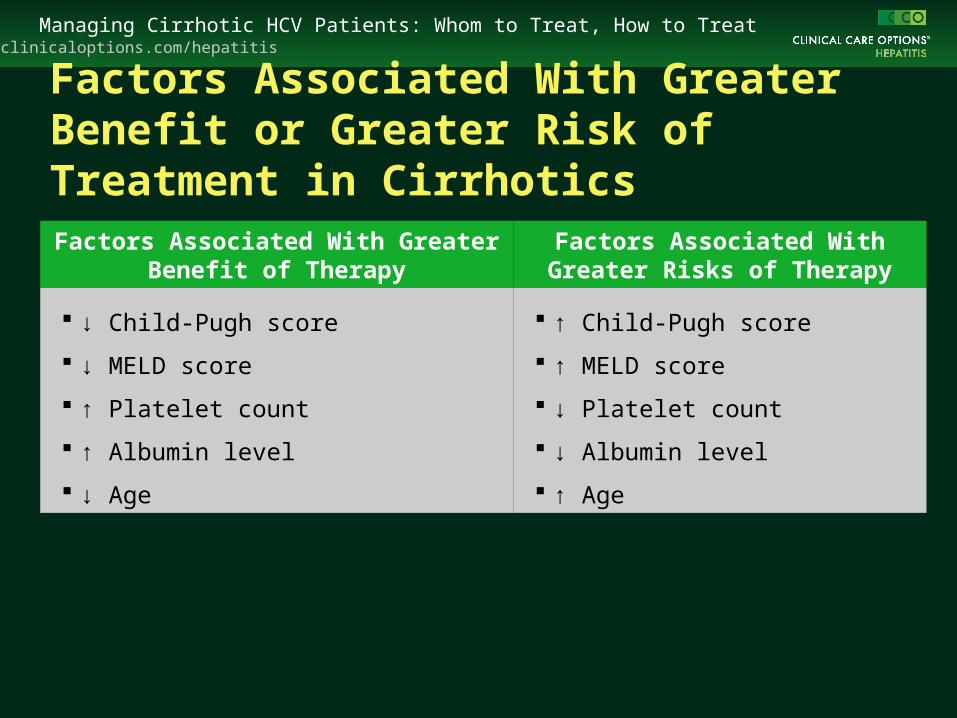
Factors Associated With Greater Benefit or Greater Risk of Treatment in Cirrhotics
Factors Associated With Greater Benefit of Therapy
Factors Associated With Greater Risks of Therapy
↓ Child-Pugh score
↓ MELD score
↑ Platelet count
↑ Albumin level
↓ Age
↑ Child-Pugh score
↑ MELD score
↓ Platelet count
↓ Albumin level
↑ Age
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
Take Home Points
HCV treatment in cirrhotic patients is associated with high rates of treatment-related adverse events and lower response rates than in patients with less advanced disease
However, immediate treatment could lead to SVR and prevent disease progression
For every patient, an informed choice is critical
Optimizing Outcomes in Patients Who Wish
To Be Treated
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
Pretreatment Optimization Strategies
Lifestyle changes
Pretreatment initiation of eltrombopag
Ultrasound to exclude ascites
Check recent endoscopy report
Consider antibiotics in cirrhotic patients with upper gastrointestinal bleeding[1]
1. Chavez-Tapia NC, et al. Cochrane Database Syst Rev. 2010;9:CD002907.
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
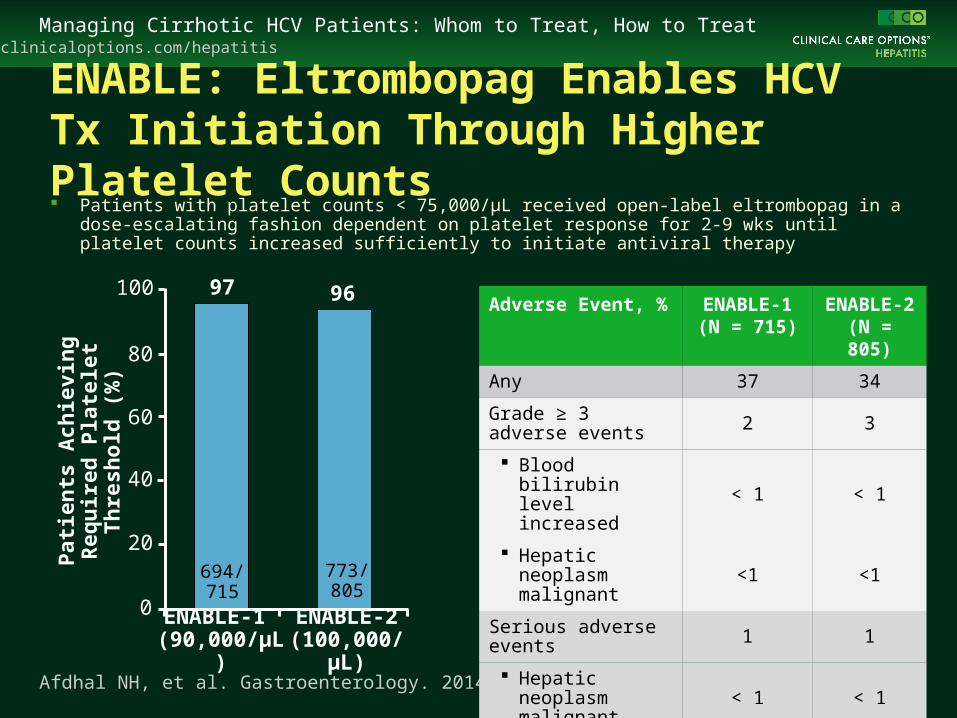
ENABLE: Eltrombopag Enables HCV Tx Initiation Through Higher Platelet Counts Patients with platelet counts < 75,000/µL received open-label eltrombopag in a
dose-escalating fashion dependent on platelet response for 2-9 wks until platelet counts increased sufficiently to initiate antiviral therapy
773/805
694/715
ENABLE-1 (90,000/µL)
ENABLE-2(100,000/µL)
9697100
80
60
40
20
0
Pat
ien
ts A
chie
vin
g R
equ
ired
P
late
let
Th
resh
old
(%
)
Afdhal NH, et al. Gastroenterology. 2014;146:442-452.
Adverse Event, % ENABLE-1(N = 715)
ENABLE-2(N = 805)
Any 37 34
Grade ≥ 3 adverse events 2 3
Blood bilirubin level increased < 1 < 1
Hepatic neoplasm malignant <1 <1
Serious adverse events 1 1
Hepatic neoplasm malignant < 1 < 1
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
On-Treatment Optimization Strategies
Anemia management
– RBV dose reductions
– Addition of erythropoietin
– Transfusions
Management of thrombocytopenia
– On-treatment initiation of eltrombopag
Monitoring of renal function
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
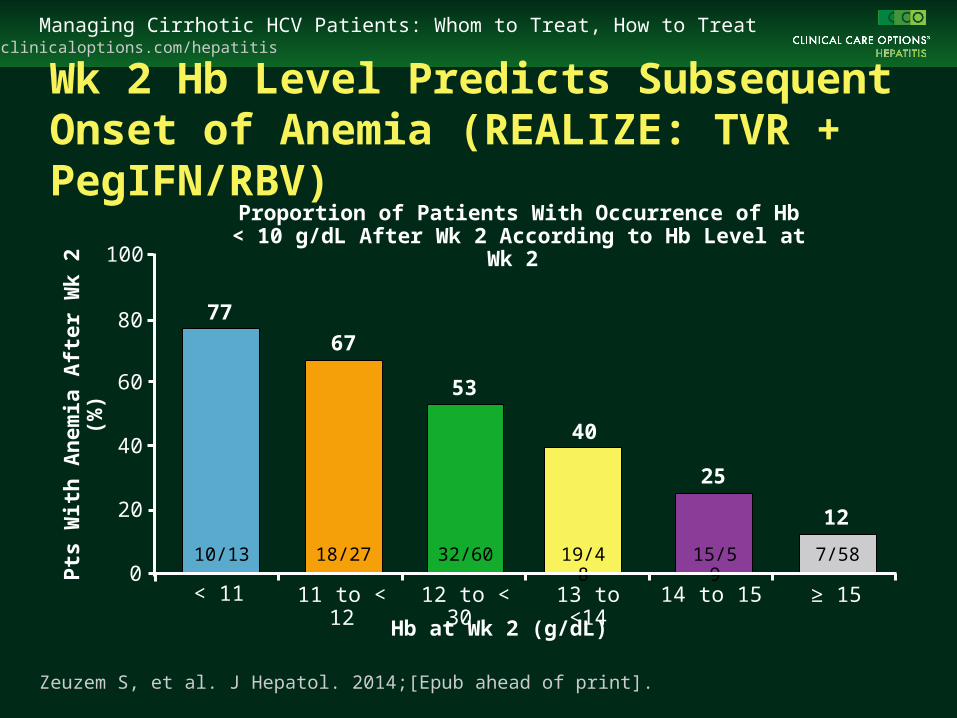
Wk 2 Hb Level Predicts Subsequent Onset of Anemia (REALIZE: TVR + PegIFN/RBV)
Pts
Wit
h A
nem
ia A
fter
Wk
2 (%
)
10/13 19/4832/60 15/59 7/5818/27
< 11 11 to < 12 12 to < 30 13 to <14 14 to 15 ≥ 15
Hb at Wk 2 (g/dL)
Proportion of Patients With Occurrence of Hb < 10 g/dL After Wk 2 According to Hb Level at Wk 2
Zeuzem S, et al. J Hepatol. 2014;[Epub ahead of print].
100
80
60
40
20
0
77
67
53
40
25
12
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
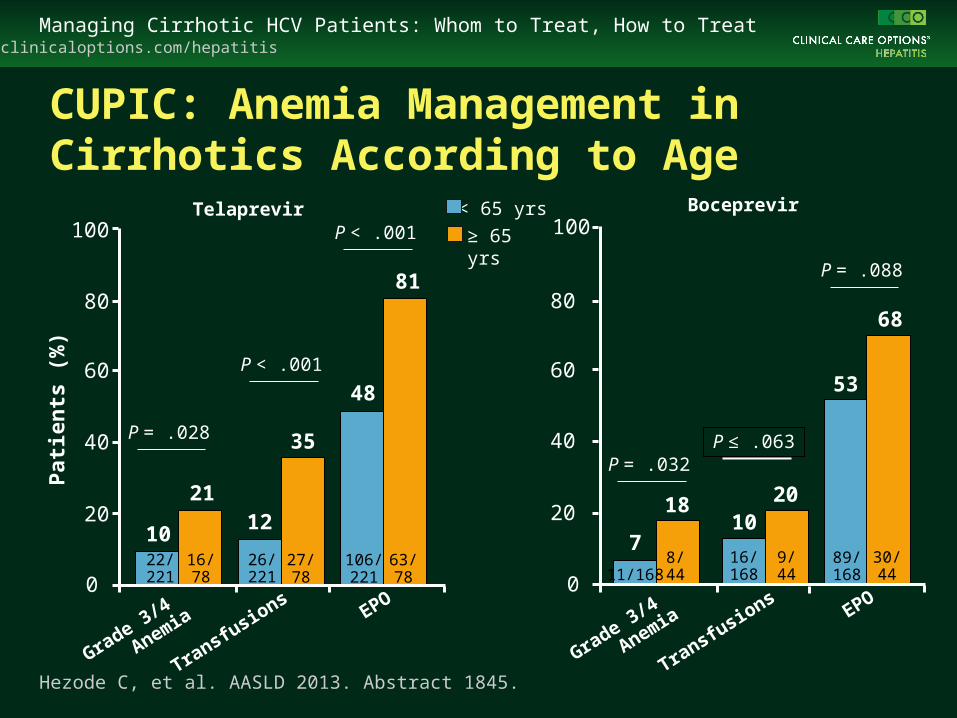
CUPIC: Anemia Management in Cirrhotics According to Age
22/221
Grade 3/4
Anemia
Transfusions
10
100
80
60
40
20
0
Pat
ien
ts (
%)
Hezode C, et al. AASLD 2013. Abstract 1845.
< 65 yrs
≥ 65 yrs
21
16/78
26/221
12
35
27/78
106/221
48
81
63/78
EPO
P = .028
P < .001
P < .001
Grade 3/4
Anemia
Transfusions
7
100
80
60
40
20
0
18
8/44
16/168
1020
9/44
89/168
53
68
30/44
EPO
P = .032P ≤ .063
P = .088
Telaprevir Boceprevir
11/168
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
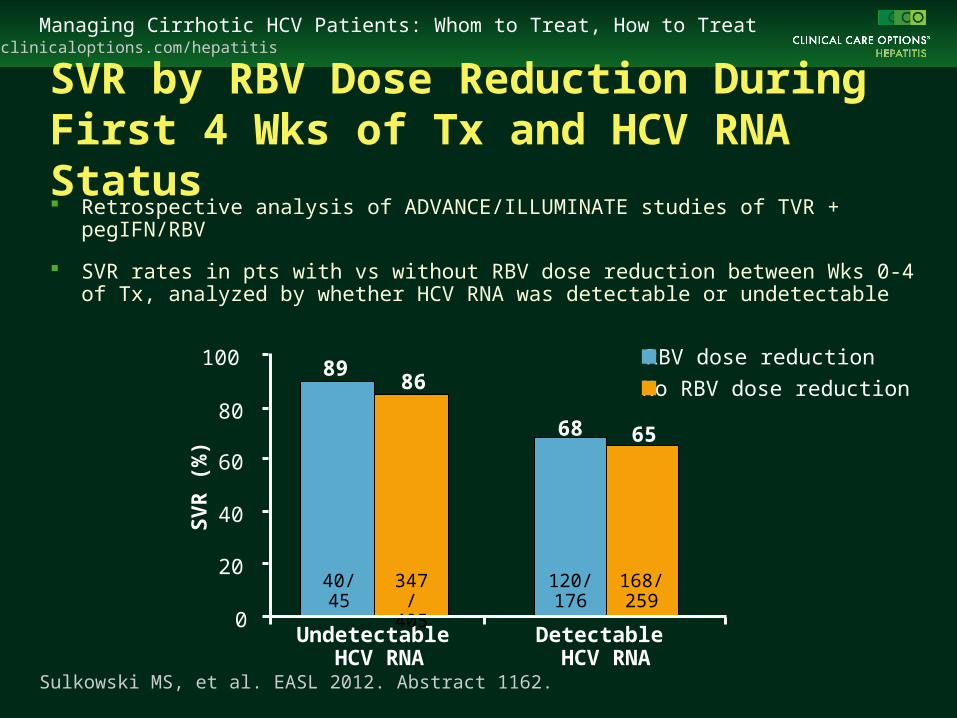
SVR by RBV Dose Reduction During First 4 Wks of Tx and HCV RNA Status Retrospective analysis of ADVANCE/ILLUMINATE studies of TVR +
pegIFN/RBV
SVR rates in pts with vs without RBV dose reduction between Wks 0-4 of Tx, analyzed by whether HCV RNA was detectable or undetectable
120/176
40/45
Undetectable HCV RNA
Detectable HCV RNA
68
89100
80
60
40
20
0
SV
R (
%)
Sulkowski MS, et al. EASL 2012. Abstract 1162.
347/405
86
168/259
65
RBV dose reduction
No RBV dose reduction
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
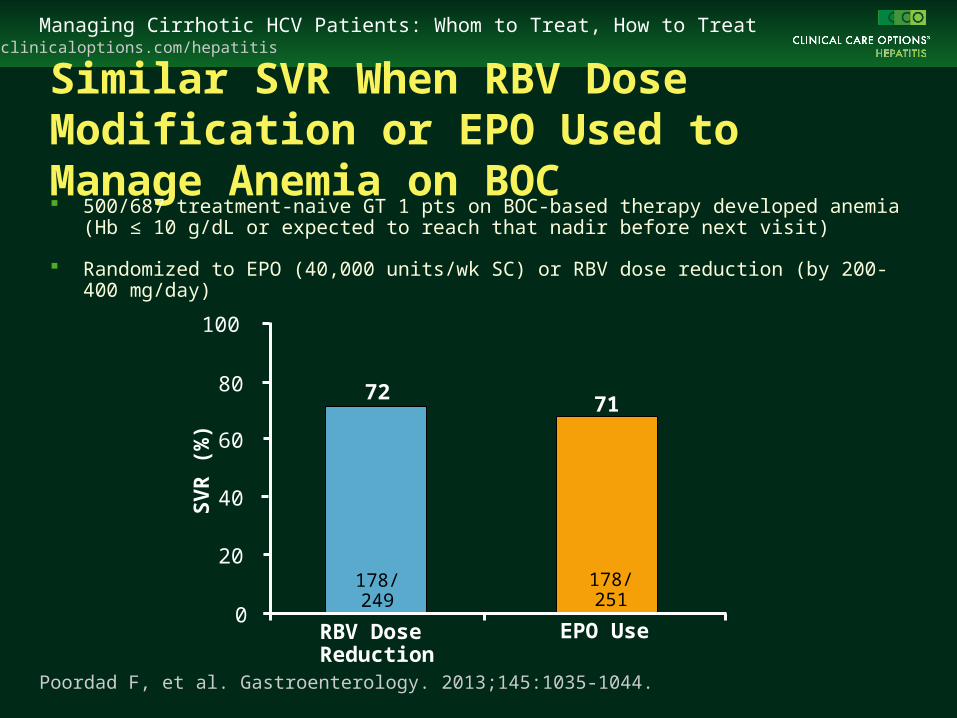
Similar SVR When RBV Dose Modification or EPO Used to Manage Anemia on BOC 500/687 treatment-naive GT 1 pts on BOC-based therapy developed anemia
(Hb ≤ 10 g/dL or expected to reach that nadir before next visit)
Randomized to EPO (40,000 units/wk SC) or RBV dose reduction (by 200-400 mg/day)
178/251
178/249
RBV Dose Reduction
EPO Use
7172
100
80
60
40
20
0
SV
R (
%)
Poordad F, et al. Gastroenterology. 2013;145:1035-1044.
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
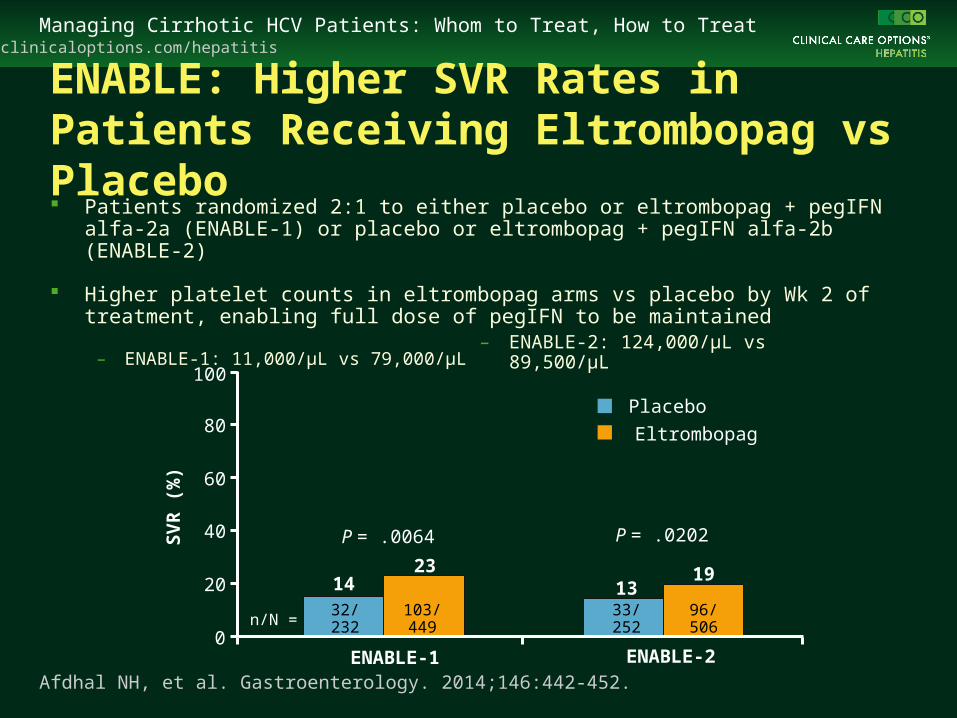
ENABLE: Higher SVR Rates in Patients Receiving Eltrombopag vs Placebo Patients randomized 2:1 to either placebo or eltrombopag + pegIFN alfa-2a (ENABLE-1)
or placebo or eltrombopag + pegIFN alfa-2b (ENABLE-2)
Higher platelet counts in eltrombopag arms vs placebo by Wk 2 of treatment, enabling full dose of pegIFN to be maintained
– ENABLE-1: 11,000/µL vs 79,000/µL
0
20
40
80
100
SV
R (
%) 60
32/232
14
ENABLE-1 ENABLE-2
103/449
33/252
96/506
2313
19
Placebo
Eltrombopag
n/N =
P = .0064 P = .0202
Afdhal NH, et al. Gastroenterology. 2014;146:442-452.
– ENABLE-2: 124,000/µL vs 89,500/µL
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
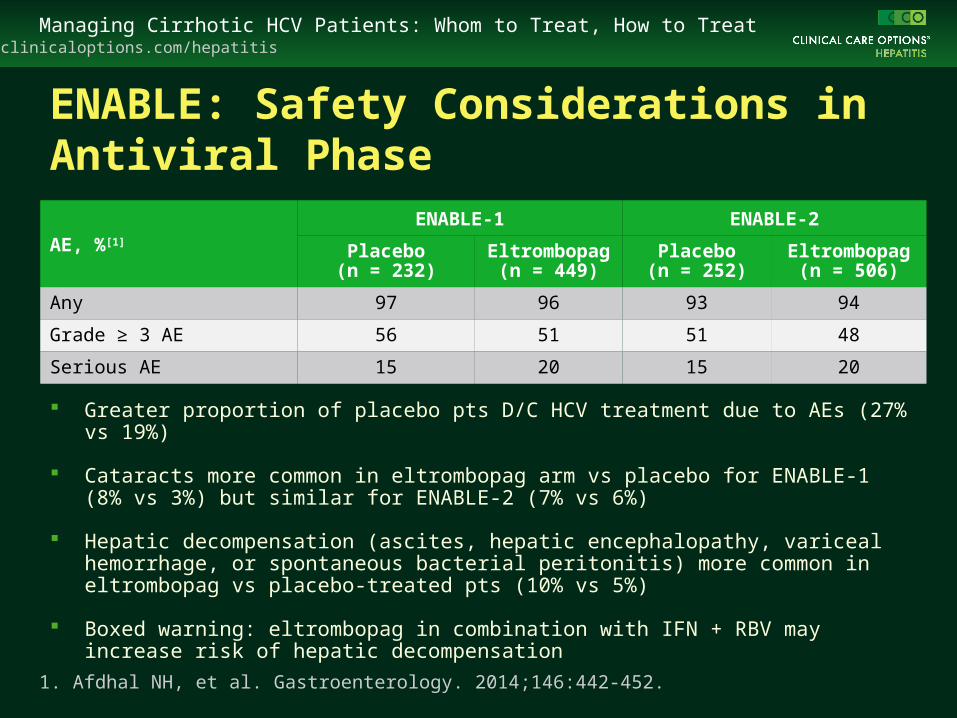
ENABLE: Safety Considerations in Antiviral Phase
Greater proportion of placebo pts D/C HCV treatment due to AEs (27% vs 19%)
Cataracts more common in eltrombopag arm vs placebo for ENABLE-1 (8% vs 3%) but similar for ENABLE-2 (7% vs 6%)
Hepatic decompensation (ascites, hepatic encephalopathy, variceal hemorrhage, or spontaneous bacterial peritonitis) more common in eltrombopag vs placebo-treated pts (10% vs 5%)
Boxed warning: eltrombopag in combination with IFN + RBV may increase risk of hepatic decompensation
1. Afdhal NH, et al. Gastroenterology. 2014;146:442-452.
AE, %[1]
ENABLE-1 ENABLE-2
Placebo(n = 232)
Eltrombopag (n = 449)
Placebo(n = 252)
Eltrombopag (n = 506)
Any 97 96 93 94
Grade ≥ 3 AE 56 51 51 48
Serious AE 15 20 15 20
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
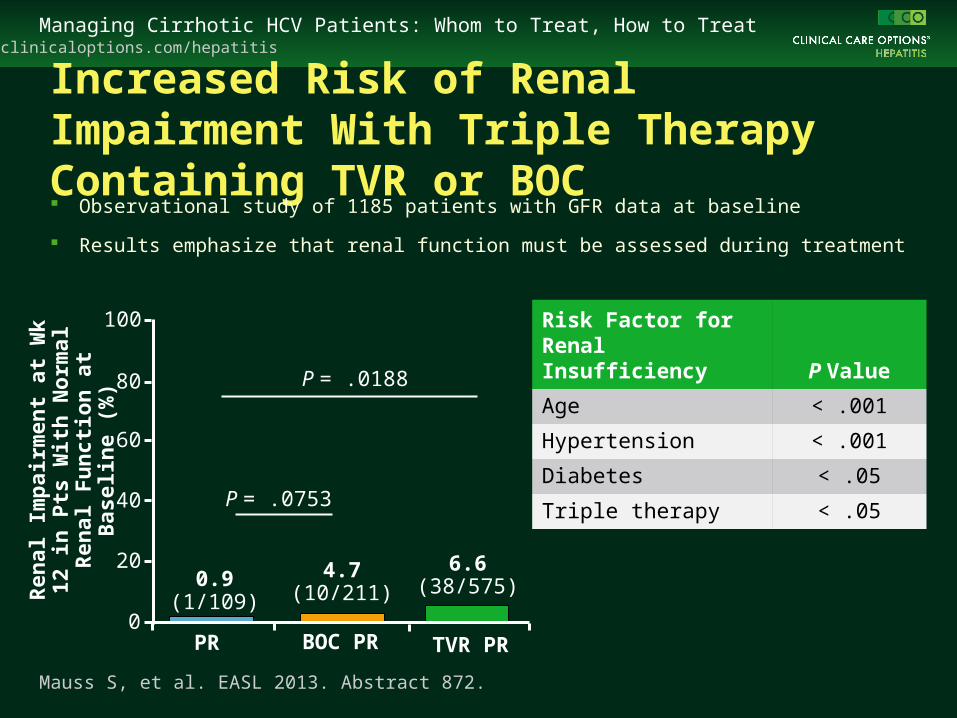
Increased Risk of Renal Impairment With Triple Therapy Containing TVR or BOC Observational study of 1185 patients with GFR data at baseline
Results emphasize that renal function must be assessed during treatment
PR BOC PR
4.7(10/211)
0.9(1/109)
100
80
60
40
20
0
Ren
al Im
pai
rmen
t at
Wk
12 in
P
ts W
ith
No
rmal
Ren
al
Fu
nct
ion
at
Bas
elin
e (%
)
Mauss S, et al. EASL 2013. Abstract 872.
6.6(38/575)
TVR PR
P = .0753
P = .0188
Risk Factor for Renal Insufficiency P Value
Age < .001
Hypertension < .001
Diabetes < .05
Triple therapy < .05
clinicaloptions.com/hepatitisManaging Cirrhotic HCV Patients: Whom to Treat, How to Treat
Take Home Points
Hb level should be frequently assess during treatment and anemia should be treated as early as possible
– EPO and RBV dose reductions for anemia lead to similar SVR rates in BOC-treated patients
In HCV patients with platelet counts < 70,000/µL, eltrombopag may increase platelet counts to levels that allow HCV therapy to be initiated and may allow for higher SVR rates with a reduced need for pegIFN dose reductions
Renal function must be assessed during treatment
Go Online for More Insights Into the Management of Cirrhotic HCV Patients
Downloadable slideset
clinicaloptions.com/treatnow
![Case Report Simeprevir and Sofosbuvir …downloads.hindawi.com › journals › crihem › 2016 › 7635128.pdffor the treatment of cirrhotic patients with HCV genotype infection []](https://img.pdfslide.net/doc/110x75/5f218a340471711893037ff4/case-report-simeprevir-and-sofosbuvir-a-journals-a-crihem-a-2016-a-7635128pdf.jpg)



![Treat To Prevent Millennials, Drugs and HCV · PDF file · 2017-02-20Treat To Prevent – Millennials, Drugs and Hepatitis C [HCV] Strategies To Identify and Advance PWID HCV Patient](https://img.pdfslide.net/doc/110x75/5aa294e57f8b9a1f6d8d6b5a/treat-to-prevent-millennials-drugs-and-hcv-2017-02-20treat-to-prevent-millennials.jpg)