Embed Size (px)
Citation preview

MANEGEMENT OF CHRONIC(NEUROGENIC) PAIN
Dr. A.V. SrinivasanMD.,DM.,Ph.D .,D.Sc (HON).F.I.A.N.,F.A.AN.Emeritus professor of Tamilnadu Dr. M.G.R Medical University. Adjunct Professor –IIT, ChennaiFormer Head, Institute of Neurology- Madras medical college.South Africa -26-07-2011

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Understanding, Impact and Understanding, Impact and AwarenessAwareness
Chronic PainChronic Pain

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
“Pain May be Inevitable, but Misery is Optional”
Dee Malchow
Pain constitutes nearly 40% of the total of patient visits to doctors.1
1 Mäntyselkä et al. Pain as a reason to visit the doctor: a study in Finnish primary health care. Pain. 2001 Jan;89(2-3):175-80.

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Pain is undertreated
• In 2001, Barry Furrow wrote “Pain is undertreated” in the American health-
care system at all levels.2
• The term "opiophobia" has been coined to describe this remarkable clinical
aversion to the proper use of opioids to control pain.
• The possible reasons for health-care providers' failures to properly manage
pain are many;
– Occasional lack of knowledge about appropriate treatment choices for
pain management
– A reflection of a Culture hostile to drug use
– Threats of legal action.
– Worry about tolerance and addiction and other adverse drug effects
– Something as trivial as the lack of insurance cover, can lead to patients
suffering unnecessary pain as a result.
2. R.M. Marks and E.J. Sachar, "Undertreatment of Medical Inpatients with Narcotic Analgesics,"Annals of Internal Medicine, 78 (1973): 173.

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Indian Scenario
• Despite an essentially stoic and less demanding Indian patient; the
obligation to manage pain comes to the fore not only to complete the
perfection of a clinicians management.
• But also, it is an independent entity with physical and psychological
components that in adherence to best practices can neither be
ignored nor treated such that adverse effects eclipse the malady.
• This importance of pain management is further increased when
benefits for the patient are realized,
– Early mobilization which tends to prevent the more dangerous
complication of a deep vein thrombosis;
– Shortening hospital stay
– Reducing costs

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Decade of Pain Control and Research
• In late 2000, US Congress passed into law a provision, which the president signed , that declared the 10 year period beginning Jan 1st 2001, as the Decade of Pain Control and Research.
• The American Pain Society has actively supported the Decade of Pain Control Research, and it has been a focal point for the development of numerous programs to advance awareness and treatment of pain and funding for research.

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
What is Pain?
• Pain is always a subjective experience
• Everyone learns the meaning of “pain” through experiences
usually related to injuries in early life
• As an unpleasant sensation it becomes an emotional experience
• Pain is a significant stress physically, emotionally
(American Society of Anesthesiologists, 2002; Loeser et al, 2001; Merskey H et al, 1994; Portenoy et al, 1996)
The International Association for the Safety of Pain (IASP) defines pain an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage, or both.

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Qualities of Pain• Organic vs. psychogenic• Acute vs. chronic• Malignant or benign• Continuous or episodic
Perceiving Pain• Algogenic substances – chemicals released at the site of the
injury• Nociceptors – afferent neurons that carry pain messages• Referred pain – pain that is perceived as if it were coming from
somewhere else in the body

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Acute vs. Chronic Pain
ACUTE CHRONIC
Function To warn None (destructive)
Etiology Usually Clear Complex/obscure
Pt. Mood Anxiety/fear Depression/anger
MD impact Comforting Frustrating/draining
Role of Rx Control/cure Improve function/QOL

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Categorization of Chronic pain
Types of PainTypes of Pain
Pain arising from pain receptors
[Nociceptive Pain]
Pain arising from pain receptors
[Nociceptive Pain]
(Psychogenic)
Pain with NO apparent cause(e.g. Low back pain or some
pelvic pain in women)
(Psychogenic)
Pain with NO apparent cause(e.g. Low back pain or some
pelvic pain in women)
Pain arising from Nervous system[Neuropathic Pain]
Pain arising from Nervous system[Neuropathic Pain]
Central(Brain and Spinal cord)
Central(Brain and Spinal cord)
Peripheral (Peripheral nervous
system)
Peripheral (Peripheral nervous
system)
Superficical / SomaticSuperficical / Somatic Deep / VisceralDeep / Visceral
Keay, KA; Clement, CI; Bandler, R (2000). "The neuroanatomy of cardiac nociceptive pathways". in Horst, GJT. The nervous system and the heart. Totowa, New Jersey: Humana Press. p. 304

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Different types of pain
Nociceptive descriptors Neuropathic descriptors
Cramping, tender Shooting
Gnawing, heavy Hot-burning
Aching Sharp
Splitting Stabbing

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Current Understanding of Pain• Chronic pain is NOT a normal part of aging.
• Emotions play a key role in painful experience
• Pain sounds a warning, signaling damage to tissues, and has survival value so pain receptors do not adapt to prolonged stimulation and pain sensation may intensify as pain thresholds are lowered by continued stimulation.
• The 19th Century viewed pain as a solely physiological entity with two theories dominating – the “specificity” & the “summation” theories. 8
• Paradigm Shift:
– Pain perception impulses are modified by ascending and by descending pain-suppressing systems activated by various environmental and psychological factors.
– 1965 Melzack & Wall: Gate Theory of Pain marked a turning point in understanding transmission and modulation of nociceptive signals, and recognition of pain as a psychophysiological phenomenon.
• The concept of Neuroplasticity was recognized and accepted adding dynamism to neuronal & brain structure with neuroimaging of the central nervous system in three domains; anatomical, functional, and chemical imaging helping measure changes in chronic pain.
• Taken together these three domains have changed our thinking on pain; now considered an altered brain state in which there may be altered functional connections or systems and components of degenerative aspects of the CNS. 9
8) 11. J.A. Paice, C. Toy, and S. Short, "Barriers to Cancer Pain Relief: Fear of Tolerance and Addiction," Journal of Pain and Symptom Management, 16 July 1998): 1-9.9) Quick Reference Guide for Clinicians No. 1a. AHCPR Publication No. 92-0019: February 1993

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Understanding Pain Pathophysiology

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
What causes pain?
• Trauma/ injury initiates immediate nerve impulses to brain
• Injury to cells result in chemical release
• H+
• K+
• Substance P• Bradykinin• 5HT• Phospholipids Prostaglandins
• Blood vessels leak resulting in inflammation
• Stimulate C-fibres (slow response)

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
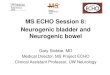
Peripheral and Central Pathways for Pain
Ascending TractsAscending Tracts Descending TractsDescending Tracts
Cortex
Midbrain
Medulla
Spinal Cord
Thalamus
Pons
(Brookoff, 2000)

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Pain Pathway

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Pathophysiology of Chronic Pain
• In chronic pain, the nervous system remodels continuously in response to repeated pain signals
– nerves become hypersensitive to pain
– nerves become resistant to anti-nociceptive system
• If untreated, pain signals will continue even after injury resolves
• Chronic pain signals become embedded in the central nervous system
(Marcus, 2000)

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Pain-Sensing System in the Malfunction in Chronic Pain
(Illustration: Seward Hung, 2000)
Acute pain:Pain-sensing signals are initiated in response to a stimulus
• They elicit a pain-relieving response
Chronic pain:Pain signals are generated for no reason and may be intensified
• Pain-relieving mechanisms may be defective or deactivated
Pain Sensing
In chronic pain, pain signals are generated without physiologic significance

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Pathophysiology of Pain
• Inferred from characteristics, etiology or pathophysiology
• Types
– Nociceptive
– Neuropathic
– Idiopathic
• Therapeutic implications
(Portenoy et al, 1996)

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Nociceptive Pain
Presumably results from ongoing activation of primary afferent neurons responding to noxious stimuli
• Pain consistent with degree of tissue injury
• Described as aching, squeezing, stabbing, throbbing
• Subtypes:
– Somatic: related to activation of somatic afferent neurons
– Visceral: related to activation of visceral afferent neurons
(Loeser et al, 2001; Portenoy et al, 1996)

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Neuropathic Pain
• Initiated by a primary lesion in the nervous system; believed to be sustained by aberrant somatosensory processing in the peripheral or central nervous system
• Independent of obvious ongoing nociceptive activation
• Burning, shooting, electrical quality; may be aching, throbbing, sharp
• Subtypes:
– Presumed “central generator”
deafferentation pain (central pain, phantom pain)
Sympathetically-maintained pain
– Presumed “peripheral generator”
Polyneuropathies and mononeuropathies
(Portenoy et al, 1996)

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Idiopathic and Psychogenic Pain
Idiopathic Pain
• Usually exists in the absence of an identifiable physical or psychologic pathology that could account for pain
• Uncommon in patients with progressive illness
Psychogenic Pain
• Presents positive evidence of a predominant psychologic contribution and may be labeled with a specific psychiatric diagnosis
(Loeser et al, 2001; Merskey et al, 1994; Portenoy et al, 1996)

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Recent Developments In Pain Management
• Greater understanding of the pathophysiology underlying chronic pain syndromes
• Scientific breakthroughs in molecular biology; insight into pain at the molecular level
• Advances in drug therapy (drug delivery technologies)
• Multimodal therapy
• Multidisciplinary teams, shared decision-making that includes patients
• Patients’ rights movement
(JCAHO, 1999; Loeser et al, 2001)

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Therapeutic Modalities for
Chronic Pain Management
Assessment
Progress in Chronic Pain Management:Progress in Chronic Pain Management:

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
“Describing pain only in terms of its
intensity is like describing music only in
terms of its loudness”
von Baeyer CL; Pain Research and Management 11(3) 2006; p.157-162

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Pain Assessment
• Characterize the pain
• Characterize the disease, relationship between pain and disease and potentially treatable etiologies
• Clarify syndromes and infer pathophysiology
• Determine need for urgent therapy
• Identify other needs
• Develop a therapeutic strategy
(Portenoy et al, 1997)

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Components• History: temporal features, intensity, topography, quality,
exacerbating/alleviating factors• Physical Exam: determine existence of underlying pathology
• Lab and Radiographic Tests: appropriate to pain syndrome
Assessment Tools• Pain Intensity Scales: VAS, NAS, “faces” scale
• Multidimensional Pain Measures: Brief Pain Inventory, McGill Pain Questionnaire
(Portenoy et al, 1997)
Pain Assessment

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Pain Intensity Rating Scales• Visual Analogue Scale (VAS)
No painNo pain ----------------------------------- ----------------------------------- Worst painWorst pain
• Categorical Scale None (0) Mild (1 None (0) Mild (1 – 4) Moderate – 4) Moderate (5 (5 – 6) Severe – 6) Severe (7 – 10(7 – 10) )
• Numerical Rating Scale0 -------------------------------------0 ------------------------------------- 10 10
No painNo painWorst pain Worst pain imaginableimaginable
(Cleeland, 1991; Jacox et al, 1994)
00
No No hurthurt
22
Hurts just a Hurts just a little bitlittle bit
44
Hurts a little Hurts a little bit morebit more
66
Hurts even Hurts even moremore
88
Hurts a whole Hurts a whole lotlot
1010
Hurts as much Hurts as much as you can as you can
imagineimagine
• Pain Faces Scale
• Brief Pain Inventory Shade areas of worst pain. Put an X on area that hurts mostShade areas of worst pain. Put an X on area that hurts most

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Progress in Chronic Pain Management
Therapeutic Modalities for Therapeutic Modalities for
Chronic Pain Management:Chronic Pain Management:
TreatmentTreatment

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Therapeutic Options for Chronic Pain Management
• Pharmacotherapy (Analgesics)– Non-opioids – Adjuvant Analgesics
• Antidepressants• Anticonvulsants
– Opioids• Rehabilitative Approaches• Psychologic Interventions• Anesthesiological Approaches• Neurostimulatory Techniques• Surgery• Complementary/Alternative Approaches• Lifestyle Changes
(Cashman, 1996; Portenoy et al, 1997; Hanks et al, 1998; Galer, 1998; Stein, 1995)

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Status of antidepressants in chronic pain management
• Best evidence: TCAs – Inhibit both NA and 5-HT reuptake
• TCAs are superior to SSRIs in pain management
• TCAs are superior to the anticonvulsant
• There is no consensus regarding which of the many TCA
derivatives is most effective.
• The choice of TCA is therefore dictated largely by adverse
effects
Neurologic Complications of Cancer Therapy Current Treatment Options in Neurology 1999, 1.428-437
Litsedge, A Double-Blind Comparison of Dothiepin and Amitriptyline for the Treatment of Depression with Anxiety, Psychopharmacologia (Berl.) 19, 153--162 (1971)

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Which TCA?
• TCAs differ little in terms of their analgesic efficacy (Dworkin et. al 2007).
• Amitriptyline is the most widely studied TCA and is commonly used in neuropathic pain.
• Prothiaden being similar to amitriptyline is a good choice for the management of pain especially as it enjoys a relatively safer adverse event profile.
Prothiaden is a derivative of amitriptyline namely its thio-analogue.Prothiaden is a derivative of amitriptyline namely its thio-analogue.
Amitriptyline Prothaiden

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Prothiaden: Pharmacokinetics
– Rapidly absorbed from GIT on oral administration
– Tmax: 3 - 4 hours– Metabolized in liver to active metabolites -
northiaden, northiaden S-oxide and dothiepin S-oxide
– Excreted mainly in urine and also in faeces– A half-life of about 50 hours has been reported
for dosulepin and its metabolites

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Safety
Adverse events:
– Atropine-like side effects including dry mouth, disturbance of accommodation, tachycardia, constipation and hesitancy of micturition, are common early in treatment, but usually lessen as treatment continues
– Initially, dosulepin may impair alertness; patients likely to drive vehicles or operate machinery should be warned of this possibility.
Contra-indications : Recent MI, heart block, arrhythmias, mania, liver disease & during breast feeding
Dose:Adults: 50 mg to 150 mg daily.
Children: Not studied
Pregnancy and lactation: Not adequately studied

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Tolerability
• Extensive clinical studies as well as over two decades of clinical experience indicate that it is a well tolerated drug.
• The nature of side-effects reported are typical of a tricyclic antidepressant, it is better tolerated than other tricyclic antidepressants.
• “The general trend appeared to show better patient tolerance of Dothiepin than to any other active controls”.
• Goldstein and Claghorn (1980)
Dothiepin is better tolerated in relation to its side effects than amitriptyline.
Litsedge, A Double-Blind Comparison of Dothiepin and Amitriptyline for the Treatment of Depression with Anxiety, Psychopharmacologia (Berl.) 19, 153--162 (1971)

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
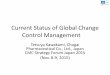
Mode of action: Dosulepin in chronic pain
Daniel a. Monti M.D. et. al. Management of chronic pain in elderly patients. Practical geriatrics; December 1996 Vol 49, No. 12 Brookoff, 2000
Dosulepin potentiate serotonin and norepinephrine in descending pain-suppressionpathways in the spinal cord.
Descending fibers that pass down from brainstem to spinal cord, inhibiting incoming sensations (ascending pathways) of pain.
A lot of these descending fibers originate in the locus ceruleus, others in the raphe nuclei.
Jann et. al. Antidepressant Agents for the Treatment of Chronic Pain and Depression. Pharmacotherapy 2007;27(11):1571–1587

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Mode of action
Ascending TractsAscending Tracts Descending TractsDescending Tracts
(Brookoff, 2000)
TCAs potentiate serotonin andnorepinephrine in descending pain-suppressionpathways in the spinal cord.
Descending fibres that pass down from brainstem to spinal cord, inhibiting incoming sensations (ascending pathways) of pain. A lot of these descending fibres originate in the locus coeruleus, others in the raphe nuclei.

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Dothiepin in management of chronic pain
• Dothiepin was used in a titrating dose in patients of atypical facial pain (Starting dose 12.5 mg, dose range 25-137.5 mglday) for 9weeks
– 34/48 dothiepin were pain free (score 0/1 mild, occasional) at week 9. vs 21/45 placebo
– Reduction in analgesic use; 83% dothiepin, 42% placebo
(Feinmannet al.,1984)

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
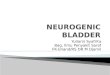
Proven efficacy in managing chronic pain
– In Prothiaden group pain
score measured on VAS
reduced from 56.7 to 42.2
– In placebo group, pain score
increased from 59.7 to 64.1
– Dothiepin is effective in
relieving pain, disability and
reducing the duration of early
morning stiffness in out-
patients with RA
– The analgesic effect of
dosulepin is INDEPENDENT
of its antidepressant effect
G. Ash et. al. The effect of dothiepin on subjects with rheumatoid arthritis and depression. Rheumatology 1999; 38: 959-967

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Recommendations of Treatment Guidelines

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Practice Guidelines for Chronic Pain Management
• Developed by American Society of Anesthesiologists Task Force on
Chronic Pain Management and the American Society of Regional
Anesthesia and Pain Medicine
• Meta-analyses of randomized controlled trials indicate that tricyclic
antidepressants provide effective pain relief for a variety of chronic
pain etiologies for assessment periods ranging from 2 to 8 weeks,
with dry mouth and somnolence or sedation as reported side effects
(Category A1 evidence).
• Strongly agree to use of TCAs in chronic pain management.
Anesthesiology 2010; 112:810 –33

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Take Homes !
Pain needs to be treated aggressively to
prevent sensitization
Chronic pain even more so as to combat Neuroplasticity
TCAs are the recommended first-line therapy in chronic pain
Dothiepin is better tolerated in relation
to its side effects than amitriptyline

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Thank you

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
Dedicated to my family for making everything worthwhile

Prothiaden in Chronic PainProthiaden in Chronic Pain Company Confidential © 2010 AbbottCompany Confidential © 2010 Abbott
THANKYOU
My sincere thanks to ABBOTT and SAMPATH(CRO)
My sincere thanks to ABBOTT and SAMPATH(CRO)
READ NOT TO CONTRADICT OR CONFUTENOR TO BELIEVE AND TAKE FOR GRANTEDBUT TO WEIGH AND CONSIDER