Embed Size (px)
Citation preview

Meningioma / craniopharyngioma/ Meningioma / craniopharyngioma/ High grade gliomaHigh grade glioma
Meningioma- Small recurrent / residual meningioma need to be treated with radiosurgery
- There is regression of tumour after high dose radiosurgery
- Usual dose for radiosurgery is 12-15 Gy in single fraction
Craniopharyngioma- Small craniopharyngioma > 4mm away from chiasm need radiosurgery
- Small para-sellar residual disease need radiosurgery
High grade glioma- Small residual / recurrent disease in well preserved patients may be treated with
radiosurgery
Fractionated radiosurgeryFractionated radiosurgeryExtended Indications for multiple fraction treatment
- Larger meningiomas (>3 cm)
- Larger acuastic schwannoma (>3 cm)
- Large solitary / oligo brain metastasis with controlled primary
- Larger residual LGG
- AVMs (>3 cm) - Chordomas
- Rec HCC
- Craniopharyngioma
- Pituitary tumour
Short term data with robotic [email protected]

New experiences with fSRSNew experiences with fSRS
Post-TreatmentPre-Treatment
- More necrosis with CK than SRT (25Gy/5# Vs 54Gy/30#)
- Difficult to have radiological interpretation
- Require longer duration of steroid
- Associated with more oedema [email protected]
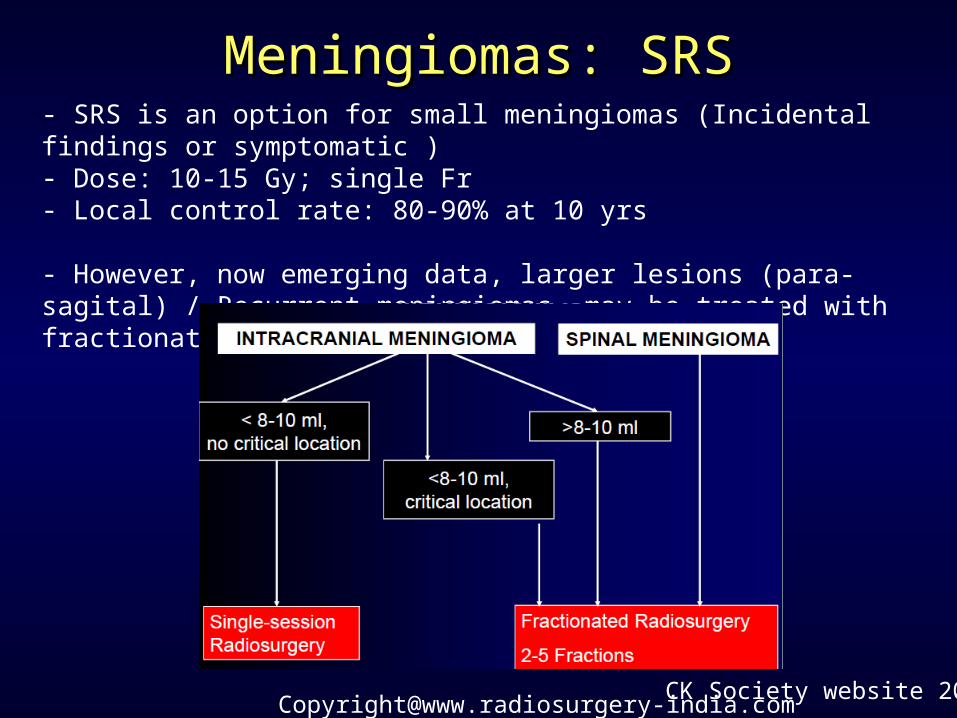
Meningiomas: SRSMeningiomas: SRS- SRS is an option for small meningiomas (Incidental findings or symptomatic )- Dose: 10-15 Gy; single Fr- Local control rate: 80-90% at 10 yrs
- However, now emerging data, larger lesions (para-sagital) / Recurrent meningiomas may be treated with fractionated approach
CK Society website [email protected]
CraniopharyngiomaCraniopharyngioma
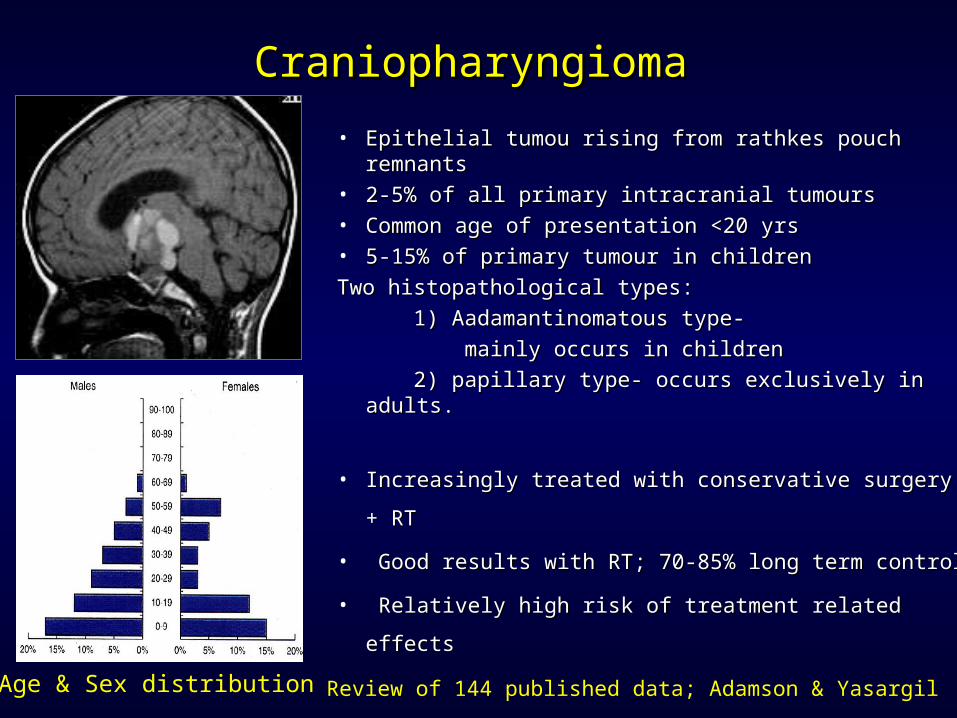
• Epithelial tumou rising from rathkes pouch remnantsEpithelial tumou rising from rathkes pouch remnants• 2-5% of all primary intracranial tumours2-5% of all primary intracranial tumours• Common age of presentation <20 yrsCommon age of presentation <20 yrs• 5-15% of primary tumour in children5-15% of primary tumour in childrenTwo histopathological types:Two histopathological types: 1) Aadamantinomatous type-1) Aadamantinomatous type- mainly occurs in children mainly occurs in children 2) papillary type- occurs exclusively in adults. 2) papillary type- occurs exclusively in adults.
• Increasingly treated with conservative surgery + RTIncreasingly treated with conservative surgery + RT
• Good results with RT; 70-85% long term controlGood results with RT; 70-85% long term control
• Relatively high risk of treatment related effectsRelatively high risk of treatment related effects
Age & Sex distribution Review of 144 published data; Adamson & Yasargil 2008
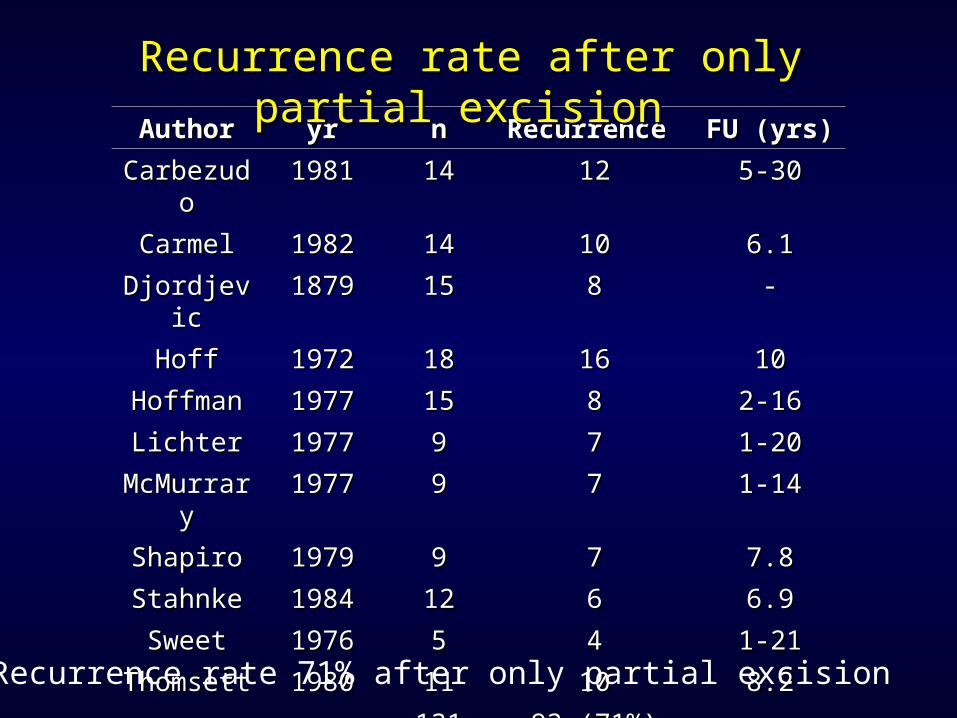
AuthorAuthor yryr nn Recurrence Recurrence FU (yrs)FU (yrs)
CarbezudoCarbezudo 19811981 1414 1212 5-305-30
CarmelCarmel 19821982 1414 1010 6.16.1
DjordjevicDjordjevic 18791879 1515 88 --
HoffHoff 19721972 1818 1616 1010
HoffmanHoffman 19771977 1515 88 2-162-16
LichterLichter 19771977 99 77 1-201-20
McMurraryMcMurrary 19771977 99 77 1-141-14
ShapiroShapiro 19791979 99 77 7.87.8
StahnkeStahnke 19841984 1212 66 6.96.9
SweetSweet 19761976 55 44 1-211-21
ThomsettThomsett 19801980 1111 1010 8.28.2
131131 93 (71%)93 (71%)
Recurrence rate 71% after only partial excision
Recurrence rate after only partial excision Recurrence rate after only partial excision
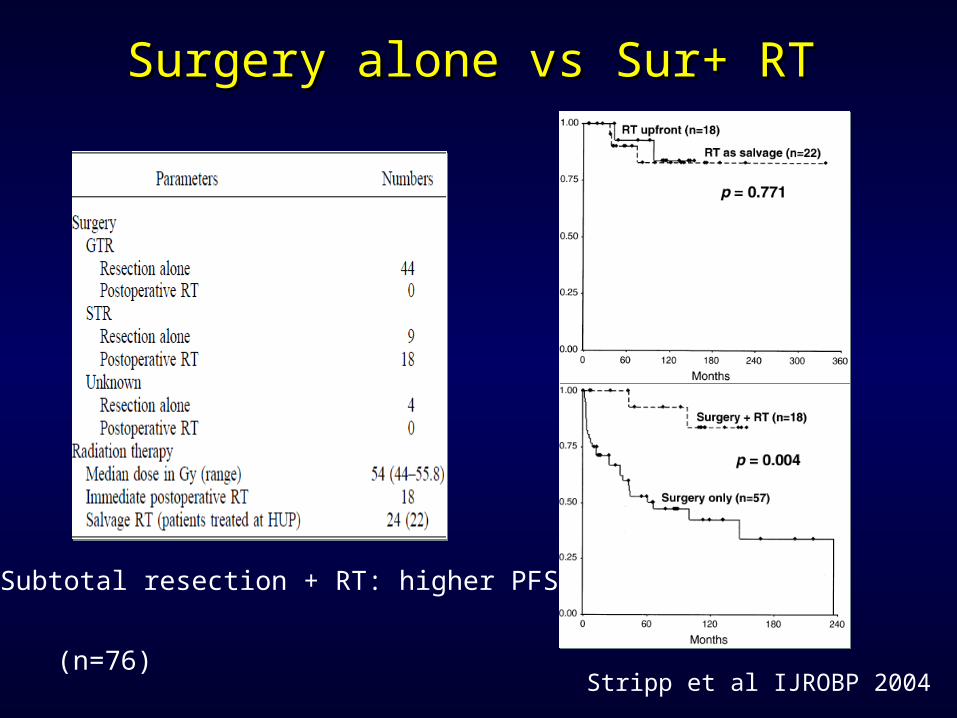
Surgery alone vs Sur+ RTSurgery alone vs Sur+ RT
Subtotal resection + RT: higher PFS
Stripp et al IJROBP 2004(n=76)
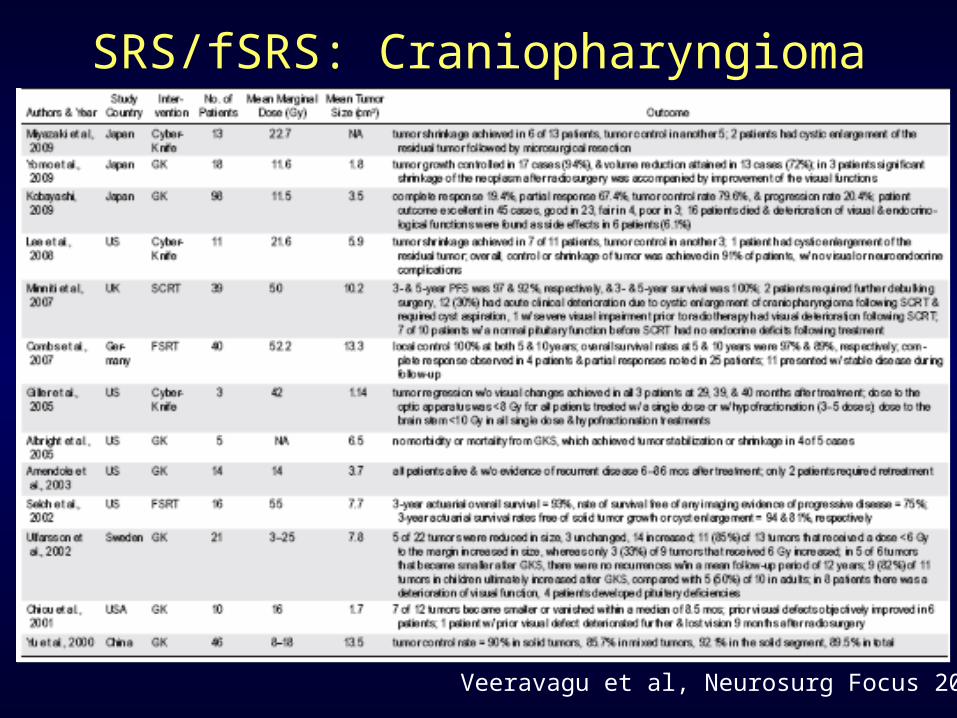
Veeravagu et al, Neurosurg Focus 2010
SRS/fSRS: Craniopharyngioma
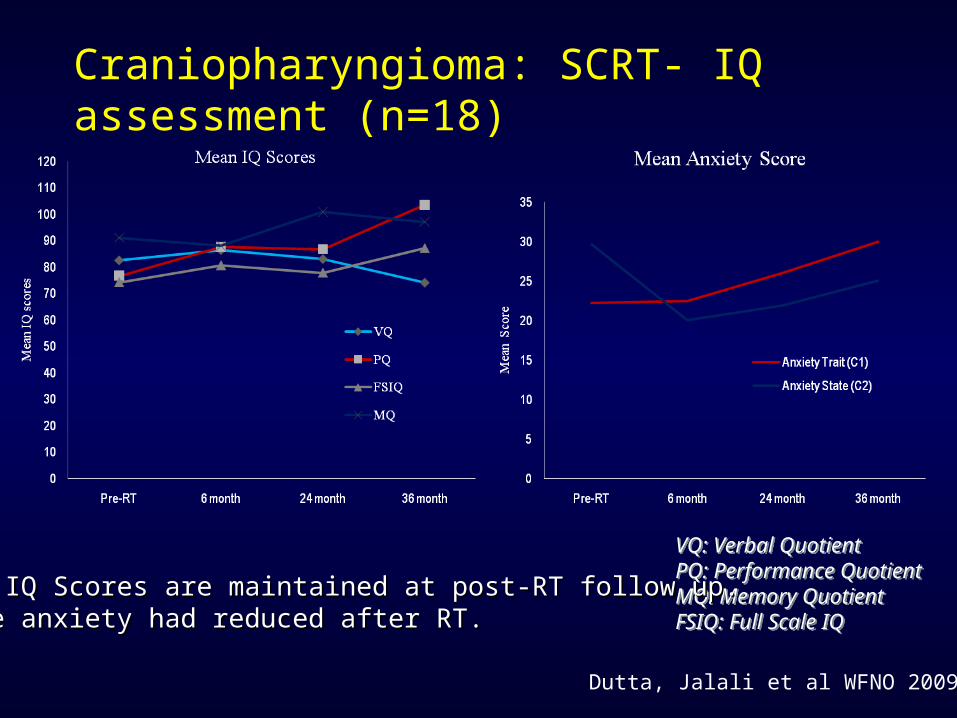
Craniopharyngioma: SCRT- IQ assessment (n=18)
VQ: Verbal QuotientPQ: Performance QuotientMQ: Memory QuotientFSIQ: Full Scale IQ
VQ: Verbal QuotientPQ: Performance QuotientMQ: Memory QuotientFSIQ: Full Scale IQ
• Mean IQ Scores are maintained at post-RT follow up.Mean IQ Scores are maintained at post-RT follow up.• State anxiety had reduced after RT.State anxiety had reduced after RT.
Dutta, Jalali et al WFNO 2009
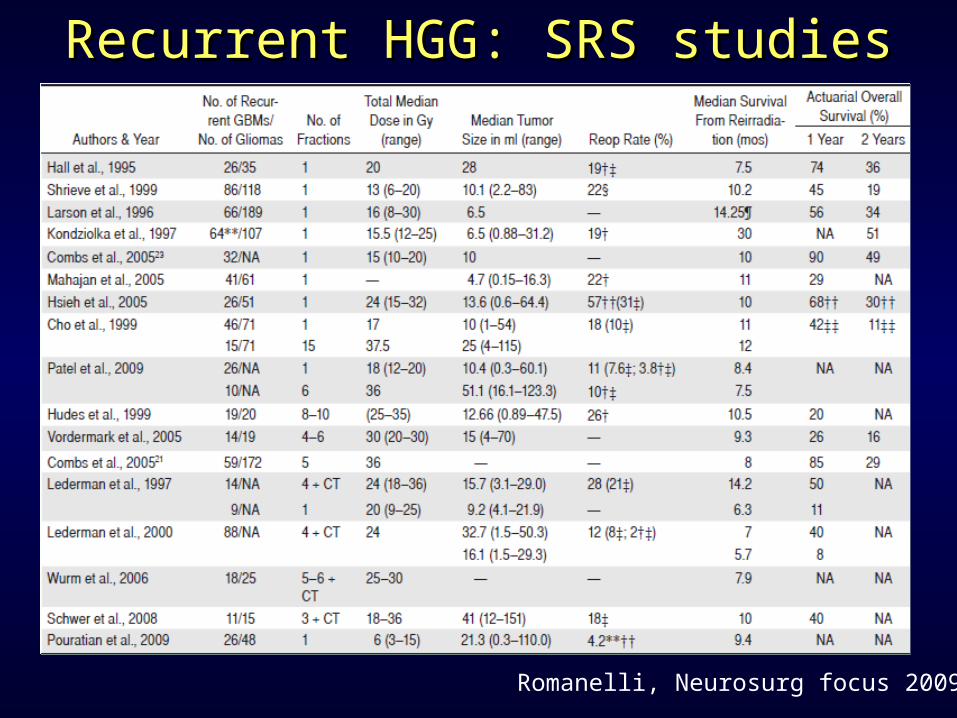
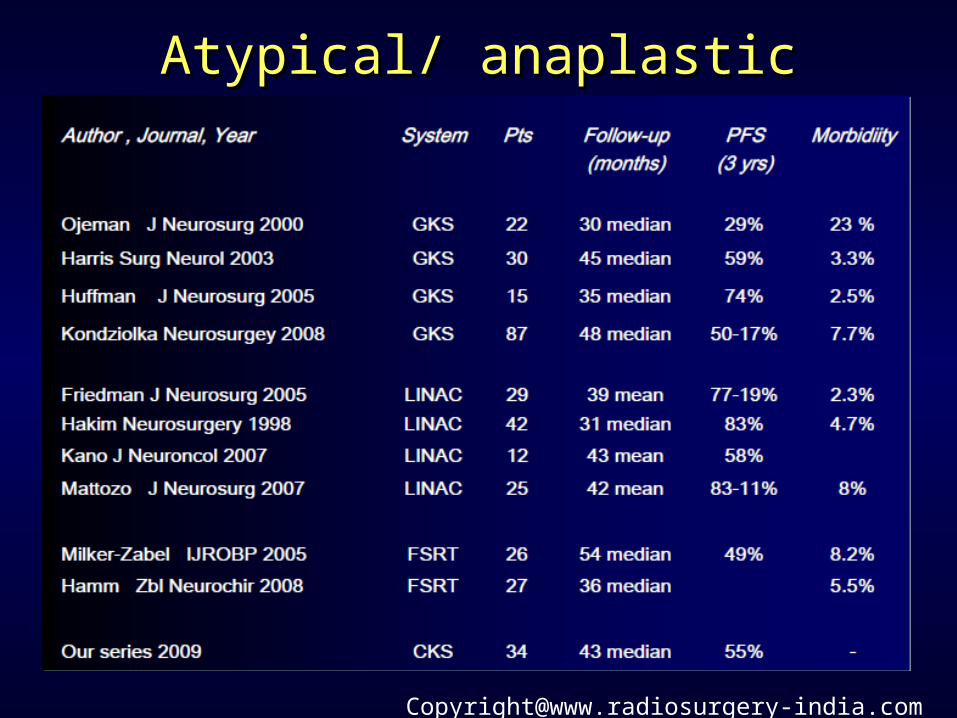
Recurrent HGG: SRS studiesRecurrent HGG: SRS studies
Romanelli, Neurosurg focus 2009
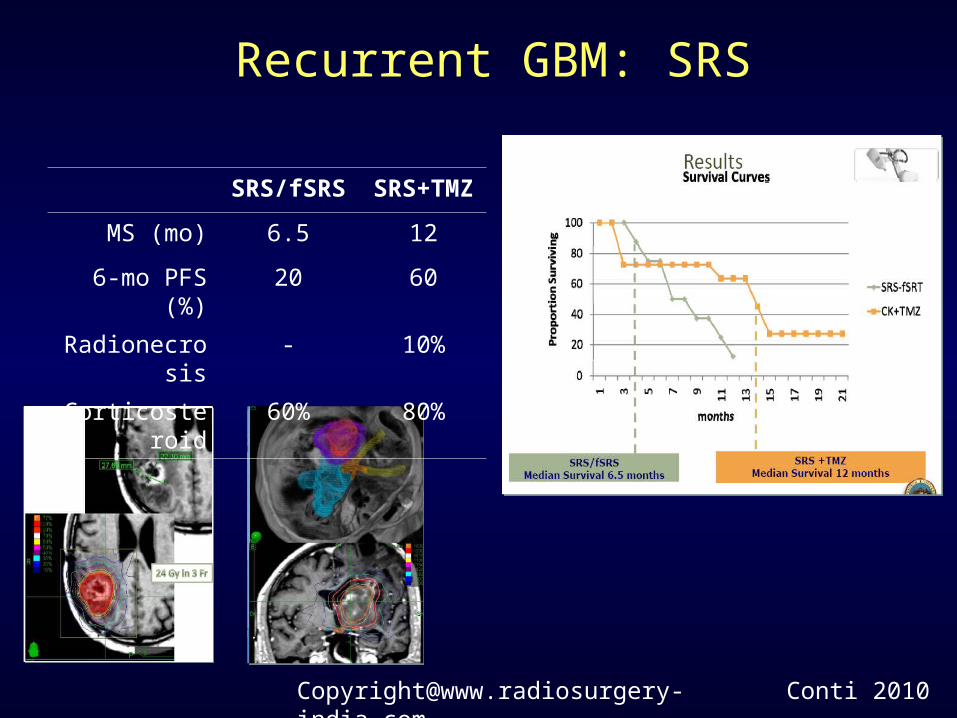
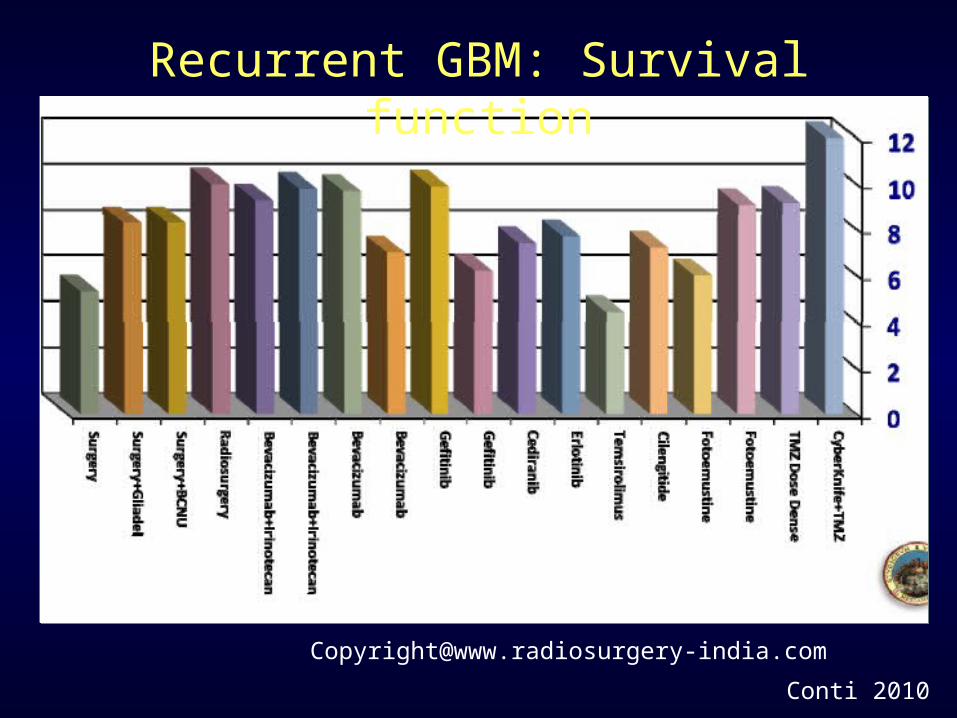
Recurrent GBM: SRS
Conti 2010
SRS/fSRS SRS+TMZ
MS (mo) 6.5 12
6-mo PFS (%) 20 60
Radionecrosis - 10%
Corticosteroid 60% 80%
New Indications for RadiosurgeryNew Indications for Radiosurgery
-Temporal lobe epilepsy
- Resistant seizure disorder
- Behavioral disorders
- Mood disorder
- Obesity
- Child hood attention deficit disorder / absence seizure
- Skull base tumour
Meningioma / craniopharyngioma/ Meningioma / craniopharyngioma/ High grade gliomaHigh grade glioma
Meningioma- Small recurrent / residual meningioma need to be treated with radiosurgery
- There is regression of tumour after high dose radiosurgery
- Usual dose for radiosurgery is 12-15 Gy in single fraction
Craniopharyngioma- Small craniopharyngioma > 4mm away from chiasm need radiosurgery
- Small para-sellar residual disease need radiosurgery
High grade glioma- Small residual / recurrent disease in well preserved patients may be treated with
radiosurgery