Embed Size (px)
Citation preview

Almost-Standard Gauge: Misadventures in Interoperability
Megan Douglas, JDAssociate Project Director, Health IT Policy
Morehouse School of Medicine
3rd Annual Policy Prescriptions SymposiumHouston, TX
June 11, 2016

The Following Presenters Have Disclosed Relevant Financial Relationships:Cedric Dark, MD MPH FAAEM FACEPCommunity Health Choice, Event Sponsorship; Schumacher Clinical Partners, Event Sponsorship Seth Trueger, MD MPHEmergency Physicians Monthly, Employee, Salary The Following Presenters Have Disclosed No Financial Relationships:Megan Douglas, JDElena M. Marks, JD MPHLaura Medford-Davis, MDBich-May Nguyen, MD MPH The Following Planners Have Disclosed Relevant Financial Relationships:Cedric Dark, MD MPH FAAEM FACEPCommunity Health Choice, Event Sponsorship; Schumacher Clinical Partners, Event Sponsorship The Following Planning Committee Members and Staff Have Disclosed No Relevant Financial Relationships:Emily DeVillers, CAEKay Whalen, MBA CAEJanet Wilson, CAE

The project described was supported by the National Institute on Minority Health and Health Disparities (NIMHD) Grant Number U54MD008173, a component of the National Institutes of Health (NIH) and Its contents are solely the responsibility of the authors and do not necessarily represent the official views of NIMHD or NIH.
Official Statement

Learning Objectives
• Define interoperability as distinguished from health information exchange
• Describe the current status of interoperability at a national level
• Assess organizational and policy barriers and facilitators to interoperability

Setting the Stage
• No Matter Where– https://www.youtube.com/watch?v=qMurGr623Ms
• Ideal vs. Reality• Evolution, NOT revolution

DEFINITIONS

Health Information Exchange (HIE*)
Ability of two or more health information systems to exchange clinical information to provide access to
longitudinal information
*Not to be confused with HIE (governance entities that facilitate HIE)

HIE (the concept)
Three types of HIE:• Directed exchange: ability to send &
receive secure information electronically between care providers
• Query-based exchange: ability for providers to find and/or request information on a patient from other providers
• Consumer-mediated exchange: ability for patients to aggregate and control the use of their health information among providers
Mr. Jones has an appointment with the cardiologist on
Friday. Here are his latest test results.
Has Mr. Jones been to the ED for his asthma lately?
Mr. Jones has been monitoring his blood sugar for the last 30 days. He has
submitted his reports through the patient portal.

HIE (Governance entities)• State, regional, system-based
– Every state has different strategy/model
– Public, private, public-private partnership
• Direct participation vs. network of networks
• Services offered– DIRECT messaging (HIPAA-
compliant e-mail)– Query-based searches– Automatic notifications
• Distinguish between adoption & utilization– How much data is actually flowing?

Interoperability
Ability of a system to exchange electronic health information with & use electronic health information from other systems without special effort by the user
-Institute of Electrical and Electronics Engineers (IEEE) https://www.ieee.org/education_careers/education/standards/standards_glossary.html
Includes concepts of: standardization (transport + vocabulary/terminology), integration, cooperation, and
technical specifications
Bottom line: Integration is automated & actionable
Basic Advanced

Interoperability vs HIE• Electronic Health Record (EHR) is necessary for
electronic HIE• HIE is necessary for interoperability• HIE is not sufficient by itself to achieve
interoperability
EHR Adoption
Health Information Exchange
Interoperability

Electronic Health Record
Clin
ical
Dec
isio
n
Health Information Exchange
AdvancedInteroperability
BasicInteroperability
Clinical Care
Document (CCD)

STATUS

The Interoperability Unicorn“Many have heard about it, but few have seen it”

Numbers...?
• We don’t know how many providers have “interoperable” systems
• But we do know:

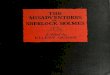
Proportion of physicians who reported electronically sharing health information, 2013 and 2014
SOURCE: 2013 and 2014 National Electronic Health Record Surveys; HealthIT.govhttp://dashboard.healthit.gov/evaluations/data-briefs/physician-electronic-exchange-patient-health-information.php

Proportion of physicians who electronically shared any patient health information with other providers, 2014
SOURCE: 2013 and 2014 National Electronic Health Record Surveys; HealthIT.govhttp://dashboard.healthit.gov/evaluations/data-briefs/physician-electronic-exchange-patient-health-information.php

Transitions with a Summary of Care Record
http://dashboard.healthit.gov/quickstats/pages/eligible-provider-electronic-hie-performance.php

Percent of non-federal acute care hospitals that electronically exchanged with providers outside their organization: 2008-2014.

Clinical care summary exchange among hospitals and outside providers between 2010 and 2014.

Percent of U.S. Hospitals that Routinely Electronically Notify Patient's Primary Care Provider upon Emergency Room Entry
HealthIT.gov Dashboard - http://dashboard.healthit.gov/quickstats/pages/FIG-Hospital-Routine-Electronic-Notification.php

BARRIERS & FACILITATORS TO INTEROPERABILITY

Why is interoperability so hard?
Technical?Business?Moral?

Moral
For the “public good”– Increases efficiency– Reduces costs to the system– Patients prefer record sharing– Improves care coordination– Improves health outcomes– Improve population health
Privacy/security– Data breaches

Technical• Many transactions
– A single EHR system at one large hospital (the Mayo Clinic in Rochester, Minnesota) processes over 660 million HL7 messages a year, or about 2 million messages a day
Benson, T. (2012). Principles of Health Interoperability HL7 and SNOMED. Available at http://www.springer.com/gp/book/9781447128007.
• Many data sources– Clinical health records (primary care, specialty, hospital)– Billing (payment information and history)– Patient-generated health data– Pharmacy and prescription information– Patient and family-health history– Genomics– Clinical-trial data
• Many languages– EHR systems and clinical systems use different language to describe the same
piece of data (ex: sex/gender; female/woman; heart attack/myocardial infarction)
BUT NOT THE BIGGEST BARRIER!

Business (aka )
• “It is usually in each vendor’s financial self-interest to provide a proprietary nonstandard interface to a customer, even though they know well that this is ultimately creating an interoperability nightmare”
Benson, T. (2012). Principles of Health Interoperability HL7 and SNOMED. Available at http://www.springer.com/gp/book/9781447128007.
• Patient “ownership” – system competition• Data ownership• Inadequate ROI/business case• Liability
– Data protection – chain of custody (“typically addressed in layers of complex legal agreements between vendors and healthcare facilities”)
Munro, D. The Healthcare IT Quote Of 2015. Available at http://healthstandards.com/blog/2015/12/01/quote-of-2015/.

State Initiatives
• Laws– North Carolina Session Law 2015-241 s. 12A.4 and 12A.5
• As of February 1, 2018, all Medicaid providers must be connected to the HIE in order to continue to receive payments for Medicaid services provided. By June 1, 2018, all other entities that receive state funds for the provision of health services, including local management entities/managed care organizations, also must be connected
• Funding– ONC has 56 cooperative agreements with
states/territories• Governance

• Public-private partnership– Texas Health Services Authority (THSA) partnered with
InterSystems in 2013• Network of networks (favored, not mandatory)• Services
– Clinical Document Exchange (Treatment)– Federated Trust Framework (Security/Confidentiality/Accuracy)– Patient Consent Management (opt-in or opt-out)– eHealth Exchange
• Fees (based on size of HIE)– Implementation fee: $20-$130k– Annual fee: $15-$110k

• State HIN, public-private partnership
• Network of networks• Members
– Payers– State agencies– Regional HIEs
• Services– Direct messaging– Query-based record
retrieval
• Mission-based Service Area HIE– Focus on small, rural
providers, practices, hospitals
• Services– Query-based record
retrieval– Direct messaging– Medication management– Quality performance
dashboard

Federal Initiatives
~$30 billion over 6 years

MACRA – Quality Payment Program
Current Volume-Based System
• Fee for Service• Provider revenue increases
with number of services performed
MACRA’s Value-Based System• Payments to providers will
vary based on factors like:– Quality measures met– Participation in APMs– Resource use– Clinical practice improvements
• Payments will be linked to quality and value – and will increase/decrease with performance

Merit-Based Incentive Payment System (MIPS) Proposed Rule• Meaningful Use Advancing Care Information• 25% of Composite Performance Score (Quality,
Resource Use, Clinical Practice Improvement Activities)
• Focus on Patient Electronic Access, Coordination of Care through Patient Engagement, Health Information Exchange
• Bonus for submitting clinical quality measures (CQM) electronically

Health IT is in its...