Embed Size (px)
Citation preview

MODERN APPROACH to the CESAREAN SECTION
TECHNIQUE(Evidence Based)
Agus Sulistyono

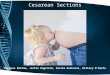
GENERAL PROCEDUREPreparation, IndicationAssessment of presenting part, FHRAnasthesia regional vs generalIdentification of incision site
TransverseVertical
Opening cavum abdomensharp blunt

GENERAL PROCEDURE
Uterine incisionTransverse - Low segmenLongitudinal – low, high
Rupturing amnionic sacDelivery the babyCutting umbilical cordRemoving placenta
manual vs gentle traction

Suturing uterine incisionexterioritazion vs intra abdomen1 vs 2 layer suture
Closing cavum abdomenperitoneum suturing vs non suturingrectus sheath Subcutan tissue suturing vs not
Skin closingsub cuticuler vs interupted
GENERAL PROCEDURE

- Access to anticipated pathology
- provide adequate exposure
- allow for extension
CHOICE OF INCISION
- interfere minimally with abdominal wall function - preserving important abdominal structures
- heal with adequate strength - reduce the risk of wound disruption - subsequent incisional hernia.

Considerations in selecting the
incision :Need for rapid entry
Certainty of the diagnosis
Body habitus
Location of previous scars
Potential for significant bleeding
Cosmetic outcome




TRANSVERSE VERTICAL
Rapid Better
Exposure Better
Wound strength Better
Adhesion formation Lower
Postop bowel obstruction Lower
Pain Less
Bleeding Less
Nerve injury Less
Impact on pulmonary function Less
Cosmetic Better
Wylie,BJ et al, Obstet Gynecol,2010; Brown SR, et al. Cochrane Database Syst Rev,2005
INCISION TYPE

SKIN INCISION
SIZE OF INCISION
Adequate for delivery of the fetus less traumatic allow delivery term fetus ± 15 cm
Adequate exposure stretch manually apart opening the
incisions angles
Scalpel vs electro-cauter no RCT prefer scalpel (either approach is acceptable)


DISSECTION of SUB-CUTAN TISSUES
Prefer blunt than sharp dissection (no RCT datas) quicker less injury to vessels (bleeding)
FASCIAL LAYER
Transverse incision & extended laterally - with scissors (Pfannenstiel)- with fingers bluntly (Joel-Cohen / Misgav-Ladach)

SUBCUTANEUS TISSUES

OPENING PERITONEUMBLUNT (FINGER) VS SHARP (PINCET & SCISSORS)
- data RCT not significant different in morbidity & mortalityBlunt (theoretical)minimize risk of injury to bowel, bladder or other
organ that addherent to peritoneumDense intra-peritoneal adhesions bluntly opening to upper abdomen (avoid dense area/scar
tissue) sharply opening cautiously using shallow incisions direct vision

TRANSVERSE vs VERTICAL no RCT principle : the incision ~ all atraumatic fetus
delivery FACTORS : fetus (EFW, position) placental location presence of myoma development of LUS
OPENING PERITONEUM


INTRA ABDOMINAL PROCEDURES
BLADDER FLAP Undergo bladder flap vs no bladder flap no RCTmorbidity (bladder injury ) ~
NO BLADDER FLAP quicker less bleeding
BLADDER FLAP
fetal head deep in the pelvis bladder attached above LUS (post SC) LUS not formed (not in labor)

HYSTEROTOMY
Be aware : placental location (avoid
laceration) fetal lie (delivery the fetus)head deep in the pelvis prolonged labor & head deep
in the pelvis avoid incision too low LUSmay transect Cx / vagina

Uterine Incisions
Kerr Incision vs Sellheim Incision vs Classical

TRANSVERSE INCISION : recommend for most SC LUS less blood loss less bladder dissection easier reapproximation lower risk rupture in VBAC RISK of laceration of major blood
vessel (extended) problematic if required larger
incision


INDICATIONS OF CLASSICAL CAESAREAN SECTION
1. when the LUS is abnormally vascular.
2. when the LUS can not identified due to adhesion.
3. Cases needs rapid delivery.
4. When the fetus lie is transverse and can not be corrected.
5. When hysterectomy will follow caesarean section
6. Poorly developed LUS when more than normal intra-ut manipulation is anticipated
7. LUS pathology (myoma, PPT anterior or accreta)
8. Post-mortem delivery

Advantages of the lower segment:
• The wound is extra peritoneal so less risk of infection.
• Healing scar is better.
• The risk of rupture of the scar is less.
• Hemorrhage is less.
• Placenta is away from the incision.
• Easier reapproximation
• Less need bladder dissection

DISADVANTAGES OF THE LOWER SEGMENT:
The operation requires more skill and experience.
The incision may extend down to the bladder.
Lateral extension risk laceration major blood
vessels
J or T incision: if need large incision weaker scar
DISADVANTAGES OF CLASSICAL OPERATION:
More liable to chest infection.
More liable to intestinal distension.
The scar is more liable to rupture (next pregnancy).

• HYSTEROTOMY EXPANSION
Blunt (finger) vs sharp (scissors) Extended the incisionBlunt :
- Fast- less risk trauma to fetus- less blood loss, lower drop in Hb and HCT
postpartum - less risk of unintended extension (RR 0,47;
95%CI 0,28-0,79)

BLUNT HYSTEROTOMY EXPANSION

FETAL EXTRACTI-
ON

CORD CLAMP
Early Cord Clamping
Delayed Cord Clamping
Milking Cord

PLACENTAL EXTRACTION
DRAIN vs NOT DRAIN umbilical cord before placental extracrion :
Drain less fetomaternal transfusiononly small trial
GENTLE TRACTION vs MANUAL EXTRACTION :MANUAL EXTRACTION :
Endometritis post-partum > (RR 1,64 95%CI 1,42-1,90)
blood loss > (mean difference 94 mL, 95%CI 17-172mL)
blood loss > 1000mL > (RR 1,81 95%CI 1,11-2,28)lower postpartum Hematocrit
Cavum uteri : wiped with gausge sponge - remove remaining membrane- stimulate uterine contraction


EXTERIORIZING vs INSITU UTERINE REPAIR
EXTERIORIZING
improve uterus exposure
facilitate closure uf hysterotomy
shorter time
Post-op nausea & vomiting
other complication ~

UTERINE EXTERIORIZING

CERVICAL CANAL
Routine manual/instrumental Cxdilatation
- unnecessary both labor or not laboring- Hb post-op ~- fever ~- wound infection ~

SUTURING
Choice of suturing ~ personal preferenceChromic catgut vs delayed absorbable not difference in maternal outcome
Chromic, monofilament (monocryl), braided (vicryl),
LOCKED vs UNLOCKED CLOSURELOCKED SUTURE:
scar weakness >thinner myometrialbell shaped wall defect dehiscence / rupture >
but data are limited

PARAMETER LUS CLOSURE
SINGLE DOUBLE
Operative time Less 6’ shorter
Endometritis ~ ~
Wound infection ~ ~
Blood transfusion ~ `
Thick LUS better
Uterine rupture (next pregnancy)
4,8% 2,9% Not significant
Risk bladder adhesion
> Need furtherstudy
SINGLE vs DOUBLE LUS CLOSURE(20 STUDY INCLUDING 15.000 PATIENTS)

ABDOMINAL IRRIGATION
maternal infection : not reduced
Increased intra-op nausea
estimated blood loss ~
operating time >
hospital stay ~
return GIT function ~

PERITONEUMCLOSURE vs NON CLOSURE (533 women)NON CLOSURE :
decreased operating time (± 6’)on repeat CS
adhesion ~time incision – delivery ~

NON CLOSURE PERITONEUM
Less time
Less post operative fever
Less post operative analgetics
Less wound infection
Less of length of hospital stay

RECTUS MUSCLES
Reapproximate naturally
Not need suturing
SUTURING :
increased pain (first start moving)
decreased dense adhesion formation

FASCIA :the most wound strengthavoid to much tension since approximationnot strangulation
MIDLINE FASCIAL INCISION :- simple running technique- no 1 or 2 delayed absorbable monofilamen- mass closure, all laye of the abdominal wall- wide tissue bites (≥ 1 cm)- short stitch interval (≤ 1 cm)- non strangulation tension suture
TRANSVERSE INCISION :- continuous closure - slow absorbable no 0 or 1 braided suture


SUBCUTANEUS TISSUE
Not need irrigationClosing with interrupted delayed absorbable
if subcutaneous layer ≥ 2 cminhibit blood and serum accumulation
WOUND DRAINAGE routine use not beneficialnot reduce :
seromahematomainfectionwound disruption

SKIN
STAPLE vs SUBCUTICULER SUTURE
STAPLE :
increase infection and separation
shortening operating time (only few
minutes)
post-op discomfort >
cosmetic appearance ~

PFANNENSTIEL PELOSI-TYPE JOEL-COHEN MISGAV-LADACH
Incision Pfannenstiel Pfannenstiel Joel-Cohen Joel-Cohen
Sub-cutan tissue Electro cauter Open 3 cm Open 3 cm
Fascia dissection Transverse, sharp Electro-cauter Transverse, blunt lateral extended
Transverse, sharp (semi open scissors)
Rectus musledissection
sharp Blunt Blunt Blunt
Peritoneal opening
Longitudinal, sharp
Blunt (finger & all layer stretched manually
Blunt (finger & all layer stretched manually
Blunt (finger & all layer stretched manually
Reflected bladder inferiorly
(+) (-) (+) (-)
SUMMARY

PFANNENSTIEL PELOSI-TYPE JOEL-COHEN MISGAV-LADACH
Uterine opening Transverse LUS Transverse LUS, blunt lateral extended
Transverse LUS, blunt lateral extended
Transverse LUS, blunt lateral extended
Uterine closing 2 layers, continuous
Single layer continuous locking
Interrupted sutures
Single layer locking sutures (exteriorization)
Peritoneal suturing (+) (-) (-) (-)
Fascia suturing Continuous /interupted
Continuous non locking
Continuous non locking
Continuous non locking
Sub-cutan layer suturing
(+) (+) in thick (>2 cm)
(-)
Skin Continuous /interupted
Staples 2-3 mattressutures
Others Placenta removed manuallyAllis clamp (5’)

RECOMMENDATION
Procedure Type of Preocedure GradeIncision abdominal wall Transverse 2 C
Skin incision Scalpel ~ cauter Personal preference
Open peritoneum Blunt -
Bladder flap No -
Hysterotomy Transverse 2 C
Expansion hysterotomy Blunt 2 B
Placental extraction Spontaneous 1 A
Uterus exteriorization Both acceptable Personal preference
Uterine closure 2 layer (if VBAC in next pregnancy)
2 C
Closing peritoneum Not closing 2 B
Subcutan tissue closure Closure (if s.c. tissue ≥ 2 cm) 1 A
Skin closure Subcuticular suture 2 C