Embed Size (px)
Citation preview

MYOMA AND
PREGNANCY

Nomenclature
Fibroid--------Fibroids
Myoma--------Myomata
Fibromyoma—Fibromyomata
Leiomyoma---Leiomyomata

Fibroids (leiomyomas) are benign smooth
muscle cell tumors of the uterus.
Although they are extremely common,
with an overall incidence of 40% to 60%
by age 35 and 70% to 80% by age 50, the
precise etiology of uterine fibroids
remains unclear.

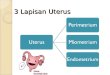
Described based on location in theuterus: Intramural: develop from withinuterine wall, do not distort uterinecavity, <50% protruding into serosalsurface
Submucosal: develop from myometrialcells just below endometrium, oftenprotrude into and distort uterine cavity

Subserosal: originate from serosalsurface of uterus, >50% protrudesout of serosal surface
Cervical: located in the cervix,rather than uterine corpus





The diagnosis of fibroids in
pregnancy is neither simple nor
straightforward. Only 42% of large
fibroids ( 5 cm) and 12.5% of
smaller fibroids (3-5 cm) can be
diagnosed on physical examination.

The ability of ultrasound to detect
fibroids in pregnancy is even more
limited (1.4%-2.7%) primarily due to the
difficulty of differentiating fibroids from
physiologic thickening of the
myometrium.


Reflecting the growing trend of
delayed childbearing, the incidence
of fibroids in older women
undergoing treatment for infertility is
reportedly 12% to 25%.
Despite their growing prevalence,
the relationship between uterine
fibroids and adverse pregnancy
outcome is not clearly understood.

the majority of fibroids (60%-78%) do
not demonstrate any significant change
in volume during pregnancy.
22% to 32% of fibroids increase in
volume & the growth was limited almost
exclusively to the first trimester,
especially the first 10 weeks of
gestation.

In the second trimester, small fibroids
grow whereas large fibroids (> 6cm)
remain unchanged or decrease in size
but all decrease in size in the third
trimester.
The majority of fibroids show no
change during the puerperium,
although 7.8% will decrease in volume
by up to 10%.

Pain
Pregnancy loss
Preterm labor and
birth
Placental
abruption
Placenta previa
PPH
Dysfunctional
labor
Malpresentation
Malposition
Cesarean delivery

The risk and type of complication appear to be
related to the: 1. Size, 2. Number, and 3. Location of the myomas.

If the placenta implants over or in close proximity to a myoma, there may be an increased risk of:
1. Miscarriage.2. Preterm labour.3. Abruption. 4. Prelabour rupture of membranes.5. Intrauterine growth restriction.


Fibroids located in the lower uterine segment may increase the likelihood of :
1. Fetal malpresentation,
2. Caesarean section, and
3. Postpartum hemorrhage.

American Journal of Obstetrics & Gynecology, Vol. 198, PC Klatsky et al, “Fibroids and
reproductive outcomes: a systematic literature review from conception to delivery," pp. 357-
366.

Most common
complication.
Causes
Red degeneration.
Tortion.
Impaction.

Theories.
rapid fibroid growth results in the tissue
outgrowing its blood supply
change in the architecture (kinking) of
the blood supply to the fibroid leading
to ischemia and necrosis
the pain results from the release of
prostaglandins from cellular damage
within the fibroid.

Multiple fibroid increase risk.
Submucosal or interstitial.
Unclear mechanism??
Increase uterine contractility.
Compressive effect.
Affection of blood supply to
developing placenta.

More common if the placenta
implants close to the fibroid.

Evidence not consistent across the
literature
Increased risk if placenta is adjacent to
or overlies a fibroid
Decreased oxytocinase activity higher
oxytocin levels premature contractions .
Fibroid uteri are less distensible, once
uterus grows to a certain point
contractions.

Conflicting evidence
Submucosal, retroplacental & volumes
> 200 cm3 are independent.
Abnormal placental perfusion:
decreased blood flow to endometrium
overlying fibroid placental ischemia,
decidual necrosis abruption (?)

Placenta previa is a less common
outcome and was positively
associated with fibroids in 2
studies (Qidwai IG et al 2006,
Vergani P et al 2007 ).
Two other studies found no
association with placenta previa,
making this association difficult
to ascribe to fibroids as
advanced maternal age and prior
uterine surgery were not
considered (Coronado GD et al
2000, Vergani P et al 1994)

Although cumulative data and a
population-based study suggested
that women with fibroids are at
slightly increased risk of delivering a
growth-restricted infant, these
results were not adjusted for
maternal age or gestational age.

Rarely, large fibroids can compress
and distort the intrauterine cavity
leading to fetal deformities.
A number of fetal anomalies have
been reported in women with large
submucosal fibroids, including
dolichocephaly , torticollis and limb
reduction defects. (Chuang J et al 2001)


Increases risk 13% vs
4.5%. (Klatsky PC et al
2008)
Risk factors :
Large fibroids.
Multiple fibroids.
Fibroids in the lower
uterine segment

Greater risk: retroplacental or
cesarean delivery.
Decreased force and coordination of
contractions uterine atony
Be prepared.

Retained placenta was more common in
women with fibroids, but only if the
fibroid was located in the lower uterine
segment.

Varying evidence
Decreased force of contractions
Asymmetric wave of contractile
force across uterus

Consistent evidence.
48.8% versus 13.3%.(Klatsky PC et al 2008)
Location in lower
uterine segment due
to higher risk of
malpresentation,
dysfunctional labor &
abruption.

Despite the increased risk of
cesarean, the presence of
uterine fibroids—even large
fibroids —should not be regarded
as a contraindication to a trial of
labor.


Rare.
However, several studies have reported that
antepartum myomectomy can be safely
performed in the first and second trimester
of pregnancy.
Acceptable indications include intractable
pain from a degenerating fibroid or from
tortion.

Obstetric and neonatal outcomes in
women undergoing myomectomy in
pregnancy are comparable with that
in conservatively managed women
except increasing rate of C.S. (De
Carolis S et al 2001, Celik C et al
2002)


Well-substantiated risk of severe
hemorrhage requiring blood
transfusion, uterine artery ligation,
and/or puerperal Hysterectomy.
It should only be performed if
unavoidable to facilitate safe delivery
of the fetus or closure of the
hysterotomy. Pedunculated subserosal
fibroids can also be safely removed.


Myomectomy remains the standard of
care for treating symptomatic fibroids
in women desiring fertility & this item
regard as relative contraindication of
uterine artery embolization.
Nevertheless, successful pregnancies
have been reported.

the outcomes of pregnancies suggest a
modest trend toward increasing risk of
preterm delivery, postpartum hemorrhage,
and abnormal placentation.
Sixty eight percent of the patients
underwent C.S.; however, the majority of
these cesareans were elective without a
trial of labor.
(Walker WJ et al 2006, Pron G et al 2005)