Embed Size (px)
Citation preview
Dr.A.GANESH BALA M.S ENT
ASSOCIATE PROFESSORVMMC - KARAIKAL
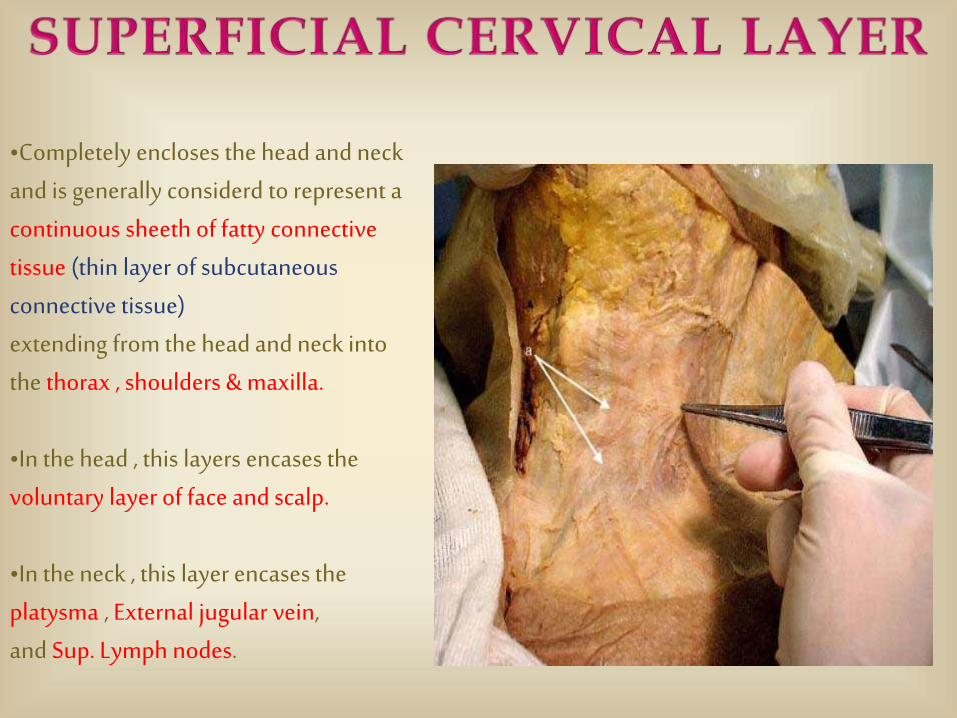
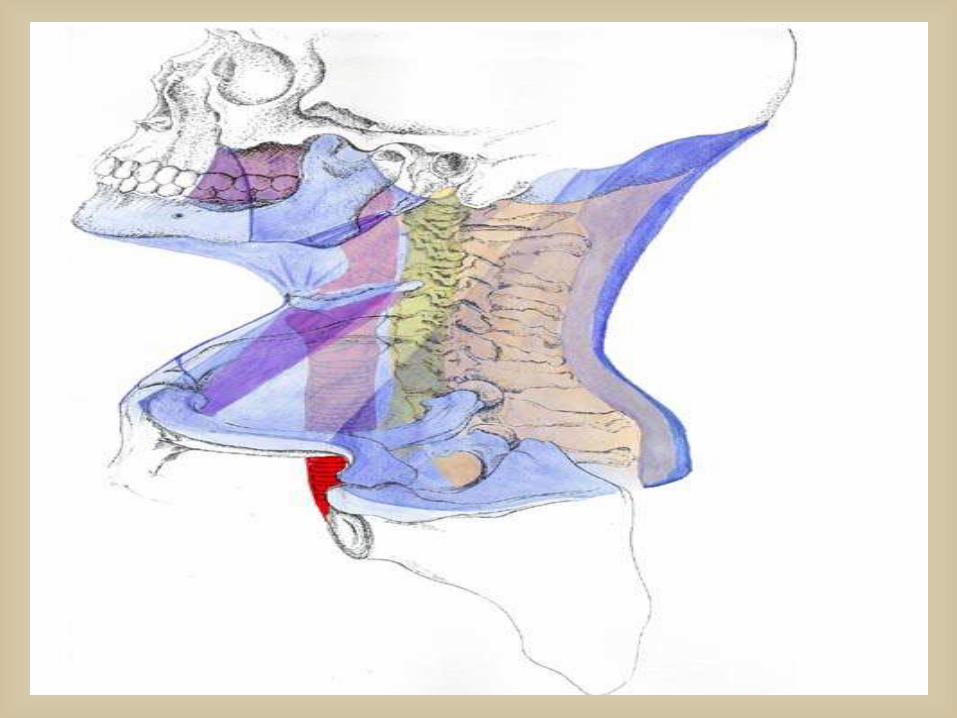
•Completely encloses the head and neckand is generally considerd to represent a continuous sheeth of fatty connective tissue (thin layer of subcutaneous connective tissue) extending from the head and neck into the thorax , shoulders & maxilla.
•In the head , this layers encases the voluntary layer of face and scalp.
•In the neck , this layer encases the platysma , External jugular vein,and Sup. Lymph nodes.
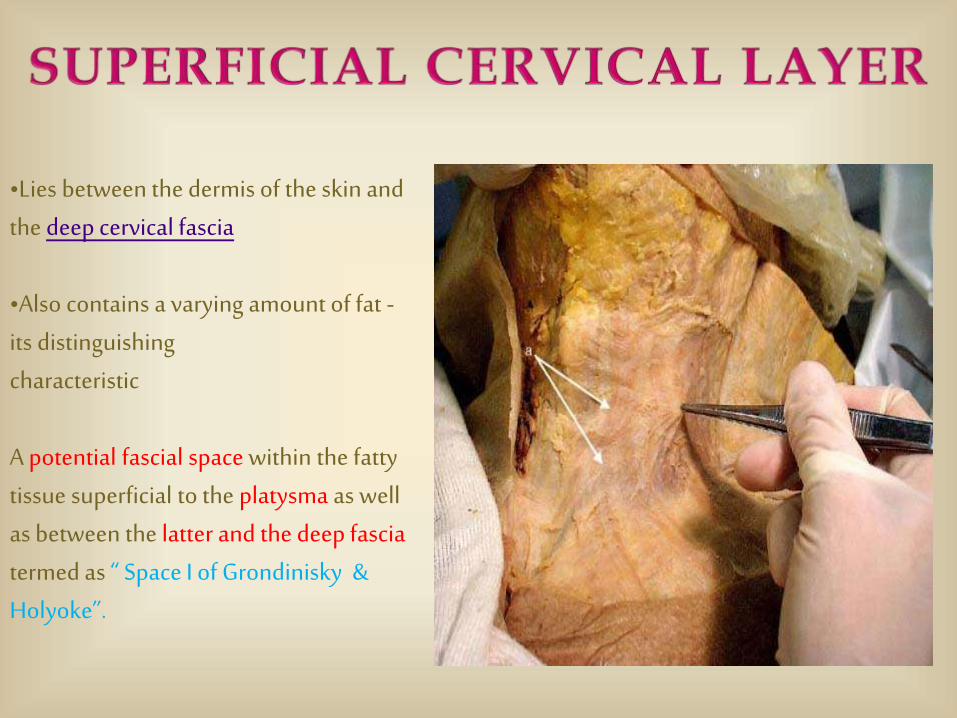
•Lies between the dermis of the skin and the deep cervical fascia
•Also contains a varying amount of fat -its distinguishing characteristic
A potential fascial space within the fatty tissue superficial to the platysma as well as between the latter and the deep fascia termed as “ Space I of Grondinisky & Holyoke”.
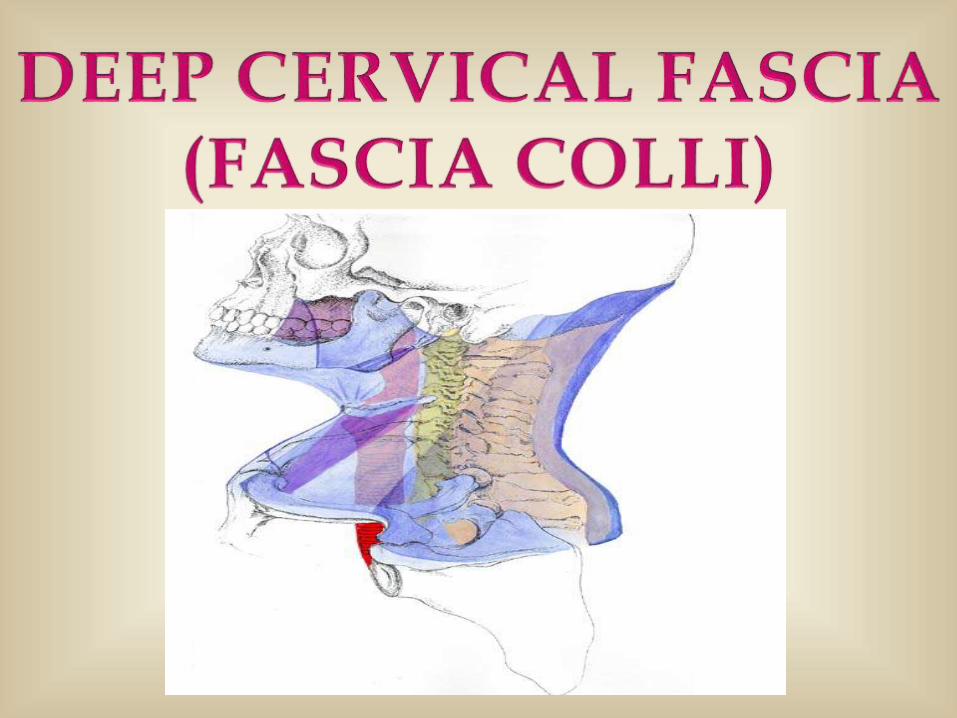
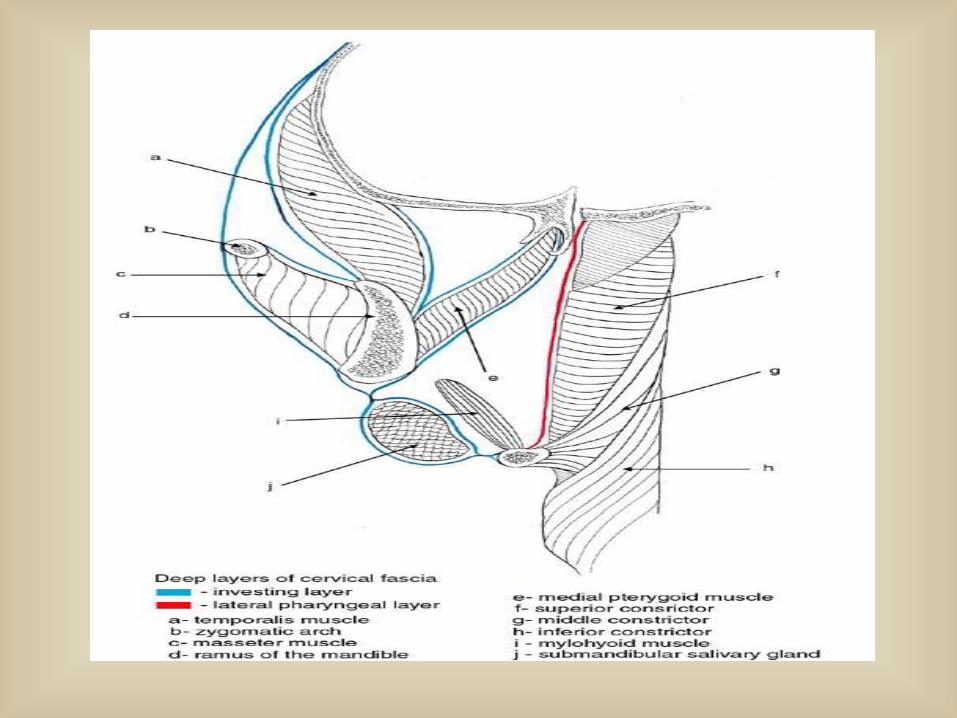
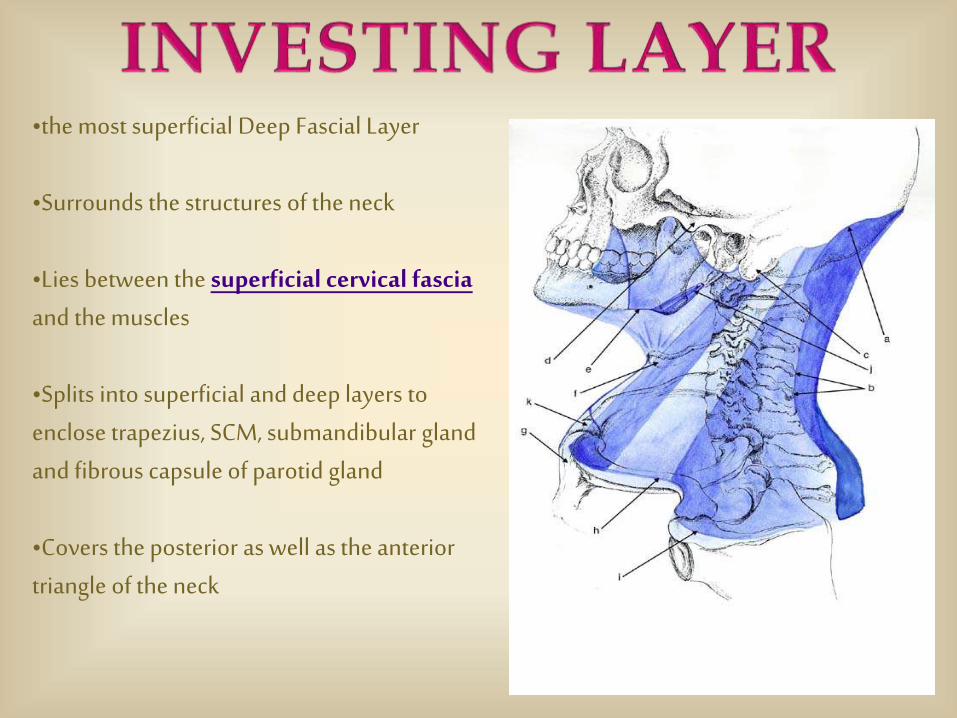
•the most superficial Deep Fascial Layer
•Surrounds the structures of the neck
•Lies between the superficial cervical fasciaand the muscles
•Splits into superficial and deep layers to enclose trapezius, SCM, submandibular gland and fibrous capsule of parotid gland
•Covers the posterior as well as the anterior triangle of the neck
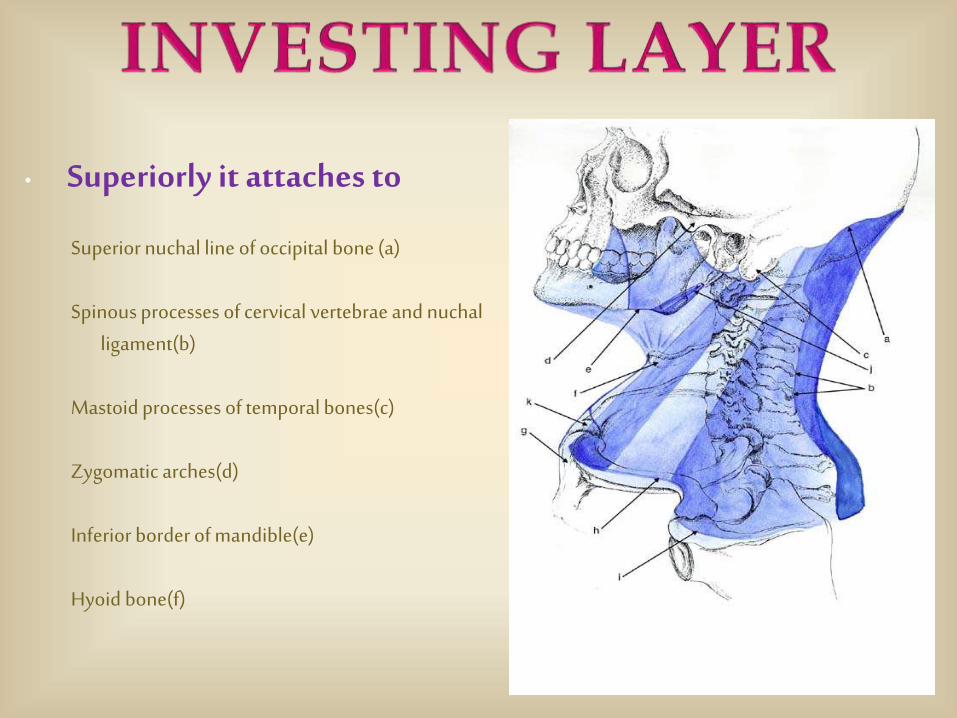
• Superiorly it attaches to
Superior nuchal line of occipital bone (a)
Spinous processes of cervical vertebrae and nuchalligament(b)
Mastoid processes of temporal bones(c)
Zygomatic arches(d)
Inferior border of mandible(e)
Hyoid bone(f)
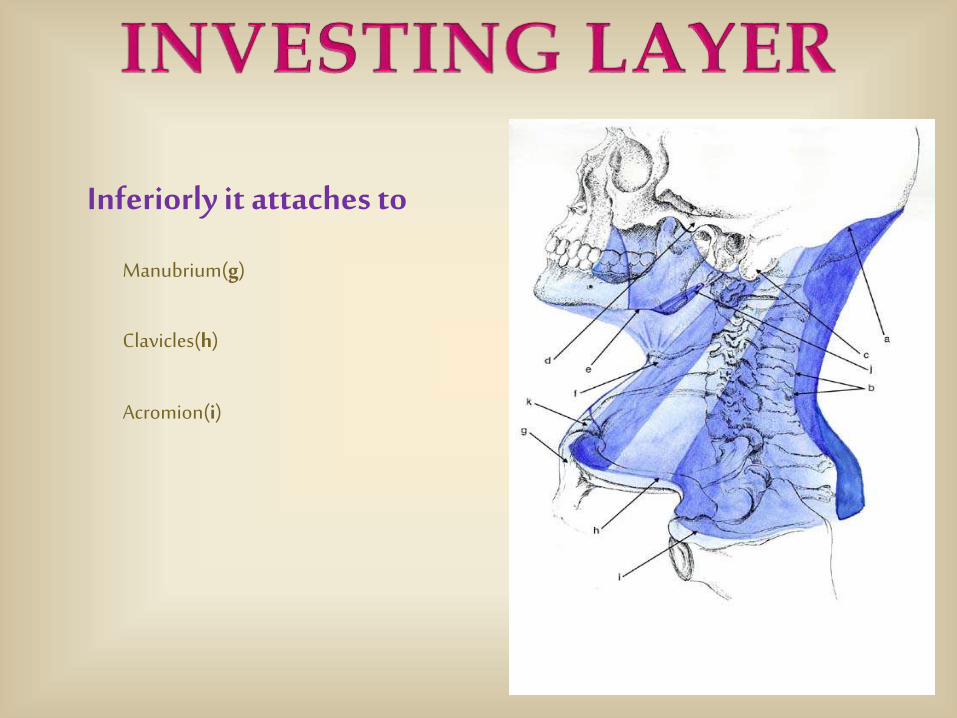
Inferiorly it attaches to
Manubrium(g)
Clavicles(h)
Acromion(i)
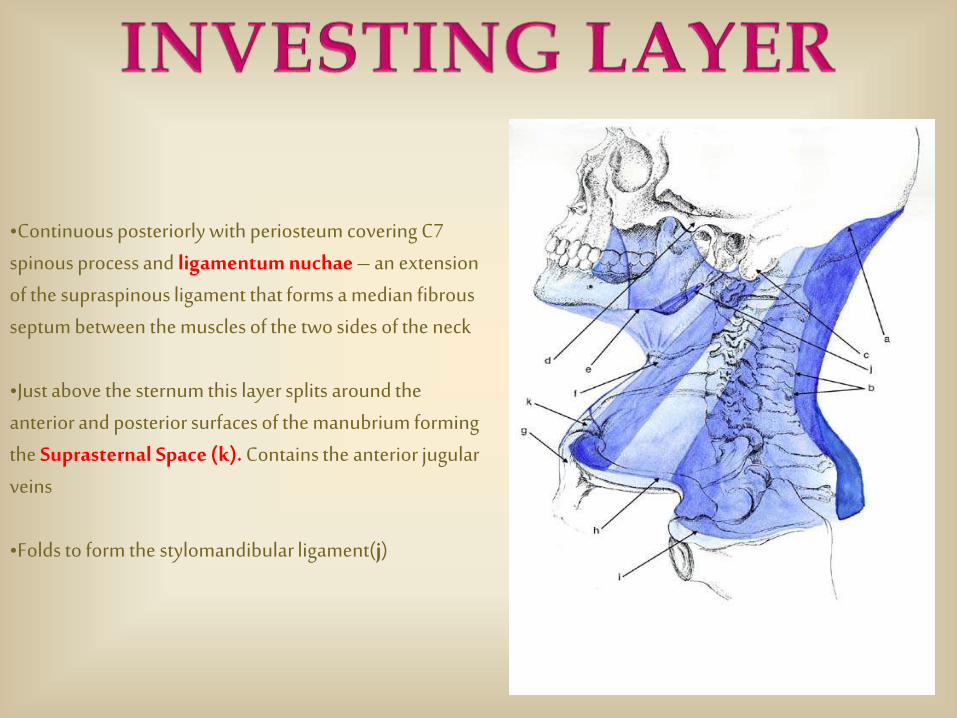
•Continuous posteriorly with periosteum covering C7 spinous process and ligamentum nuchae – an extension of the supraspinous ligament that forms a median fibrous septum between the muscles of the two sides of the neck
•Just above the sternum this layer splits around the anterior and posterior surfaces of the manubrium forming the Suprasternal Space (k). Contains the anterior jugular veins
•Folds to form the stylomandibular ligament(j)
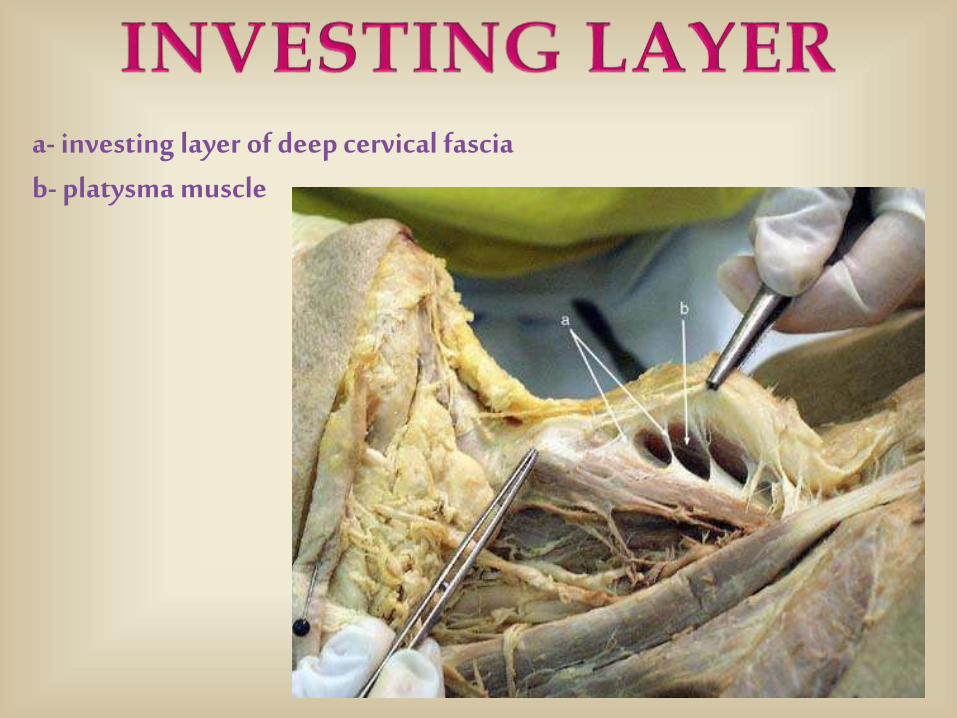
a- investing layer of deep cervical fasciab- platysma muscle
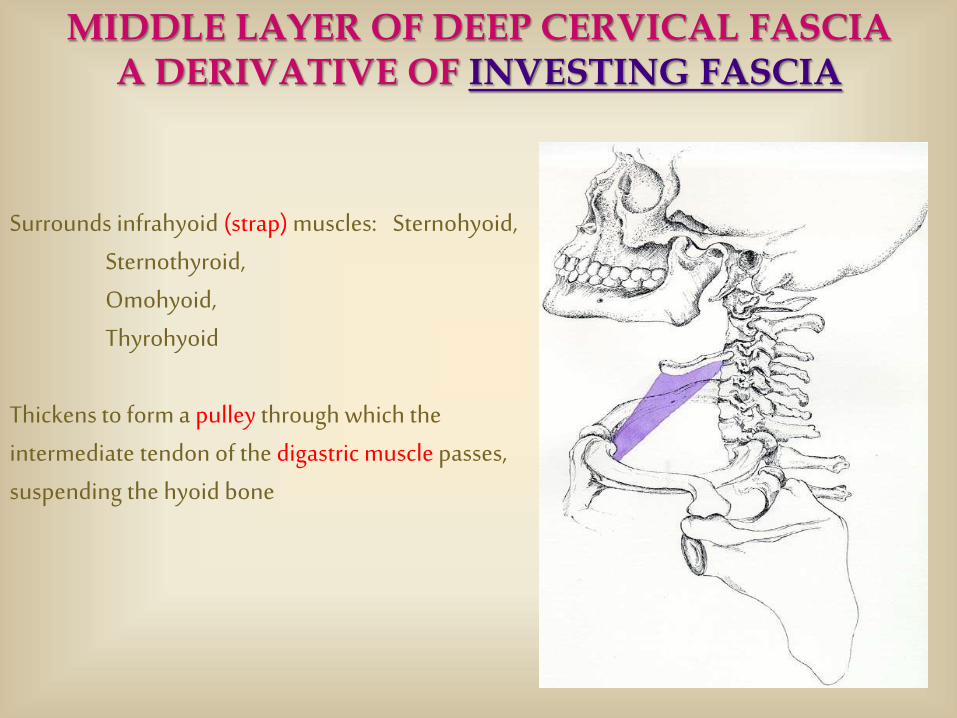
Surrounds infrahyoid (strap) muscles: Sternohyoid, Sternothyroid, Omohyoid, Thyrohyoid
Thickens to form a pulley through which the intermediate tendon of the digastric muscle passes, suspending the hyoid bone
MIDDLE LAYER OF DEEP CERVICAL FASCIAA DERIVATIVE OF INVESTING FASCIA
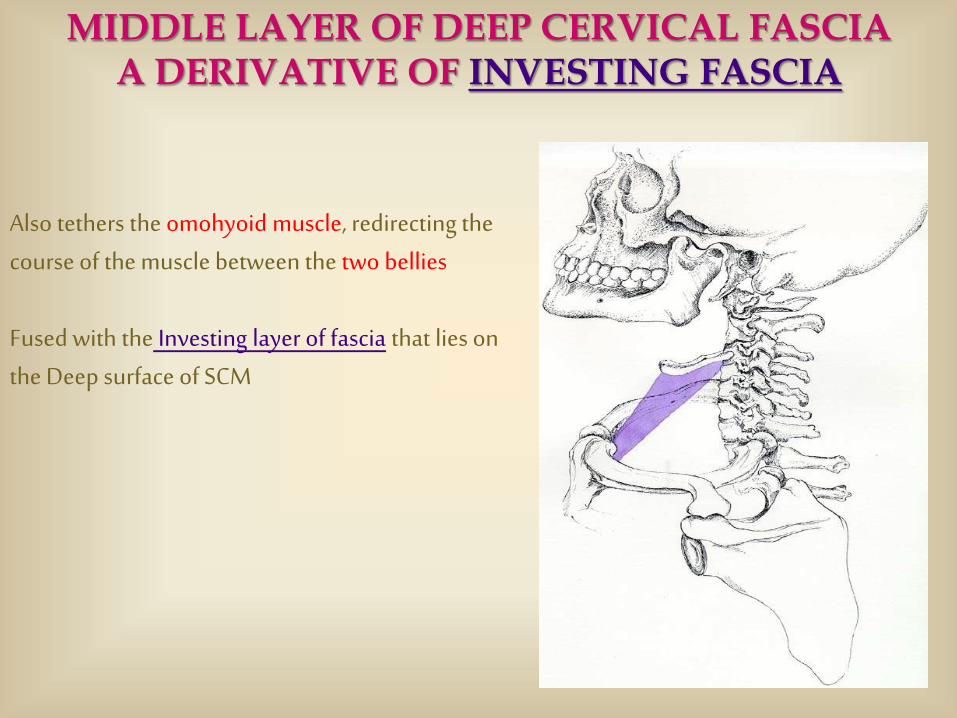
Also tethers the omohyoid muscle, redirecting the course of the muscle between the two bellies
Fused with the Investing layer of fascia that lies on the Deep surface of SCM
MIDDLE LAYER OF DEEP CERVICAL FASCIAA DERIVATIVE OF INVESTING FASCIA
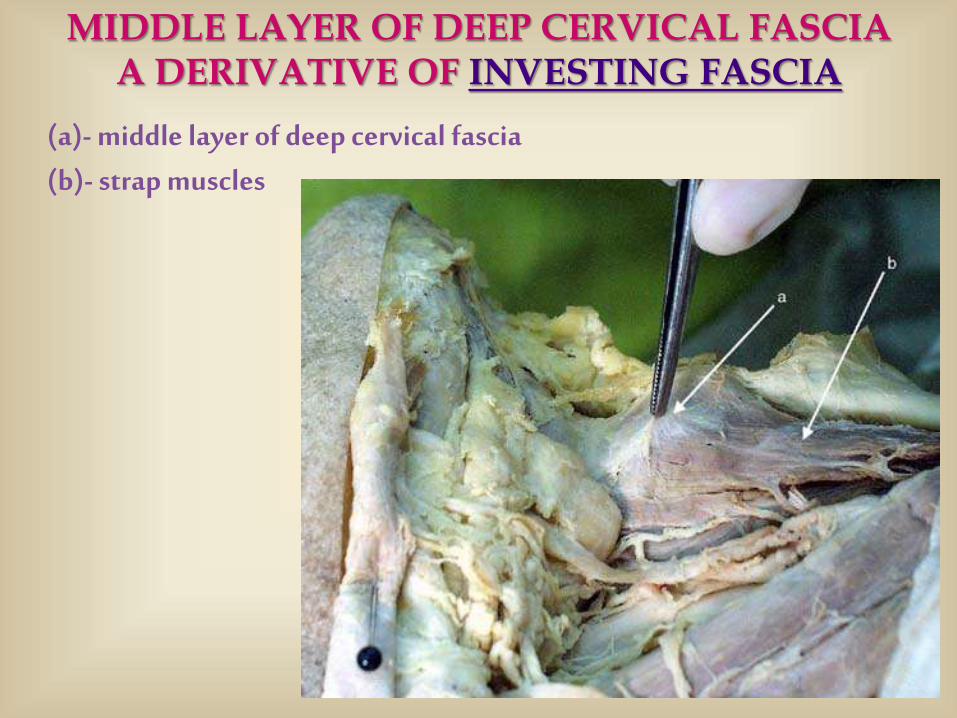
(a)- middle layer of deep cervical fascia(b)- strap muscles
MIDDLE LAYER OF DEEP CERVICAL FASCIAA DERIVATIVE OF INVESTING FASCIA
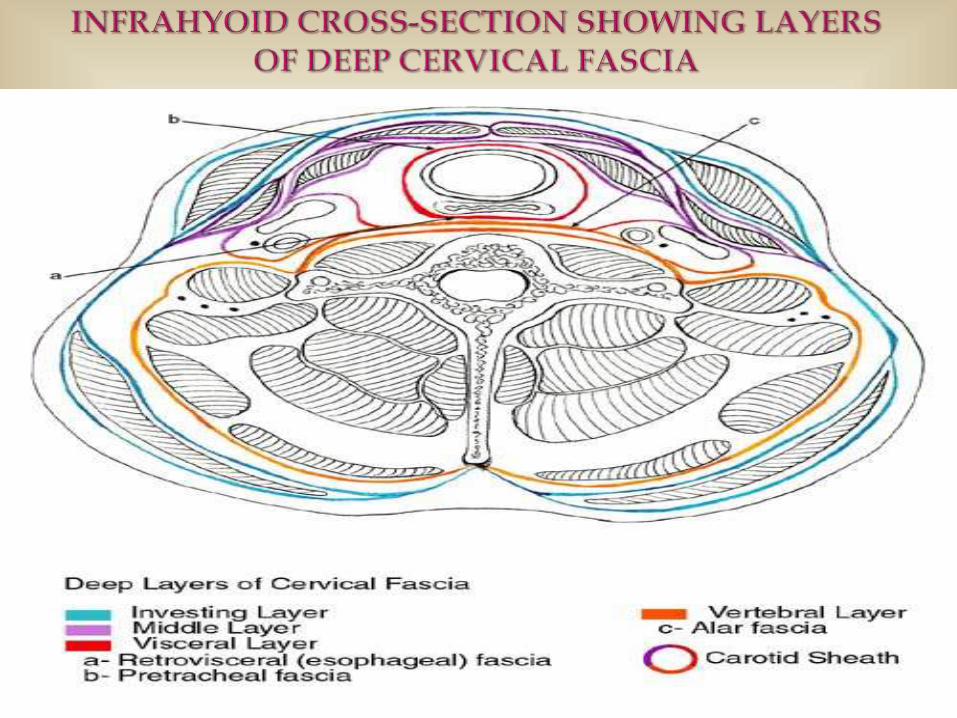
Visceral Layer of Deep Cervical Fascia
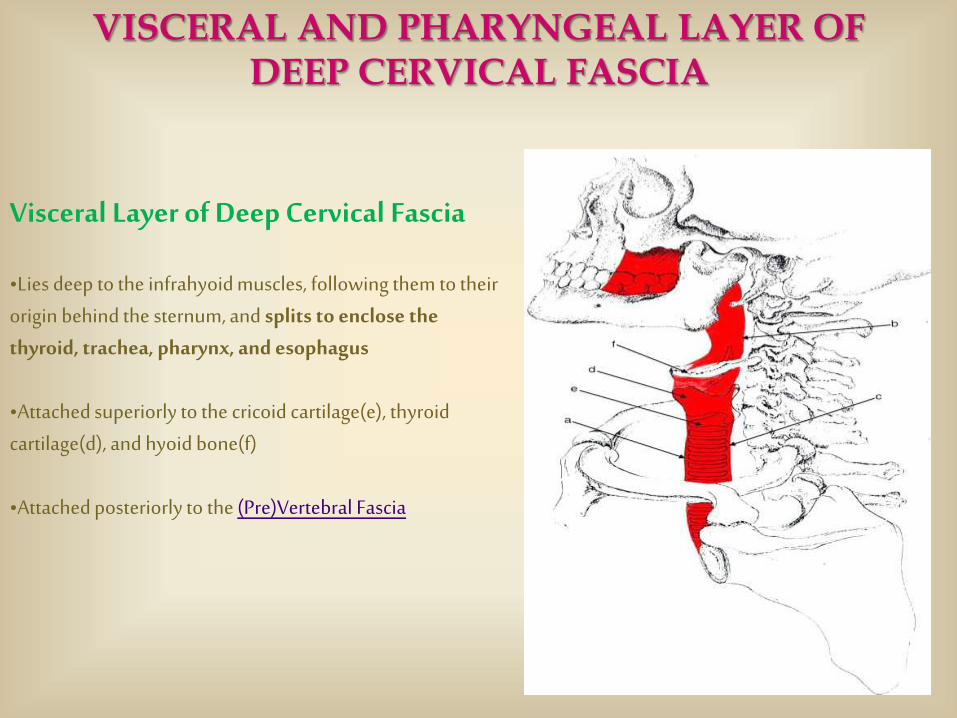
•Lies deep to the infrahyoid muscles, following them to their origin behind the sternum, and splits to enclose the thyroid, trachea, pharynx, and esophagus
•Attached superiorly to the cricoid cartilage(e), thyroid cartilage(d), and hyoid bone(f)
•Attached posteriorly to the (Pre)Vertebral Fascia
VISCERAL AND PHARYNGEAL LAYER OF DEEP CERVICAL FASCIA
Visceral Layer of Deep Cervical Fascia
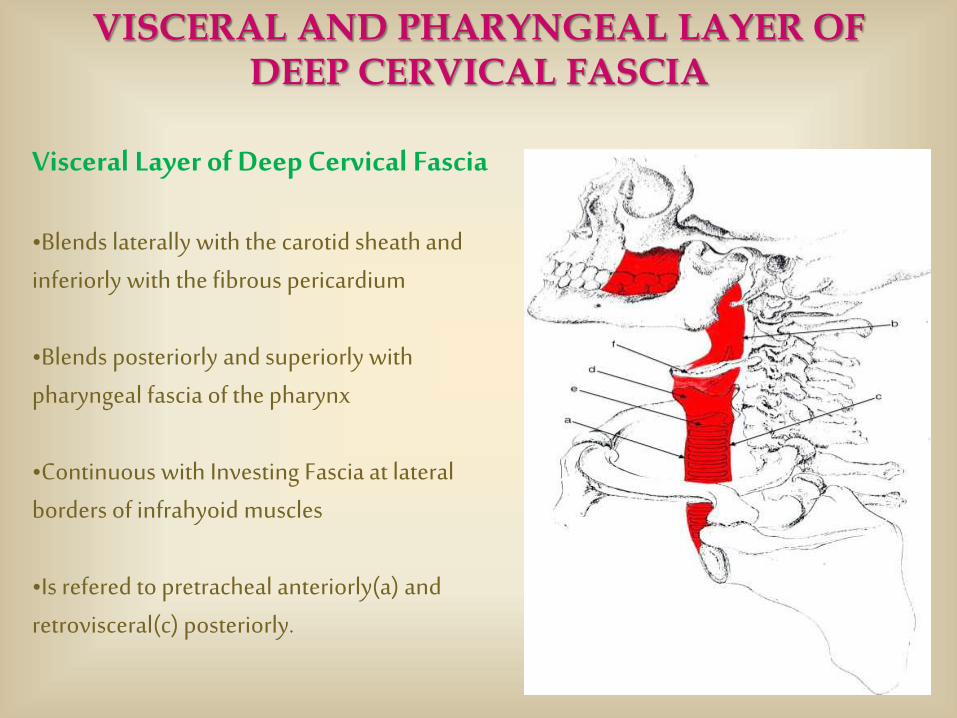
•Blends laterally with the carotid sheath and inferiorly with the fibrous pericardium
•Blends posteriorly and superiorly with pharyngeal fascia of the pharynx
•Continuous with Investing Fascia at lateral borders of infrahyoid muscles
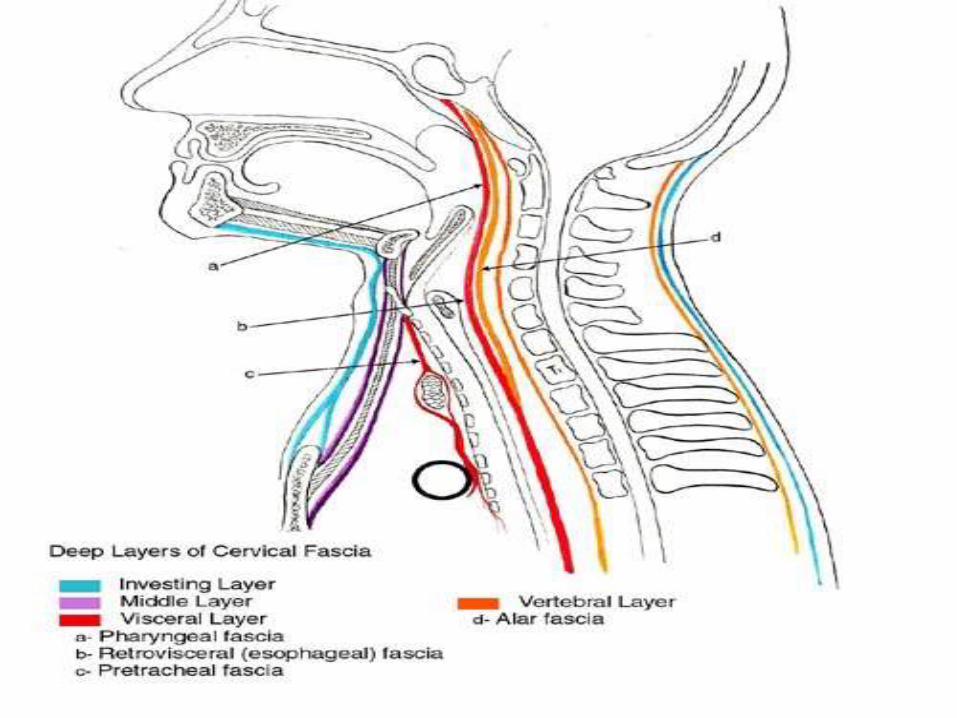
•Is refered to pretracheal anteriorly(a) and retrovisceral(c) posteriorly.
VISCERAL AND PHARYNGEAL LAYER OF DEEP CERVICAL FASCIA
Visceral Layer of Deep Cervical Fascia
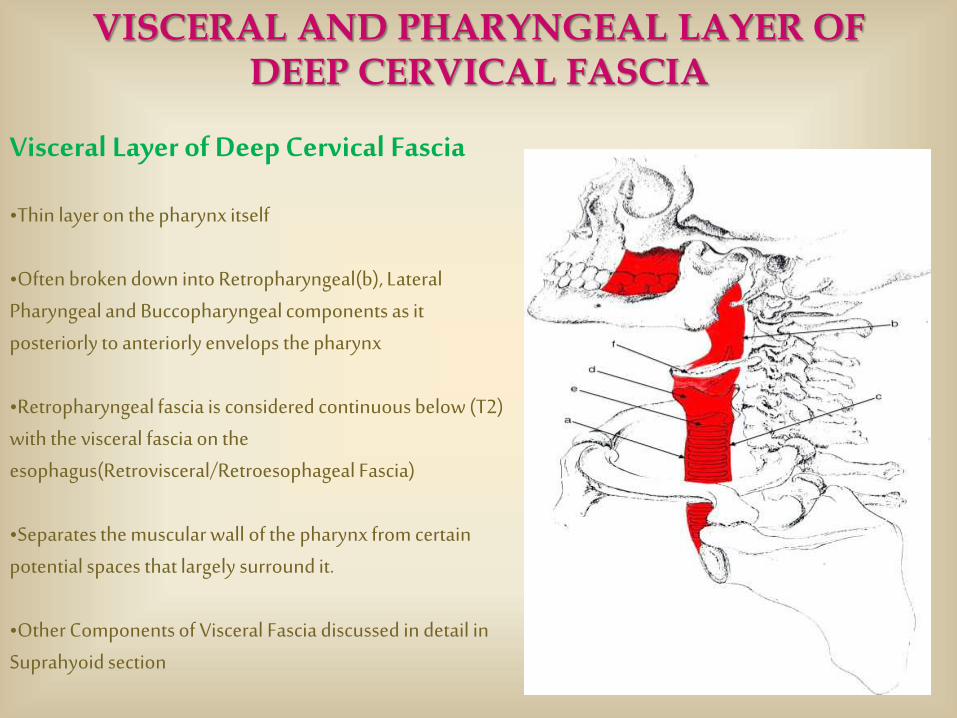
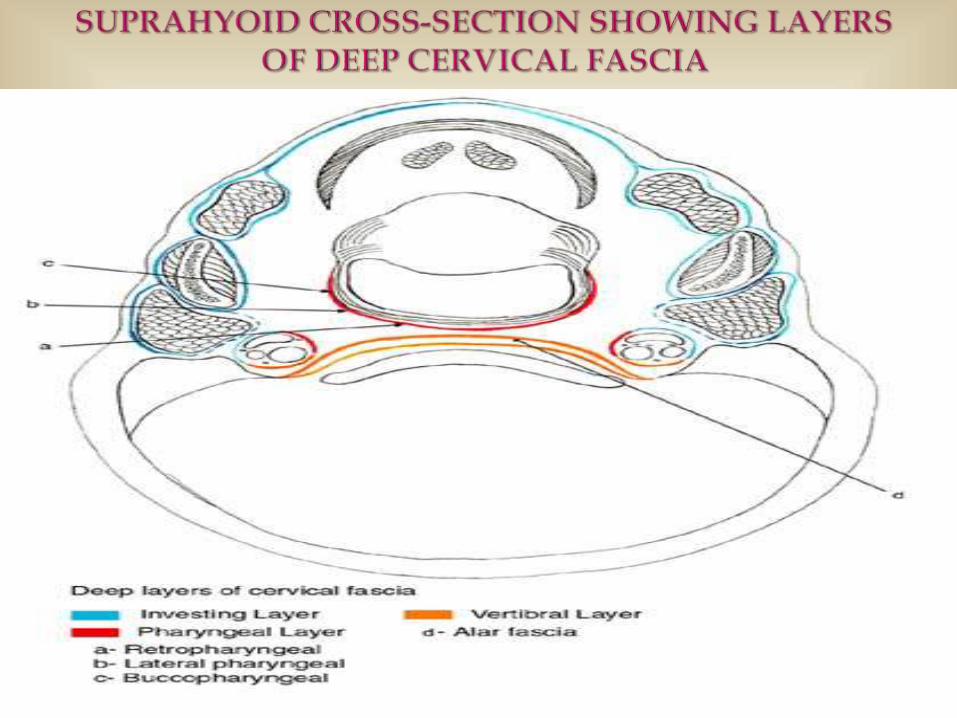
•Thin layer on the pharynx itself
•Often broken down into Retropharyngeal(b), Lateral Pharyngeal and Buccopharyngeal components as it posteriorly to anteriorly envelops the pharynx
•Retropharyngeal fascia is considered continuous below (T2) with the visceral fascia on the esophagus(Retrovisceral/Retroesophageal Fascia)
•Separates the muscular wall of the pharynx from certain potential spaces that largely surround it.
•Other Components of Visceral Fascia discussed in detail in Suprahyoid section
VISCERAL AND PHARYNGEAL LAYER OF DEEP CERVICAL FASCIA
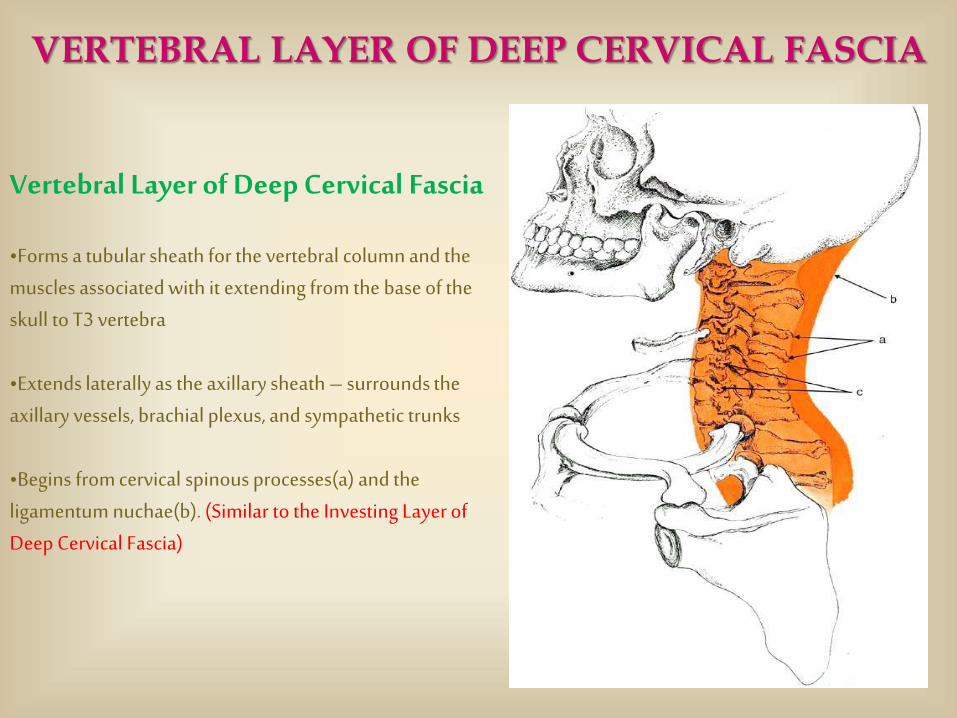
Vertebral Layer of Deep Cervical Fascia
•Forms a tubular sheath for the vertebral column and the muscles associated with it extending from the base of the skull to T3 vertebra
•Extends laterally as the axillary sheath – surrounds the axillary vessels, brachial plexus, and sympathetic trunks
•Begins from cervical spinous processes(a) and the ligamentum nuchae(b). (Similar to the Investing Layer of Deep Cervical Fascia)
VERTEBRAL LAYER OF DEEP CERVICAL FASCIA
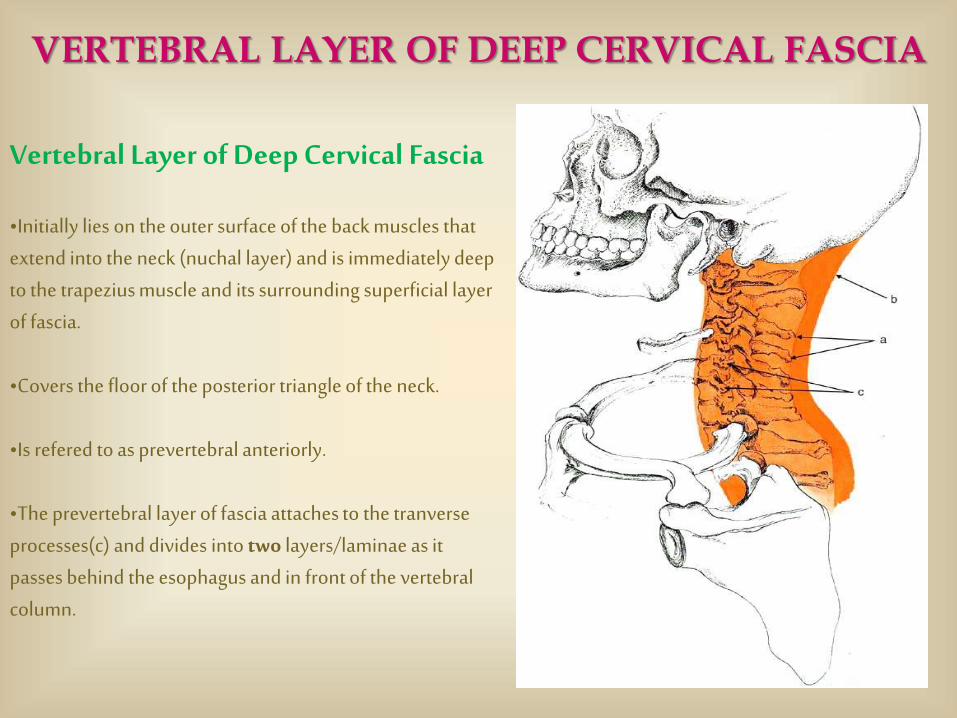
Vertebral Layer of Deep Cervical Fascia
•Initially lies on the outer surface of the back muscles that extend into the neck (nuchal layer) and is immediately deep to the trapezius muscle and its surrounding superficial layer of fascia.
•Covers the floor of the posterior triangle of the neck.
•Is refered to as prevertebral anteriorly.
•The prevertebral layer of fascia attaches to the tranverseprocesses(c) and divides into two layers/laminae as it passes behind the esophagus and in front of the vertebral column.
VERTEBRAL LAYER OF DEEP CERVICAL FASCIA
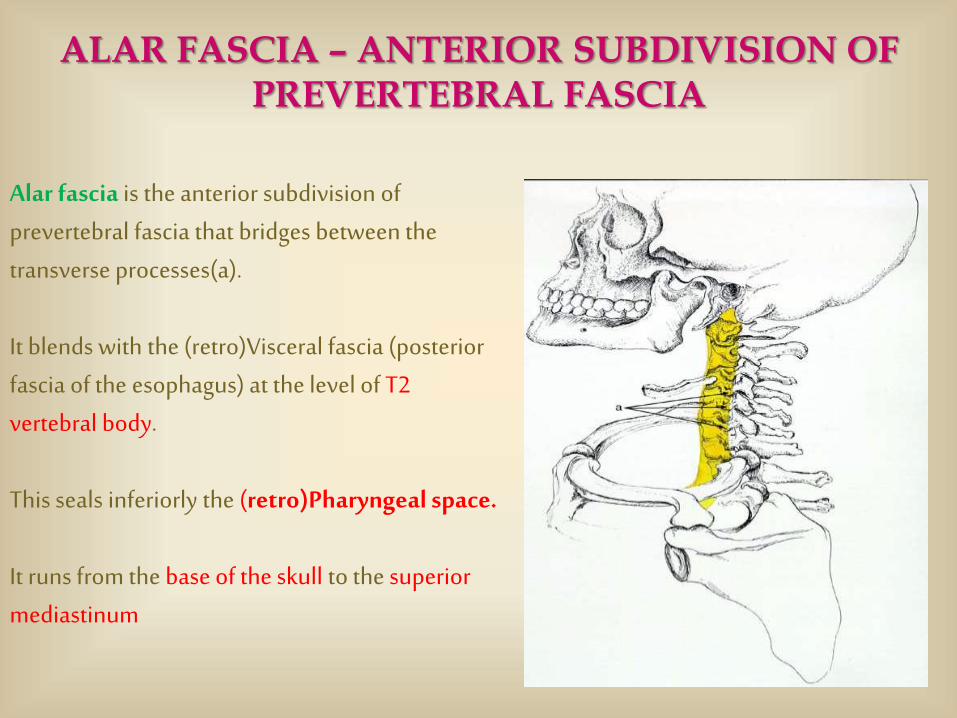
Alar fascia is the anterior subdivision of prevertebral fascia that bridges between the transverse processes(a).
It blends with the (retro)Visceral fascia (posterior fascia of the esophagus) at the level of T2 vertebral body.
This seals inferiorly the (retro)Pharyngeal space.
It runs from the base of the skull to the superior mediastinum
ALAR FASCIA – ANTERIOR SUBDIVISION OF PREVERTEBRAL FASCIA

(a)- tongue
(b)- inferior concha
(c)- danger space #4
(d)- alar fascia
(e)- oropharynx
(f)- epiglottis
ALAR FASCIA – ANTERIOR SUBDIVISION OF PREVERTEBRAL FASCIA
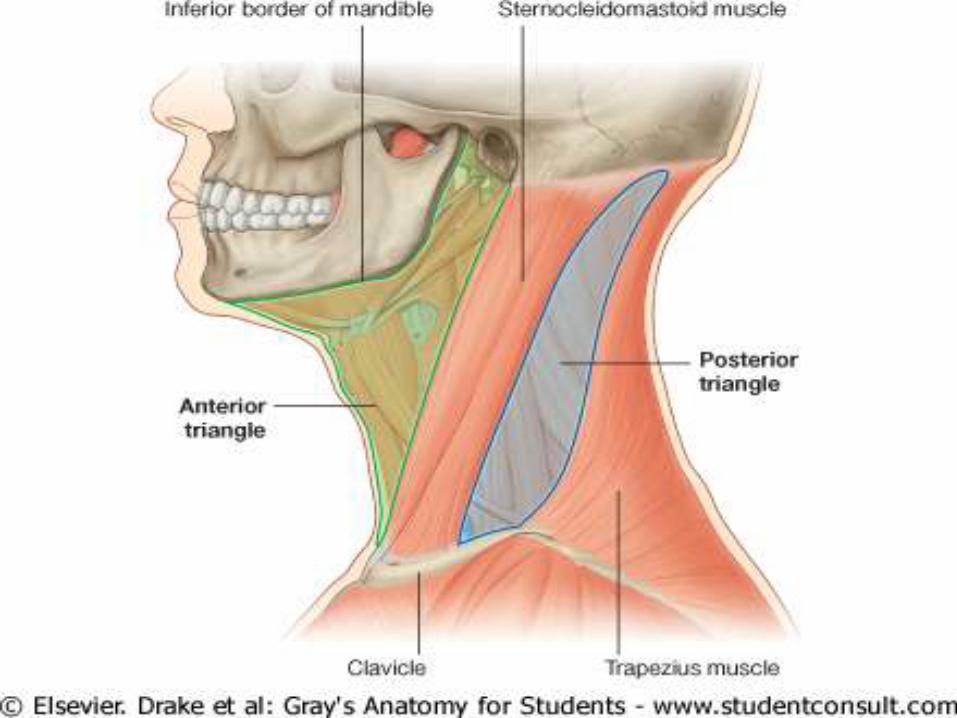
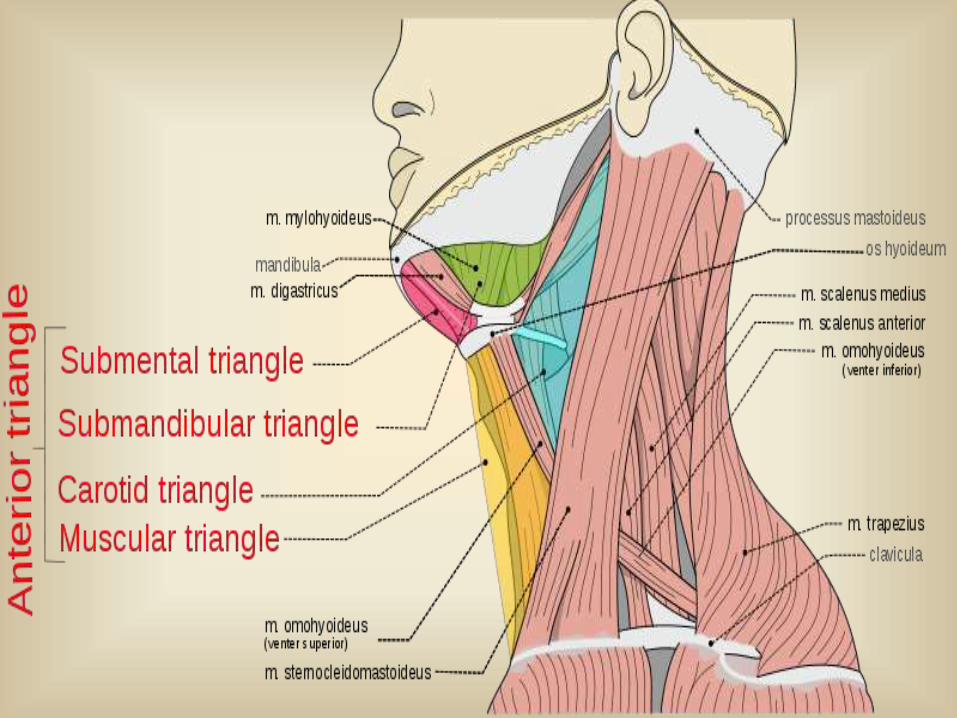
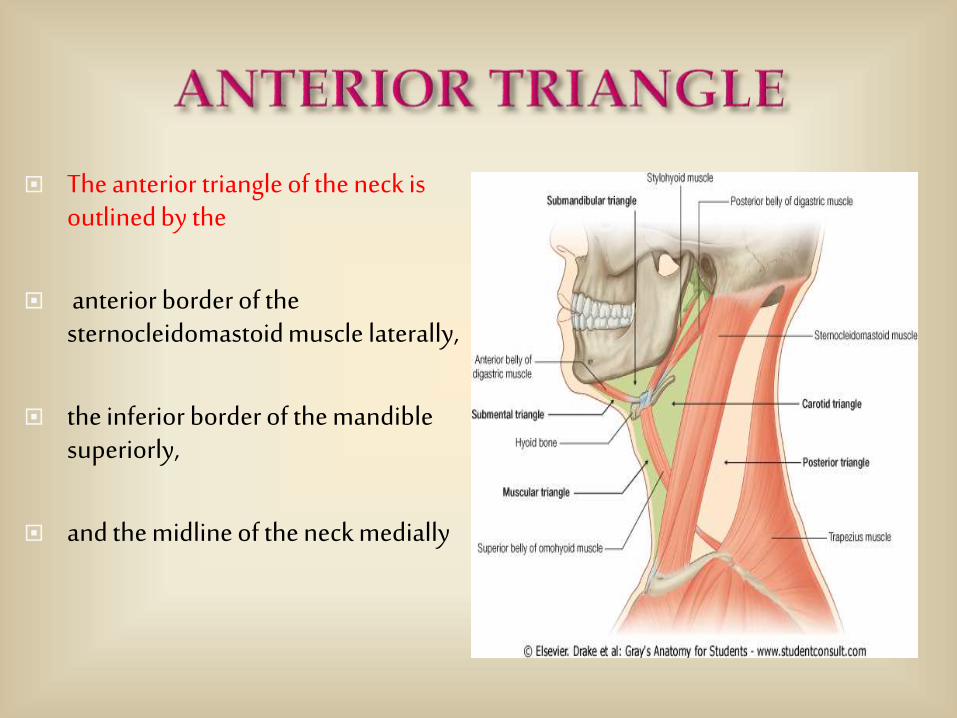
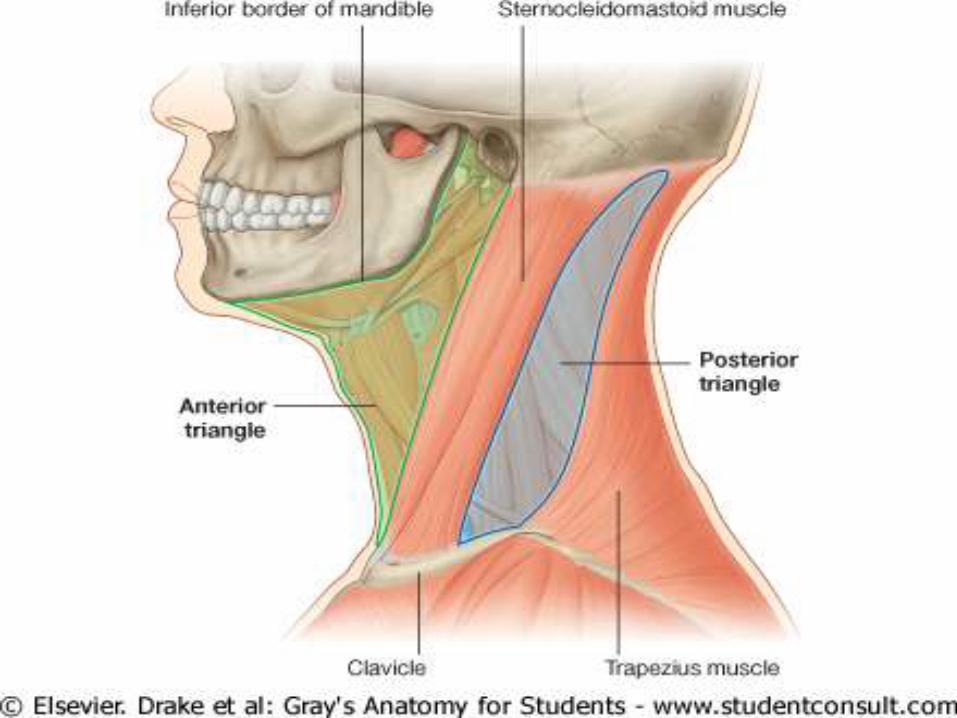
The anterior triangle of the neck is outlined by the
anterior border of the sternocleidomastoid muscle laterally,
the inferior border of the mandible superiorly,
and the midline of the neck medially
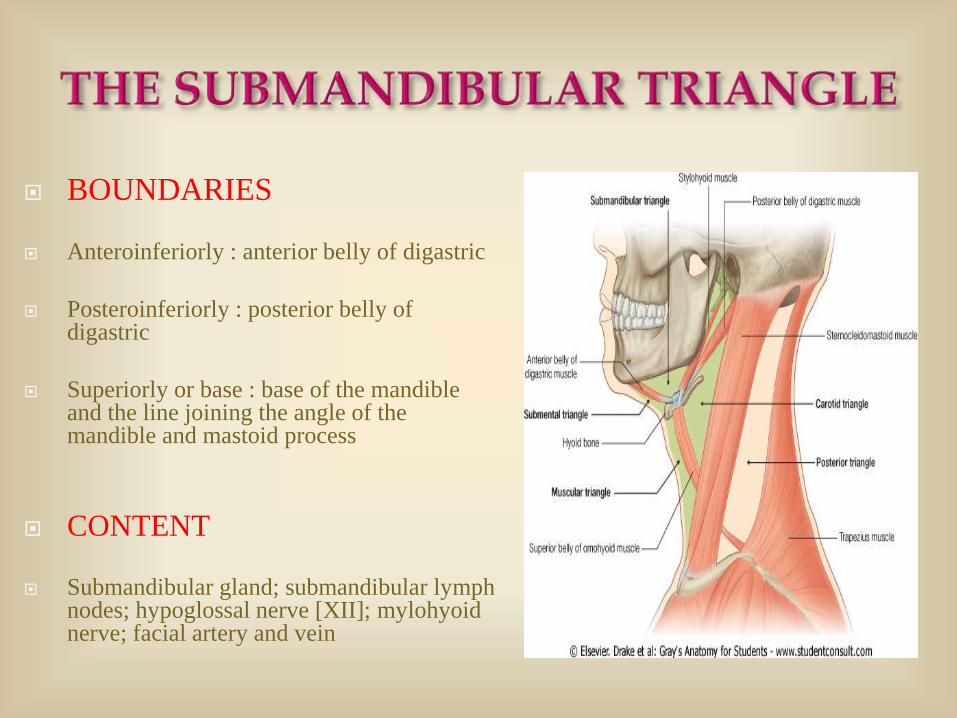
BOUNDARIES
Anteroinferiorly : anterior belly of digastric
Posteroinferiorly : posterior belly of digastric
Superiorly or base : base of the mandible and the line joining the angle of the mandible and mastoid process
CONTENT
Submandibular gland; submandibular lymph nodes; hypoglossal nerve [XII]; mylohyoidnerve; facial artery and vein
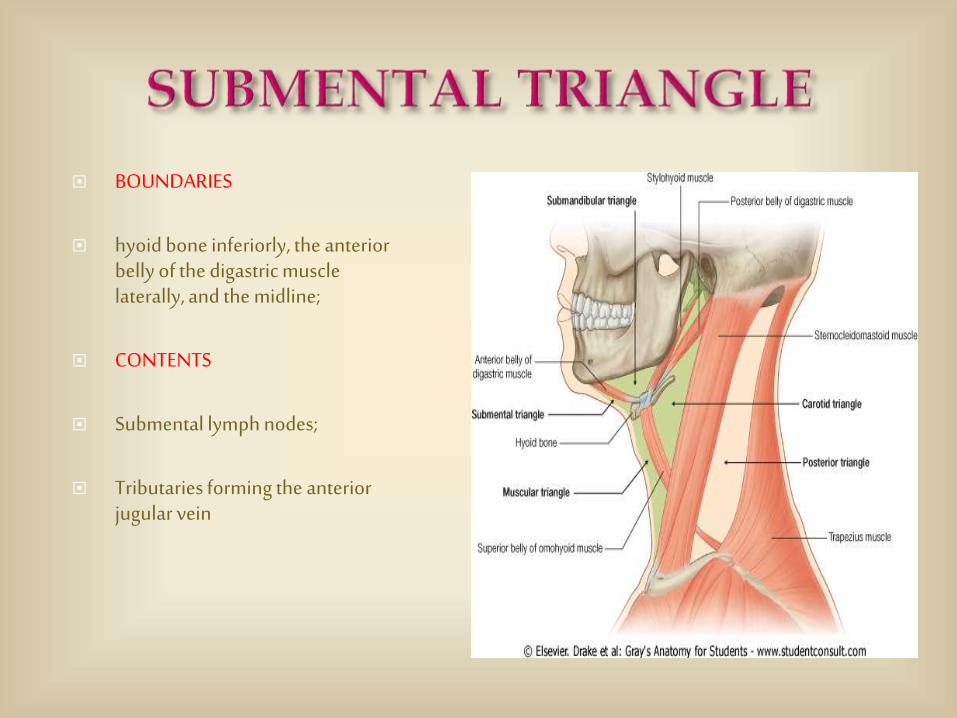
BOUNDARIES
hyoid bone inferiorly, the anterior belly of the digastric muscle laterally, and the midline;
CONTENTS
Submental lymph nodes;
Tributaries forming the anterior jugular vein
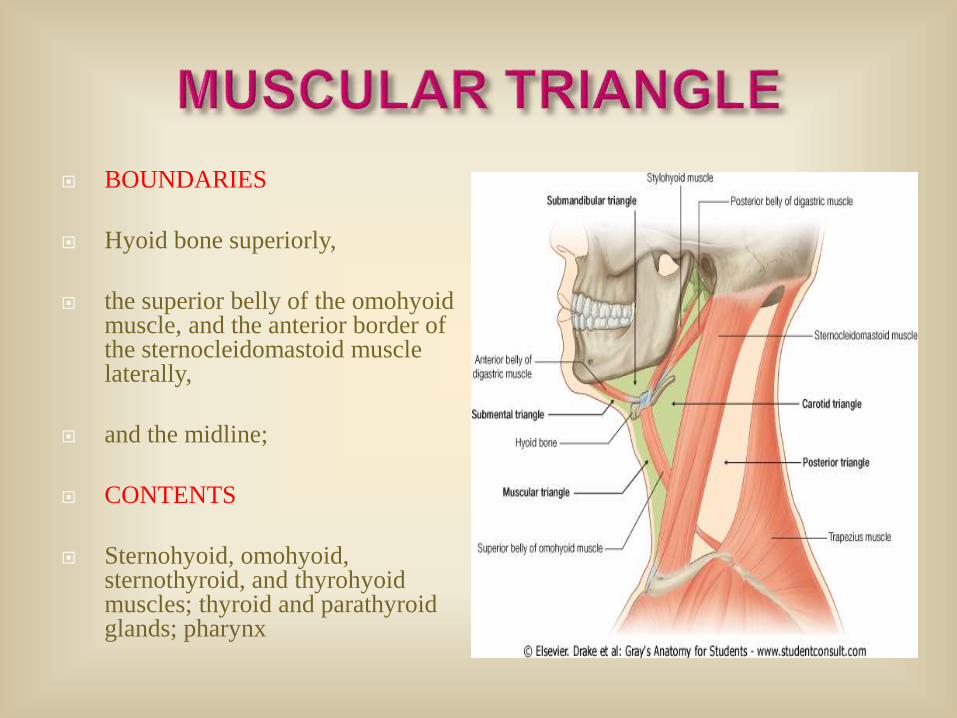
BOUNDARIES
Hyoid bone superiorly,
the superior belly of the omohyoidmuscle, and the anterior border of the sternocleidomastoid muscle laterally,
and the midline;
CONTENTS
Sternohyoid, omohyoid, sternothyroid, and thyrohyoidmuscles; thyroid and parathyroid glands; pharynx
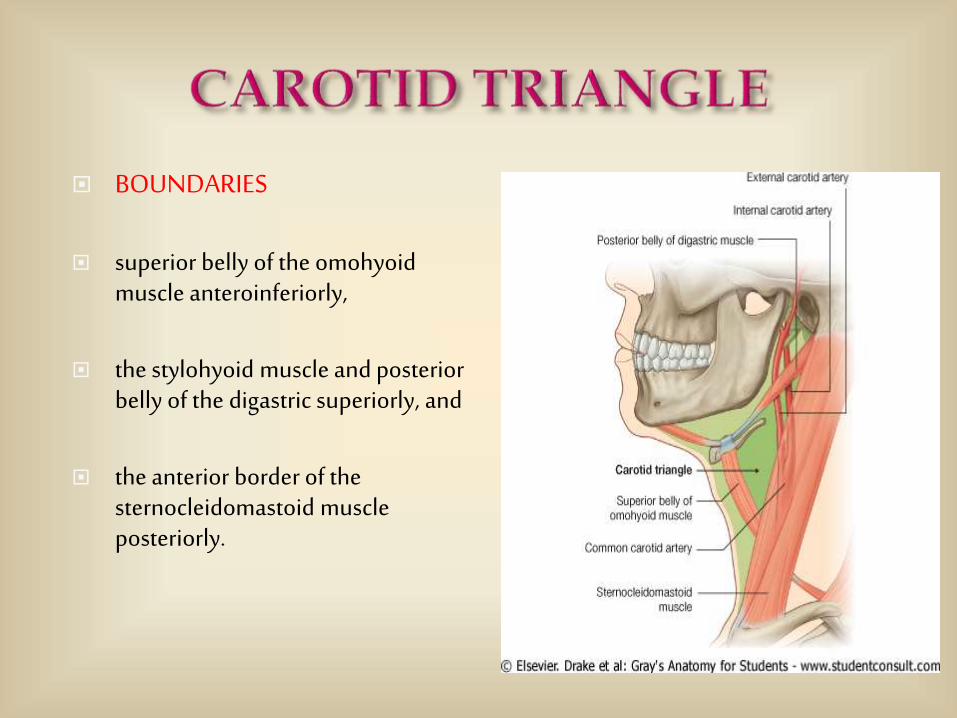
BOUNDARIES
superior belly of the omohyoidmuscle anteroinferiorly,
the stylohyoid muscle and posterior belly of the digastric superiorly, and
the anterior border of the sternocleidomastoid muscle posteriorly.
Tributaries to common facial vein
Cervical branch of facial nerve [VII]
Common carotid artery
External and internal carotid arteries
Superior thyroid; ascending pharyngeal; lingual, facial, and occipital arteries
Internal jugular vein
Vagus [X], accessory [XI], and hypoglossal [XII] nerves
Superior and inferior roots of ansa cervicalis
Transverse cervical nerve
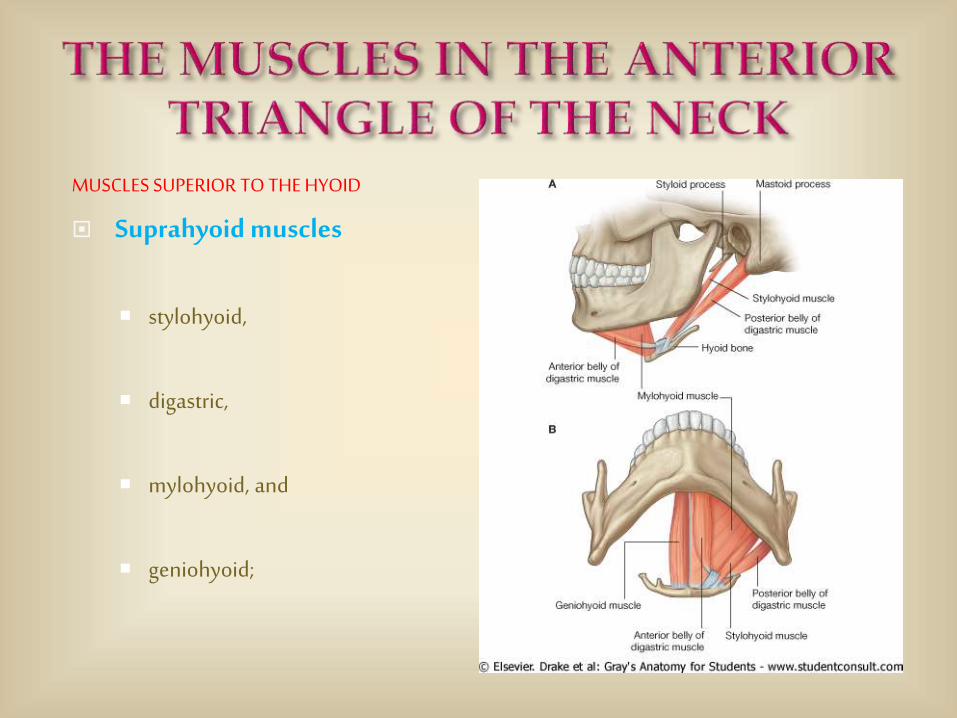
MUSCLES SUPERIOR TO THE HYOID
Suprahyoid muscles
stylohyoid,
digastric,
mylohyoid, and
geniohyoid;
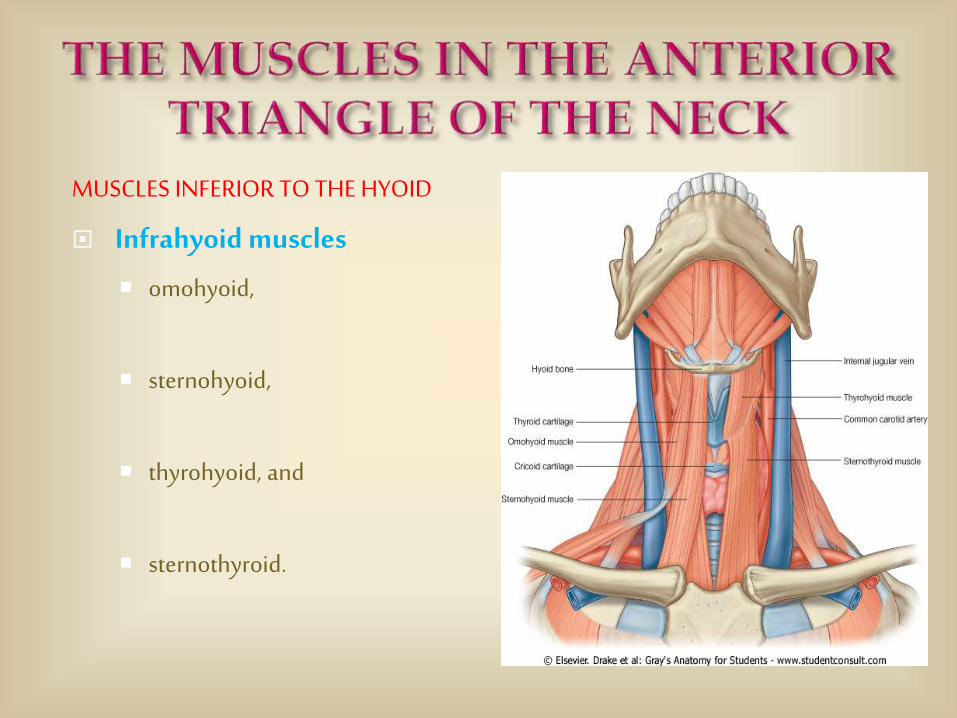
MUSCLES INFERIOR TO THE HYOID
Infrahyoid muscles
omohyoid,
sternohyoid,
thyrohyoid, and
sternothyroid.
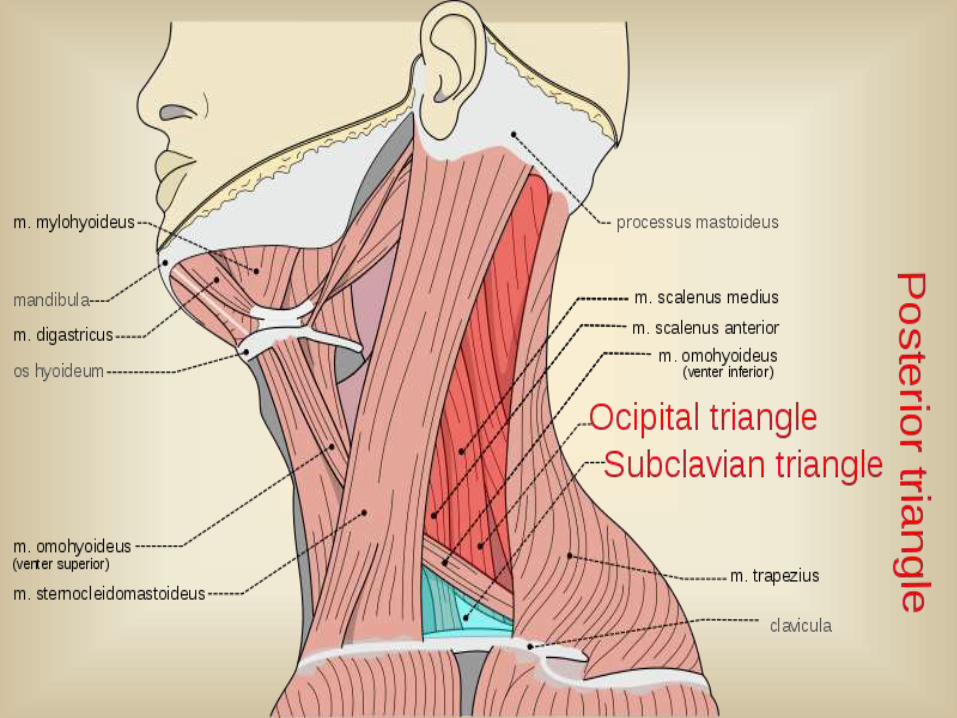
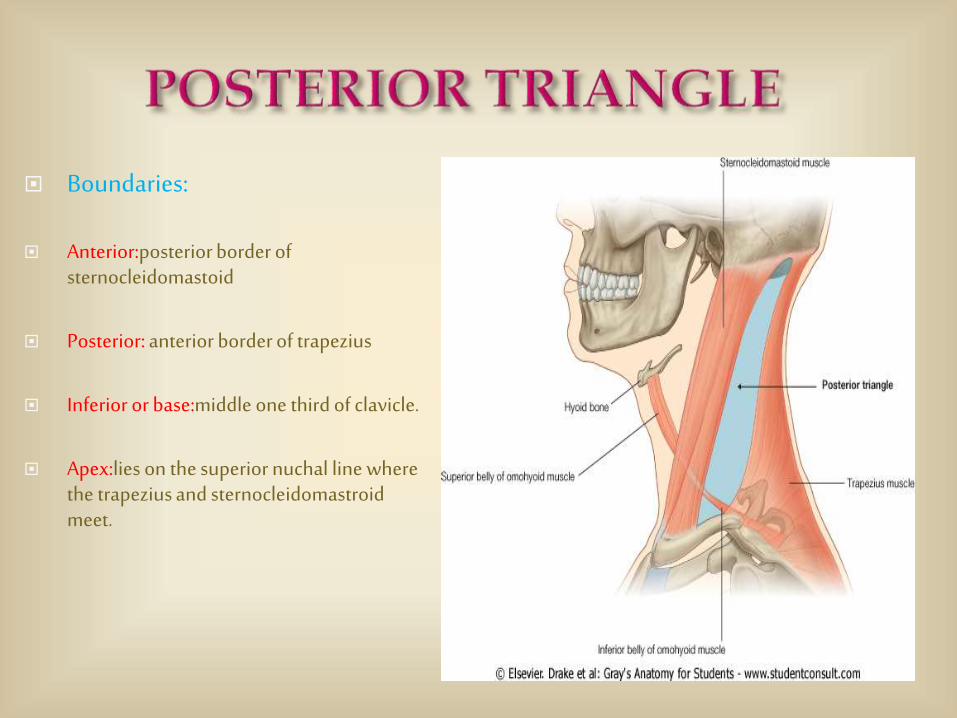
Boundaries:
Anterior:posterior border of sternocleidomastoid
Posterior: anterior border of trapezius
Inferior or base:middle one third of clavicle.
Apex:lies on the superior nuchal line where the trapezius and sternocleidomastroidmeet.
The roof is formed by the investing layer of deep cervical fascia.
The superficial fascia over the posterior triangle contains (a) the platysma(b) the external jugular and posterior external jugular veins.(c) parts of the supraclavicular,great auricular,transverse cutaneous and lesser occipital nerves,(d) transverse cervical and suprascapular arteries and lymph vessels which pierce the deep fascia to end in the supraclavicular nodes.
The floor of the posterior triangle is formed by the prevertebal layer of the deep cervical fascia coverting the following muscles:
(a) splenius capitus
(b) levator scapule
(c) scalenus medius and occasionaly scalenus posterior.
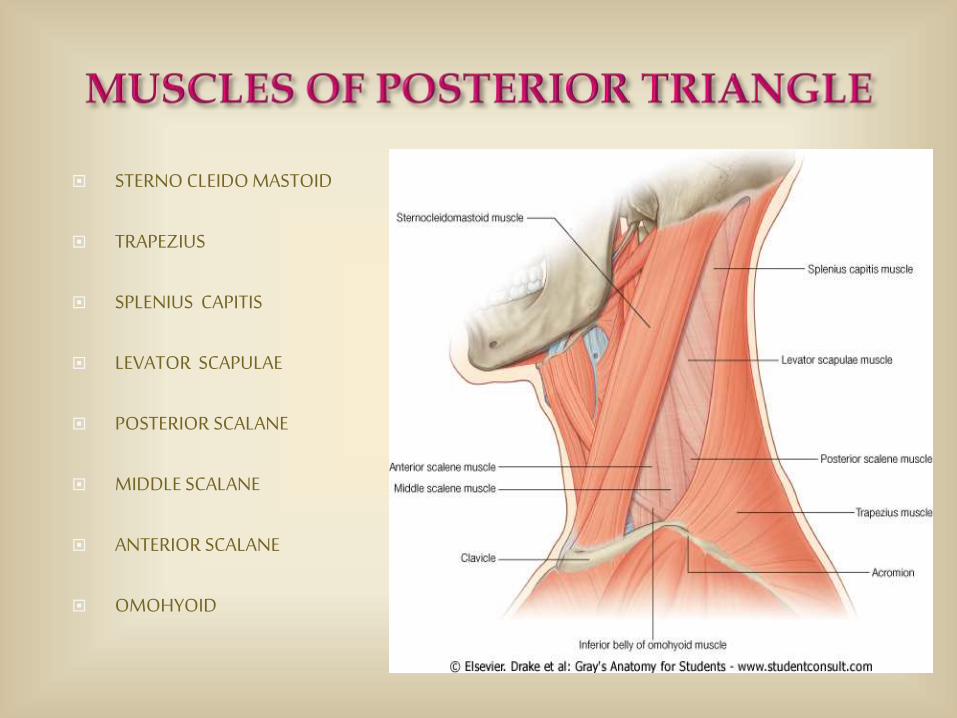
STERNO CLEIDO MASTOID
TRAPEZIUS
SPLENIUS CAPITIS
LEVATOR SCAPULAE
POSTERIOR SCALANE
MIDDLE SCALANE
ANTERIOR SCALANE
OMOHYOID
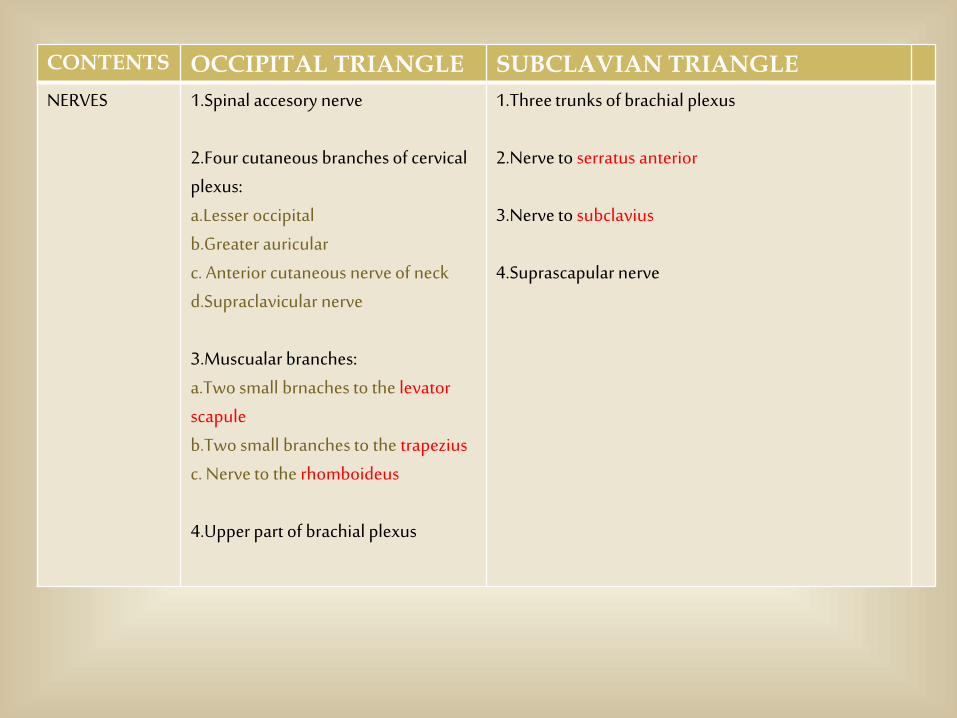
CONTENTS OCCIPITAL TRIANGLE SUBCLAVIAN TRIANGLE
NERVES 1.Spinal accesory nerve
2.Four cutaneous branches of cervical plexus:a.Lesser occipitalb.Greater auricularc. Anterior cutaneous nerve of neckd.Supraclavicular nerve
3.Muscualar branches:a.Two small brnaches to the levatorscapuleb.Two small branches to the trapeziusc. Nerve to the rhomboideus
4.Upper part of brachial plexus
1.Three trunks of brachial plexus
2.Nerve to serratus anterior
3.Nerve to subclavius
4.Suprascapular nerve
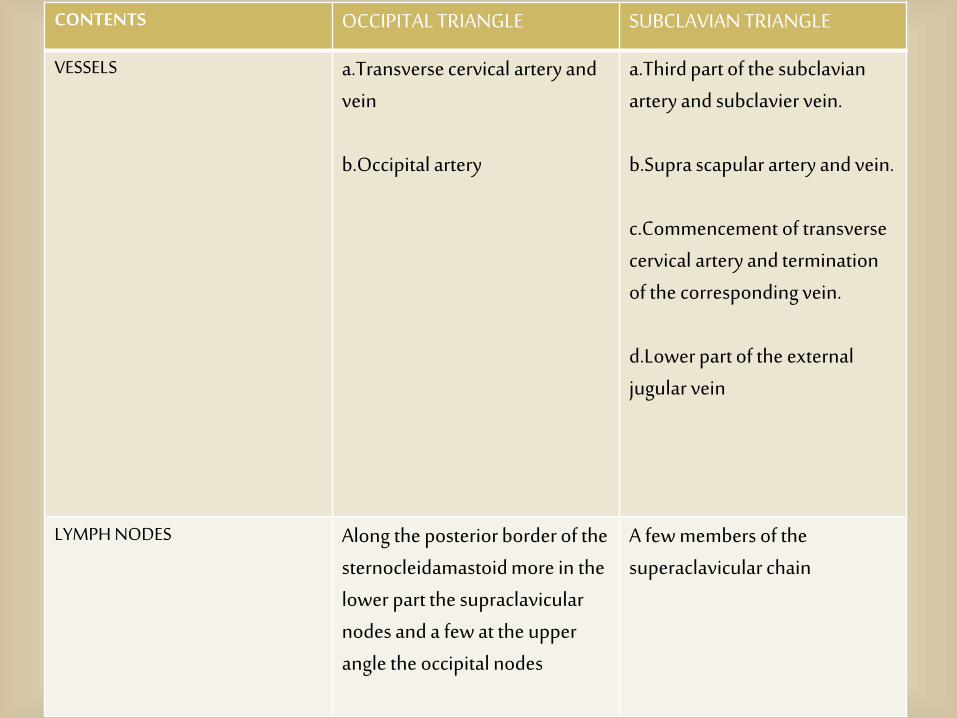
CONTENTS OCCIPITAL TRIANGLE SUBCLAVIAN TRIANGLE
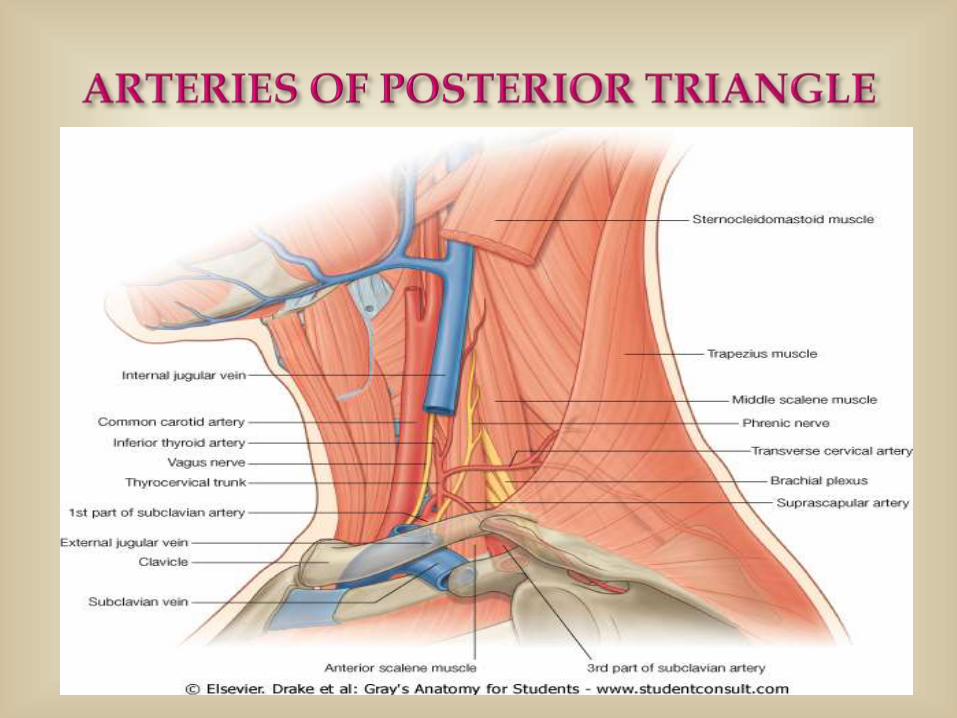
VESSELS a.Transverse cervical artery and vein
b.Occipital artery
a.Third part of the subclavianartery and subclavier vein.
b.Supra scapular artery and vein.
c.Commencement of transverse cervical artery and termination of the corresponding vein.
d.Lower part of the external jugular vein
LYMPH NODES Along the posterior border of the sternocleidamastoid more in the lower part the supraclavicularnodes and a few at the upper angle the occipital nodes
A few members of the superaclavicular chain
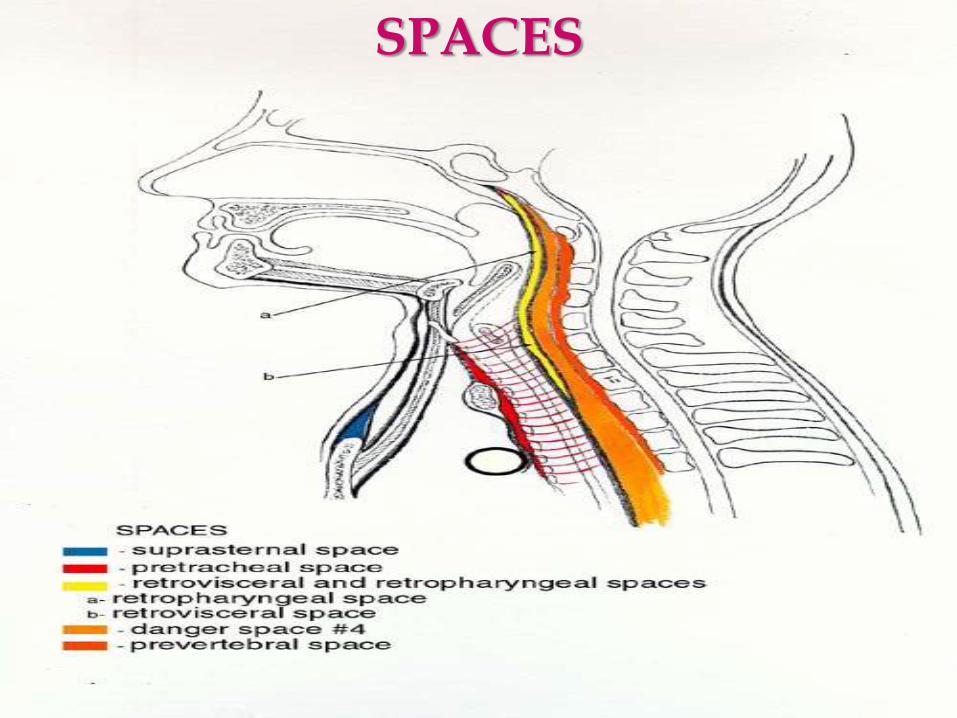
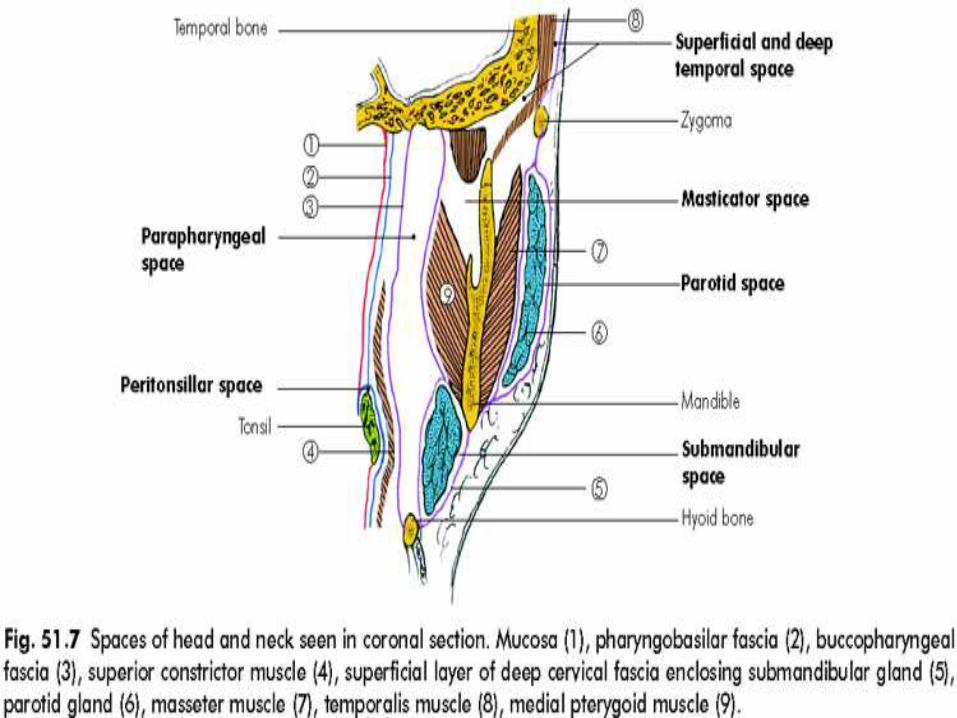
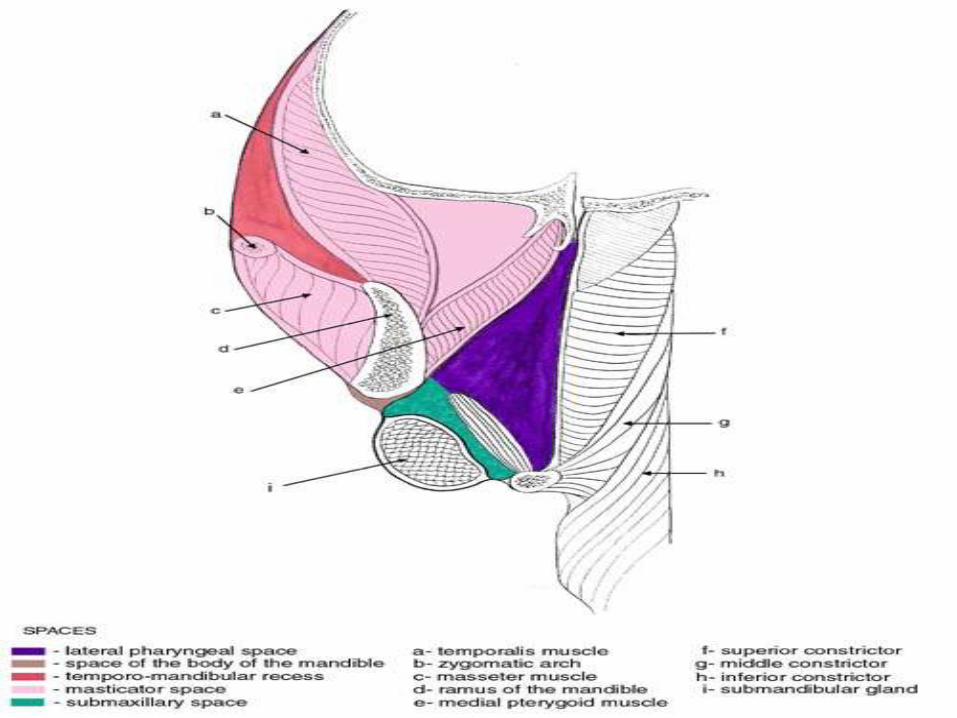
SPACES

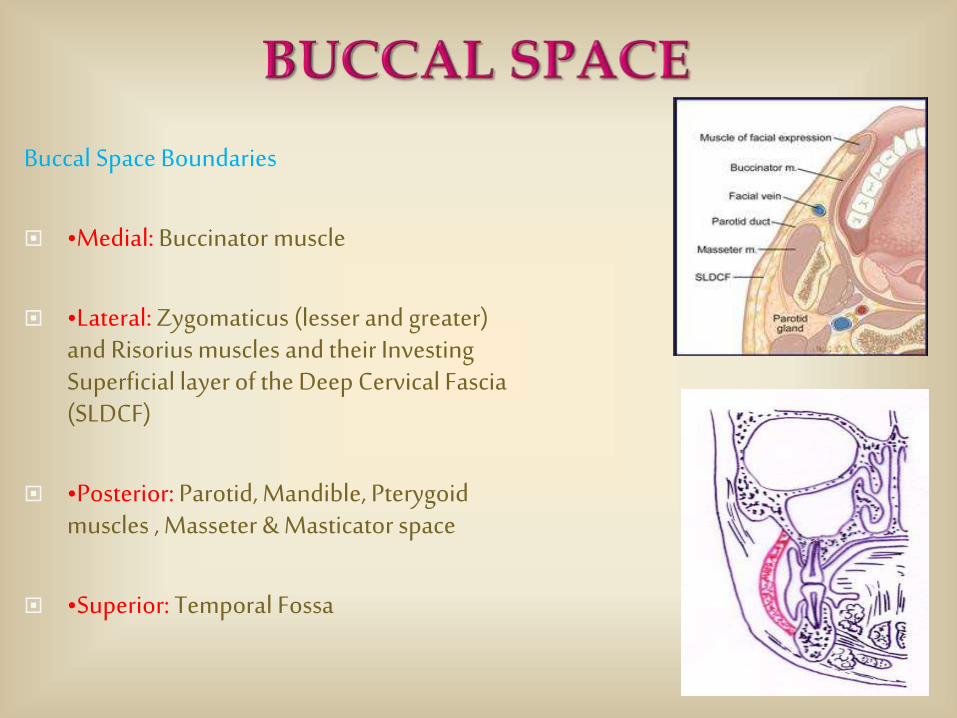
Buccal Space Boundaries
•Medial: Buccinator muscle
•Lateral: Zygomaticus (lesser and greater) and Risorius muscles and their Investing Superficial layer of the Deep Cervical Fascia (SLDCF)
•Posterior: Parotid, Mandible, Pterygoidmuscles , Masseter & Masticator space
•Superior: Temporal Fossa
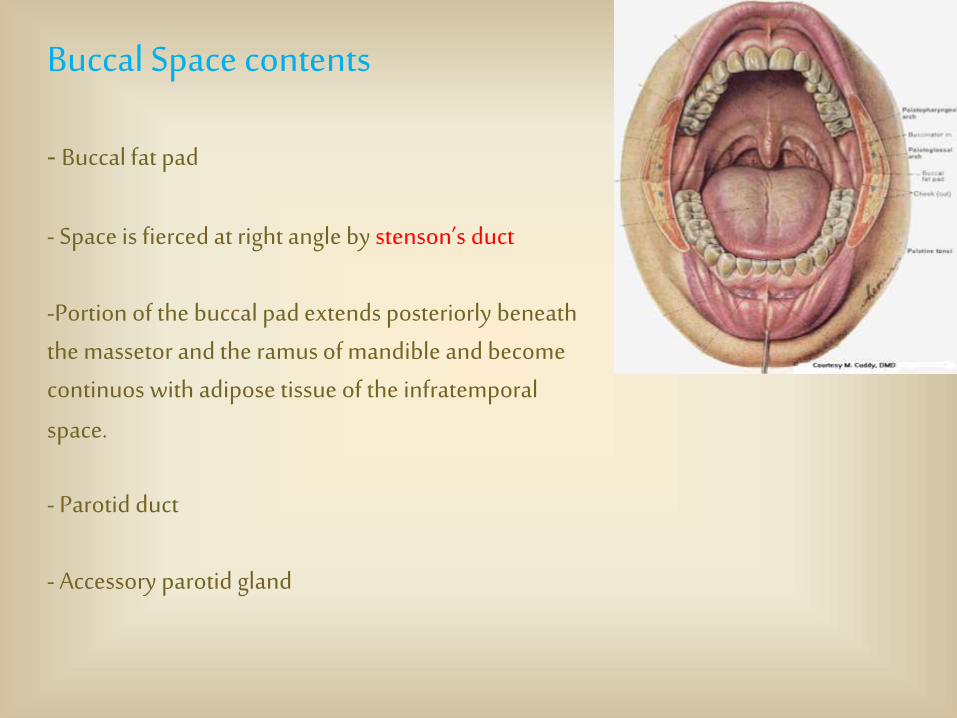
Buccal Space contents
- Buccal fat pad
- Space is fierced at right angle by stenson’s duct
-Portion of the buccal pad extends posteriorly beneath the massetor and the ramus of mandible and become continuos with adipose tissue of the infratemporal
space.
- Parotid duct
- Accessory parotid gland
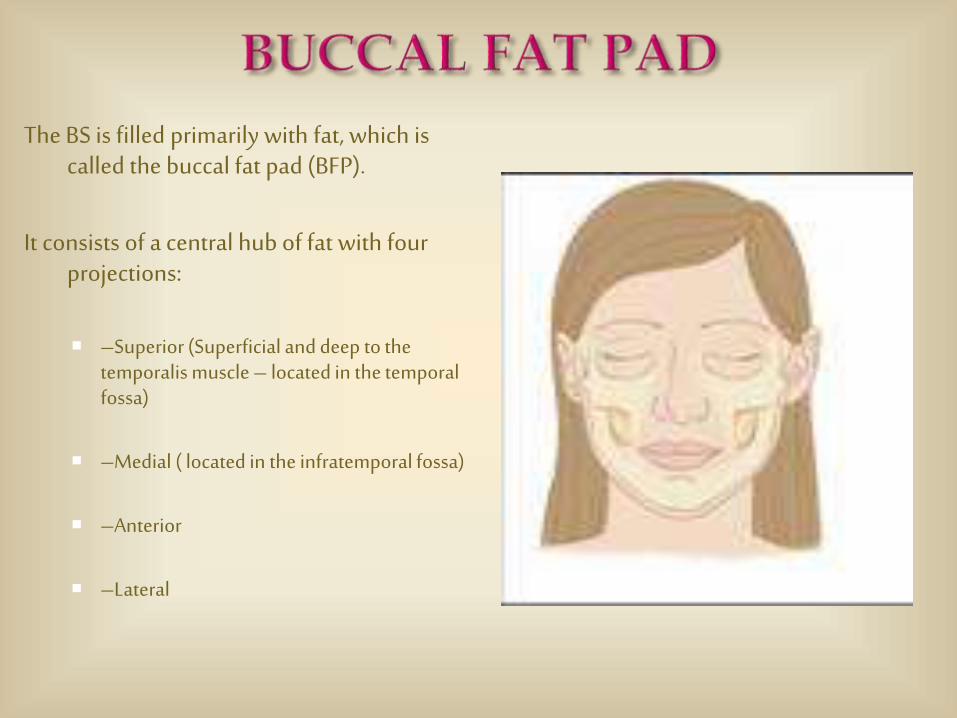
The BS is filled primarily with fat, which is called the buccal fat pad (BFP).
It consists of a central hub of fat with four projections:
–Superior (Superficial and deep to the temporalis muscle – located in the temporal fossa)
–Medial ( located in the infratemporal fossa)
–Anterior
–Lateral
Superiorly : Levator labii superiorris , Zygomaticminor & Alar Nasi
Posteriorly : Buccinator muscle
Anteriorly : Orbicularis oris muscle
Source of infection : Anterior maxillary teeth & pre-molars Skin of nose Upper lips
(Drainage is done intraorally and carried through the periosteum and down to the bone.)
This space lies between the superficial fascia and the deep layer of the deep cervical fascia. (Entire length of neck)
Surrounds platysma
Site of superficial cellulitis of neck usually secondary to supparation of lymph node.
Clinically the signs of infection are obvious as these abscesses point and fluctuant, as opposed to deep space neck infections.
Treatment : I & D (Treat with incision along Langer’s lines)and Antibiotics

Entire length of neck.
Anterior border - pharynx and esophagus (buccopharyngeal fascia)
Posterior border - alar layer of deep fascia
Superior border - skull base
Inferior border – superior mediastinum
Combines with buccopharyngeal fascia at level of T1-T2( communicate
with the pretracheal space, )
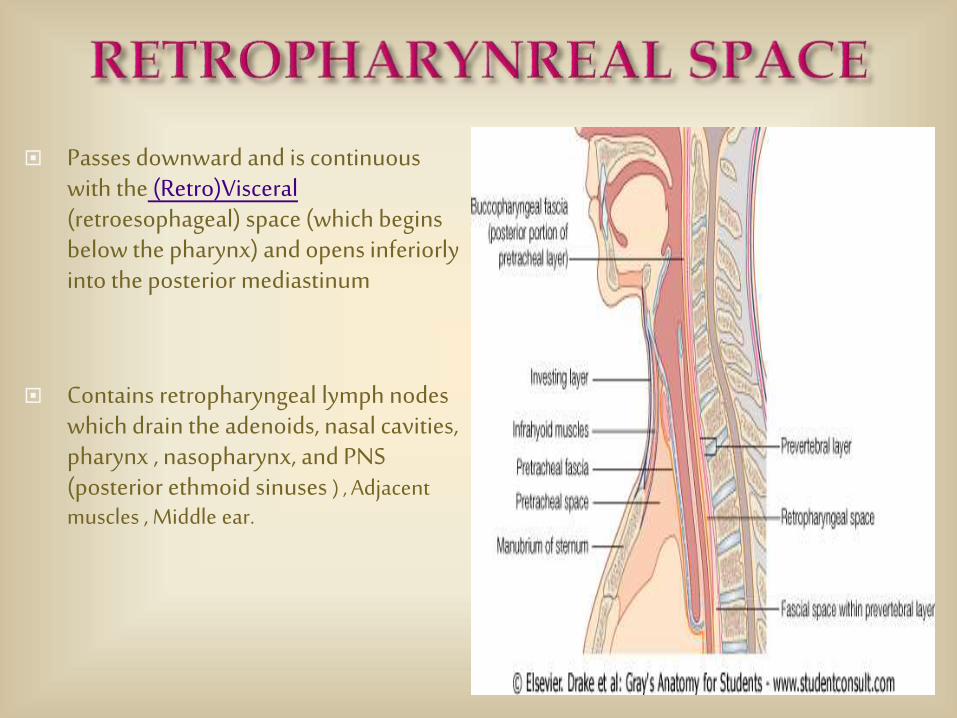
Passes downward and is continuous with the (Retro)Visceral(retroesophageal) space (which begins below the pharynx) and opens inferiorly into the posterior mediastinum
Contains retropharyngeal lymph nodes which drain the adenoids, nasal cavities, pharynx , nasopharynx, and PNS (posterior ethmoid sinuses ) , Adjacent muscles , Middle ear.
ClinicalAbscess : drained by trans oral drainage.( Horizontal incision is made over the bulging posterior
pharyngeal mucosa to establish the drainage)
If contagious space involvement suggested : External Drainage.
Horizontal incision in the neck and dissecting anterior to the anterior border of the SCM. The greater vessels are identified and retracted laterally. RPS is then identified and entered with blunt dissection(between the carotid sheath & and the constrictor muscle) , first laterally and then posterior to the pharyngeal musculatare. A drain is left in position.
ClinicalCommonly regarded as a route through which infections of the mouth and throat reach the
mediastinum. It can break through the posterior wall of the space through the alar fascia, and can enter Danger Space 4, between the two lamellae of the prevertebral layer of fascia (extends from the base of the skull to the level of the diaphragm).
A sagitically oriented fibrous septum connects the anterior and the posterior pillar in the midline and divides it into two compartments called THE SPACES OF GILLETTE. Abscess in this space is unilateral .
Retropharyngeal edema may occur due to post radiation fluid collection and non infectious inflammatory processes.
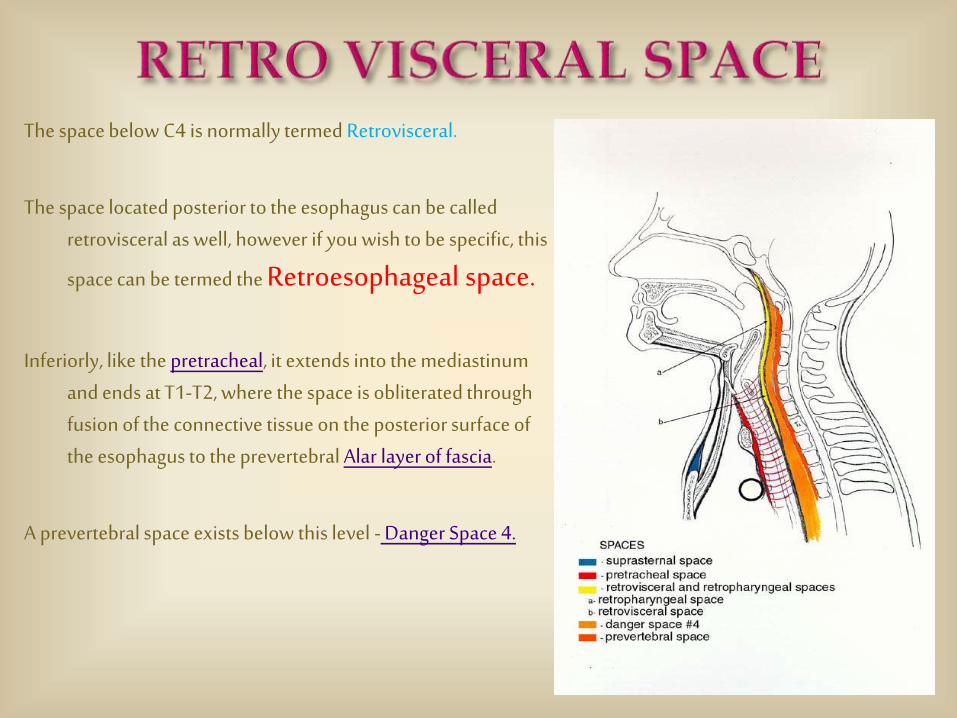
The space below C4 is normally termed Retrovisceral.
The space located posterior to the esophagus can be called retrovisceral as well, however if you wish to be specific, this
space can be termed the Retroesophageal space.
Inferiorly, like the pretracheal, it extends into the mediastinumand ends at T1-T2, where the space is obliterated through fusion of the connective tissue on the posterior surface of the esophagus to the prevertebral Alar layer of fascia.
A prevertebral space exists below this level - Danger Space 4.

Clinical
Important pathway by which infections orginating from various locations in the head and the upper portion of the neck reach the mediastinum.
The retrovisceral space may also be infected directly from posterior perforations of the esophagus or by infections of the deep cervical nodes lying adjacent to it.
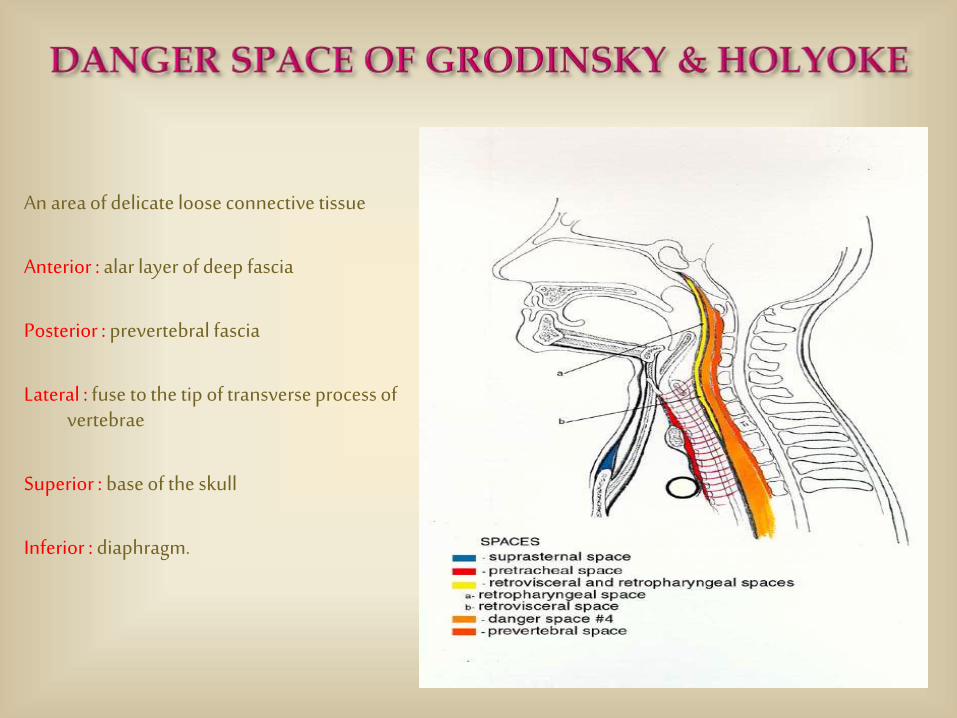
An area of delicate loose connective tissue
Anterior : alar layer of deep fascia
Posterior : prevertebral fascia
Lateral : fuse to the tip of transverse process of vertebrae
Superior : base of the skull
Inferior : diaphragm.
Infection can communicate from posterior wall of the oropharynx and oral cavity to the thorax by traveling from the Retropharyngeal Space, and passing downward to the Retrovisceral space (which begins below the pharynx).
It can then pierce thru the weak alar fascia - into Danger Space #4
"Dangerous" because an infection can easily travel to the thoracic cage and mediastinum, i.e., mediastinitis , empyema , sepsis
Abscess in the mediastinum could go anteriorly to the pericardial area and could affect the manubrium, sternum, etc..
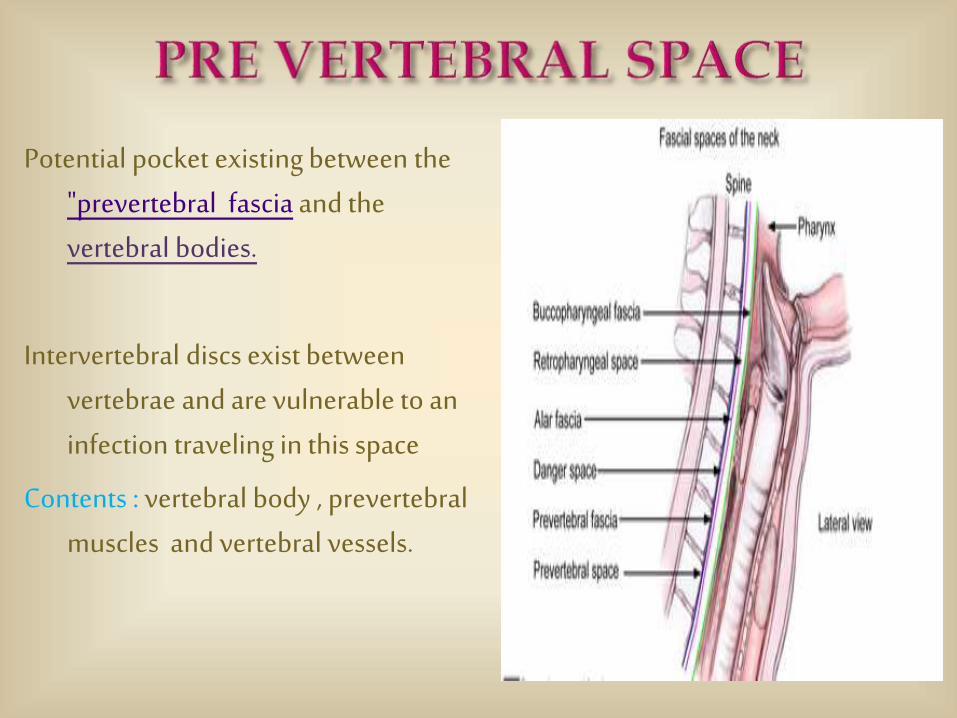
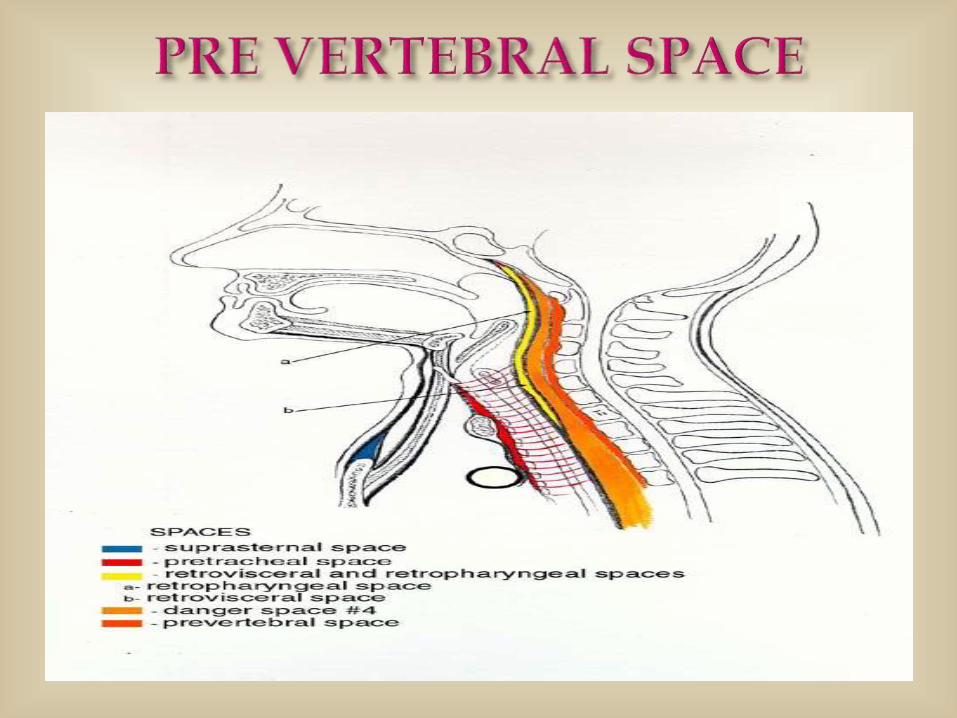
Potential pocket existing between the "prevertebral fascia and the vertebral bodies.
Intervertebral discs exist between vertebrae and are vulnerable to an infection traveling in this space
Contents : vertebral body , prevertebralmuscles and vertebral vessels.

Superiorly : Skull base
Inferiorly : Coccyx
Anteriorly : RetroPharyngeal Space & Danger Space ,
Anterolaterally : Carotid Space
Posteriorly - vertebral bodies and deep neck muscles
Lateraly – transverse processes
Any mass in prevertebral space will displace the retropharyngeal space and the prevertebral muscles anteriorly, if the leision is primary to the vertebral body.
Infection in the neck can track even to psoas muscle due to its anatomical continuity.
Secondary metastsis is more common than the primary
Leukemia and myeloma can also been seen
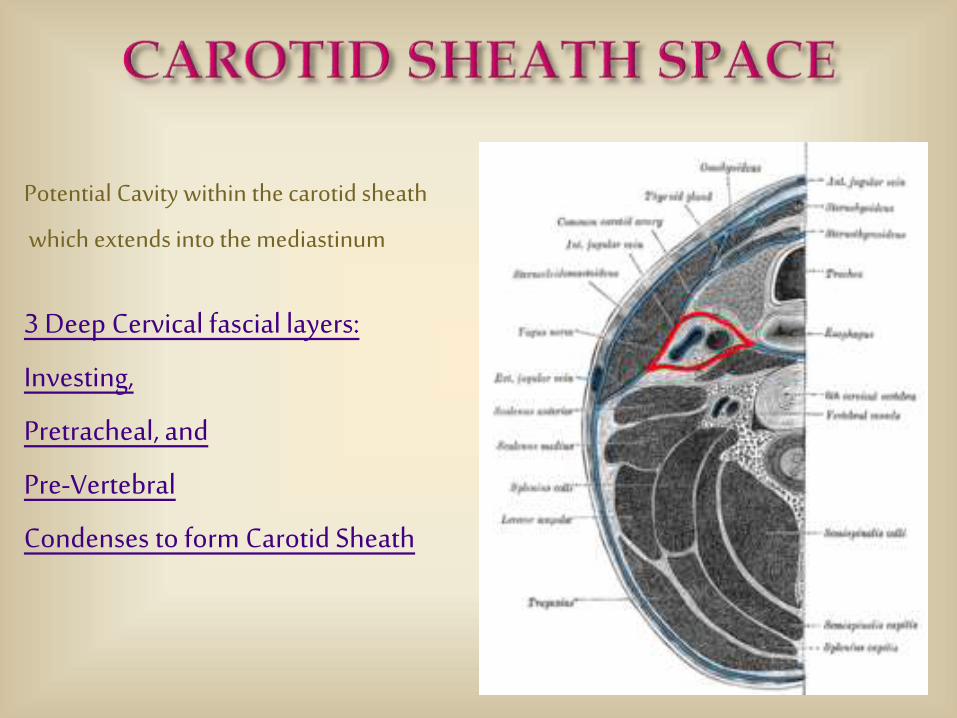
Potential Cavity within the carotid sheath
which extends into the mediastinum
3 Deep Cervical fascial layers:
Investing,
Pretracheal, and
Pre-Vertebral
Condenses to form Carotid Sheath

Contains the carotid artery , internal jugular vein , lymphatics , cranial nerves IX through XII and sympathetic trunk behind.
Extends from the base of skull (where it communicates with the carotid canal or jugular foramen ) to aortic arch at the level of root of neck .
Anterolateral wall is composed of investing layer , deep to sternomastoid , and pre-tracheal layers.
Posterior and medial wall : Pre-vertebral layer of cervical fascia.
Laterally related with parotid space , anteriorly with parapharyngeal space , and medially with retropharyngeal space , posteriorly the vertebral bodies of the cervical spine
- Common and internal carotid arteries
-Internal Jugular vein
-Vagus nerve (CN X)
-Deep cervical lymph nodes
-Sympathetic fibers
-In the upper part, the carotid sheath also contains the glossopharyngeal nerve (IX), the accessory nerve (XI), and the hypoglossal nerve (XII), which pierce the fascia of the carotid sheath.
-Sheath is extremely strong which prevents easy compression.
(Therefore a problem in the carotid sheath can crush the internal jugular vein and vagus nerve)
Clinical : It can be involved in any neck infection because it is made of those three layers: Investing, Pretracheal and Prevertebral Fascia.
Infections (between hyoid and root of the neck) because the sheath is closely adherent to vessels & also arises from thrombosis of the internal jugular vein (“Picket Fence” type of fever) , carotid artery thrombosis , or from infection of those deep cervical lymph nodes that lie within the sheath .
Drug use (Heroin) usually use carotid route to obtain a fast high. A result can be abscess of the carotid sheath presenting in a patient who is groggy with a weak pulse (bradycardia) and low blood pressure due to the compression of the carotid sinus and irritation of the vagus nerve.
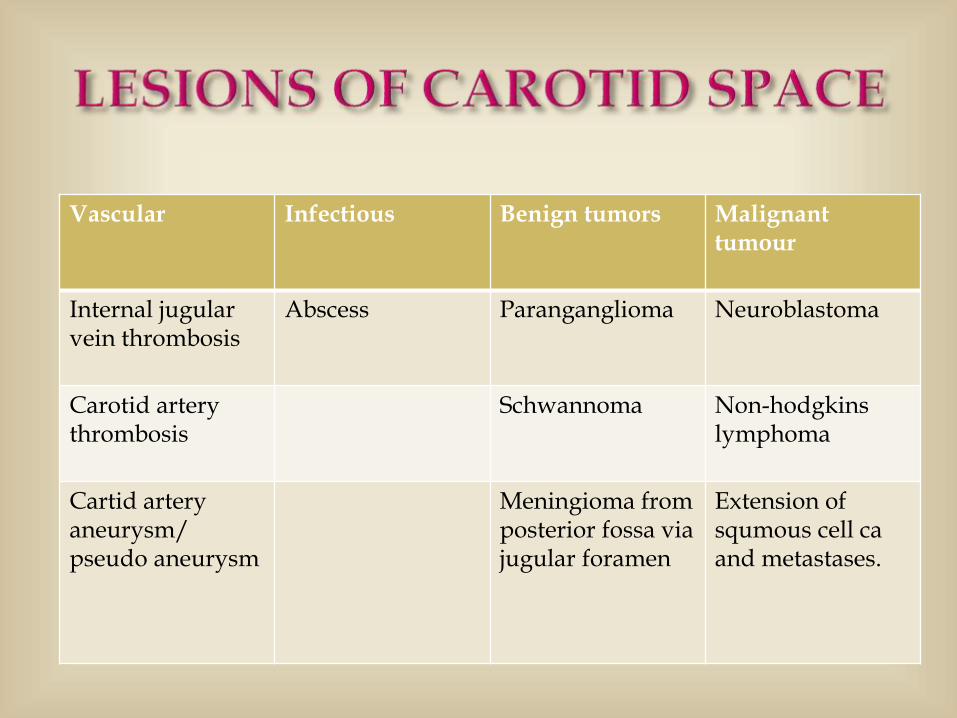
Vascular Infectious Benign tumors Malignant tumour
Internal jugular vein thrombosis
Abscess Paranganglioma Neuroblastoma
Carotid artery thrombosis
Schwannoma Non-hodgkinslymphoma
Cartid artery aneurysm/pseudo aneurysm
Meningioma from posterior fossa via jugular foramen
Extension of squmous cell ca and metastases.

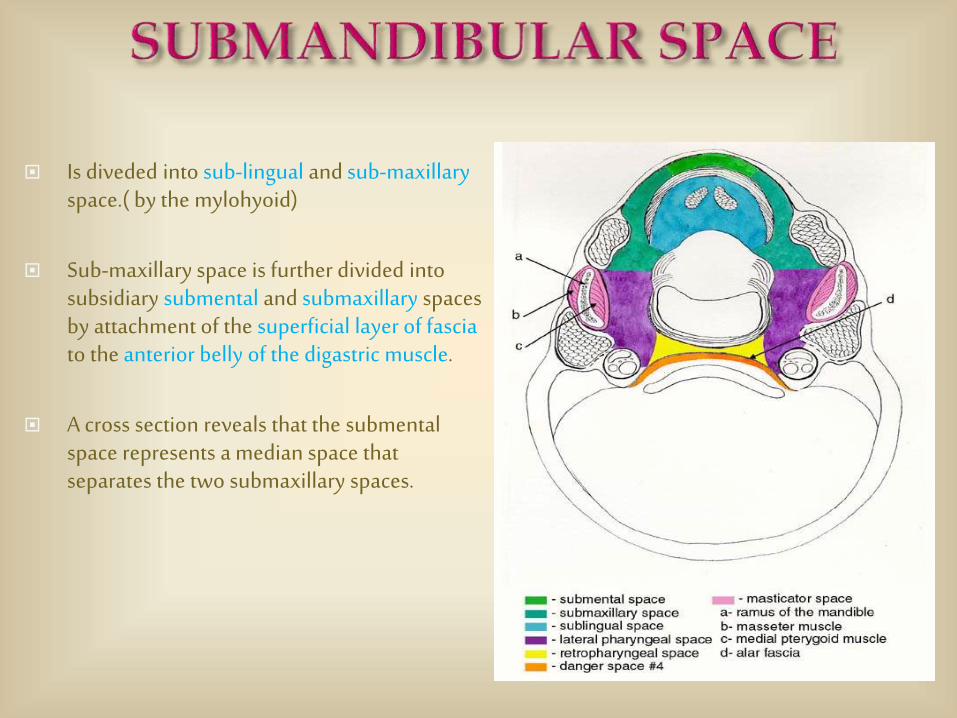
Is diveded into sub-lingual and sub-maxillary space.( by the mylohyoid)
Sub-maxillary space is further divided into subsidiary submental and submaxillary spaces by attachment of the superficial layer of fascia to the anterior belly of the digastric muscle.
A cross section reveals that the submentalspace represents a median space that separates the two submaxillary spaces.
Inferior : Superfacial layer of the deep cervical fascia extending from the hyoid to the mandible.
Laterally and Anteriorly : Body of mandible
Posteriorly : Hyoid bone
Superiorly : Mucosa of floor of the mouth
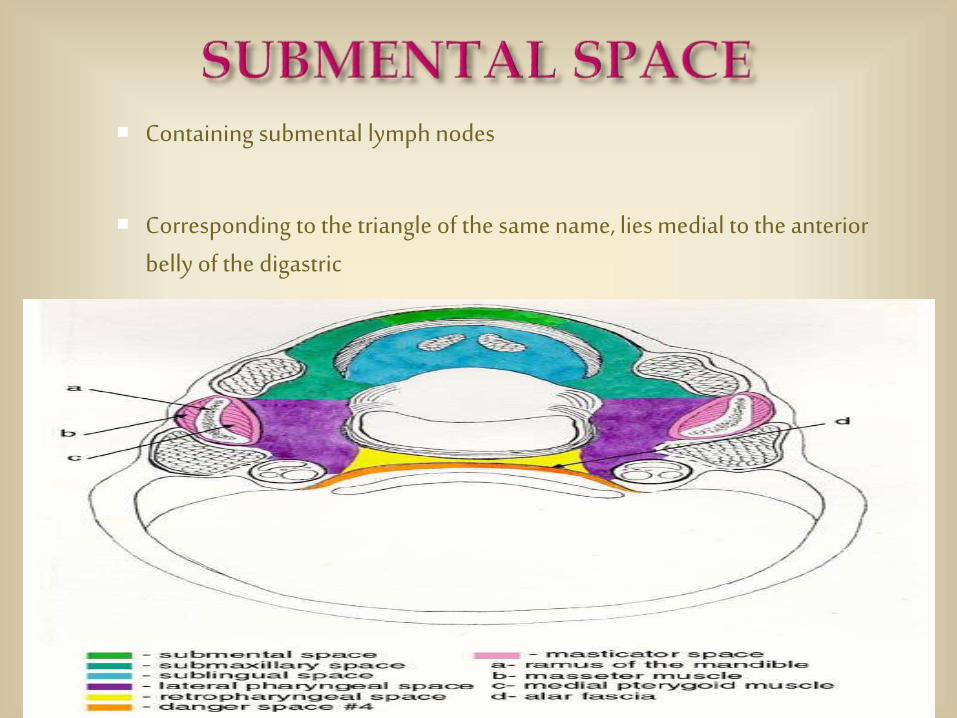
Containing submental lymph nodes
Corresponding to the triangle of the same name, lies medial to the anterior belly of the digastric
Lateral and posterior to sub-mental space
Contains Submandibular Gland with its fascial covering, Facial Artery and Vein, Hypoglossal Nerve, Vena hypoglossi commitantes
These spaces consist only of an easy line of cleavage between the fascia and the muscles, unless they are abnormally distended.
The roots of the third, second, and first molars are all below the level of the mylohyoid.
Infection of these teeth pass through the root, directly into the submaxillaryspace and then to the lateral pharyngeal space.
Patient can present with problems in their airway.
Never give a nerve block if there is an infection of the submandibular space.
Infection can be passed by way of a needle tract infection to a deeper area of the body.
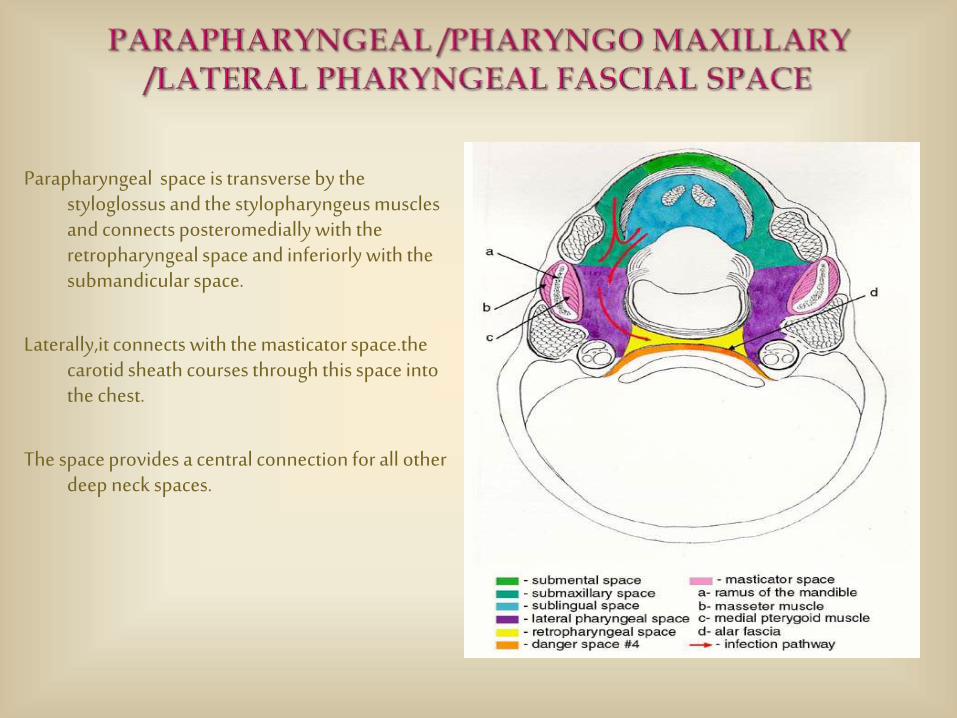
Parapharyngeal space is transverse by the styloglossus and the stylopharyngeus muscles and connects posteromedially with the retropharyngeal space and inferiorly with the submandicular space.
Laterally,it connects with the masticator space.thecarotid sheath courses through this space into the chest.
The space provides a central connection for all other deep neck spaces.
Boundaries: base of skull superiorly,
medially pharynx or buccopharyngeal fascia over the constrictors.
Posterolaterally parotid gland with the deep layer of the deep cervical fascia.
Anterolaterally, ramus of the mandible with the medial pteryoid on its inner side.
Posteriorly, carotid sheath and its contents but separated by the styloidapparatus and the prevertebral fascia.
The lateral pharyngeal space can be divided into anterior and posterior compartments by the styloid process and its attachmanets namely the 3 muscles and 2 ligaments shortly known as the RIOLAN’S BOUQUET.
The prestyloid compartment called the muscular compartment the internal maxillary artery,inferior alveolar nerve,lingual nerve and auriculotemporal nerve,fat,lymph nodes and muscles.
The retrostyloid comparantments known as the neurovascular comparantment contains the carotid and internal jugular vessels,sympahtic chain as well as cranial nervers IX through XII.
The accessory nerve is somewhat protected from pathological process in this region by its position behind the sternocleidomastoid muscle.
1.infections can srise from the tonsils,pharynx,dentition,salivary glands,nasal infections,petrous portion of the temporal bone or bezold abscess.
Infections of the prestyloid comparantment present with pain,fever,external swelling below the angle of jaw,prolapsed of tonsils,tonsillar fossa and trismus.
Omnious signs of retrosyloid comparantment involvement include Horner syndrome.
Cranial nerve IX and XII palasis,bulge of pharynx behind the posterior pillar and complications include septic jugular thrombophlebits and carotid artery erosion or thrombosis
Hematogenous dissemelation can also occur with the major vessel involvemet.
Drainage is by using a horizontal incision or an incision along the anterior border of the sternomastoid.
2. The parapharyngeal space absess reaches the mediastinum through the
“LINCONS HIGHWAY”(CAROTID SHEATH).
3. EAGELS SYNDROME: it is seenin cases of congenital elongated styloid process or acquired elongation due to ossification of the stylohyoid ligament. The elongated styloid process impinges on the glossopharyngeal nerve and produces stylalgia.
4.Asuperficial parotid swelling like plemorphic adenoma can pass through the stylomandibular tunnel and may present in the parappharyngeal space forming a Dumb Bell tumour.
5. Masses in the surrounding spaces displace the pharyngeal space fat. Assessing the centre oda deep fascial mass relative to the parapharyngeal space and observing the direction in which this mass displaces the fat,the site of the lesion can be localized radiologically.
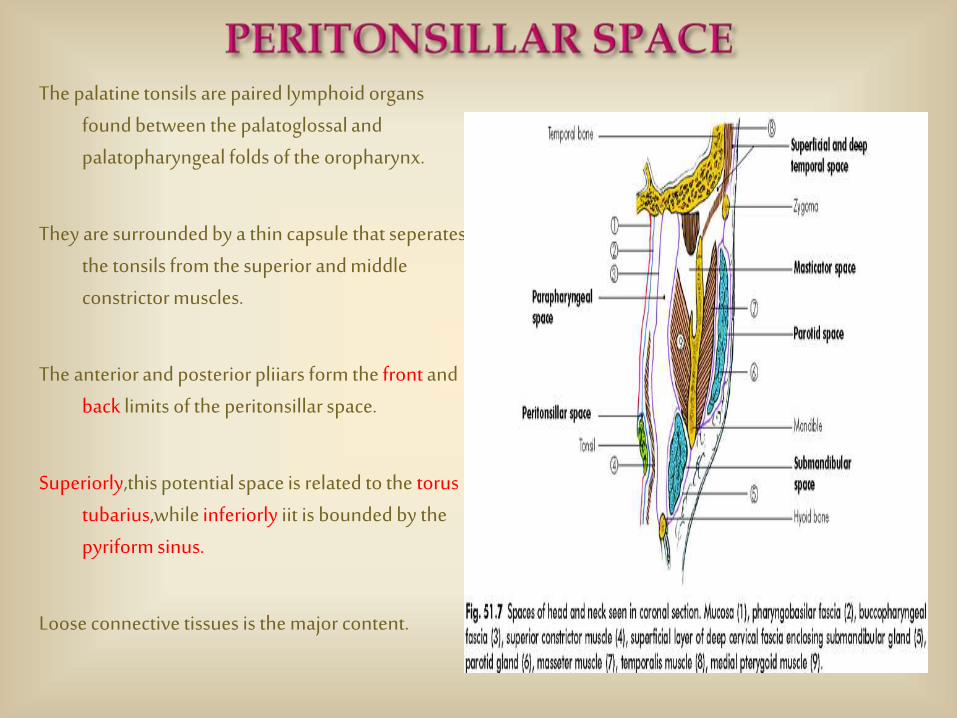
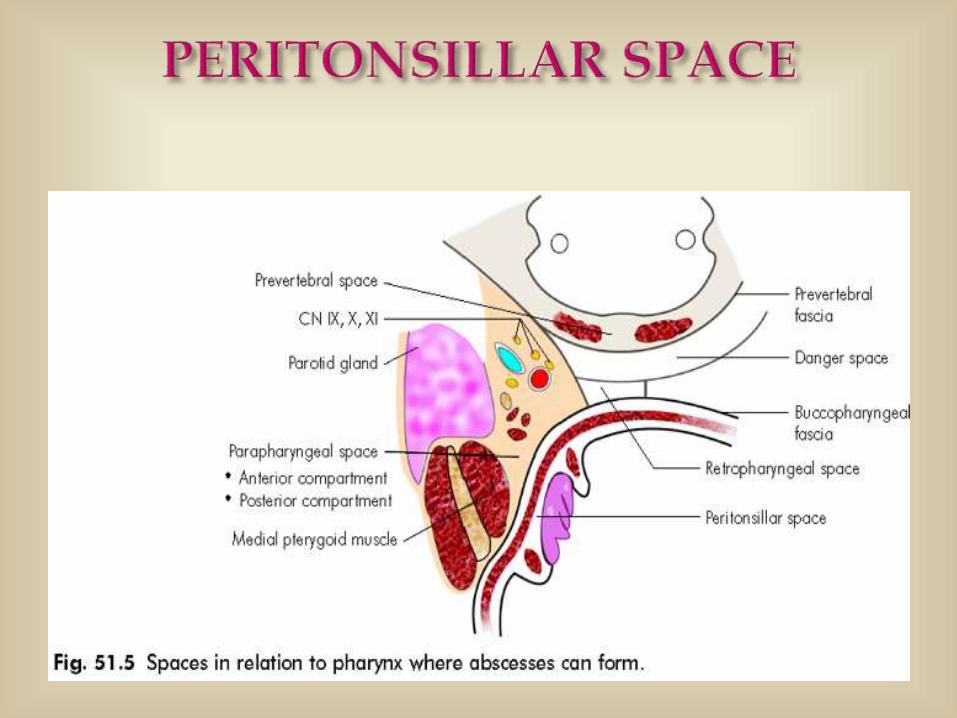
The palatine tonsils are paired lymphoid organs found between the palatoglossal and palatopharyngeal folds of the oropharynx.
They are surrounded by a thin capsule that seperatesthe tonsils from the superior and middle constrictor muscles.
The anterior and posterior pliiars form the front and back limits of the peritonsillar space.
Superiorly,this potential space is related to the torus tubarius,while inferiorly iit is bounded by the pyriform sinus.
Loose connective tissues is the major content.
Applied clinical significance
1.Peritonsillar abscess/quinsy is produced usually following tonsillitis and presents with odynophagia,hot potato voice,trisums,ipsilateral otalgia. The inflammation and suppurative process of the space may extend to involve the soft palate , the lateral wall of the pharynx and occasionally, the base of the tongue.
2.The tonsillar fossa has a rich network of lymphatic vessels leading to the paraphyngealspace and the upper cervical lymph nodes.which explains the pattern of adenopathyObserverd clinically. Ipsilateral upper cervical lymphadenopathy is the result of the spread of the infection to the regional lympahtics. occasionally the severity of the suppurativeprocess may lead to the cervical abscess,especially in very fulminant or rapidly progressive cases.

3. Early absesses generally extend superior and anterior. Later posterior extension allows it to decompress into the parapharyngealspace. Hence all peritonsillar abscesses are potential parapharyngealor retropharyngeal abscesses.
4. The treatment includes Hydration,Analgesics,Antibiotics,Surgicalintervation including I&D with interval tonsillectomy.

Superior : skull base
Inferior : inferior surface of mandible.
Superomedially : the fascia attaches to the skull base just medial to foramen ovale
Superolaterally : zygomatic arch
Laterally : medial pterygoid fascia
Medially : masseter muscle
Anterolateraaly : parapharyngeal space

CONTENTS :
Pterygoid and Massetor muscles
Insertion of Temporalis tendon
Inferior Alveolar nerve & vessels
Clinical
Infections of the zygomatic or temporal bones may pass to the masticator space, and so may abscesses from the lower molar teeth
Abscesses within this space may apparently point at the anterior aspect of the massetermuscle, either into the cheek or the mouth, or they may point posteriorly below the parotid gland.
Drainage : Intraoral approach
External approach : Horizontal incision along the angle of mandible.
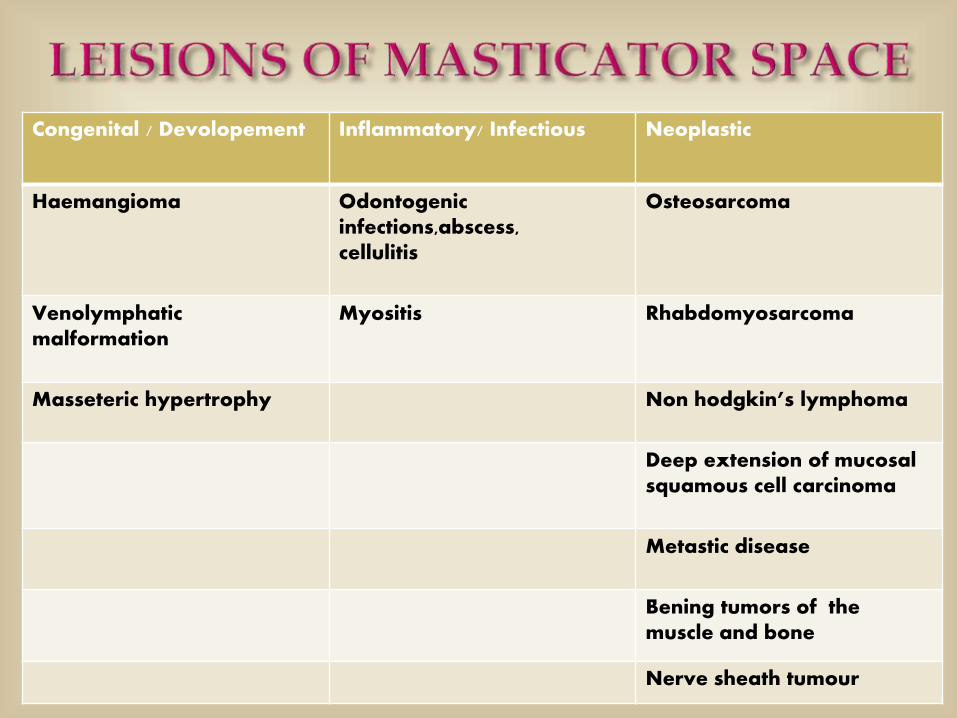
Congenital / Devolopement Inflammatory/ Infectious Neoplastic
Haemangioma Odontogenicinfections,abscess,cellulitis
Osteosarcoma
Venolymphaticmalformation
Myositis Rhabdomyosarcoma
Masseteric hypertrophy Non hodgkin’s lymphoma
Deep extension of mucosal squamous cell carcinoma
Metastic disease
Bening tumors of the muscle and bone
Nerve sheath tumour
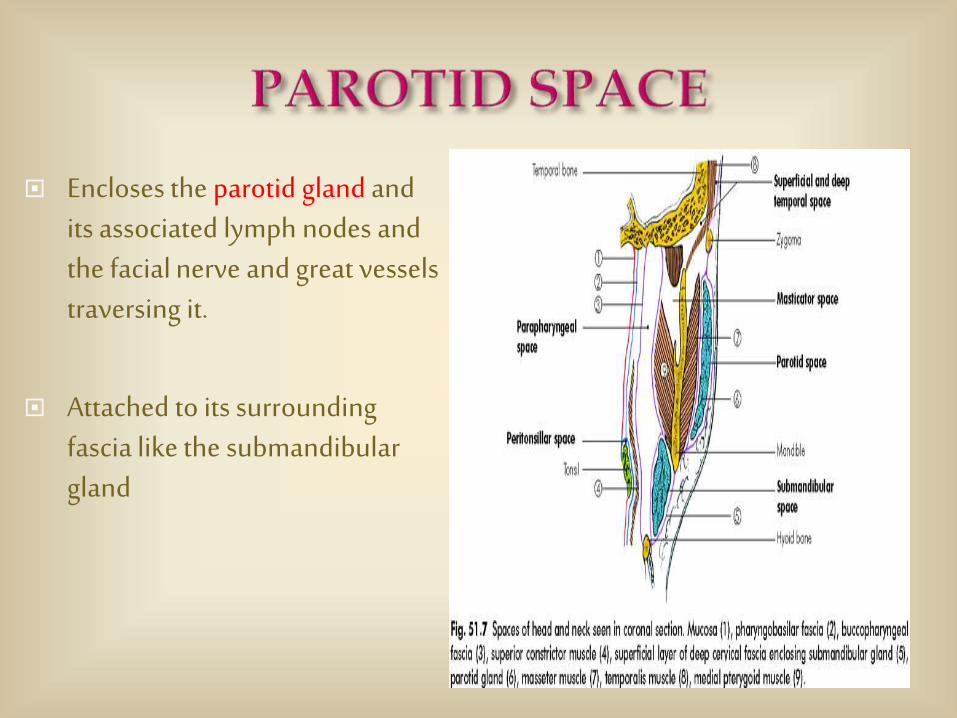
Encloses the parotid gland and its associated lymph nodes and the facial nerve and great vessels traversing it.
Attached to its surrounding fascia like the submandibulargland

Anteriorly : Masticator space
Anterolaterally : Parapharyngeal Space
Posteromedially : Carotid Space
Laterally : Sub-cutaneous fat
Postero-superiorly : Temporal bone

Contents :
Parotid gland
Facial nerve
Intraparotid lymphnodes
Parotid duct exits anteriorly
External carotid artery
Posterior facial vein
Clinical: Though the deep surface of the parotid gland is strong, infections (usually of the glands or the nodes) may readily pass deeply and therefore into the important lateral pharyngeal space lying deep to the parotid gland.
When orally palpating and examining the area, it is important to note that the deep fascia around the parotid gland is weaker medially than laterally . Therefore an infection in this space can evidence itself as a bulge that sticks out medially into the oral cavity.
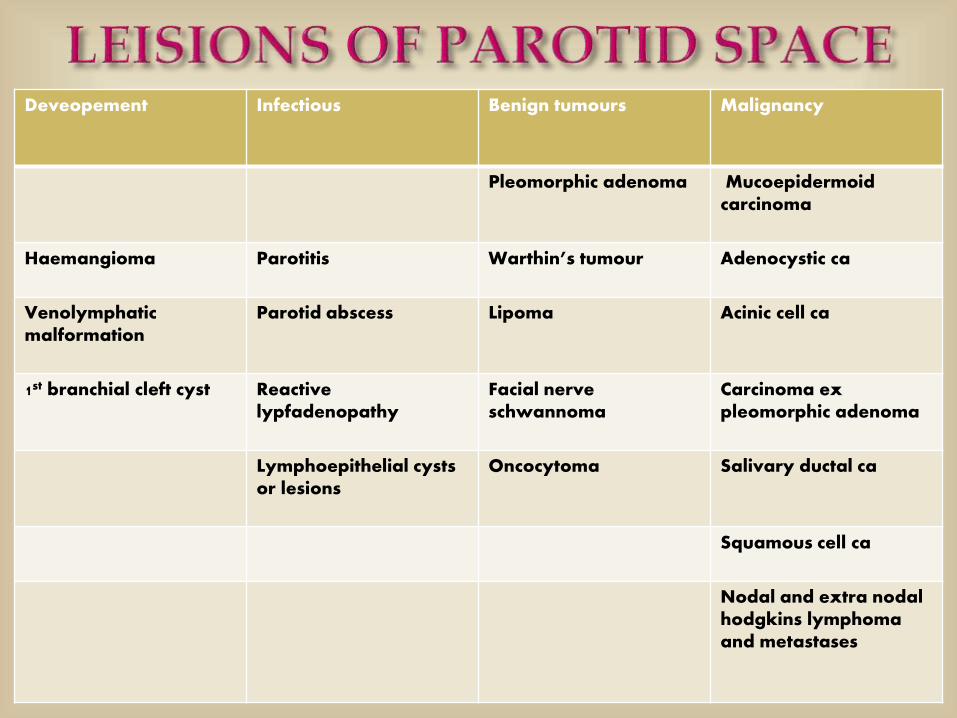
Deveopement Infectious Benign tumours Malignancy
Pleomorphic adenoma Mucoepidermoidcarcinoma
Haemangioma Parotitis Warthin’s tumour Adenocystic ca
Venolymphaticmalformation
Parotid abscess Lipoma Acinic cell ca
1st branchial cleft cyst Reactive lypfadenopathy
Facial nerve schwannoma
Carcinoma ex pleomorphic adenoma
Lymphoepithelial cysts or lesions
Oncocytoma Salivary ductal ca
Squamous cell ca
Nodal and extra nodal hodgkins lymphoma and metastases
Defined by both the superficial and deep layer of the deep cervical fascia.
Superior : Skull base
Inferior : Clavicle
Anterior : Carotid space
Medial : Peri-vertebral Space
Lateral : Sternomastoid & Sub-cutaneous fat.
Contents :
Fat
Cranial nerve XI
Lymph nodes
Trunks of branchial plexus

Bounded anteriorly by pretracheal fascia and posteriorly by prevertebral fascia
Contents :
Thyroid gland
Parathyroid gland
Larynx
Trachea
Hypopharynx
Osephagus
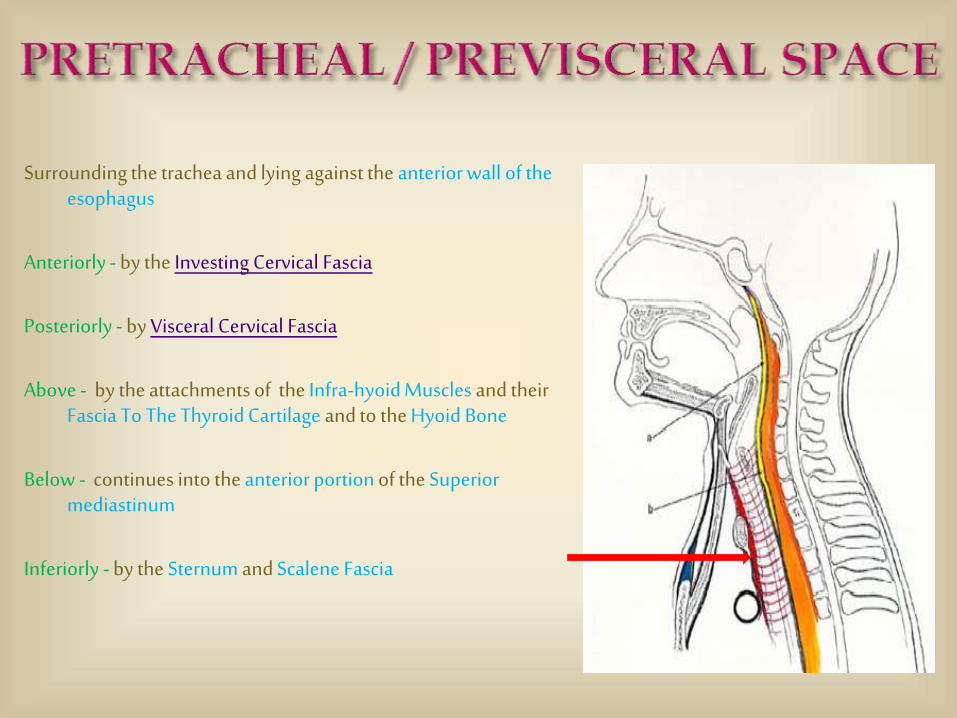
Surrounding the trachea and lying against the anterior wall of the esophagus
Anteriorly - by the Investing Cervical Fascia
Posteriorly - by Visceral Cervical Fascia
Above - by the attachments of the Infra-hyoid Muscles and their Fascia To The Thyroid Cartilage and to the Hyoid Bone
Below - continues into the anterior portion of the Superior mediastinum
Inferiorly - by the Sternum and Scalene Fascia
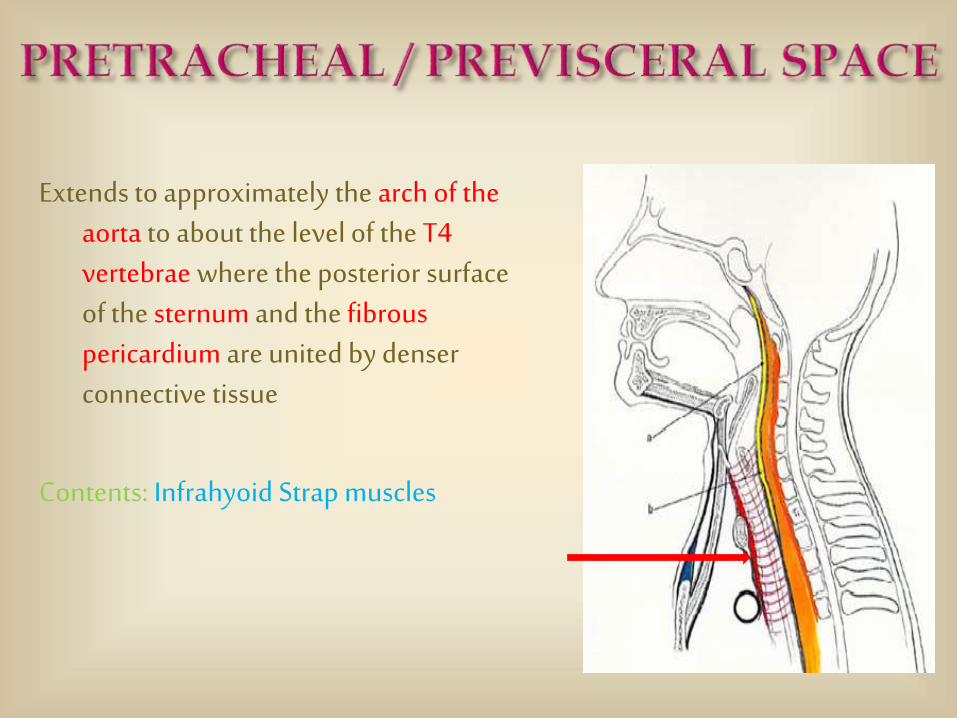
Extends to approximately the arch of the aorta to about the level of the T4 vertebrae where the posterior surface of the sternum and the fibrous pericardium are united by denser connective tissue
Contents: Infrahyoid Strap muscles
Clinical:
Can be infected directly by anterior perforations or rupture of the esophagus or indirectly by spread from the retrovisceral portion, around the sides of the esophagus and thyroid gland between the levels of the inferior thyroid artery and the oblique line of the thyroid cartilage.
Both pretracheal and retrovisceral spaces descend into the superior mediastinum.
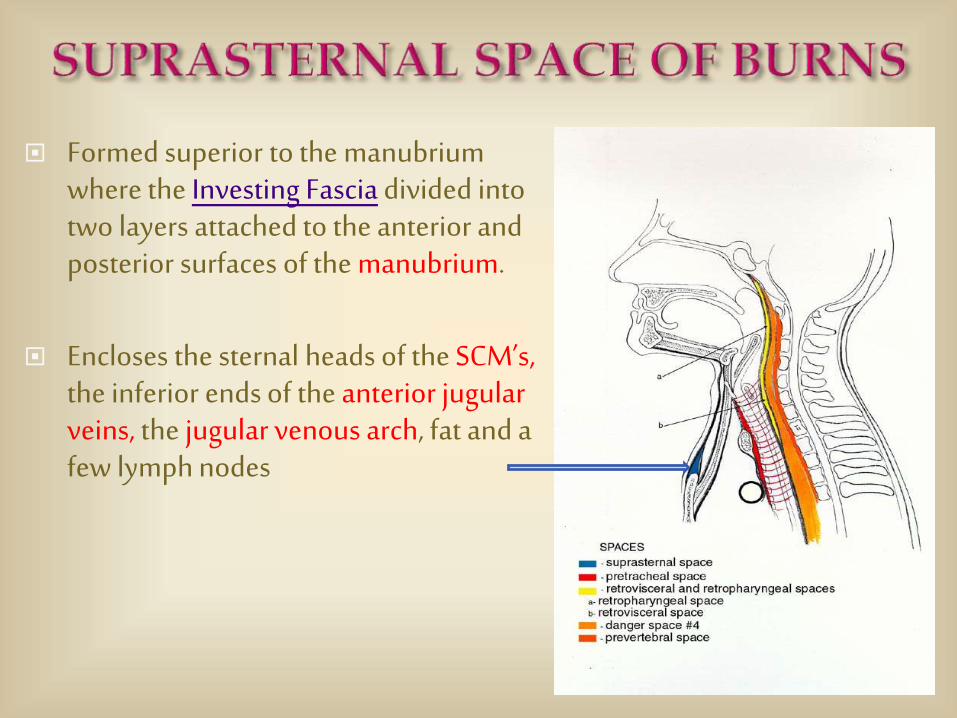
Formed superior to the manubriumwhere the Investing Fascia divided into two layers attached to the anterior and posterior surfaces of the manubrium.
Encloses the sternal heads of the SCM’s, the inferior ends of the anterior jugular veins, the jugular venous arch, fat and a few lymph nodes
Clinical:
Above this space lies the JACKSON’S TRIANGLE (used for tracheostomy) formed superiorly by the cricoid cartilage and on either side by the anterior border of the sternemastoids.
Trauma to this SPACE can cause a bleeder and subsequently a large bulging above the manubrium and even might distend down posterior to the manubrium into the superior mediastinum.
Near the root of the neck the investing layer splits into 2 layers, the superficial layer attaches to the upper border and the deep layer attaches to the lower border of the back of the clavicle in the region of the lower part of the post. triangle thereby creating the omohyoid space
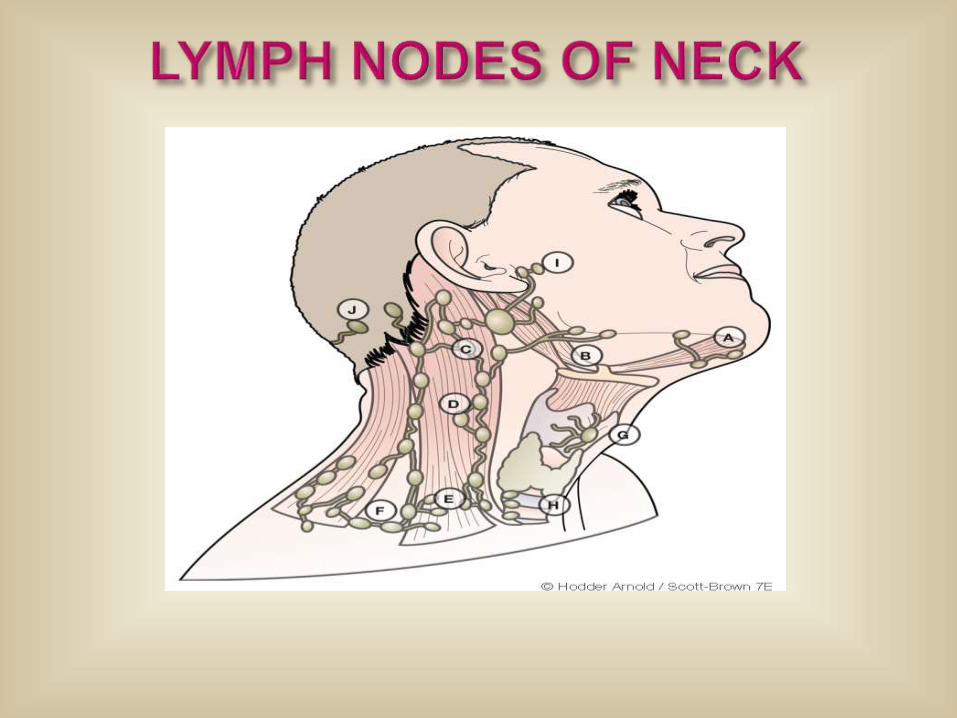
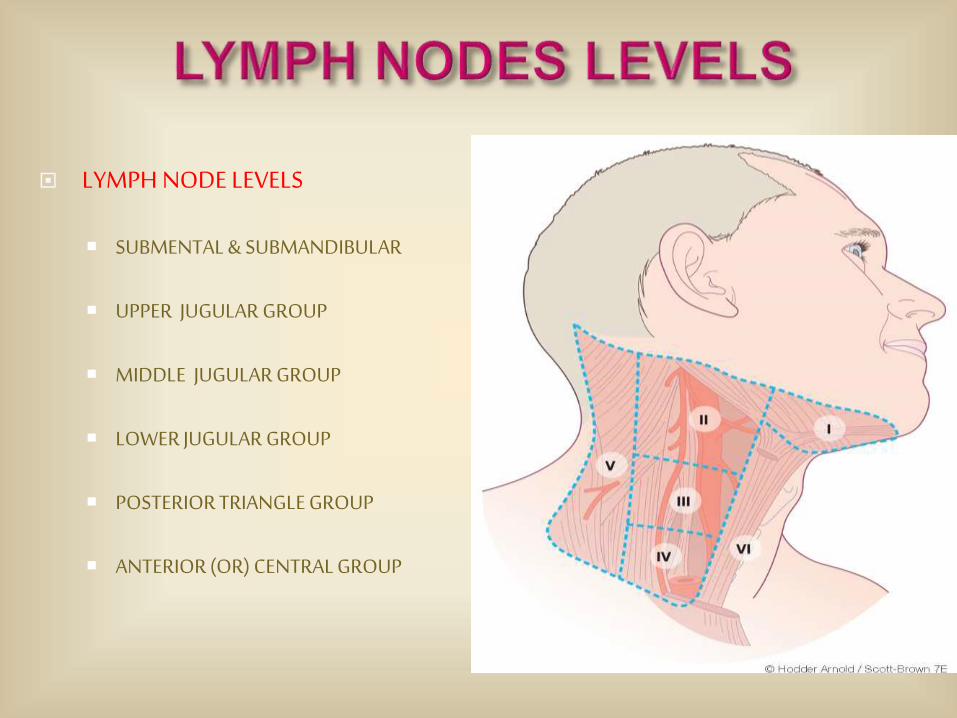
LYMPH NODE LEVELS
SUBMENTAL & SUBMANDIBULAR
UPPER JUGULAR GROUP
MIDDLE JUGULAR GROUP
LOWER JUGULAR GROUP
POSTERIOR TRIANGLE GROUP
ANTERIOR (OR) CENTRAL GROUP
IA – Sub-mental nodes
Drains : anterior floor of mouth , lower lip & ventral tongue.
IB – Sub-mandibular nodes
Drains : Other subsites in oral cavity
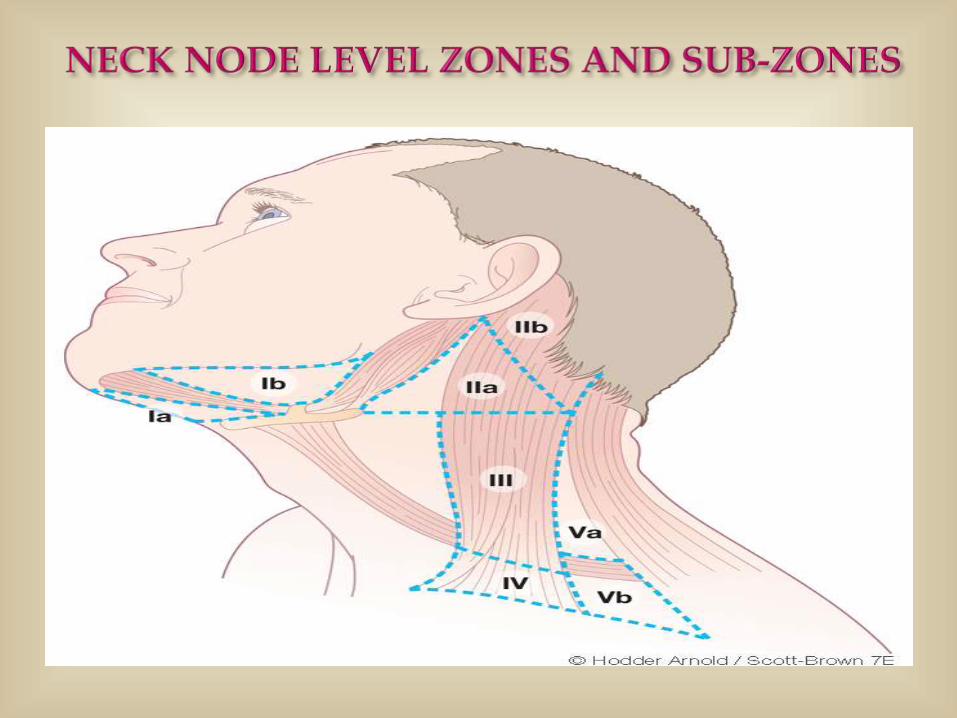
II A – Lies antero-inferior to the spinal accessory nerve
II B – Lies postero-superior to the spinal accessory nerve
(also known as sub-muscular recess)
Drains : oropharynx , larynx , hypopharynx & parotid.
LEVEL III is not further sub-divided.
Drains : pharynx & larynx
LEVEL IV is not further sub-divided.
Drains : Hypopharynx & larynx
VA – Superior To The Inferior Belly Of Omohyoid
Drains : Nasopharynx( contain the chain along the accessory nerve)
VB – Inferior To The Inferior Belly Of Omohyoid
Drains : Thyroid gland ( more related to thryocervical trunk)
Includes Paratracheal , Perithyroidal & Delphian nodes