Embed Size (px)
DESCRIPTION
neuro
Citation preview

1
NEUROMUSCULAR NEUROMUSCULAR JUNCTION DISEASEJUNCTION DISEASE
Alina Valdes, M.D.

2
BackgroundBackground • Disorders of neuromuscular junction interfere with
transmission of electrical impulses from peripheral nerve to muscle
• Acquired or inherited
• Weakness and fatigability on exertion
• Specific defects:– Acetylcholine (ACh) synthesis or packaging into
synaptic vesicles– Release of ACh from nerve terminal by nerve impulse– Efficiency of released ACh to generate postsynaptic
depolarization

3
Myasthenia GravisMyasthenia Gravis• Acquired autoimmune disorder• Pathogenic autoantibodies induce ACh
receptor deficiency at motor end plate• Circulating AChR antibodies present in 80%
to 90% of cases• IgG and complement components deposited on
postsynaptic membrane• Female-to-male ratio is 6:4• Peaks in women in third decade and in men in
sixth or seventh decade

4
• Symptoms– Ocular MG
• Involves external ocular muscles selectively• Usually bilateral, asymmetric, and associated with
ptosis and diplopia
– Generalized MG• Involves general voluntary muscles
– Symptoms may fluctuate from hour to hour, from day to day, or even longer periods
– Provoked or worsened by exertion, temperature extremes, infections, menses, and excitement

5
– Fatigue most reliably shown in eyes• Curtain sign of worsening ptosis with upgaze
or asymmetric nystagmus on extremes of lateral and medial gaze
– Proximal limb muscles affected more than distal
– ⅔ have thymic hyperplasia
– 10% to 15% have thymoma
– 10% have another autoimmune disease

6
• Diagnosis– Anticholinesterase tests
• IV edrophonium: acts within few seconds and lasts few minutes; assess degree of ptosis and range of ocular movements
– Electromyography• Supramaximal stimulation results in 10% or greater
decrement of amplitude of evoked potential from first to fifth response
• Test positive in most patients with generalized MG
– Blood tests• AChR antibody test measures binding of antibody to
AChR labeled with radioactive α-bungarotoxin• Test positive in nearly all adults with moderately
severe to severe MG

7
• Treatment– Anticholinesterases
• Useful in all forms of disease• Pyridostigmine bromide: fewer muscarinic side effects• Neostigmine bromide
– Thymectomy• Increases remission rate• Improves clinical course• Thymoma indication for removal since locally
invasive
– Alternate-day prednisone• Induces remission or improves disease in >½ of
patients

8
– Azathioprine• Induces remission or improvement in >½ of patients• Need 12 to 15 months for improvement• Adjunct to alternate-day prednisone to reduce side
effects
– Cyclosporine
– Plasmapheresis• Helpful in patients with sudden worsening• Indicated in severe, generalized, refractory MG
– IV immunoglobulin• May improve severe MG with 2 to 3 weeks of therapy

9
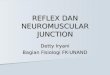
Myasthenia gravis. The edrophonium (Tensilon) test can be used to confirm the diagnosis. Facial weakness is provoked by repeated facial movements (left of slide). Edrophonium chloride, a short-acting anticholinesterase, is then injected intravenously – initially, 2 mg as a test dose, followed after one minute by a further 8 mg if there are no adverse effects. In myasthenia gravis the facial weakness is rapidly relieved by this test (right of slide). Objective testing of muscular power elsewhere in the body will reveal similar responses.

10
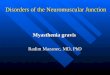
Thymoma (arrow) in a patient with myasthenia gravis. A lateral film confirmed that this mass was in the anterior mediastinum. The differential diagnosis of this appearance includes lymphadenopathy, retrosternal thyroid tissue or a dermoid tumor; but in the presence of myasthenia gravis, thymoma is the most likely diagnosis. Thymectomy may result in cure or great improvement in the myasthenia.

11
Lambert-Eaton Myasthenic Lambert-Eaton Myasthenic SyndromesSyndromes
• Acquired autoimmune disease• Pathogenic autoantibodies cause deficiency of
voltage-sensitive calcium channels at motor nerve terminal
• In patients >40 years old, 70% of men and 30% of women have associated carcinoma, usually small cell of lung
• Non-neoplastic syndrome associated with other autoimmune disorders
• Weakness and fatigability of proximal limb and trunk muscles

12
• Relative sparing of extraocular and bulbar muscles
• Lower limbs more severely involved• Tendon reflexes usually hypoactive or absent• Autonomic manifestations in 50% of patients
– Dry mouth, impotence, decreased sweating, orthostatic hypotension, or altered pupillary reflexes
• Treatment– Corticosteroids, azathioprine, and IV immune
globulin

13
Drug-Induced Myasthenic Drug-Induced Myasthenic Syndromes Syndromes
• Symptoms not usually appear unless overdose or renal or hepatic elimination impaired
• Drugs may worsen syndromes– Polymixin and aminoglycoside antibiotics– Antiarrhythmic agents (procainamide, quinidine)– β-adrenergic blockers (propranolol, timolol)– Phenothiazines, lithium– Succinylcholine, curare and related drugs– Trimethaphan– Methoxyflurane– Magnesium given parenterally or in cathartics

14
Organophosphate Organophosphate IntoxicationIntoxication
• Irreversibly inhibit cholinesterases
• Alterations in sensorium, convulsions, coma, severe muscarinic side effects, cramps, fasciculations, and muscle weakness from depolarization block