Embed Size (px)
Citation preview

Ocular Emergencies
Capt RIFATMedical Officer7 Fd Amb

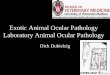
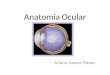
Anatomy of the Eye

OCULAR EMERGENCIES
Conjunctivitis, IritisPeriorbital CellulitisStyeGlaucomaCorneal
Abrasion,laceration,ulcer
Extraocular Foreign Bodies
Subconjunctival hemorrhage
Chemical BurnsRetinal DetachmentOrbital FractureHyphemaEyelid LacerationGlobe RuptureCetral retinal artery
occlusionRetrobulber Hematoma

AssessmentHistory Gross assessment External appearance Always use contralateral eye for comparison Edema of lids, Conjunctiva and sclera for color and inflammation Hazy cornea Opaque, gray-white area of cornea Lesions, Foreign body
Pupils

Fine assessmentDirect ophthalmoscopyTonometryFluorescein stainingSlit-lamp examInvestigations
Culture and sensitivityCBCPlain X ray of skull and orbitCT scan

Priorities
ABCsPrevent further damagePrevent or minimize complicationsControl painRelieve anxiety

Common Ocular Emergencies

Conjunctivitis
Inflammation of the conjunctivaCauses:
bacterial/viral inflammation allergies Chlamydiachemical burnsFBIrritants

SymptomsHyperemiaUnilateral or bilateralSlight pain“Gritty” sensationDischarge
SignsEdema of eyelidsVisual acuity: NormalCornea: ClearPupil: NormalConjunctiva: red or pink

TreatmentAntibiotics
ointment/dropsObtain culture, if
indicatedCleanse eyes gently to
remove debrisAnti histamine
Prevention Explain contagious
nature Medication admin. Wipe from nose to
outer corner of eye Cleanse lid Avoid eye makeup

Iritis
Inflammatory process that includes the iris and sometimes the ciliary body
Predisposing conditions:rheumatic disease, and syphillis

SymptomsBlurring of visionUnilateral painEdema of upper lidRed eyePhotophobiaDecreased visual acuity Lacrimation
Redness at eyelashClear to hazy cornea
Small, irregular, sluggish reaction of pupils
Pain on eye pressure

TreatmentAnalgesics
Cycloplegics to paralyze ciliary muscle Darkened environment
Rest eyesWarm compresses Shield eyes or dark glassesFollow-up

Periorbital Cellulitis
Infection of the cells around the eye
May occur after trauma such as laceration or an insect bite
Pneumococcal, staphylococcal, streptococcal

SymptomsMarked periorbital edema and erythema.
Pain: severe that is aggravated by movement of eye
.Conjunctival infection.Fever.
Signs
Visual acuity: Decreased
Decreases pupil reflexes
Paralysis of EOM

Treatment
BedrestIV antibioticsWarm compresses

GlaucomaAcute angle-closure glaucoma occurs when the distance between the iris and the cornea becomes inadequate or is blocked completely.
The aqueous fluid production is greater than the amount leaving through the canal of Schlemn.
May lead to irrecoverable blindness.

Pathophysiology
Aqueous humor produced by ciliary body, enters ant. chamber, drains via trabecular meshwork at angle to enter canal of Schlemm
In AACG, iris obstructs trabecular meshwork by closing off angle
Optic nerve damage

SymptomsRed eyeSevere, sudden-onset, deep, unilateral painIntense headacheDecreased visual acuityHalos (around lights)Visual loss (usually peripheral)Nausea/vomiting
Signs:Conjunctival congestionCorneal edemaMid-dilated, fixed pupilHazy, lusterless corneaIncreased intraocular
pressure (>20 mm Hg)Rocklike hardness
DiagnosticTonometry

Medical TxReduce production of aqueous humor Topical -blocker (timolol) Carbonic anhydrase inhibitor (acetazolamide) Systemic osmotic agent (mannitol 1-2 g/Kg IV over 45
min)Or increase outflow Topical -agonist (phenylephrine) Miotics (pilocarpine 1-2%)Topical steroid (prednisolone acetate 1%)
Definitive Tx Laser peripheral iridectomy

Central retinal artery occlusion
Blockage of the the retinal artery by thrombus or embolus
Prompt recognition and intervention must be obtained within 1-2 hours of onset
Etiology:Emboli – cardiac, atherosclerotic, fatVasculitisCoagulopathySickle cell diseasesDiabetesHTN

Signs and Symptoms
Sudden onset monocular vision loss over seconds
PainlessVisual acuity is limited to light
perception in affected eyePupil reaction: dilated, nonreactive
in affected eye

Treatment of CRAO
Mannitol 0.25-2.0 g/kg IV or acetazolamide 500 mg PO once to reduce IOP.
IV anticoagulant, tPA
Oral nitrates
Lay the patient flat on his/her back Massage orbit. This is thought to help dislodge the clot from a larger to smaller retinal artery branch, minimizing area of visual loss.

Alkali burns more common and worse than acid
Alkali – saponification – denatures collagen, thromboses vessels
Household cleaners, fertilizers, drain cleaners
Acid – coagulation, H+ precipitates protein - barrier
Industrial cleaners, batteries, vegetablepreservatives
Chemical burns

Initial TreatmentImmediate copious irrigation
Topical anesthesia (tetracaine) Lids should be retracted and fornices swabbed Check pH with litmus paper after initial irrigation Continue irrigating until ph 7.0 – 7.3Once pH is stabilized Cycloplegic agent (0.25% scopolamine) Broad-spectrum antibiotic (ciprofloxacin,
ofloxacin, gentamicin, or tobramycin) should be applied.

Corneal Foreign bodyOften metallic foreign body following work injury.
Signs and symptoms: foreign body sensation, tearing, red, or painful eye. Pain often relieved with the instillation of anesthetic drops.
Stain with fluorescein stain and illuminate under blue fluorescent light (Wood’s lamp) is effective to see corneal epithelial defects.

TreatmentApply topical anesthetic
Remove foreign body with sterile irrigating solution or moistened sterile cotton swab
Never use needle
Apply antibiotic ointment
24-hour follow-up is mandatory
Refer if foreign body cannot be removed

Retrobulber hematoma
Hemorrhage into closed space of orbit IOP leading to vision loss from optic
nerve damage / retinal ischemiaClinical diagnosis:
Ocular pain, APD, proptosis, ophthalmoplegia, diminished vision, IOP
Immediate lateral canthotomy and cantholysis indicated if IOP > 40mmHg or vision loss

Corneal injuriesAbrasions, lacerations, ulcersSymptoms:
extreme eye pain, relieved with lidocaine drops.
Visual acuity usually decreased, depending on location of injury in relation to visual axis.
Inflammation leading to corneal edema
can decrease VA.Diagnosis: fluorescein staining to see
epithelial defect. Seidel’s test for aqueous
leakage to diagnose laceration.

Topical antibiotics and follow up with ophthalmologist.
For lacerations, <1 cm, topical antibiotics and discharge with follow up.
If >1 cm, refer to ophthalmologist to rule out globe rupture and for possible suture placement.Avoid contact lensesAvoid patching
Management of Corneal Injury

CONCLUSION

Any Question?