Embed Size (px)
Citation preview

Oral Mucositis in Cancer Care:Is The End in Sight?
Peter B. Lockhart, DDS, FDS RCPSChair, Department of Oral
Medicine Carolinas Medical Center

Oral MucositisOral Mucositis
Mucositis vs. stomatitisMucositis vs. stomatitis Inflammation vs. ulceration Inflammation vs. ulceration Chemotherapy- vs. radiotherapy-inducedChemotherapy- vs. radiotherapy-induced Complication vs. sequelaComplication vs. sequela
Is the end in sight?Is the end in sight?
Terminology:Terminology:

Absolutely
Absolutely
DoubtfulDoubtful
No wayNo way
PossiblyPossiblyNeverNever
Perhaps
Perhaps
LikelyLikely
YesYes
Could beCould be
NoNo

Oral MucositisOral Mucositis– “ “ collective consequence of a number of collective consequence of a number of
concurrent and sequential biological processes”concurrent and sequential biological processes”– Can be the most debilitating of side effectsCan be the most debilitating of side effects
– oral and GIoral and GI– Ranges from mild inflammation to ulcerationRanges from mild inflammation to ulceration

Who Oral Mucositis ScaleWho Oral Mucositis Scale Grade 0: No changesGrade 0: No changes
Grade 1: Soreness/erythema Grade 1: Soreness/erythema ■ ■ Grade 2: Ulceration/solid foods Grade 2: Ulceration/solid foods
Grade 3: Liquid diet Grade 3: Liquid diet ■ ■ Grade 4: No alimentation Grade 4: No alimentation

Oral Mucositis – IncidenceOral Mucositis – Incidence
High dose chemo. + Stem cell therapy High dose chemo. + Stem cell therapy Near 100% for Near 100% for anyany grade grade 30-50% Grade 3 & 4 without TBI30-50% Grade 3 & 4 without TBI >60% Grade 3 & 4 with TBI>60% Grade 3 & 4 with TBI
?

Mucositis Complications Mucositis Complications and Sequelaeand Sequelae
PainPain Oral infectionOral infection Systemic infection?Systemic infection? Bacteremia/SepsisBacteremia/Sepsis Oral bleedingOral bleeding XerostomiaXerostomia
TasteTaste Hydration/NutritionHydration/Nutrition FatigueFatigue Interrupted cancer Interrupted cancer
treatmenttreatment

Mucositis - ImpactMucositis - Impact
Drugs – antibiotics, pain medicationsDrugs – antibiotics, pain medications Additional clinic visits Additional clinic visits Re-admissions to hospitalRe-admissions to hospital Increased hospitalization - up 74 daysIncreased hospitalization - up 74 days Feeding tubes ~ 85-90%Feeding tubes ~ 85-90% Quality of life issuesQuality of life issues

Economic ImpactEconomic Impact
Non-transplantNon-transplant chemotherapy chemotherapy With grade 3 or 4 oral mucositis:With grade 3 or 4 oral mucositis:
35% require dose delays35% require dose delays 60% require dose reduction60% require dose reduction 30% have cessation of chemotherapy30% have cessation of chemotherapy
Cost: $5,565/cycleCost: $5,565/cycle

Economic ImpactEconomic Impact
High dose chemo. and transplantHigh dose chemo. and transplant With oral ulceration: With oral ulceration:
required 5.8 additional days of narcoticsrequired 5.8 additional days of narcotics required 1.9 additional days of TPNrequired 1.9 additional days of TPN
systemic infection and fatiguesystemic infection and fatigue intensive nursing care; medical and dental intensive nursing care; medical and dental
specialistsspecialists
Cost: $42,749Cost: $42,749

Stomatotoxicity 1978 - 1988Stomatotoxicity 1978 - 1988
Unpredictable incidence/severityUnpredictable incidence/severity Duration variableDuration variable Mechanism?Mechanism? Role of trauma, xerostomia, and Role of trauma, xerostomia, and
oral flora?oral flora?

Chemotherapy Stomatotoxicity 1978 - 1988Chemotherapy Stomatotoxicity 1978 - 1988
DirectDirect IndirectIndirect
BleedingBleeding
Decreased nutritionDecreased nutrition
Mucosal infectionMucosal infection
Cell renewalCell renewal
ThinningThinning
MucositisMucositisand ulcerationand ulceration
ThrombocytopeniaThrombocytopenia
NeutropeniaNeutropenia
XerostomiaXerostomia

Clinical ConsiderationsClinical Considerations
Oral Mucositis Risk FactorsOral Mucositis Risk Factors Chemotherapy dose and protocolChemotherapy dose and protocol Concomitant H&N RT or TBIConcomitant H&N RT or TBI TraumaTrauma Pre-chemotherapy oral statusPre-chemotherapy oral status Real vs. hypothetical vs. teleologicalReal vs. hypothetical vs. teleological

Trauma – Dentures

Concomitant Chemotherapy and RT

Trauma – Teeth and Restorations

Soft Tissue NecrosisSoft Tissue Necrosis
Traumatic vs. Traumatic vs. spontaneousspontaneous
Intraoral source RTIntraoral source RT Can occur lateCan occur late Prolonged durationProlonged duration

Histologic Changes from Histologic Changes from ChemotherapyChemotherapy
120 necropsies from 30 patients120 necropsies from 30 patients Death within 30 d. myelosuppresive chemo.Death within 30 d. myelosuppresive chemo. Multiple oral anatomical sitesMultiple oral anatomical sites ““Blinded” oral pathologistBlinded” oral pathologist
MethodsMethods
Lockhart P, Sonis ST. J Dermatol Surg Oncol 1981; 7(12):1019-1025

Histologic ChangesHistologic Changes
Collagen degenerationCollagen degeneration
HyperplasiaHyperplasia
ParakeratosisParakeratosis
Glandular degenerationGlandular degeneration
AtrophyAtrophy
DysplasiaDysplasia
1515
15151111
1010
77
77
(75%)(75%)
(75%)(75%)(55%)(55%)
(50%)(50%)(35%)(35%)
(35%)(35%)
(N=20)(N=20)Lockhart P, Sonis ST, J Dematol Surg, 1981

Atrophy and Collagen Degeneration

Mucosal Sloughing

Pathobiology of Oral MucositisPathobiology of Oral Mucositis
1970s – 1980s 1970s – 1980s • • Defining the problems – incidence, nature Defining the problems – incidence, nature and severityand severity• • Clinical prevention and mClinical prevention and management issuesanagement issues•• Focus on epitheliumFocus on epithelium
1990s1990s• • NIH consensus conference (1989)NIH consensus conference (1989)• • Focus on mucosal cells and mediatorsFocus on mucosal cells and mediators• • Pharmaceutical studies – clinical trialsPharmaceutical studies – clinical trials

Mucositis Study GroupMucositis Study Group
International Society for Oral Oncology (ISOO) International Society for Oral Oncology (ISOO) 19851985
Multinational Association of Supportive Care in Multinational Association of Supportive Care in Cancer (MASCC) 1995Cancer (MASCC) 1995

Mucositis Pathobiology and Practice Mucositis Pathobiology and Practice Guidelines - 2004Guidelines - 2004
© M
AS
CC
20
04
Cancer Supplement May 1, 2004

DNA damage and apoptosisDNA damage and apoptosis
Reactive oxygen species (free Reactive oxygen species (free radicals)radicals)
Mucositis, damaged cells, blood Mucositis, damaged cells, blood vesselsvessels
Mechanism – Current ThinkingMechanism – Current Thinking

HealingUlcerationSignaling andAmplification
Upregulationand
Message GenInitiation
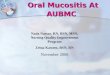
Today’s Pathobiology Perspective: Today’s Pathobiology Perspective: A Multiple Mechanism ModelA Multiple Mechanism Model
Keefe and Sonis – Cancer Supplement. 100:1995-2011, 2004.

HealingUlcerationSignaling andAmplification
Upregulationand
Message GenInitiation
Apoptosis
Tissue Injury
DNA Injury
FibronectinBreaks Up
ActivatesMacrophages MMP
IL-1
TNF-IL-6
GeneUpregulation
NF-B
Angiogenesis
Cell Membrane
Epithelium
Endothelium
ConnectiveTissue
Macrophages
SphingomyelinaseCeramidePathway
Ceramide Synthase
Expressionof AdhesionMolecules COX-2
Clonogenic Cell Death
ROS
Today’s Pathobiology Perspective: Today’s Pathobiology Perspective: A Multiple Mechanism ModelA Multiple Mechanism Model
CTCT
RTRT

Feb. 2007

Basic Oral CareBasic Oral Care
Guidelines:Guidelines:
– Dental assessment and care – pre-Dental assessment and care – pre-treatment, during treatment, follow-uptreatment, during treatment, follow-up
– ““...basic oral care including an ultra soft ...basic oral care including an ultra soft toothbrush with regular replacement of the toothbrush with regular replacement of the toothbrush”toothbrush”
– Bland rinsesBland rinses
– Promote mucosal moisturization and Promote mucosal moisturization and protectionprotection
– Check for fungal, bacterial or viral Check for fungal, bacterial or viral infectionsinfections Keefe DM, et al. Cancer, 109; 2007Keefe DM, et al. Cancer, 109; 2007

Topical AnestheticsTopical Anesthetics
No recommendationsNo recommendations (lack of well designed (lack of well designed trials)trials)
Reasonable for mild/moderate and Reasonable for mild/moderate and breakthrough pain management breakthrough pain management
Check that the patient eatsCheck that the patient eats
Keefe DM, et al. Cancer, 109; 2007Keefe DM, et al. Cancer, 109; 2007

Prevention Anti-inflammatory Prevention Anti-inflammatory AgentsAgents
Multiple small studies but results still Multiple small studies but results still conflictingconflicting
May be helpful for:May be helpful for:
Rectal and pelvic cancer RTRectal and pelvic cancer RT
AmifostineAmifostine
Keefe DM, et al. Cancer, 109; 2007Keefe DM, et al. Cancer, 109; 2007

Prevention – Alternative Prevention – Alternative TherapiesTherapies
Vitamins A, E, B12, Folate, and diet Vitamins A, E, B12, Folate, and diet supplementssupplements
Glutamine (II C)Glutamine (II C) Aloe veraAloe vera PV701 – Milk-derived protein extract PV701 – Milk-derived protein extract
No Guideline possible No Guideline possible - Conflicting and - Conflicting and insufficient evidenceinsufficient evidence
Keefe DM, et al. Cancer, 109; 2007Keefe DM, et al. Cancer, 109; 2007

Prevention - CryotherapyPrevention - Cryotherapy
RecommendedRecommended for: for: Bolus 5 FU and Leucovorin/5FU (II A)Bolus 5 FU and Leucovorin/5FU (II A)
SuggestedSuggested for: for: Etidronate (IV B)Etidronate (IV B) High dose Melphalan in HSCT (II A)High dose Melphalan in HSCT (II A)
Keefe DM, et al. Cancer, 109; 2007Keefe DM, et al. Cancer, 109; 2007 © M
AS
CC
20
04

Agents in Clinical Trials Agents in Clinical Trials
IL-11IL-11 trials stopped early for excess toxicitytrials stopped early for excess toxicity
GM-CSF and G-CSF (II,C)GM-CSF and G-CSF (II,C) still no evidence for reduced oral mucositisstill no evidence for reduced oral mucositis
KGF-1 (palifermin)KGF-1 (palifermin) Recommended for HDC and TBI with HSCTRecommended for HDC and TBI with HSCT
KGF-2 (repifermin)KGF-2 (repifermin) withdrawn by companywithdrawn by company
PreventionPrevention
Keefe DM, et al. Cancer, 109; 2007Keefe DM, et al. Cancer, 109; 2007

Antimicrobial LozengesAntimicrobial Lozenges
Polymyxin tetracycline Amphotericin B (PTA)Polymyxin tetracycline Amphotericin B (PTA) Bacitracin Clotrimazole Gentamicin (BCoG) Bacitracin Clotrimazole Gentamicin (BCoG)
H&N RT, adults, preventionH&N RT, adults, preventionResults: Equal to placeboResults: Equal to placebo
GuidelineGuideline: : Recommend Recommend againstagainst use for use for preventionprevention
Keefe DM, et al. Cancer, 109; 2007Keefe DM, et al. Cancer, 109; 2007

Guidelines: Oral MucositisGuidelines: Oral Mucositis
Pain ManagementPain Management RecommendedRecommended PCA with morphine for oral PCA with morphine for oral
mucositis pain for stem cell transplant (I A)mucositis pain for stem cell transplant (I A)
BenzydamineBenzydamine RecommendedRecommended for prevention of RT for prevention of RT
induced mucositis in patients with H&N Ca induced mucositis in patients with H&N Ca receiving moderate dose RTreceiving moderate dose RT
Note closure of North American trialNote closure of North American trialKeefe DM, et al. Cancer, 109; 2007Keefe DM, et al. Cancer, 109; 2007

MASCC/ISOO SUMMARYMASCC/ISOO SUMMARY
Mucosal alteration associated with chemo- and Mucosal alteration associated with chemo- and radiotherapy is multifactorialradiotherapy is multifactorial
Many clinical studies failed to meet current standardsMany clinical studies failed to meet current standards Guidelines demonstrate few preventive and Guidelines demonstrate few preventive and
treatment options for mucositistreatment options for mucositis Further research necessary Further research necessary
pathophysiologypathophysiology epidemiologyepidemiology therapytherapy
Keefe DM, et al. Cancer, 109; 2007Keefe DM, et al. Cancer, 109; 2007

Role of Xerostomia in MucositisRole of Xerostomia in Mucositis
Mucositis - No prevention available Xerostomia? - H&N RT data and 1 chemo.
abstract Pilocarpine stimulation of salivary glands
incidence severity duration
Lockhart PB et al Bone Marrow Transplantation35:713-720, 2005

Prospective, double-blind, randomized, Prospective, double-blind, randomized, placebo-controlled trialplacebo-controlled trial
40 stem cell transplant patients40 stem cell transplant patients 5 mg pilocarpine vs. placebo every 4 hrs 5 mg pilocarpine vs. placebo every 4 hrs
beginning day -1 (4 tabs/day)beginning day -1 (4 tabs/day) Bedside evaluations on alternate daysBedside evaluations on alternate days
MethodsMethods

No statistically significant differences No statistically significant differences in:in:
Overall incidenceOverall incidencePilocarpinePilocarpine 16/20 16/20 (80%)(80%)PlaceboPlacebo 15/1615/16 (94%)(94%)
SeveritySeverityDurationDuration
Results - MucositisResults - Mucositis
Lockhart PB et al Bone Marrow Transplantation35:713-720, 2005


No statistically significant differences in: No statistically significant differences in: Mouth drynessMouth dryness Nutritional intakeNutritional intake HygieneHygiene EatingEating SpeakingSpeaking SleepingSleeping Pain at rest or with swallowingPain at rest or with swallowing Systemic narcotic useSystemic narcotic use
ResultsResults
Lockhart PB et al Bone Marrow Transplantation35:713-720, 2005

Mucositis - Bacteremia and Mucositis - Bacteremia and SepsisSepsis
Mucosal barrier to pathogenic Mucosal barrier to pathogenic bacteria and fungibacteria and fungi
FeverFever Role in mucositis?Role in mucositis?

Alteration in the Profile of Oral Flora Alteration in the Profile of Oral Flora Following Cancer ChemotherapyFollowing Cancer Chemotherapy
Aim:Aim: Characterize oral bacterial flora before Characterize oral bacterial flora before
and after first cycle of intensive and after first cycle of intensive chemotherapychemotherapy
Culture-independent molecular Culture-independent molecular techniques. techniques.
Napenas, J et al Unpublished Napenas, J et al Unpublished datadata

Gram-negative Bacteria and Oral Gram-negative Bacteria and Oral MucositisMucositis
G (-) bacilli
Lipopolysaccharide release
Binding to epithelium
Cytokine release: TNF, IL-6, IL-1
Increased inflammatory process

Study DesignStudy Design
Prospective cohort studyProspective cohort study OutpatientsOutpatients Inclusion criteria:Inclusion criteria:
newly diagnosed breast cancernewly diagnosed breast cancer Adriamycin 50 mg/mAdriamycin 50 mg/m22

Oral Examination and Sample Oral Examination and Sample CollectionCollection
Oral bacterial sampling (buccal swab) on Oral bacterial sampling (buccal swab) on Chemotherapy – Day 0 and Day 7-14Chemotherapy – Day 0 and Day 7-14
Mucositis score (World Health Organization)Mucositis score (World Health Organization)

Culture Independent Culture Independent MethodologyMethodology
Bacterial isolate PCR of 16S rRNA
TOPO TA cloning kit
E. Coli
16S rRNA library (24-25 clones)DNA sequencing
Species identification

ResultsResults
9 female patients9 female patients 41 bacterial species41 bacterial species
9 species – pre and post-chemotherapy9 species – pre and post-chemotherapy 7 species - pre-chemotherapy only7 species - pre-chemotherapy only 25 species - post-chemotherapy only25 species - post-chemotherapy only

Pre- vs. Post ChemotherapyPre- vs. Post Chemotherapy
Increased species diversity – 6Increased species diversity – 6 Decreased species diversity – 2Decreased species diversity – 2 No changes in number of species - 1No changes in number of species - 1
Conclusion:Conclusion:
Appears to be a shift to a more complex Appears to be a shift to a more complex oral bacterial profile on the buccal mucosa oral bacterial profile on the buccal mucosa of breast cancer patients undergoing of breast cancer patients undergoing chemotherapychemotherapy

Few clinical histology studiesFew clinical histology studies Mucositis demonstrates a wide variety of Mucositis demonstrates a wide variety of
histologic changes:histologic changes: collagen degeneration, epithelial collagen degeneration, epithelial
hyperplasia, atrophyhyperplasia, atrophy variability likely due to the biologic variability likely due to the biologic
complexitycomplexity Need further understanding of genetic Need further understanding of genetic
regulationsregulations
Molecular Analysis of Mucosa with Molecular Analysis of Mucosa with Chemotherapy–Induced Oral Chemotherapy–Induced Oral
MucositisMucositis
Brennan MT et all Unpublished data

MethodsMethods
Five newly diagnosed AML patientsFive newly diagnosed AML patients
Buccal mucosa punch biopsy specimens (3 Buccal mucosa punch biopsy specimens (3 mm)mm) Immediately prior to induction chemotherapy Immediately prior to induction chemotherapy
and 2 days following and 2 days following 3 healthy controls (HC)3 healthy controls (HC)
RNA extractedRNA extracted

ResultsResults Microarray analysis completed for: Microarray analysis completed for:
AML pre-chemotherapy (n=4) AML pre-chemotherapy (n=4) AML post-chemotherapy (n=4) AML post-chemotherapy (n=4) Healthy controls (n=3)Healthy controls (n=3)
3 main pair-wise comparisons in gene 3 main pair-wise comparisons in gene expression changesexpression changes HC vs. pre-chemoHC vs. pre-chemo HC vs. post-chemoHC vs. post-chemo Pre-chemo vs. post-chemoPre-chemo vs. post-chemo

ResultsResults
26 genes found to be differentially 26 genes found to be differentially expressed* expressed*
Half of the genes appear to be differentially Half of the genes appear to be differentially expressed solely from chemotherapyexpressed solely from chemotherapy no statistical significance between HC and PreC no statistical significance between HC and PreC
group group significant shift when the PostC group is significant shift when the PostC group is
compared to both HC and PreC compared to both HC and PreC
* p<0.001, q<11.5%)

ResultsResults
Validated the following genes by real-time Validated the following genes by real-time RT-PCRRT-PCR ASSASS PolHPolH LIV-1 LIV-1 TNFRSF10A TNFRSF10A
ASS is downregulated while the other ASS is downregulated while the other genes were upregulated – all 2.5 foldgenes were upregulated – all 2.5 fold

Conclusions:Conclusions: Damage to the oral mucosa is significant Damage to the oral mucosa is significant
and reflected by the differential and reflected by the differential expression of genes involved in nitric expression of genes involved in nitric oxide metabolism, DNA repair, and wound oxide metabolism, DNA repair, and wound repairrepair
Identifiable genetic susceptibility Identifiable genetic susceptibility polymorphisms could provide polymorphisms could provide pharmacogenomics-based tailored pharmacogenomics-based tailored prevention or managementprevention or management

Laser Capture MicrodissectionLaser Capture Microdissection
Tissues are comprised of many different cell Tissues are comprised of many different cell typestypes
Each cell type expresses a different set of genesEach cell type expresses a different set of genes Genes expressed, and the level of expression of Genes expressed, and the level of expression of
each gene in a given cell type, provides insight each gene in a given cell type, provides insight into biological processes that are active in those into biological processes that are active in those cell typescell types

Laser Capture MicrodissectionLaser Capture Microdissection
•Gene expression analysis from whole biological samples can obscure changes that occur in particular tissues or cell types
•Laser Capture Microdissection allows relevant cell types to be purified from complex mixtures
Whole Tissue Targeted Cells
Remaining Cells Captured Cells

Microarray analysis of mucosal necropsy samples
Basal cells isolated by laser-assisted microdissection from eight 25-year old mucosa samples
Control group – 3 oral mucosal biopsies from healthy controls
Full genome gene expression analysis using Affymetrix GeneChip Human X3P Arrays
Verification made prior to comparison between control group (n=6) and archival group (n=8)
Lockhart PB et al Unpublished data

Results
Significant upregulation observed for: human Ribosomal Protein L11 (~15 times) iNOS homologs (~20 times)
Both involved in nitric oxide and p53-mediated epithelial inflammation

CONCLUSIONSCONCLUSIONS
Excellent RNA recovery and microarray Excellent RNA recovery and microarray data from 30-year old tissue samplesdata from 30-year old tissue samples
Results in concordance with those obtained Results in concordance with those obtained from the AML studyfrom the AML study

Mucositis AccomplishmentsMucositis Accomplishments1978 – 20081978 – 2008
Mechanism – progress made but much to be done
Prevention – disappointing
Pain control – essentially unchanged
Oral care – essentially unchanged
Pharmaceutical studies – slow progress after many
approaches
Funding – largely pharmaceutical

The FutureThe Future
RadiotherapyRadiotherapy – tissue sparing (IMRT, IGRT) – tissue sparing (IMRT, IGRT)
ChemotherapyChemotherapy – more targeted therapies – more targeted therapies
MechanismMechanism – basic science and animal data – basic science and animal data
PreventionPrevention – novel clinical studies – novel clinical studies
Pain controlPain control – billion dollar drug – billion dollar drug
MicrobiologyMicrobiology – further studies needed – further studies needed
Emergence of new challengesEmergence of new challenges – –
Bisphosphonates...Bisphosphonates...

Institute for Oral MedicineInstitute for Oral MedicineCarolinas Medical Center, Carolinas Medical Center,
Charlotte, NCCharlotte, NC
Farah Bahrani-Mougeot, Farah Bahrani-Mougeot, PhDPhD
Peter Lockhart, DDSPeter Lockhart, DDS Michael Brennan, DDSMichael Brennan, DDS Jen-Luc Mougeot, PhDJen-Luc Mougeot, PhD Philip Fox, DDS Philip Fox, DDS Louise Kent, RNLouise Kent, RN Jenene Noll, RNJenene Noll, RN