Embed Size (px)
Citation preview

1
CANCER THERAPY-INDUCED ORAL MUCOSITIS:
A REVIEW OF EPIDEMIOLOGY, PATHOPHYSIOLOGY, AND TREATMENT
Eugen Popa, Mihaela Pauna, Stefan-Ioan Stratul, Sergiu Ionita TMJ 2008, Vol. 58, No. 1 - 2

2
Contents:
• Introduction• Epidemiology• Pathophysiology• Treatment Options• Review of cross references• Merits & Demerits

3
• Oral mucositis is a frequent adverse reaction of the
radiation therapy of the head and neck cancers, as well as
of chemotherapy.
• Mucositis may confine the patient's tolerance of
antineoplastic therapy, and the nutritional status is
endangered.
• Compromised patient’s quality of life.
-Oral Mucositis ComplicatingChemotherapy and/or Radiotherapy; CA Cancer J Clin 2001;51:290-315
Term oral mucositis emerged in the late 1980s to describe the chemotherapy- and radiotherapy-induced inflammation of the oral mucosa.
Effects are so debilitating resulting in consecutive protraction or termination of antineoplastic therapy.

4
• Annually, the incidence is of approximately 400,000
cases of treatment-induced oral lesions.
• Oral complications subsequent to chemotherapy and/or
radiation therapy include mucositis, xerostomia, infection
(bacterial, fungal, or viral), particular neutropenia, dental
caries, taste alterations, and osteoradionecrosis.
• Oral mucositis represents a major nonhematologic
complication of cytoreductive chemotherapy and
radiotherapy
• Associated with morbidity, pain, odynodysphagia,
dysgeusia, followed by dehydration and malnutrition.
Complications of radiation therapy for head and neck cancers : the patients perspective. Cancer Nursing 2002:25:461-7
It is the most common cause of pain during the treatment of cancer and most distressing side effect of head and neck radiation therapy, myelosuppressive chemotherapy and stem cell transplantion.

5
• This mucosal changes can interfere with the cancer
therapy protocol
• It may require dose adjustments, Rx schedule
modifications
• The treatment is then usually discontinued in cases
of severe oral morbidity
• These interruptions in dosing regimens secondary to
oral complications can negatively affect the overall
patient prognosis.
-Oral Mucositis Complicating Chemotherapy and/or Radiotherapy; CA Cancer J Clin 2001;51:290-315
Hyperfractionation, combined radiotherapy, use of radiosensitizers cause increased severity of oral mucositis.
Oral Mucositis: understanding the pathology and management: HIPPOKRATIA 2012, 16, 3: 215-216
Chemotherapy induced stomatitis – less severe- lasts upto 3-12 daysRadiotherapy induced stomatitis- upto 3-12 weeks

6
Epidemiology
• Incidence & severity varies individually.
• Depends upon therapeutic agent.
• Berger and Kilroy estimated that about 40% of
patients which undergo chemotherapy develop
mucositis
• This risk grows with the number of
therapy cycles and previous
episodes of mucositis.

• Drugs interfering DNA synthesis (S-phase–specific
agents like fluorouracil, methotrexate, and cytarabine)
develop more significant cytototoxic effects.
• Studies by Peterson and Wilkes estimated that with
bolus and continuous infusions there is an increased
risk of mucositis, compared to prolonged or repetitive
regimens of lower doses of cytoreductive agents
Incidence:
76% - bone marrow transplantation
30-60% - radiation therapy
90% chemotherapy
7

• The severity and duration of mucositis depends on
type of radiation source, total dose, dose intensity,
amount of the irrradiated mucosa, smoking, alcohol
ingestion, and level of oral hygiene.
• In patients treated with standard 2 Gy of daily
fractionated radiotherapy programs, mucosal
erythema occurs in the first seven days.
8

9
• Mucositis (patchy or confluent) peaks after 4-5 weeks
of treatment with the same dose of radiation.
• In less than 2 Gy, the severity of mucositis might be
low.
• In spite of this, in accelerated radiotherapy programs,
mucositis increase in gravity at 21 days.
• Interstitial radioactive implants - in 7-10 days and
peaks after 14 days.
Risk Factors:
Patient Related:
• Age
• Gender- Women
• Smoking, excessive alcohol – as they alter epithelial
mucosal environment (Raber-Durlacher, 1999)
Treatment Related:
• Radiotherapy- Head & Neck and total body irradiation
during bone marrow transplantation
• Chemotherapeutic agents:
Anti-metabolites like etoposide, 5 FU, and methotrexate.
Bleomycin, cisplatin, cyclophosphamide, cytarabine,
dactinomycin, daunorubicin, docetaxel, doxorubicin,
mitomycin, paclitaxel, vinblastine, vincristine, and
vinorelbine (Wilkes & Ades, 2004).

Pathophysiology
• Exact pathophysiology – not elucidated• Two proposed mechanisms – Direct mucositis– Indirect mucositis
• Direct mucositis is related with chemotherapy and radiation therapy interference with the maturity and cellular growth of epithelial cells, who present a rapid turnover, every 7-14 days.
10

• These cells are susceptible to the effects of cytotoxic therapy and finally appear changes to normal turnover and cell death.
• Indirect invasion of Gram-negative bacteria and fungal species can cause the indirect mucositis.
• • The neutropenic patients have an increased risk
The onset of indirect mucositis varies, and is related with the timing of the polymorphonuclear granular leukocytes nadir, associated with the cytoreductive agent administered develops from 10-21 days after the onset of the chemotherapy regimen.
11

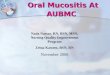
• Mechanism is explained in four stages.
• Phase 1: Initial inflammatory/vascular phase Radiation exposed cells death cytokines TNF-alpha
• Inflammatory mediators increasing vascular
permeability enhancing cytotoxic drug uptake into the oral mucosa damage to tissue
12
TNF-alpha has the ability to cause necrosis by interfering with blood flow, cytotoxic inflammation, andregulation of immune responses .(Rieger, 2001).

Phase 2: Epithelial phase
• Antineoplastic therapy inhibits cell division in
the oral mucosal epithelium reduced epithelial
turnover and renewal epithelial breakdown.
• The erythema appears from increased vascularity
and epithelial atrophy 4-5 days after the beginning of
chemotherapy.
• At this stage, any microtrauma leads to ulceration of
the oral mucosa.13

Phase III: ulcerative / bacteriological phase
• Breakdown of the oral epithelium an
ulcerative stage epithelial loss and furious
exudation formation of pseudomembranes
and ulcers microbial colonization
• Exacerbated by concomitant neutropenia.
14

• Infectious complications arising in neutropenic bone marrow transplantation recipients are due to aggressive myelo-suppressive antineoplastic drug therapy.
• The ulcerative mucositis is an important etiologic factor in the development of systemic streptococcal infections in the neutropenic cancer patients
15

Phase IV: Healing phase.
• Duration- 12-16 days
• Depends on epithelial proliferation rate,
hematopoietic recovery, reestablishment of the local
microbial flora, and absence of factors interfering
with the wound healing
16
Current trends in managing oral mucositis: Clinical journal of oncology nursing, volume 9, number 5 •
Current trends in managing oral mucositis: Clinical journal of oncology nursing, volume 9, number 5 •

Treatment options available:Prophylactic measures:• Good oral hygiene & prevention, identification and
early treatment of oral lesions• Avoidance of wearing removable dentures,
orthodontic Rx and applying chlorine releasing products like chlorhexidine gluconate (0.12% and 0.2%), carbonated water, hydrogen peroxide etc.,
• Soft foods, low carbohydrate diet, high fluid intake- recommended.
• Avoid toothpaste above grade 1 mucositis
17

Therapeutic attitude – WHO staging- 1979• 0 = normality• I = generalized erythema (painless pink mucosa
with abundant saliva and normal voice function)• II = erythema involving small ulcerations and
preserved solid swallowing capacity• III = extensive ulcers with edematous gingival
tissue and thick saliva, preserved liquid swallowing capacity, pain and speech difficulties
• IV = very extensive ulcers with bleeding gums, infections, the absence of saliva, incapacity to swallow, and intense pain. 18

Rx indications:
• Grades 0 and I: Hygiene measures:
(a) correct tooth brushing (b) chlorhexidine
digluconate mouth rinsing (c) fluid intake to
maintain salivation (d) preservation of lip integrity
• Grade II: grade 0 & 1 measures every 4 hours +
carbonated water and nystatin solution (5 ml every 6
hours) as rinses. Dentures to be worn only during
mealtimes19

Grade III & IV:• Grade II measures + topical and systemic treatments
based on etiology of the lesions• For Fungal infections - nystatin solution (5 ml/ 4 hrs)
and fluconazole in solution (200 mg/day via the oral route)
• For local herpetic infections -aciclovir cream (5 applications a day).
• For oral ulcerations - 0.1% fluocinolone acetonide in orabase, 0.1% triamcinolone acetonide in orabase, 1% hydrocortisone in orabase.
20

Patient education:
• Sit upright, eat soft food, in small proportions and chew completely.
• Avoid acid foods, hot and crunchy foods. • Measures to keep mouth moist
21

Conclusion
• Oral mucositis is a serious and challenging complication of cytoreductive therapy in cancer patients.
• As treatment is limited- prophylaxis is stressed• Patient’s psychological condition has to be assesed • Although mucositis is rarely life-threatening, it will
interfere, to a great extent, with the outcome of the cancer treatment.
22

23
Review of Cross References
Magic Mouthwash: Mixture of lidocaine, diphenhydramine
and magnesium or aluminium hydroxide.
Amifostine
• A radioprotective compound & antioxidant.
• Indicated in prevention of radiotherapy induced
xerostomia
• No effect on incidence of mucositis but reduced severity.
• Dose: 200 mg/m2. Limitation - Nausea
Prophylactic use of amifostine to prevent :Int J Radiat Oncol Biol Phys. 2002; 52

Biologic Response Modulators:
• Recombinant Human Keratinocyte Growth Factor 1
(Palifermin) – reduced severity and duration of
mucositis
• Palifermin or placebo was administered for 3 days
before and 3 days after transplant.
• The results showed that the incidence of grades 3
and 4 oral mucositis, were 63% with palifermin
versus 98% with placebo. 24
Spielberger et al., 2004.

A randomized clinical trial of two different durations of oral cryotherapy for prevention of 5-fluorouracil- related stomatitis. Cancer 1993;72:2234- 2238.
Cryotherapy:• Application of ice chips prior to administration of
bolus vasoconstriction decreased uptake of drug by mucous membrane.
• Proven useful in 5-FU, which has short plasma half-life
• Also useful in melphalan and edatrexate-based chemotherapy regimens.
25

(Cancer J Clin 2001;51:290-315)
Capsaicin:
• Capsaicin, a potent inhibitor of neuropathic pain demonstrated
a marked reduction of oral pain in patients experiencing oral
mucositis.
Vitamin E:
• Tocopherol’s antioxidant and membrane stabilizing potency
interferes with inflammatory damage caused by reactive
oxygen species and free radicals.
Vitamin A:
• Inhibitory effects upon inflammation and epithelial proliferation26

27
Non-Pharmacological Methods:• Radiation Shields:
Fabrication of protective radiation stents and midline mucosa-sparing blocks
• Laser:Low energy He-Ne lasers (soft lasers) hastens oral re-epithelialization by producing photochemical reactions in cells. Studies showed that they decreased duration and pain
Current trends in managing oral mucositis: clinical journal of oncology nursing: Vol 9: 2005

Merits:• Grading of mucositis • Grading of treatment
indications given• Good focus on
prophylactic measures
28
Demerits:• Treatment options
are not enumerated

29