Embed Size (px)
DESCRIPTION
Citation preview

Thyroid Ophthalmopathy
Thyroid Ophthalmopathy
Ellen DavisApril 27, 2007
Ellen DavisApril 27, 2007

Thyroid OphthalmopathyThyroid Ophthalmopathy
Inflammatory disorder of the eye
Commonly complicates Graves’ disease but can also be associated with Hashimoto’s thyroiditis, or in euthyroid pts
50% of pts with Graves’ have clinical ophthalmopathy, but up to 70% of the remaining half have ophthalmopathy by imaging
Inflammatory disorder of the eye
Commonly complicates Graves’ disease but can also be associated with Hashimoto’s thyroiditis, or in euthyroid pts
50% of pts with Graves’ have clinical ophthalmopathy, but up to 70% of the remaining half have ophthalmopathy by imaging

EpidemiologyEpidemiology Prevalence of thyroid ophthalmopathy = 0.4% Women > Men
But severity greater in men Mean age of appearance = 41 yrs May of exacerbated by stress, smoking, and infection
with certain gram-negs Most common cause of exophthalmos
>50% of cases Of note, other causes of exophthalmos include primary
hyperadrenalism, longstanding steroid use or acromegaly.
Prevalence of thyroid ophthalmopathy = 0.4% Women > Men
But severity greater in men Mean age of appearance = 41 yrs May of exacerbated by stress, smoking, and infection
with certain gram-negs Most common cause of exophthalmos
>50% of cases Of note, other causes of exophthalmos include primary
hyperadrenalism, longstanding steroid use or acromegaly.

PathogenesisPathogenesis Autoimmune process manifesting as:
Extraocular m. myositis T-cell inflammatory infiltrate
Fibroblast proliferation Glycosaminoglycan overproduction Orbital congestion
Increase in soft tissue mass within bony orbit due to extraocular muscle enlargement, increased orbital fat and connective tissue
Later in disease, inflammatory infiltrate replaced by widespread fibrosis “Inactive” phase Occurs about 8mo to 3yrs after onset
Autoimmune process manifesting as: Extraocular m. myositis
T-cell inflammatory infiltrate Fibroblast proliferation Glycosaminoglycan overproduction Orbital congestion
Increase in soft tissue mass within bony orbit due to extraocular muscle enlargement, increased orbital fat and connective tissue
Later in disease, inflammatory infiltrate replaced by widespread fibrosis “Inactive” phase Occurs about 8mo to 3yrs after onset

PathogenesisPathogenesis
Inflammatory cells activated by TSH receptor antigen TSH receptor mRNA and protein found in
orbital fibroblasts and adipocytes TSHR expression greater in retro-orbital
tissues of Graves’ pt compared to other tissues.
Correlation between severity of ophthalmopathy and serum TSHR Ab concentrations
Inflammatory cells activated by TSH receptor antigen TSH receptor mRNA and protein found in
orbital fibroblasts and adipocytes TSHR expression greater in retro-orbital
tissues of Graves’ pt compared to other tissues.
Correlation between severity of ophthalmopathy and serum TSHR Ab concentrations

Initial Signs/SymptomsInitial Signs/Symptoms
Foreign body sensation Epiphora (tearing) Photophobia Lid retraction (normally, should not see
sclera above iris) Lid lag Lid, conjunctival and periorbital edema Injection over horizontal muscle
insertions
Foreign body sensation Epiphora (tearing) Photophobia Lid retraction (normally, should not see
sclera above iris) Lid lag Lid, conjunctival and periorbital edema Injection over horizontal muscle
insertions

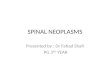
ExophthalmosExophthalmos Usually bilateral and symmetric Pathological changes displace eye
forward and can interfere with muscle actions and venous drainage.
Usually bilateral and symmetric Pathological changes displace eye
forward and can interfere with muscle actions and venous drainage.
Note enlarged extraocular mm.

HistologyHistology
Fluid and inflammatory cells separate the muscle bundles of the extraocular muscles.
Fluid and inflammatory cells separate the muscle bundles of the extraocular muscles.

ComplicationsComplications
Limitation of ocular motility --> diplopia Inferior rectus > medial r. > superior r.
Exposure keratopathy --> dry eye, tearing, corneal ulceration or infection
Limitation of ocular motility --> diplopia Inferior rectus > medial r. > superior r.
Exposure keratopathy --> dry eye, tearing, corneal ulceration or infection

ComplicationsComplications
Optic nerve compression at orbital apex by enlarged muscles May present with blurry vision, color
loss, afferent pupillary defect, or visual field loss
More likely when superior rectus is enlarged or if no exophthalmos (form of self-decompression)
Optic nerve compression at orbital apex by enlarged muscles May present with blurry vision, color
loss, afferent pupillary defect, or visual field loss
More likely when superior rectus is enlarged or if no exophthalmos (form of self-decompression)

Optic neuropathyOptic neuropathy
Optic neuropathy as result of optic nerve compression from enlargement of extraocular muscles
Optic neuropathy as result of optic nerve compression from enlargement of extraocular muscles

DDx of Thyroid OphthalmopathyDDx of Thyroid
Ophthalmopathy Orbital tumors (primary or
metastatic) Orbital pseudotumor Wegener’s granulomatosis Orbital infection Carotid-cavernous sinus fistula
Orbital tumors (primary or metastatic)
Orbital pseudotumor Wegener’s granulomatosis Orbital infection Carotid-cavernous sinus fistula

Radiologic EvaluationRadiologic Evaluation
Usually employed if cause of exophthalmos is unclear (ie. normal thyroid lab studies, or hx/PE inconsistent with thyroid disease)
Also to determine optic nerve involvement if not obvious by fundoscopic exam
Distinct sparing of muscle tendons in thyroid ophthalmopathy
Usually employed if cause of exophthalmos is unclear (ie. normal thyroid lab studies, or hx/PE inconsistent with thyroid disease)
Also to determine optic nerve involvement if not obvious by fundoscopic exam
Distinct sparing of muscle tendons in thyroid ophthalmopathy

Radiologic EvaluationRadiologic Evaluation Non-contrast enhanced coronal orbital CT scan
most helpful to assess size of extraocular mm. Non-contrast enhanced coronal orbital CT scan
most helpful to assess size of extraocular mm.
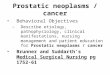
A. Symmetric bilateral exophthalmos and hypertrophy of fat. Axial muscles are mildly involved.
B. Enlargement of levator palpebrae superioris and superior rectus complex.

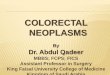
Axial CT of orbits demonstrating medial rectus enlargement
Axial CT of orbits demonstrating medial rectus enlargement

Medial and lateral rectus muscle enlargement with orbital apex crowding, leading to optic neuropathy
Medial and lateral rectus muscle enlargement with orbital apex crowding, leading to optic neuropathy

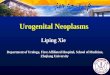
Axial, coronal and oblique sagittal T1-weighted orbital sections:Hypertrophy of retrobulbar fat and enlargement of all four rectus muscles. Belly of inferior rectus m. moderately hyperintense due to fatty infiltration.
Axial, coronal and oblique sagittal T1-weighted orbital sections:Hypertrophy of retrobulbar fat and enlargement of all four rectus muscles. Belly of inferior rectus m. moderately hyperintense due to fatty infiltration.

TreatmentTreatment Symptomatic treatment:
Artificial tears Eye shades Raise head of bed at night
Diplopia can be managed with prism glasses Eventually may require strabismus surgery, most often
with recession of inferior rectus to compensate for restriction.
Conserve useful vision Minimize amount of exposed cornea
May require lid surgery Treat optic neuropathy
Symptomatic treatment: Artificial tears Eye shades Raise head of bed at night
Diplopia can be managed with prism glasses Eventually may require strabismus surgery, most often
with recession of inferior rectus to compensate for restriction.
Conserve useful vision Minimize amount of exposed cornea
May require lid surgery Treat optic neuropathy

Antithyroid TreatmentAntithyroid Treatment
Randomized trial of 443 Graves’ pts with slight or no ophthalmopathy Radioiodine alone (150 pts)
15% developed or had worsening ophthalmopathy
Radioiodine + prednisone (135 pts) None developed or had worsening of eye disease
Radioiodine + Methimazole (148 pts) 2% of pts with ophthalmopathy improved 3% worsened Remaining had no change
Randomized trial of 443 Graves’ pts with slight or no ophthalmopathy Radioiodine alone (150 pts)
15% developed or had worsening ophthalmopathy
Radioiodine + prednisone (135 pts) None developed or had worsening of eye disease
Radioiodine + Methimazole (148 pts) 2% of pts with ophthalmopathy improved 3% worsened Remaining had no change

Antithyroid TreatmentAntithyroid Treatment
Radioiodine therapy can increase risk of development or worsening of Graves’ ophthalmopathy Worsening may be prevented by
steroids No change with concurrent
methimazole
Radioiodine therapy can increase risk of development or worsening of Graves’ ophthalmopathy Worsening may be prevented by
steroids No change with concurrent
methimazole

Radioiodine TherapyRadioiodine Therapy
Probably best to avoid radioiodine in pts with moderate/severe ophthalmopathy, or delay until ophthalmopathy stable
Use in caution in pts with other risk factors for ophthalmopathy
Probably best to avoid radioiodine in pts with moderate/severe ophthalmopathy, or delay until ophthalmopathy stable
Use in caution in pts with other risk factors for ophthalmopathy

ThyroidectomyThyroidectomy
Near total thyroidectomy may be associated with less progression of proptosis compared to subtotal surgery
Radioiodine therapy after near total thyroidectomy --> less active ophthalmopathy compared to pts with thyroidectomy alone.
Near total thyroidectomy may be associated with less progression of proptosis compared to subtotal surgery
Radioiodine therapy after near total thyroidectomy --> less active ophthalmopathy compared to pts with thyroidectomy alone.

Treatment: Immunosuppression
Treatment: Immunosuppression
Steroids controversial Immediate benefit decays with time Usually reserved for pts with optic
neuropathy
Azathioprine or cyclophosphamide May have role in combo with steroids,
but are less beneficial alone Cyclosporine esp when steroids are
tapered or stopped.
Steroids controversial Immediate benefit decays with time Usually reserved for pts with optic
neuropathy
Azathioprine or cyclophosphamide May have role in combo with steroids,
but are less beneficial alone Cyclosporine esp when steroids are
tapered or stopped.

Orbital RadiationOrbital Radiation
Kills retroorbital inflammatory cells Effectivity controversial
May have role in pts who cannot tolerate steroids
May be more effective if combined with steroids
One randomized trial showed improved eye motility and diplopia, but no prevention of worsening of ophthalmopathy.
Kills retroorbital inflammatory cells Effectivity controversial
May have role in pts who cannot tolerate steroids
May be more effective if combined with steroids
One randomized trial showed improved eye motility and diplopia, but no prevention of worsening of ophthalmopathy.

Orbital Decompression Surgery
Orbital Decompression Surgery
Restore normal orbital anatomy Indications:
Progression despite steroids or radiation
Vision threatened by corneal or optic nerve compromise
Severe proptosis --> cosmetic improvement
Restore normal orbital anatomy Indications:
Progression despite steroids or radiation
Vision threatened by corneal or optic nerve compromise
Severe proptosis --> cosmetic improvement

Orbital DecompressionOrbital Decompression
Transantral decompression Involves removal of floor and medial
wall of orbit No facial scarring, no craniotomy
Usually improvement in proptosis and edema
May not improve diplopia Strabismus surgery usually needed
Transantral decompression Involves removal of floor and medial
wall of orbit No facial scarring, no craniotomy
Usually improvement in proptosis and edema
May not improve diplopia Strabismus surgery usually needed

CT guided orbital decompression shows inferomedial periorbita incision with extensive fat decompression into sinus cavity
CT guided orbital decompression shows inferomedial periorbita incision with extensive fat decompression into sinus cavity

Transantral decompression. Transantral decompression.

The EndThe End

ReferencesReferences Yanoff: Ophthalmology, 2nd ed., Copyright 2004 Mosby, Inc. Chapter 201: Ocular
myopathies. UptoDate: Graves’ orbitopathy: Diagnosis and Treatment. Grainger & Allison's Diagnostic Radiology: A Textbook of Medical Imaging, 4th
ed., Copyright 2001. Chapter 106: Inflammatory disease of the orbit. Relation between therapy for hyperthyroidism and the course of Graves' ophthalmopathy.
Bartalena L; Marcocci C; et al. NEJM 1998 Jan 8;338(2):73-8. Total thyroidectomy for the treatment of hyperthyroidism in patients with ophthalmopathy.
Kurihara H. Thyroid 2002 Mar;12(3):265-7.
El-Kaissi S. Frauman AG. Wall JR. Thyroid-associated ophthalmopathy: a practical guide to classification, natural history and management. Internal Medicine Journal. 34(8):482-91,
2004 Aug. Selected images from:
Cummings: Otolaryngology: Head & Neck Surgery, 4th ed., Copyright ゥ 2005 Mosby, Inc.
Kumar: Robbins and Cotran: Pathologic Basis of Disease, 7th ed., Copyright ゥ 2005
Yanoff: Ophthalmology, 2nd ed., Copyright 2004 Mosby, Inc. Chapter 201: Ocular myopathies.
UptoDate: Graves’ orbitopathy: Diagnosis and Treatment. Grainger & Allison's Diagnostic Radiology: A Textbook of Medical Imaging, 4th
ed., Copyright 2001. Chapter 106: Inflammatory disease of the orbit. Relation between therapy for hyperthyroidism and the course of Graves' ophthalmopathy.
Bartalena L; Marcocci C; et al. NEJM 1998 Jan 8;338(2):73-8. Total thyroidectomy for the treatment of hyperthyroidism in patients with ophthalmopathy.
Kurihara H. Thyroid 2002 Mar;12(3):265-7.
El-Kaissi S. Frauman AG. Wall JR. Thyroid-associated ophthalmopathy: a practical guide to classification, natural history and management. Internal Medicine Journal. 34(8):482-91,
2004 Aug. Selected images from:
Cummings: Otolaryngology: Head & Neck Surgery, 4th ed., Copyright ゥ 2005 Mosby, Inc.
Kumar: Robbins and Cotran: Pathologic Basis of Disease, 7th ed., Copyright ゥ 2005