Embed Size (px)
Citation preview

PARALYTIC STRABISMUS
K.RAJESWARIM.OPTOM – 1ST YEAR151141002

May 1, 2023PARALYTIC STRABISMUS
2
INTRODUCTION•There are 6 extra ocular muscles – 4 rectus muscles, 2 oblique musclesSuperior
RectiInferior Recti
Medial Recti
Lateral recti
Inferior oblique
Superior Oblique

May 1, 2023PARALYTIC STRABISMUS
3
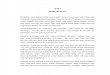
ORIGIN AND
INSERATION

May 1, 2023PARALYTIC STRABISMUS
4
May 1, 2023
4
MR
LR
IR
SR
ANNULUS OF ZINN
SCLERA @ 5 . 5mm
OCCULOMOTOR
ANNULUS OF ZINN
SCLERA @ 6 . 9mm
TROCLEAR
ANNULUS OF ZINN
SCLERA @ 6 . 5mm
OCCULOMOTOR
ANNULUS OF ZINN
SCLERA @ 7 . 7mm
OCCULOMOTOR

May 1, 2023PARALYTIC STRABISMUS
5
May 1, 2023
5
SO
IO
LPS
SPHENOID BONE
POSTIOSUPERIOR
QUADRENTABDUSENT
ORBITAL FLOOR
POSTIOINFERIOR
QUADRENTOCCULOMO
TOR
SPHENOID BONE
SUPRA TARSAL PLATE
OCCULOMOTOR

May 1, 2023PARALYTIC STRABISMUS
6MUSCLE
PRIMARY ACTION
SECONDARY ACTION
TERTIARY ACTION
MEDIAL RECTUS Adduction -- --
SUPERIOR RECTUS Elevation Intortion Adduction
INFERIOR RECTUS Depression Extortion Adduction
INFERIOR OBLIQUE Extorsion Elevation Abduction
SUPERIOR OBLIQUE Intorsion Depression Abduction
LATERAL RECTUS Abduction ---- ----

May 1, 2023PARALYTIC STRABISMUS
7TERMS Agoni
st Prime mover
Antagonist
Muscle Having The Opposed Action
Synergist
Muscle Having The Same Actions c
ontr
acti
on &
R
elax
atio
n

May 1, 2023PARALYTIC STRABISMUS
8
Ipsilateral
On The Same Side
Contralateral
On The Opposite
Side7
Contracture
Increased Resistance
Against Passive Stretching Of
The Muscle, Loss Of Elasticity

May 1, 2023PARALYTIC STRABISMUS
9
Muscle Ipselateral Antagonist
Contralateral synergist
Contralateral antagonist
RMR RLR LLR LMR RLR RMR LMR LLR RSR RIR LIO LSO RIR RSR LSO LIO RIO RSO LSR LIR RSO RIO LIR LSR
Contralateral antagonist
Contralateral Synergist
Ipselateral antagonist Muscle
For right eye read from the top
For left eye read from the bottom

May 1, 2023PARALYTIC STRABISMUS
10
An equal and simultaneous innervation flows from the brain to a pair of muscles of both eyes (yoke muscles) which contract simultaneously in different binocular movements
E.g. Equal and simultaneous innervation flows to:
1. RLR and LMR muscles during dextroversion
2. RSR and LIO muscles during dextroelevation
Hering’s Law of Equal
Innervation

May 1, 2023PARALYTIC STRABISMUS
11
Whenever an agonist receives an impulse to contract, an equivalent inhibitory impulse is sent to its antagonist, which relaxes
e.g. during dextroversion , an increased innervational flow to the RLR and LMR is accompanied by decreased flow to the RMR and LLR muscle.
Sheringtons Law of Reciprocal Innervation

May 1, 2023PARALYTIC STRABISMUS
12Under action of the primary muscle
Over action of the contralateral synergist
Over action of the ipsilateral antagonist
Under action of the contralateral antagonist
Overaction of the ipsilateral synergist??
Sequelae
Ocular Muscle Palsy

May 1, 2023PARALYTIC STRABISMUS
13
PARALYTIC STRABISMUS

May 1, 2023PARALYTIC STRABISMUS
14
Due to motor deficiency of one or a group of extra ocular muscles
Incomplete
paralysis
paresis
Complete deficiency paralysis
Palsy

May 1, 2023PARALYTIC STRABISMUS
15
SIGNS• Eyes that do not align in the same direction•Uncoordinated eye movements (eyes do not move together)• Reduced of vision• Reduced depth perception• Compensatory HP

May 1, 2023PARALYTIC STRABISMUS
16
SYMPTOMS:1.Limitation of ocular
movements2.Sudden onset ocular
deviation3.Diplopia4.Confusion5.Nausea , vertigo

May 1, 2023PARALYTIC STRABISMUS
17
CLASSIFICATION
NEUROGENIC
JUNCTION
MYOGENIC

May 1, 2023PARALYTIC STRABISMUS
18
NEUROGENIC • Localisation
• Supra nuclear • Nuclear • Internuclear • Infra nuclear
Nerves
• Oculomotor nerve (III CN)• Trochlear nerve (IV
CN)• Abducens nerve (VI
CN)

May 1, 2023PARALYTIC STRABISMUS
19
•Etiology: •Congenital hypoplasia or absence of nucleus: third and sixth cranial nerve palsies.•Inflammatory lesions: encephalitis, meningitis, Neuro syphilis, peripheral neuritis (viral),infectious lesions of cavernous sinus and orbit.•Neoplastic lesions – brain tumors

May 1, 2023PARALYTIC STRABISMUS
20
•Vascular lesions: HTN, DM and atherosclerosis. Haemorrhage, thrombosis, embolism, aneurysms or vascular occlusions•Traumatic lesions: head injury•Toxic lesions: CO poisoning, -OH neuropathy.•Demyelinating lesions: multiple sclerosis

May 1, 2023PARALYTIC STRABISMUS
21
THIRD NERVE PALSY

May 1, 2023PARALYTIC STRABISMUS
22
•The III nerve divides into two branches.• The superior branch supplies the LPS and SR•The inferior branch supplies the MR, IR and IO muscles.
•A complete lesion deficit of elevation, adduction and depression.

May 1, 2023PARALYTIC STRABISMUS
23
LOCALIZATION OF LESION
Nuclear:•Bilateral ptosis
Internuclear • Ophthalmoplegia
Infranuclear• partial or complete
impairment of pupillary reactions

May 1, 2023PARALYTIC STRABISMUS
24AETIOLOGYPupil-sparing causes tend to relate to
ischaemic microvascular disease (and rarely, cavernous sinus syndrome).
Pupil-involving disease usually arises as a result of an aneurysm but can also occur as a result of• tumour, • trauma, • pituitary apoplexy, • herpes zoster and • leukaemia.
Children may exhibit third nerve palsy as part of an ophthalmoplegic migraine.

May 1, 2023PARALYTIC STRABISMUS
25
INVESTIGATIONS1. VISUAL ACUITY:
a) It is necessary to lift the ptotic lid to evaluate visual acuity.
b) May be reduced due to mydriasis, particularly for near visual acuity
2. COVER TESTa) An exo- and hypo-deviation is present
3. OCULAR MOTILITYa) be limited elevation, depression and
adduction,b) complete or partial limitations

May 1, 2023PARALYTIC STRABISMUS
26
4. Hess chart a. The affected eye will show a markedly constricted fieldb. The other eye demonstrates overaction of its muscles
5. Diplopiaa) There will be constant diplopia unless complete ptosis
is present and blocks the vision of the affected eye6. Convergence
a) This will be absent if the medial rectus muscle is paralysed
7. Binocular functiona) This is usually absent unless the III nerve paresis is
mild and partial8. Accommodation
a) Due pupillary dilatation, the accommodation will be defective

May 1, 2023PARALYTIC STRABISMUS
27
ABERRANT REGENERATION
•Change in the regrowth of damaged nerve fibres following complete or severe third nerve palsy• It is liable to occur when either trauma or an aneurysm has caused the lesion•May occur from weeks to months after the onset of the III nerve paresis

May 1, 2023PARALYTIC STRABISMUS
28
CYCLIC OCULOMOTOR PALSY
•This rare condition is usually congenital and unilateral in origin • It is often associated with some degree of ptosis.•Acquired cyclic ocular motor palsy may occur following irradiation of the skull base and is similar to ocular neuro-myotonia

May 1, 2023PARALYTIC STRABISMUS
29
Contd…•The condition is described as having cyclical fluctuation in two phases:Paralytic phase: There is a partial III nerve palsy.
Miotic phase: There is convergence, lid retraction, accommodation and pupil constriction

May 1, 2023PARALYTIC STRABISMUS
30
FOURTH NERVEPALSY

May 1, 2023PARALYTIC STRABISMUS
31
•The IV cranial nerve supplies the superior oblique muscle only.• Any lesion affecting the nerve may result in difficulties of •depression, • incyclorotation and •abduction of the eye

May 1, 2023PARALYTIC STRABISMUS
32
LOCATION OF LESION
•Fourth nerve palsy may be due to lesions in the nucleus or fascicular lesions of the midbrain.• It can be difficult to differentially diagnose nuclear and fascicular lesions as the IV nerves crosses immediately after exiting the nuclei and exit the•dorsal midbrain after a very short intra-midbrain course.

May 1, 2023PARALYTIC STRABISMUS
33
PRESENTATION:
•Binocular vertical diplopia, •difficulty in reading and •the sense that ------- things appear to be tilted.

May 1, 2023PARALYTIC STRABISMUS
34
•There is often facial asymmetry consisting of shallowing of the midfacial region between the lateral canthus and the edge of the mouth

May 1, 2023PARALYTIC STRABISMUS
35
ETIOLOGY•Trauma,•Vasculopathy (often related to diabetes and hypertension) and •Demyelinating disease. •This may also be congenital or • idiopathic

May 1, 2023PARALYTIC STRABISMUS
36
INVESTIGATIONS1.COVER TEST
The test is performed with and without the abnormal head posture for comparison.
A latent deviation exists if a compensatory abnormal head posture is adopted.
2.OCULAR MOTILITY (sequelae)The primary under action of the affected superior oblique muscle.

May 1, 2023PARALYTIC STRABISMUS
37
3. CONVERGENCE :• This may be reduced, either due to
convergence insufficiency or the vertical deviation
4. DIPLOPIA• greater degree of diplopia on near
testing when looking down• usually uncrossed
5. Torsion Diagnostic prisms• Excyclotorsion is frequently present.• Fresnel prisms may be used temporarily
to correct the angle of deviation.• If the prism releves abnormal head
posture, then the indication is that the IV nerve was responsible for the abnormal head posture rather than a non-ocular cause.

May 1, 2023PARALYTIC STRABISMUS
38
SIXTH NERVE PALSY

May 1, 2023PARALYTIC STRABISMUS
39
•The VI cranial nerve supplies the lateral rectus muscle only. •A lesion affecting the nerve will result in defective abduction of the eye•Presentation:Horizontal diplopia (D>N)

May 1, 2023PARALYTIC STRABISMUS
40
AETIOLOGY• Trauma, • Vascular insults and • inflammation.• Palsy secondary to raised intracranial pressure is regarded as a typical false localising sign. •Other causes have included post-operative complications, viral infection, multiple sclerosis and otitis

May 1, 2023PARALYTIC STRABISMUS
41
CONTD…•Congenital• Following birth trauma• Hereditary• Infection (maternal)• Failure of lateral rectus development
•Young adults:• Trauma• Space-occupying lesions• Post-viral inflammatio•Multiple sclerosis• High myopia• – Ophthalmoplegic migraine

May 1, 2023
42
INVESTIGATION1. VISUAL ACUITY • This may be reduced if the affected eye fails to fixate due to the presence of deviation.
2. ABNORMAL HEAD POSTURE• The face is turned towards the affected side
3. Cover test • An eso-deviation is present (D>N)•with and without an abnormal head posture.

May 1, 2023PARALYTIC STRABISMUS
43
4.Ocular motility•The primary underaction of the lateral rectus results.
5.Binocular function•This is often retained in the presence of an abnormal head posture

May 1, 2023PARALYTIC STRABISMUS
44
MYOGENIC • ETIOLOGY:• Congenital - Absence ,hypoplasia mal insertion or muscular facial anomalies• Traumatic laceration, disinertion• Inflammatory - Myositis (viral) , influenza, measles.•Myopathies: These include thyroid myopathy, carcinomatous myopathy, Progressive external Opthalmoplegia

SINGLE MUSCLE PALSY1. Medial rectus• This produces an exo-deviation, which is greater for near fixation.
2. Inferior rectus: • This produces hyper- and exo-deviation
3. Superior rectus: • This is often bilateral and may present with a V exo pattern.
4. Inferior oblique:• This is a feature of an A eso pattern 01/05/2023
45

DIFFERENTIAL DIAGNOSIS OF SINGLE MUSCLE PALSIES•MR palsy
Atypical Duane’s retraction syndromeUni/bilateral inter nuclear ophthalmoplegia
• IR palsyMyogenic (myasthenia gravis)Mechanical limitation (thyroid eye disease)
Trauma (blowout fracture)01/05/2023
46

May 1, 2023PARALYTIC STRABISMUS
47
•IO palsyBrown’s syndrome
•SR palsy Trauma (blowout fracture)Mechanical limitation (thyroid eye disease

DOUBLE ELEVATOR PALSY
•This often has a congenital origin and is presumed to be caused by a supra nuclear defect. •The superior rectus and inferior oblique muscles of the same eye are affected.•Bell’s phenomenon is usually present.
01/05/2023
48

DIFFERENTIAL DIAGNOSIS DOUBLE ELEVATOR PALSY
•The following conditions should be differentiated from double elevator palsy as they will have a positive forced duction test:• Blowout fracture• Thyroid eye disease• Brown’s syndrome• Congenital fibrosis of the inferior rectus muscle• General fibrosis syndrome
49

May 1, 2023PARALYTIC STRABISMUS
50
MULTIPLE NERVE PALSIES
Presentation: oThere may be a combination of unilateral III, IV and VI cranial nerves oFacial pain corresponding to one or more branches of the fifth cranial nerve, oPtosis and small pupil (Horner's syndrome) or a dilated pupil if the third cranial nerve is affected.

May 1, 2023PARALYTIC STRABISMUS
51
ETIOLOGY:• Tumours within the cavernous sinus (primary or
metastatic).• Intracavernous aneurysm.• Mucormycosis (particularly in those patients with
uncontrolled diabetes and in immuno compromised patients).• Pituitary apoplexy.• Herpes zoster.• Cavernous sinus thrombosis.• Tolosa-Hunt syndrome.• Rare causes: sarcoidosis, Wegener's granulomatosis,
tuberculosi

May 1, 2023PARALYTIC STRABISMUS
52
OTHER IMPORTANT
TESTS…

May 1, 2023PARALYTIC STRABISMUS
53
FORCED DUCTION TEST
To differentiate the palsy and restrictions due to mechanical factors• Anesthesia• Supine position• Speculum to hold the lids• Forceps without teeth kept in the right
angle to the deviation• Grab the globe• Passive rotation of the globe
FDT +VE – Mechanical restrictions (resistance)
FDT –VE – Muscle palsy (no resistance)

May 1, 2023PARALYTIC STRABISMUS
54
PARK'S THREE-STEP TEST
?Which eye is hyper deviated in primary gaze
?Is the vertical deviation greater in right gaze or left gaze
?Is the vertical deviation greater with right head tilt or left head tilt.
LIMITATIOS• only for vertical deviations• Cannot tested for neuromyopathic
conditions.

May 1, 2023PARALYTIC STRABISMUS
55
HESS CHARTING

May 1, 2023PARALYTIC STRABISMUS
56
DIPLOPIA CHARTINGTo assess Extra ocular muscle paresis.Disadvantages:• Qualitative• Requires co-
operatio and intelligent patient
• Cannot do for colour blind patients

May 1, 2023PARALYTIC STRABISMUS
57
POST POINTING TEST • A test of the integrity of vestibular system.

May 1, 2023PARALYTIC STRABISMUS
58
LESS CHARTING

May 1, 2023PARALYTIC STRABISMUS
59
NEUROMUSCULAR JUNCTION LESION
It includes myasthenia gravis:A rare chronic autoimmune disease marked by muscular weakness without atrophy, and caused by a defect in the action of acetylcholine at neuromuscular junctions.

May 1, 2023PARALYTIC STRABISMUS
60differences
Paralytic Non paralytic
Age of onset
Usually late Usually early childhood
Type of onset
Sudden Gradual, sudden manifestation
Precipitating events
Usually head injury , systemic illness
Rarely present. Even if present no cause effect relationship
Associated neurological signs
May be present None
Comitance
May develop in late stages
Usually present (except in extreme gazes)

May 1, 2023PARALYTIC STRABISMUS
61
REFERENCES1) BINOCULAR VISION & STRABISMUS –GK
VON NOORDEN 2) CLINICAL MANGEMENT OF STRABISMUS-
ELEZABETH E.CALAROSSA & MICHAEL W. ROUSE
3) AAO- SECTION: PEDIATRIC OPHTHALMOLOGY & STRABISMUS
4) STRABISMUS SIMPLIFIED- PRADEEP SHARMA
5) PRACTICAL ORTHOPTICS IN THE TREATMENT OF SQUINT- LYLE AND JACKSON’S.

May 1, 2023PARALYTIC STRABISMUS
62