Embed Size (px)
Citation preview
Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
Pediatric Vaccine Preservatives
Aluminum, Thimerosal, and Formaldehyde
By Kimmer Collison-Ris
MSN, FNP-BC, WOCN, MS CAM ACHS Chem 501 Fall 2015
Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
1
Abstract
Vaccines are used to decrease disease in humans and have been used for the past 100 years.
Since the 1960’s a number of vaccines have been added to the vaccine schedule with the required
pediatric doses nearly tripling since 1983 (Graphic 1 at left). Today the diseases vaccines address
are less prevalent in developed nations due to modern health and hygiene practices along with
aggressive vaccination programs (CDC, 2015). Pediatric autoimmune and neurodevelopmental
disorders have significantly increased in the last few decades (Velasques-Manoff, 2012).
Because our current vaccines contain several different preservatives which have a recognized
negative health impact; health providers, researchers and parents are questioning the risk verses
benefit to pediatric patients. A literature Search was performed utilizing the search engine
Google Scholar and Google for information on the current vaccine schedule and each vaccine’s
ingredients. Three main preservatives were chosen as the topic of interest: Aluminum,
Thimerosal (Ethylmercury), and Formaldehyde. Did a reasonable concern exist regarding
specific vaccine preservatives and safety in some populations? Could Aluminum, Thimersal
(Ethylmercury), and Formaldehyde used as preservatives in small doses in vaccines be more
harmful than beneficial to special populations? This paper seeks to analyze three preservative
ingredients and their impact on health to evaluate if cautions should be considered for the current
vaccine schedule in specific vulnerable populations.

Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
2
Pediatric Vaccine Preservatives: Aluminum, Thimerosal, and Formaldehyde
Introduction
Vaccines are used to decrease disease in humans and have been used for the past 100 years.
Since the 1960’s a number of vaccines have been added to the vaccine
schedule with the required pediatric doses nearly tripling since 1983
(Graphic at left). Pediatric autoimmune and neurodevelopmental
disorders have significantly increased in the last few decades
(Velasques-Manoff, 2012). Because our current vaccines contain
several preservatives which have a recognized negative health impact;
health providers, researchers and parents are questioning the risk
verses benefit to pediatric patients.
There has been great controversy and concern over the safety and efficacy of the current
vaccine schedule given the myriad of ingredients contained in the vaccines on the developing
neurological system and the necessity regarding the types and numbers of required pediatric
vaccines. Today the diseases vaccines address are less prevalent in developed nations due to
modern health and hygiene practices along with aggressive vaccination programs (CDC, 2015).
Many vaccine proponents believe the current vaccine schedule is necessary for continued disease
control. Opponents question their safety and efficacy as preservatives used in vaccines may be to
blame for the increase in pediatric neurodevelopmental disorders, immune dysfunction, and
some cases of pediatric mortality. Could the rising incidence of neurodevelopmental disorders be
related to a cumulative effect of increased vaccine preservatives, genetic vulnerability and
immune dysfunction? Could Aluminum, Thimersal (Ethylmercury), and Formaldehyde used as
preservatives in small doses in vaccines be more harmful than beneficial to special populations?
Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
3
This paper seeks to analyze three preservative ingredients and their impact on health to evaluate
if cautions should be considered for the current vaccine schedule in specific populations.
Research Methodology
A literature Search was performed utilizing the search engine Google Scholar and Google for
information on the current vaccine schedule and each vaccine’s ingredients. Three main
preservatives were chosen as the topic of interest: Aluminum, Thimerosal (Ethylmercury), and
Formaldehyde. Research Parameters involved searching abstracts and articles by scientists and
healthcare providers from 1985 to the present on vaccine ingredients, vaccine preservatives,
Aluminum and health, Aluminum and development, Aluminum and human toxicity,
Ethylmercury and vaccines, Ethylmercury and health, Ethylmercury and toxicity, Ethylmercury
and Methyl Mercury, Formaldehyde and vaccines, Formaldehyde and human health,
Formaldehyde absorption, Formaldehyde health effects, and Formaldehyde and development.
Additionally, searches for descriptions of vulnerable populations and relationship to Aluminum,
Ethylmercury, and Formaldehyde were also performed.
History of Vaccination
Immunization began when it was discovered that a milkmaid who contracted cowpox did not
then develop smallpox when later exposed. From this observation, Edward Jenners created the
world's first vaccine for smallpox in the 1790s. The Pertussis vaccine was licensed in 1949, Polio
in 1955, Mumps in 1967, Measles in 1963, and Hepatitis A received licensing in 1995 and
Hepatitis B in 1991. These diseases have reportedly been on the decline in developed nations
believed to be due to increased nutrition, sanitation, health and hygiene practices prior to the
aforementioned vaccine requirements (McKinlay, McKinlay, and Milbank; 1977). However, the
WHO (2014) and the CDC (2014) report that the decline in the infectious diseases named is
Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
4
related to their aggressive vaccination and booster programs worldwide. Pertussis has
experienced a resurgence among the vaccinated (Mughal, Kazi, Bukhari, Ali, 2012).
Purpose of Vaccines
Prior to birth, a baby receives antibodies from the mother. These maternal antibodies provide
protection against many of the previously “usual childhood infections” such as measles, mumps
and chickenpox, and bacteria such as H. influenzae and Streptococcus pneumoniae. For a few
weeks after birth, babies have some protection from germs that cause diseases; this protection is
passed from their mother through the placenta before birth. The levels of these antibodies
decrease so that by 6 months, protection is minimal. “The decision as to when to give a vaccine
is based on the epidemiology of the vaccine preventable disease. Often, these diseases are more
severe in younger children. Therefore, we start early to ensure that the youngest and often most
fragile are protected as soon as possible” (NIH, 2015). The vaccine schedule ensures that while
the levels of maternal antibody are falling, infants are developing their own antibodies due to
immunizations. The goal is to protect the infant as soon as possible. Although the incidence of
most vaccine-preventable diseases in the United States is very low, the CDC claims this is
because the majority of U.S. children are immunized (Fisher and Bocchini 2009).
Vaccine Ingredients
Vaccines contain antigens, which cause the body to develop
immunity. Additionally, they contain adjunctive ingredients which
assist in producing the vaccine, or in prolonging shelf life and
protection from viral and/or bacterial contamination (CDC, 2014).
Chemicals used in the production of vaccines include suspending
fluid (sterile water, saline, or fluids containing protein);
Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
5
preservatives and stabilizers (albumin, phenols, and glycine); adjuvants or enhancers that
enhance the vaccine's effectiveness, and culture material used to grow the virus or bacteria
(http://www.cdc.gov/vaccines/vac-gen/additives.html). Key preservatives used in vaccines
include Aluminum, Ethyl Mercury (Thimerosal), and Formaldehyde. The graphic lists common
vaccine ingredients and their function (socioecohistory.wordpress.com). For a detailed list of
current vaccines and their specific ingredients see (Table 3) at the end of this paper.
Key Vaccine Preservatives
Aluminum
Aluminum (Al) is a trivalent cation found in its ionic form in most kinds of animal and plant
tissues and in natural waters everywhere. It is the third most prevalent element and the most
abundant metal in the earth's crust, representing approximately 8% of total mineral components.
Due to its reactivity, Al in nature is found only in combination with other elements (Bernardo,
2014). There is no known physiological role for aluminum within the body and hence this metal
may produce adverse physiological effects (Nayak 2002). Al is used in vaccines as a
preservative in the form of a gel or salt and added to the vaccine to enhance the vaccine by
promoting an earlier, more potent response, and more persistent immune response to the vaccine
(CDC, 2014).
Al impact upon animal and human health
Al is absorbed from the GI tract in the form of oral phosphate-binding agents (aluminum
hydroxide), parenterally via immunizations, in dialysate, total parenteral nutrition contamination,
via bladder irrigation, and transdermally (antiperspirants). Lactate, citrate, and ascorbate all
facilitate GI absorption. If a significant Al load exceeds the body's excretory capacity, excess is
deposited in various tissues (bone, brain, liver, heart, spleen, and muscle). This accumulation
Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
6
causes morbidity and mortality through various mechanisms (Bernardo, 2014).
In healthy subjects, only 0.3% of oral Al is absorbed via the GI tract and the kidneys
effectively eliminate Al from the human body. When the GI barrier is bypassed, as in IV infusion
or advanced renal disease, does Al accumulate. For example, 40% of IV infused Al is retained in
adults but up to 75% is retained in neonates (Yokel, 2000). Decreased renal function increases
human risk of Al-induced accumulation and toxicity. Brain Al entry from blood may involve
transferrin-receptor mediated endocytosis and a more rapid process transporting small molecular
weight Al species. Al efflux appears from the brain, possibly as Al citrate. Potential for
accumulation of Al exists from repeated exposure, as there is prolonged retention of Al fraction
that enters the brain.
Al is a neurotoxicant in animals and humans exhibiting similar effects on the brain as
mercury. This neurotoxicity, produced by several mechanisms, (Xu, Farkas, Kortbeek, Zhang,
Chen, Zamponi, and Syed (2012) damages the immune system and may be key in increased
pediatric autoimmune diseases. Mitochondrial disorder is suspected in association with severe
vaccine-injury, including autism as Al toxicity targets the mitochondria (Piper-Terry, 2012). Al
is now implicated in the etiology of sporadic Alzheimer's disease (AD) and other
neurodegenerative disorders (Yokel, 2000; Mercola 2010). Excess, insoluble amyloid beta
protein (A beta) contributes to AD; promoting formation and accumulation of insoluble A beta
and hyperphosphorylated tau. Al mimics cortical cholinergic neuro-transmission deficit as seen
in AD; Al increases Fe-induced oxidative injury. Al toxicity affects plants, aquatic life and
humans; likely by common mechanisms: disruption of the inositol phosphate system and Ca
regulation. Fe-induced oxidative injury facilitation and disruption of basic cell processes may
mediate primary molecular mechanisms of Al-induced neurotoxicity (Yokel, 2000). Largely
Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
7
95% of an Al load becomes bound to transferrin and albumin intravascularly; later renally
excreted (Barnardo, 2014).
Animal studies using rats, mice, and rabbits; found that Al is distributed transplacentally and
is present in milk. Oral Al ingestion during pregnancy produces a syndrome including growth
retardation, delayed ossification, and malformations at doses that also cause reduced maternal
weight gain. The severity of the effects is dependent on the form of Al given. Postnatally,
reduced pup weight gain and neuromotor development effects are a result of developmental
exposures (Golub and Domingo, 1996). Al Injections to animals produce behavioral,
neuropathological and neurochemical changes that partially model AD (Yokel, 2000).
When Al Toxicity occurs the action potential is blocked, decreasing neuron transmission
within the brain. Enzymes as catalysts are inhibited. This neurotransmitter inhibition of
Dopamine, Norepinephrine and Serotonin (5-HTP) directly impacts attention, impulse control,
mood regulation, sleep/wake cycles, hunger/satiety, voluntary/involuntary movement, and fight-
or-flight responses; thus leading to ineffective sensory processing of auditory/visual stimuli;
auditory processing disorder, visual processing disorder, and sensory integration dysfunction
(Piper-Terry, 2012). In all cases, Aluminum toxicity is largely related to Al bioavailability,
which then depends upon Al coordination chemistry in vivo. The highly polarizing power of the
Al3+ ion dictates its particular affinity for oxygen donors that abound in essential biomolecules
and dietary substances. The influence of these substances on Al bioavailability, metabolism and
toxicity can be assessed through animal models. However, understanding the mechanisms
through which Al–ligand interactions may influence physiological processes on the molecular
level requires knowledge of the speciation of the metal in the main biofluids (Berthon, 2002).
Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
8
Formaldehyde
Formaldehyde is an odorless, highly toxic, slightly heavier than air, volatile organic
compound, that easily becomes a vapor or flammable gas at room temperature. It has a pungent,
highly irritating, suffocating odor; detectable at low concentrations, but may not provide
adequate warning of hazardous concentrations for sensitized persons (ATSDR, 2015). It is also
naturally produced in small, harmless amounts in the human body. The chemical symbol for
formaldehyde is CH2O (Geier and Geier, 2004). Synonyms include formalin, formic aldehyde,
methanal, methyl aldehyde, methylene oxide, oxomethane, and paraform (ATSDR, 2015).
Formaldehyde is used in vaccines in an aqueous solution stabilized with methanol and used as a
preservative to inactive bacterial toxin products for toxoid vaccines, to produce immunity, and to
kill viruses during the manufacturing and storage process. A large percentage of formaldehyde
is removed from the vaccine before packaging (CDC, 2015).
Impact on human/animal health
Formaldehyde is highly toxic to all animals, regardless of method of intake (ATSDR, 2015;
ChemSee, 2015) being absorbed well by the lungs, gastrointestinal tract, and, to a lesser extent,
skin. Systemic effects include metabolic acidosis, CNS depression and coma, respiratory
distress, and renal failure. Formaldehyde reacts with strong oxidizers, alkalis, acids, phenols, and
urea. Children may be more susceptible than adults to the respiratory effects. It interacts with
proteins and DNA on cell membranes in body tissues and fluids; disrupting cellular functions.
High concentrations cause precipitation of proteins, which results in cell death. It is a potent
sensitizer and known human carcinogen and listed as a human carcinogen in the Thirteenth
Report on Carcinogens published by the National Toxicology Program as it causes cancer of the
throat, nose, and blood (ATSDR, 2015).
Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
9
Studies on the interactions between formaldehyde and proteins at the molecular level, affect
the body’s carrier protein, serum albumin. This binding loosens the skeletal structure of albumin
and exposure of the aromatic ring amino acids in the internal hydrophobic region (Wikepedia,
2015). Exposure affects personal awareness, causing fatigue and if prolonged, can cause severe
allergic reactions of the eyes, skin (rashes), and asthma-like symptoms (coughing, wheezing,
chest tightness), menstrual disorders, and subnormal body temperature. Asthmatics appear more
sensitive to formaldehyde (Geier and Geier, 2004; NIH, 2015).
Thimersol (Ethylmercury)
Mercury exists in several chemical forms; each with specific effects on human health:
Methylmercury, Ethylmercury, Elemental mercury, inorganic and organic mercury compounds
(EPA.gov, 2014; WHO, 2014). It is a highly toxic element second only to radioactive plutonium,
when combined with other ingredients, specifically aluminum and formaldehyde, as the
synergistic effects increase 10,000-fold (Laibow, 2015).
Thimerosal (Ethylmercury), an organic compound, is 49.6% mercury by weight and is
metabolized or degraded into Ethylmercury and thiosalicylate. Ethylmercury is a cation
composed of an ethyl group bound to a mercury(II) center; its chemical formula is C2H5Hg+.
Known as, C9H9HgNaO2S, it is formed from combining of ethyl mercuric chloride, thiosalicylic
acid, sodium hydroxide, and ethanol. Currently, there are no existing guidelines for
Ethylmercury, the metabolite of Thimerosal (FDA.gov, 1999). Thimerosal (sodium
ethylmercurithiosalicylate), a preservative, used in some United States vaccines, was first
introduced by Eli Lilly Company in the 1930's (CDC, 2014). It was added to vaccine vials
containing more than one dose to prevent contamination and growth of harmful bacteria.
However, it was removed from U.S.A. childhood vaccines (2001) and single-dose flu vaccines;
Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
10
except for the multi-dose inactivated flu vaccine vial (CDC, 2015).
Impact on human/animal health
Thimerosal has been studied in animal models only. Blair and colleagues (1975) studied
Thiomersal administered to adult squirrel monkeys who received a dose equivalent of 1 or 6
μg/kg/day Ethylmercury. Researchers noted Ethylmercury significantly converted to inorganic
mercury; with the highest levels were found in the kidney but low levels were present in the
brain. Adult male and female rats in another study were administered 5 daily doses of equimolar
concentrations of ethyl or methylmercury by gavage and tissue distribution, neurotoxicity and
nephrotoxicity assessed (Magos, Brown, Sparrow, Bailey, Snowden, Skipp; 1985). Researchers
found neurotoxicities of methyl and ethyl mercury were similar in the subjects. In this study,
higher levels of inorganic mercury were seen in the brains of the Ethylmercury treated rats and
renal damage was greater in Ethylmercury treated rats. Researchers concluded neither time-
course nor dose response attempted; they found the biological half-life in adults of ethyl mercury
30 - 50 days. Other studies report Ethylmercury clears from blood with a half-life of about 18
days in adults and is eliminated from the brain in about 14 days in infant monkeys.
Comparative Critical Toxicology Studies on Thiomersal related Ethyl mercury and
methylmercury have been performed. Both studied developmental neurotoxicity, assessing dose
response and age dependent responses. Mechanistic studies focused on critical changes in gene
function and cellular pathways. Evaluation of possible sensitive subpopulations based on genetic
predisposition, diet, and cumulative risk. Biomarkers of exposure including hair need to be
evaluated. “Ethylmercury is probably slightly less toxic than methylmercury. However, the
database for Ethylmercury is weak which creates considerable uncertainty in risk assessment
comparisons (Barrett, 2005). Ethylmercury should be considered equipotent to methylmercury as
Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
11
a developmental neurotoxin. This conclusion is clearly public health protective. Ethylmercury
exposure from vaccines (added to dietary exposures to methylmercury) probably caused
neurotoxic responses (likely subtle) in some children (IOM, 2015;).
Clinical manifestations of Ethylmercury poisoning include speech and vision disorders,
tremor, Ataxia, spasticity, delirium, and death. Fetuses exposed to forms of mercury in utero are
the most severely affected; symptoms include low birth weight, seizure disorders, profound
developmental delay, incomplete visual loss or total blindness, and hearing loss (Olson, 2014).
Neuronal atrophy is diffuse and widespread, found in severe in cases exposed in utero. Long-
term studies may indicate that even prenatal exposure at low concentrations can cause subtle, but
detectable, decrements in the areas of motor function, language, and memory. Affected children
may have long-term stigmata, including motor impairment, visual loss, hearing loss,
developmental delay, and seizure disorders (Olson, 2014).
The severity of health effects regarding Ethylmercury exposure include: the chemical form of
mercury, the dose, individual’s age at exposure (fetus most susceptible), duration of exposure,
route of exposure, and health at time of exposure (IOM, 2015). Blood levels of Ethylmercury
greater than 500 ppb can produce these adverse effects. Subtle measures of developmental
neurotoxicity (as done for Methylmercury) have not been evaluated. The Institute of Medicine
(IOM) emphasize infants are more susceptible than adults (IOM, 2015). Individuals who suffer
from chronic mercury exposure will have a unique expression of symptoms (Laibow, 2015).
Although Ethylmercury is approximately 5 times less acutely toxic than methylmercury,
Ethylmercury is a neurotoxin (IOM, 2015). Data is not adequate to compare potencies of
Ethylmercury and methylmercury for developmental neurotoxicity. The mechanisms responsible
for organomercurial caused developmental neurotoxicity are unknown and this also complicates
Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
12
evaluation of structure/ activity relationships. While the toxicity of low‐levels of Ethylmercury is
still under debate, the American Academy of Pediatrics, along with the American Academy of
Family Physicians, the Advisory Committee of Immunization Practices, and the US Public
Health Service issued a joint recommendation that Thimerosal be removed from vaccines as
quickly as possible as a precautionary measure (MountSinai.org, 2015).
Vulnerable Populations
There are a variety of definitions for vulnerable populations. The World Health Organization
(WHO) defines vulnerable populations as infants under 6 months, the elderly, breastfeeding or
pregnant women, and persons with underlying medical conditions (WHO, 2015b). Vulnerable
populations in this paper includes low birth weight or preterm infants, babies <6 months, nursing
or pregnant women, young children; individuals with chronic heart, lung, metabolic, renal or
liver disease; chronic neurological conditions, or immunodeficiencies, children aged 6 months to
5 years, and residents in long term care facilities. Seneff, Davidson, and Liu (2012) reported that
persons on the Autism spectrum were particularly vulnerable to Aluminum and Mercury. The
Mount Sinai Hospital website lists their group of vulnerable populations to Mercury exposure as
infants and young children (2015). Adverse Vaccine Reactions (VAERS)
The CDC recommends giving vaccinations to healthy persons; but often all infants, very
young children, low birth weight, poor renal function, and immunocompromised persons are
given vaccines regardless. The CDC states on the VAER website, “as with all medical products,
no vaccine is perfectly safe or effective. Vaccines can cause minor adverse effects such as fever
or local reactions at the injection site. Rarely, they can cause serious adverse effects such as
febrile seizures or severe allergic reactions. Adverse events (AE) can also occur coincidentally
Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
13
after vaccines…”(2015). A person can experience any of the symptoms listed in the hours, days
or weeks following vaccination which should be reported to VAERS.
Discussion
Safety and efficacy in specific populations
Children are especially sensitive to chemical exposure, particularly because their livers may
not be as effective at ridding the body of toxins, they have a high rate of cell growth and
division, which makes the cells more susceptible to damage. Damage to cells at an early age can
lead to defects that persist throughout their lifetimes. We do not even have sufficient testing
methods to evaluate the effect of chemical exposure on learning and cognitive ability. The
dramatic increase in Autism and Attention Deficit Hypersensitivity Disorder (ADHD) may be
linked to chemicals in the environment (IOM, 2015). "Given the large number of new chemicals
introduced into the environment each year, and the lack of information about their effect on
human function and health, particularly their potential effect on children, there is a growing need
to measure the exposures of children to these agents more systematically and to understand better
their potential effect on children's development. In addition, the levels of agents currently in the
environment known to pose an appreciable risk to children need to be monitored and child
populations at greater risk of environmental exposures identified (IOM, 2004).
Aluminum
Aluminum (Al) is a toxic metal to all living organisms; it can reach and accumulate in almost
every human body organ but the CNS is targeted for these deleterious effects. Select human
population can be at risk of Al neurotoxicity, and Al is implicated in neurodegenerative disease
etiology. Numerous efforts and accumulating research evidence, in the mechanisms of Al
neurotoxicity is still not fully understood (Verstraeten SV, Aimo L, and Oteiza PI, 2008). Yet
Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
14
developmental aluminum (Al) toxicity is available from clinical and animal testing studies
showing Al toxicity syndrome (encephalopathy, osteomalacia, and anemia) found in uremic
children receiving dialysis. Other nondialyzed uremic children receiving Al-based phosphate
binders, nonuremic infants receiving parenteral nutrition with Al-containing fluids, and
nonuremic infants given high doses of Al antacids manifest this syndrome as well. The number
of children in clinical populations that are at risk of Al toxicity is not known and needs to be
determined (Golub and Domingo, 1996). The significance of these findings for human health
requires better understanding of the amount and bioavailability of Al in food, drinking water, and
medications and from sources unique to infants and children such as breast milk, soil ingestion,
and medications used specifically by pregnant women and children (Golub and Domingo, 1996).
The factors initiating AD, how Al gains access to the brain in Alzheimer’s Disease (AD), and the
relative contributions of food, pharmaceuticals and skin absorption, remain unknown. The
devastating nature of the disease, lack of an effective treatment or prevention, high human and
health care costs; weighed against the cost of eliminating Al from vaccines to reduce exposure,
indicates that this action is reasonable and timely (McLachlan, 1995).
Formaldehyde
Studies on the interactions between formaldehyde and proteins at the molecular level, affect
the body’s carrier protein, serum albumin. This binding loosens the skeletal structure of albumin
and exposure of the aromatic ring amino acids in the internal hydrophobic region (Wikepedia,
2015). Children may be more vulnerable because of relatively increased minute ventilation per
kg and failure to evacuate an area promptly when exposed CNS impacts chronic exposure may
be more serious for children because of their potential longer latency period (ATSDR, 2015).
Formaldehyde is toxic, allergenic, and carcinogenic to most individuals (ChemSee, 2015). For
Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
15
children with a prior history of allergies or reactions, parents should consult their child’s
healthcare provider before vaccination (CDC, 2014).
Thimerosal (Ethylmercury)
Mercury is considered to toxic at any concentration in the body and can cause a very wide
range of psychophysiological disturbances (Pizzorno and Murray, 1993). Ethylmercury exposure
at high levels can harm the brain, heart, kidneys, lungs, and immune system of people of all ages.
The Institute of Medicine (2015) demonstrated that high levels of Ethylmercury in the
bloodstream of unborn babies and young children may harm the developing nervous system,
making the child less able to think and learn.
The World Health Organization reports that the half-life of ethyl mercury is short (<7 days)
verses methyl mercury (1.5 months) making exposure to ethyl mercury in blood comparatively
brief. Yet, recent studies reported by the Institute of Medicine state that clearance of
Ethylmercury in the body may take as long as 30 days (2015). WHO reports that Ethylmercury is
safer than methylmerchury as it is actively excreted via the gut (WHO, 2015) but the IOM
reports that Ethylmercury is also excreted via the kidneys (2015). The General Advisory Council
on Vaccine Safety (GACVS) concluded that the most recent pharmacokinetic and developmental
studies do not support concerns over the safety of Thiomersal (Ethylmercury) in vaccines. They
stated, “there is no reason on grounds of safety to change current immunization practices with
Thiomersal-containing vaccines, as the risks are unproven. However, data for well-nourished
neonates born at term cannot necessarily be extrapolated to preterm or malnourished infants”
(WHO, 2015). Other researchers emphasized, that the risks associated with low-level exposures
to inorganic mercury in the developing brain are unknown, and they describe other research
linking persistent inorganic mercury exposure with increased activation of microglia in the brain,
Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
16
an effect recently reported in children with autism. Further research was recommended to focus
specifically on the biotransformation of Thimerosal and its neurotoxic potential (Barrett, 2005).
There are many human developmental and genetic variants along with a growing list of
individuals experiencing adverse vaccine reactions and vaccine injury that proof of safety for
everyone is next to impossible without pre vaccine testing and individual assessments. The key
vaccine preservatives, Aluminum, Thimerosal, and Formaldehyde although placed in minute
doses in vaccines, do demonstrate health risks and negative health consequences.
Future Implications
We need a better understanding of the unique biological actions of Al that may occur during
developmental periods, and unique aspects of the developing organism that make it more or less
susceptible to Al toxicity (Golub and Domingo, 1996). Ethylmercury may not currently be
placed in U.S.A. pediatric vaccines, but the lack of concern by several Vaccine Councils suggest
it could return to market to decrease vaccine costs, so further vigilance to keep this out of
vaccines is necessary. Although formaldehyde is placed in minute quantities in vaccine,
numerous reports of formaldehyde- induced health problems, including poisoning and cancer
exist. Minimal quality epidemiological studies and basic data on exposed populations
emphasizes the need for extensive formaldehyde studies and its related health effects (Tang , Bai,
Duong, Smith, Li , and Zhang 2009) especially on the developing child.
Pre-vaccine Testing and Alternative Vaccine Schedules
Pre-vaccine testing is not currently performed but would be reasonable before embarking on
the recommended vaccine schedule. Testing for MTHFR gene deletions or variants, optimal
renal function, and sensitivities/reactivity/allergies to key vaccine ingredients is a necessary
option for parents and clinicians to pursue.
Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
17
Alternative current vaccine schedules should be considered. Examples include staggering
vaccines doses or eliminating certain vaccines for pediatric patients based upon individual
medical history. Total abstinence of vaccines in vulnerable populations: family or personal
history of adverse vaccine reaction or, genetic mutations, personal history of autoimmune
dysfunction, or severe allergies to key vaccine ingredients is reasonable. Although the CDC and
WHO report children need to be vaccinated early before their natural immunity wears off; it
would seem prudent in populations where children have low birth weight, were preterm, have
decreased renal function, are immunocompromised, have autoimmune dysfunction, demonstrate
neurodevelopmental disorders, or have genetic contraindications (as in MTHFR gene deletions).
Another proposal to the alternative schedule would be to stress breast-feeding up to 2 years of
age (or access to breast milk banks for non-breastfed babies) and vaccinate only when the child
reaches 24 months of age. Parents could decrease children’s exposure to illness through
continued health and hygiene practices, limiting exposure to large crowds, and opting out of
daycare centers where acquiring infectious illnesses pose a higher risk.
Dr. Rima Laibow, reports there is compelling evidence of vaccine related injury linking
neurological injuries and disorders, auto immune disorders, cancer, immune suppression, autism,
and lethal consequences to vaccine preservatives. Early and frequent administration of vaccines
multiplies this risk substantially (Laibow, 2015). Seneff and collegues state, “there are several
signs and symptoms that are significantly more prevalent in vaccine reports after 2000, including
cellulitis, seizure, depression, fatigue, pain and death, which are also significantly associated
with aluminum-containing vaccines. We propose that children with the autism diagnosis are
especially vulnerable to toxic metals such as aluminum and mercury due to insufficient serum
sulfate and glutathione. A strong correlation between autism and the MMR vaccine is also
Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
18
observed, which may be partially explained via an increased sensitivity to acetaminophen
administered to control fever” (Seneff, Davidson, and Liu; 2012).
Final Summary
Based upon the evidence, caution should be exercised in the following areas: giving vaccines
to women prior to conception, during pregnancy, and while nursing. Pre vaccination testing
should be performed to assess for genetic variants, neurodevelopmental disorders, decreased
renal function, and immune dysfunction. Vaccination delay is recommended for premature and
low birth weight infants, and children younger under 2 years of age; as excretion of these
preservatives may be poor.
Key take away points: Aluminum, Thimerosal (Ethylmercury), and Formaldehyde are
standard vaccine preservatives. Formaldehyde is a known carcinogen, immunosuppressive, and
mutanogen. Aluminum is neurotoxic, mutanogenic and immunosuppressive. Mercury and
Aluminum potentiate each other 100 fold which can occur when multiple vaccines are given
together. Although Ethylmercury is not contained in single dose flu vials, potential exists to
minimize its effects and to place it back in vaccines. It is also a neurotoxic, mutanogenic, and
immunosuppressive. All three preservatives demonstrate increased absorption in utero, in early
developmental phases, in vulnerable patients, and those with reduced renal function. Overall,
children are more systemically vulnerable to Aluminum, Mercury, and Formaldehyde.
Individuals with vulnerable immune systems and genetic variations should be protected from
the systemic threats that any of these preservatives possess. As each individual responds
uniquely, caution should be taken when mandating compulsory vaccination for the public as
multiple simultaneous preservatives appear to pose a valid threat to vulnerable populations. The
increase in proven vaccine injuries warrants further comprehensive analysis to study the

Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
19
simultaneous impact of these preservatives in different populations. Currently, there is enough
evidence to question the safety of the mandated vaccine schedule upon vulnerable populations.
Unfortunately, other preservative alternatives have not been introduced into the market.
Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
20
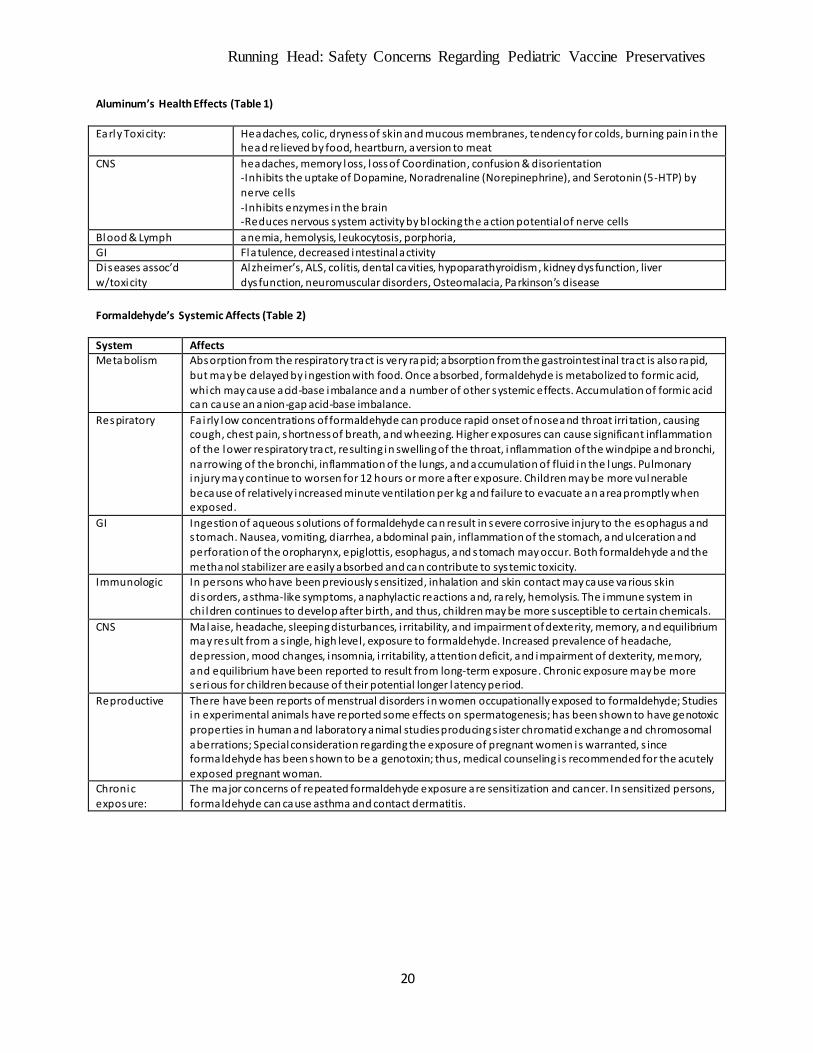
Aluminum’s Health Effects (Table 1)
Early Toxicity: Headaches, colic, dryness of skin and mucous membranes, tendency for colds, burning pain in the head relieved by food, heartburn, aversion to meat
CNS headaches, memory loss, loss of Coordination, confusion & disorientation -Inhibits the uptake of Dopamine, Noradrenaline (Norepinephrine), and Serotonin (5-HTP) by
nerve cells -Inhibits enzymes in the brain -Reduces nervous system activity by blocking the action potential of nerve cells
Blood & Lymph anemia, hemolysis, leukocytosis, porphoria, GI Flatulence, decreased intestinal activity
Diseases assoc’d w/toxicity
Alzheimer’s, ALS, colitis, dental cavities, hypoparathyroidism , kidney dysfunction, liver dysfunction, neuromuscular disorders, Osteomalacia, Parkinson’s disease
Formaldehyde’s Systemic Affects (Table 2)
System Affects Metabolism Absorption from the respiratory tract is very rapid; absorption from the gastrointestinal tract is also rapid,
but may be delayed by ingestion with food. Once absorbed, formaldehyde is metabolized to formic acid,
which may cause acid-base imbalance and a number of other systemic effects. Accumulation of formic acid can cause an anion-gap acid-base imbalance.
Respiratory Fa irly low concentrations of formaldehyde can produce rapid onset of nose and throat irri tation, causing cough, chest pain, shortness of breath, and wheezing. Higher exposures can cause significant inflammation
of the lower respiratory tract, resulting in swelling of the throat, inflammation of the windpipe and bronchi, narrowing of the bronchi, inflammation of the lungs, and accumulation of fluid in the lungs. Pulmonary injury may continue to worsen for 12 hours or more after exposure. Children may be more vulnerable because of relatively increased minute ventilation per kg and failure to evacuate an area promptly when exposed.
GI Ingestion of aqueous solutions of formaldehyde can result in severe corrosive injury to the es ophagus and s tomach. Nausea, vomiting, diarrhea, abdominal pain, inflammation of the stomach, and ulceration and
perforation of the oropharynx, epiglottis, esophagus, and s tomach may occur. Both formaldehyde and the methanol stabilizer are easily absorbed and can contribute to systemic toxicity.
Immunologic In persons who have been previously sensitized, inhalation and skin contact may cause various skin disorders, asthma-like symptoms, anaphylactic reactions and, rarely, hemolysis. The immune system in chi ldren continues to develop after birth, and thus, children may be more susceptible to certain chemicals.
CNS Malaise, headache, sleeping disturbances, i rritability, and impairment of dexterity, memory, and equilibrium may result from a s ingle, high level, exposure to formaldehyde. Increased prevalence of headache,
depression, mood changes, insomnia, i rritability, attention deficit, and impairment of dexterity, memory, and equilibrium have been reported to result from long-term exposure. Chronic exposure may be more serious for children because of their potential longer latency period.
Reproductive There have been reports of menstrual disorders in women occupationally exposed to formaldehyde; Studies in experimental animals have reported some effects on spermatogenesis; has been shown to have genotoxic
properties in human and laboratory animal studies producing s ister chromatid exchange and chromosomal aberrations; Special consideration regarding the exposure of pregnant women is warranted, s ince formaldehyde has been shown to be a genotoxin; thus, medical counseling i s recommended for the acutely exposed pregnant woman.
Chronic
exposure:
The major concerns of repeated formaldehyde exposure are sensitization and cancer. In sensitized persons,
formaldehyde can cause asthma and contact dermatitis.
Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
21
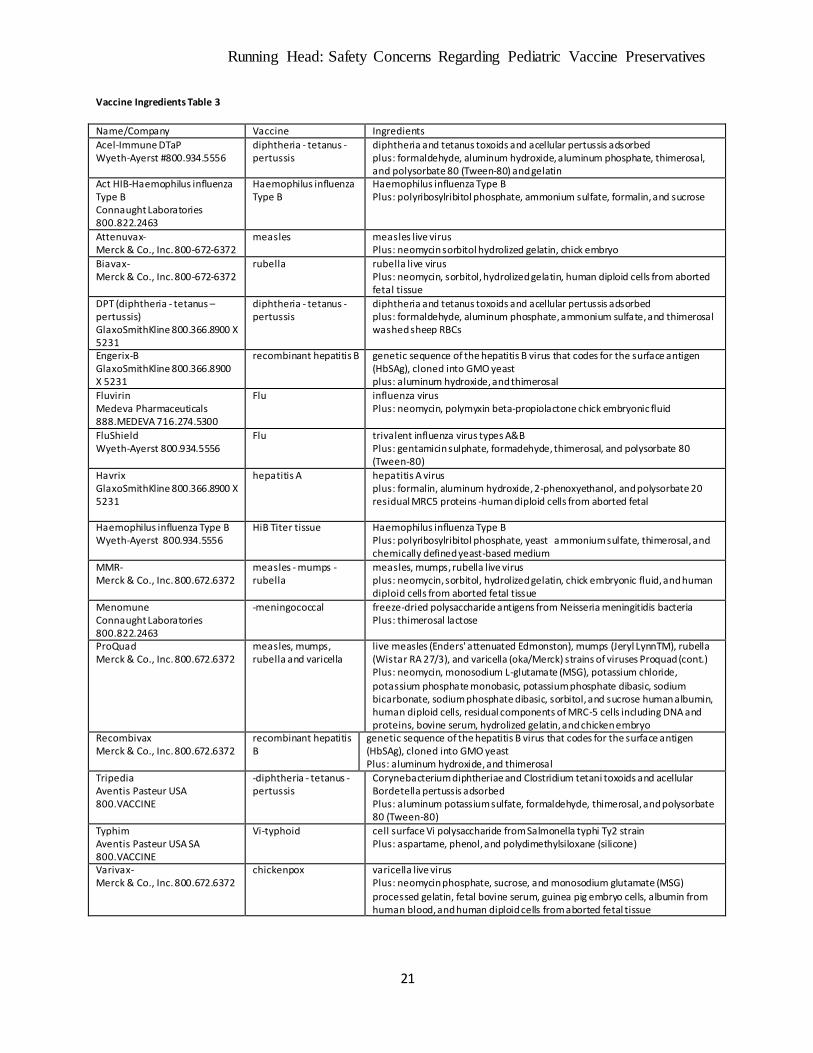
Vaccine Ingredients Table 3
Name/Company Vaccine Ingredients
Acel-Immune DTaP Wyeth-Ayerst #800.934.5556
diphtheria - tetanus - pertussis
diphtheria and tetanus toxoids and acellular pertussis adsorbed plus: formaldehyde, aluminum hydroxide, aluminum phosphate, thimerosal, and polysorbate 80 (Tween-80) and gelatin
Act HIB-Haemophilus influenza Type B Connaught Laboratories 800.822.2463
Haemophilus influenza Type B
Haemophilus influenza Type B Plus: polyribosylribitol phosphate, ammonium sulfate, formalin, and sucrose
Attenuvax- Merck & Co., Inc. 800-672-6372
measles measles live virus Plus: neomycin sorbitol hydrolized gelatin, chick embryo
Biavax- Merck & Co., Inc. 800-672-6372
rubella rubella live virus Plus: neomycin, sorbitol, hydrolized gelatin, human diploid cells from aborted fetal tissue
DPT (diphtheria - tetanus – pertussis) GlaxoSmithKline 800.366.8900 X 5231
diphtheria - tetanus - pertussis
diphtheria and tetanus toxoids and acellular pertussis adsorbed plus: formaldehyde, aluminum phosphate, ammonium sulfate, and thimerosal washed sheep RBCs
Engerix-B GlaxoSmithKline 800.366.8900 X 5231
recombinant hepatitis B genetic sequence of the hepatitis B virus that codes for the surface antigen (HbSAg), cloned into GMO yeast plus: aluminum hydroxide, and thimerosal
Fluvirin Medeva Pharmaceuticals 888.MEDEVA 716.274.5300
Flu influenza virus Plus: neomycin, polymyxin beta-propiolactone chick embryonic fluid
FluShield Wyeth-Ayerst 800.934.5556
Flu trivalent influenza virus types A&B Plus: gentamicin sulphate, formadehyde, thimerosal, and polysorbate 80 (Tween-80)
Havrix GlaxoSmithKline 800.366.8900 X 5231
hepatitis A hepatitis A virus plus: formalin, aluminum hydroxide, 2-phenoxyethanol, and polysorbate 20 residual MRC5 proteins -human diploid cells from aborted fetal
Haemophilus influenza Type B Wyeth-Ayerst 800.934.5556
HiB Titer tissue Haemophilus influenza Type B Plus: polyribosylribitol phosphate, yeast ammonium sulfate, thimerosal, and chemically defined yeast-based medium
MMR- Merck & Co., Inc. 800.672.6372
measles - mumps - rubella
measles, mumps, rubella live virus plus: neomycin, sorbitol, hydrolized gelatin, chick embryonic fluid, and human diploid cells from aborted fetal tissue
Menomune Connaught Laboratories 800.822.2463
-meningococcal
freeze-dried polysaccharide antigens from Neisseria meningitidis bacteria Plus: thimerosal lactose
ProQuad Merck & Co., Inc. 800.672.6372
measles, mumps, rubella and varicella
live measles (Enders' attenuated Edmonston), mumps (Jeryl LynnTM), rubella (Wistar RA 27/3), and varicella (oka/Merck) strains of viruses Proquad (cont.) Plus: neomycin, monosodium L-glutamate (MSG), potassium chloride,
potassium phosphate monobasic, potassium phosphate dibasic, sodium bicarbonate, sodium phosphate dibasic, sorbitol, and sucrose human albumin, human diploid cells, residual components of MRC-5 cells including DNA and proteins, bovine serum, hydrolized gelatin, and chicken embryo
Recombivax Merck & Co., Inc. 800.672.6372
recombinant hepatitis B
genetic sequence of the hepatitis B virus that codes for the surface antigen (HbSAg), cloned into GMO yeast Plus: aluminum hydroxide, and thimerosal
Tripedia Aventis Pasteur USA 800.VACCINE
-diphtheria - tetanus - pertussis
Corynebacterium diphtheriae and Clostridium tetani toxoids and acellular Bordetella pertussis adsorbed Plus: aluminum potassium sulfate, formaldehyde, thimerosal, and polysorbate 80 (Tween-80)
Typhim Aventis Pasteur USA SA 800.VACCINE
Vi-typhoid cell surface Vi polysaccharide from Salmonella typhi Ty2 strain Plus: aspartame, phenol, and polydimethylsiloxane (silicone)
Varivax- Merck & Co., Inc. 800.672.6372
chickenpox varicella live virus Plus: neomycin phosphate, sucrose, and monosodium glutamate (MSG)
processed gelatin, fetal bovine serum, guinea pig embryo cells, albumin from human blood, and human diploid cells from aborted fetal tissue
Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
22
Bibliography
ATSDR (2015). Toxic Portal: Formaldehyde, Medical Management Guideline for
Formaldehyde. Retrieved from http://www.atsdr.cdc.gov/mmg/mmg.asp?id=216&tid=39
Barrett, J (2005). Thimerosal and Animal Brains: New Data for Assessing Human Ethylmercury
Risk. Environ Health Perspect. Aug 2005; 113(8): A543–A544. Retrieved from
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1280369/
Bernardo JF (2014). Aluminum Toxicity. Medscape.
http://emedicine.medscape.com/article/165315-overview
Berthon G (2002). Aluminium speciation in relation to aluminium bioavailability, metabolism
and toxicity. Coordination Chemistry Reviews Volume 228, Issue 2, 3 June 2002, Pages
319–341. Retrieved from
http://www.sciencedirect.com/science/article/pii/S0010854502000218
CDC.gov (7/30/1999). Achievements in Public Health, 1900-1999: Control of Infectious
Diseases. Retrieved from
http://www.cdc.gov/mmwr/preview/mmwrhtml/mm4829a1.htm.
CDC.gov (2014). Vaccines and Vaccine Additives. Retrieved from
http://www.cdc.gov/vaccines/vac-gen/additives.htm
ChemSee (2015). Detectors for formaldehyde. Retrieved from
http://formaldehydetests.com/index.php?route=product/product&product_id=54)
Center for Biologics Evaluation and Research, U.S. Food and Drug Administration. 2008-06-03.
Retrieved 2008-07-25. Retrieved from http://en.wikipedia.org/wiki/Ethylmercury
Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
23
Ellison, S (2015). Herd Immunity: Three Reasons Why I Don’t Vaccinate My Children… And
Why Vaccine Supporters Shouldn’t Care That I Use Vaccine Exemption Forms. The
People’s Chemist. Retrieved from http://thepeopleschemist.com/reasons-dont-vaccinate-
children-vaccine-supporters-shouldnt-give/
EspInosa EC. Amenic and Merucry in Traditional Chinese Herbal Baits. NewEngjof Mod;
1995:333.803-804. Retrieved from
http://www.vaccinationnews.org/dailynews/may2002/mercurydetox.htm
EPA.gov (1999). Mercury Health Effects. Retrieved from
http://www.epa.gov/mercury/effects.htm.
FDA.gov (2014). Thimerosal in Vaccines Questions and Answers. Retrieved from
http://www.fda.gov/BiologicsBloodVaccines/Vaccines/QuestionsaboutVaccines/UCM07
0430
Fisher, MC and Bocchini, JA (2009). Adhering to vaccine schedule is best way to protect
children from disease. AAP News, Vol 30 No 1 Jan 2009. Retrieved from
http://www.immunize.org/aap/fisher.pdf
Foster HD (1992). Aluminum and Health. Retrieved from
http://www.orthomolecular.org/library/jom/1992/pdf/1992-v07n04-p206.pdf
Geier, D and Geier M (2004). Neurodevelopmental disorders following thimerosal-containing
childhood immunizations: a follow-up analysis. Int J Toxicol. 2004 Nov-Dec;23(6):369-
76. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/15764492
Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
24
Gilbert-Barness E, Barness LA, Wolff J, and Harding C (1998). Aluminum Toxicity. Arch
Pediatr Adolesc Med. 1998;152(5):511-512. doi:10.1001/archpedi.152.5.511.Retrieved
from http://archpedi.jamanetwork.com/article.aspx?articleid=189474
Golub MS and Domingo JL (1996). What we know and what we need to know about
developmental Aluminum toxicity. Journal of Toxicology and Environmental Health
Volume 48, Issue 6, 1996. Retrieved from
http://www.tandfonline.com/doi/abs/10.1080/009841096161087#.VK4h7U10zIU
Institute of Medicine (n.d.) Lucier-Comparative Toxicity of Ethyl and Methyl Mercury IOM,
Retrieved from
http://www.iom.edu/~/media/Files/Activity%20Files/PublicHealth/ImmunizationSafety/L
ucier.ashx.
Institute of Medicine (2004). Children's Health, the Nation's Wealth: Assessing and Improving
Child Health IOM, Board on Children, Youth and Families (BOCYF).
Informedchoice (2015). Vaccine Ingredients. Retrieved from
fromhttp://www.informedchoice.info/cocktail.html
Laibow, R (2015). Dr. Rima Truth Reports. Natural Solutions Foundation. Retrieved from
http://drrimatruthreports.com/whats- in-that-syringe-doctor/
Madhusudan G. Sonia, Susan M. Whiteb, W.Gary Flammc, and George A (2001). Safety
Evaluation of Dietary Aluminum. BurdockaRegulatory Toxicology & Pharmacology.
Volume 33, Issue 1, February 2001, Pages 66–79.
Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
25
Magos L, Brown AW, Sparrow S, Bailey E, Snowden RT, Skipp WR (1985). The comparative
toxicology of ethyl- and methylmercury. Arch Toxicol. 1985 Sep;57(4):260-7. Retrieved
from http://www.ncbi.nlm.nih.gov/pubmed/4091651.
McKinlay JB, McKinlay SM, Milbank (1977). The questionable contribution of medical
measures to the decline of mortality in the United States in the twentieth century. Mem
Fund Q Health Soc. 1977 Summer; 55(3): 405-28. Retrieved from
https://childhealthsafety.wordpress.com/graphs/
McLachlan DRC (1995). Aluminium and the risk for alzheimer's disease. Environmetrics,
Special Issue: Aluminium and Alzheimer's Disease. Volume 6, Issue 3, pages 233–275,
May/June 1995. Retrieved from
http://onlinelibrary.wiley.com/doi/10.1002/env.3170060303/abstract
Mercola, J (3/10/2010). New Warning About Everyday Poison Linked to Alzheimer's, ADHD,
and Autism. Retrieved from
http://articles.mercola.com/sites/articles/archive/2010/03/20/david-ayoub-interview-
february-2010.aspx
Mughal A, Kazi YF, Bukhari HA, Ali M (2012). Pertussis resurgence among vaccinated children
in Khairpur, Sindh, Pakistan. Public Health. 2012 Jun;126(6):518-22. doi:
10.1016/j.puhe.2012.02.001. Epub 2012 Mar 23. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/22445714.
Nayak P (2002). Aluminum: Impacts and Disease. Environmental Research. Volume 89, Issue 2,
June 2002, Pages 101–115. Retrieved from http://www.livingwhole.org/dear-parents-are-
Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
26
you-being- lied-to/)and
http://www.sciencedirect.com/science/article/pii/S0013935102943525
NIH (2015). Vaccines (immunizations) – overview. MedlinePlus. Retrieved from
http://www.nlm.nih.gov/medlineplus/ency/article/002024.htm
Olson DA (2014). Mercury Poisoning. Medscape.
http://emedicine.medscape.com/article/1175560-overview.
Parshad CohlyHH & Panja A (2005). Immunological Findings in Autism. International Review
of Neurobiology Volume 71, 2005, Pages 317–341DOI: 10.1016/S0074-7742(05)71013-
8. Retrieved at http://www.sciencedirect.com/science/article/pii/S0074774205710138>
Piper-Terry M (2012). Mercury and Aluminum in Vaccines: a Primer on NVIC’s Vaccine
Ingredients Calculator. Retrieved from <http://vaxtruth.org/2012/01/aluminum-toxicity-
and-a-primer-on-the-vic/>).
Pizzorno J and Murray M. Textbook of Natural Medicine. Churchill-Livingstone, 1993.
Seneff S, Davidson RM, and Liu J (2012). Empirical Data Confirm Autism Symptoms Related to
Aluminum and Acetaminophen Exposure. Entropy 2012, 14, 2227-2253;
doi:10.3390/e14112227. Retrieved from
http://people.csail.mit.edu/seneff/Entropy/entropy-14-02227.pdf.
Tang X, Bai Y, Duong A, Smith MT, Li L, and Zhang L (2009). Formaldehyde in China:
Production, consumption, exposure levels, and health effects. Environment International
Volume 35, Issue 8, November 2009, Pages 1210–1224. Retrieved from
http://www.sciencedirect.com/science/article/pii/S0160412009001378
Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
27
Tchounwou PB, Ayensu WK, Ninashvili N and Sutton D (2003). Environmental exposure to
mercury and its toxicopathologic implications for public health.DOI: 10.1002/tox.10116.
Retrieved from
http://onlinelibrary.wiley.com/doi/10.1002/tox.10116/abstract;jsessionid=2B8EBF5E61C
D8DBCDF207A9C6E250443.f03t04
Verstraeten SV, Aimo L, and Oteiza PI (2008). Aluminium and lead: molecular mechanisms of
brain toxicity. Archives of Toxicology November 2008, Volume 82, Issue 11, pp 789-
802. Retrieved from http://link.springer.com/article/10.1007/s00204-008-0345-3.
WHO (2015a). Statement on thiomersal. Retrieved from
http://www.who.int/vaccine_safety/committee/topics/thiomersal/statement_jul2006/en/
WHO (2015b). Protecting vulnerable groups from influenza. Retrieved from
http://www.euro.who.int/en/health-topics/communicable-diseases/influenza/protecting-
vulnerable-groups-from-influenza
Velasques-Manoff (8/25/2012). An Immune Disorder at the root of Autism. Retrieved from
http://www.nytimes.com/2012/08/26/opinion/sunday/immune-disorders-and-
autism.html?pagewanted=all&_r=0
Yokel RA (2000).Neurotoxicology. 2000 Oct;21(5):813-28. 200The toxicology of aluminum in
the brain: a review.Pasted from http://www.ncbi.nlm.nih.gov/pubmed/11130287
Xu F, Farkas S, Kortbeek S, Zhang F-X, Chen L, Zamponi GW, and SyedNI (2012).Mercury-
induced toxicity of rat cortical neurons is mediated through N-methyl-D-Aspartate

Running Head: Safety Concerns Regarding Pediatric Vaccine Preservatives
28
receptors. Mol Brain. 2012; 5: 30 Published online Sep 14, 2012. doi: 10.1186/1756-
6606-5-30. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3462706/.
Zhou W, Pool V, Iskander JK, English-Bullard R, Ball R, Wise RP, Haber P, Pless RP, Mootrey
G, Ellenberg SS, Braun MM, and Chen RT, (2003). Surveillance for Safety After
Immunization: Vaccine Adverse Event Reporting System (VAERS) --- United States,
1991—2001. CDC. Retrieved from
http://www.cdc.gov/MMWr/preview/mmwrhtml/ss5201a1.htm