Embed Size (px)
Citation preview

POSTO
PERAT
IVE
PULM
ONARY
HYPERT
ENSION
IN C
ARDIAC S
URGERY
PATI
ENTS
BY- D
R. ARM
AAN SIN
GH
BY- D
R. ARM
AAN SIN
GH
GUIDELINES FOR MANAGEMENT OF PULMONARY HYPERTENSION IN CARDIAC SURGERY PATIENTS
Increased PVR during postop period:
• SIRS 20 to CPBP (pulmonary vasoconstriction)
• Protamine (pulmonary vasoconstriction)
• Hypoxia (pulmonary vasoconstriction)
• ↑ pCO2, acidemia (pulmonary vasoconstriction)
• PEEP, ventilator dysynchrony (pulmonary vasoconstriction)
Sidebotham D, et al: Cardiothoracic critical care. Butterworth-Heinemann, Philadelphia 2007;24:374-382.
Sidebotham D, et al: Cardiothoracic critical care. Butterworth-Heinemann, Philadelphia 2007;20:296-308.
GUIDELINES FOR MANAGEMENT OF PULMONARY HYPERTENSION IN CARDIAC SURGERY PATIENTS
Pulmonary vasoconstriction:
• Hyperventilation counteracts hypoxic pulmonary vasoconstriction in man
• PAP increased (p < 0.001) with elevations in PaCO2
• Marked decrease in SVR with increasing PaCO2
• Blood pressure decreased (p < 0.001) with ↑ in PaCO2 up to 50 mmHg
Bindslev L, et al. Hypoxic pulmonary vasoconstriction in man: effects of hyperventilation. Acta Anesthesiol Scand. 1985;29:547-551.
Avidan MS, et al. Mild hypercapnia after uncomplicated heart surgery is not associated with hemodynamic compromise. J Cardiothorac Vasc Anesth 2007;21:371-374.
GUIDELINES FOR MANAGEMENT OF PULMONARY HYPERTENSIONIN CARDIAC SURGERY PATIENTS
Pulmonary vasoconstriction:
• Can precipitate acute right heart failure
• More frequent conditions: MVR, CHD with L → R shunt
• Heart Tx, Lung Tx
• Pneumonectomy
Sidebotham D, et al: Cardiothoracic critical care. Butterworth-Heinemann, Philadelphia 2007;24:374-382.
GUIDELINES FOR MANAGEMENT OF PULMONARY HYPERTENSIONIN CARDIAC SURGERY PATIENTS
Treatment of the underlying cause:
• Pulmonary vasoconstriction (pre-capillary PH) Avoidance of hypoxemia, hypercarbia & acidosis Sedation, analgesia & muscle relaxants Selective pulmonary vasodilatation
• Passive pulmonary hypertension with ↑ LAP (post-capillary PH) Improve LV contractility Decrease degree of MR Nesiritide
Sidebotham D, et al: Cardiothoracic critical care. Butterworth-Heinemann, Philadelphia 2007;24:374-382.
MANAGEMENT OF LEFT HEART FAILURE WITH SECONDARY PULMONARY HYPERTENSION
IN CARDIAC SURGERY PATIENTS
Nesiritide :
Perioperative management of patients with severe MR, severe LV dysfunction and secondary pulmonary hypertension
Expected mortality by EuroSCORE 26% Preoperative treatment with Nesiritide for 13-55 hr (mean=24 hr) Postoperative treatment with Nesiritide for 2-80 hr (mean=22 hr) Improves postop renal function and survival
Salzberg SP, et al: High-Risk mitral valve surgery. Perioperative hemodynamic optimization with Nesiritide (BNP). Ann Thorac Surg 2005;80:502-506.
MANAGEMENT OF LEFT HEART FAILURE WITH SECONDARY PULMONARY HYPERTENSION
IN CARDIAC SURGERY PATIENTS
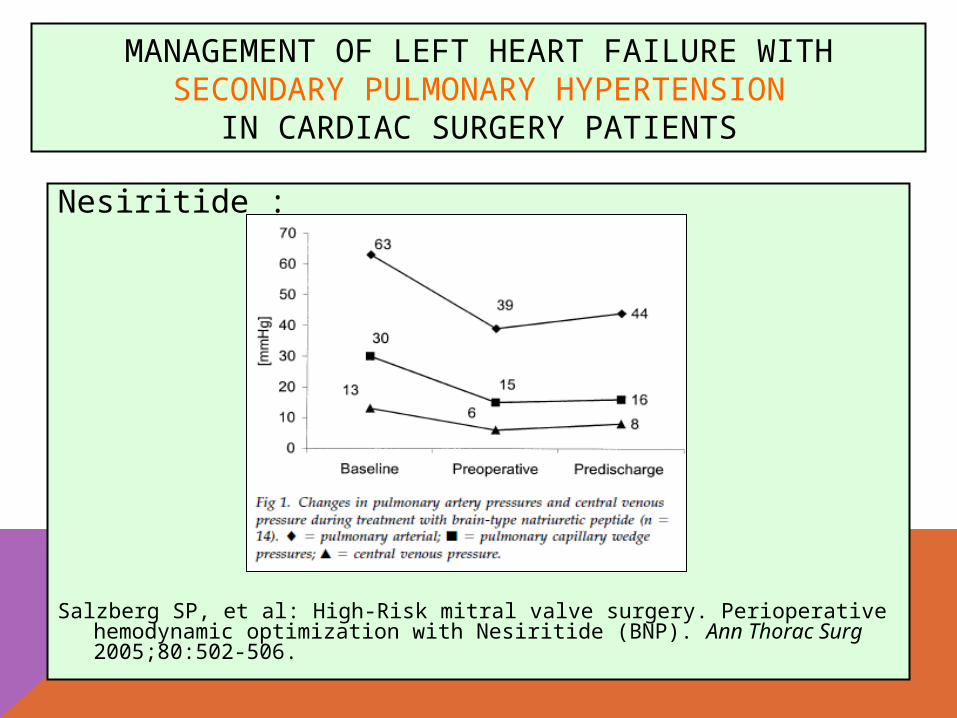
Nesiritide :
Salzberg SP, et al: High-Risk mitral valve surgery. Perioperative hemodynamic optimization with Nesiritide (BNP). Ann Thorac Surg 2005;80:502-506.
MANAGEMENT OF LEFT HEART FAILURE WITH SECONDARY PULMONARY HYPERTENSION
IN CARDIAC SURGERY PATIENTS
Nesiritide:
Hemodynamic benefits: ↓ PAP, ↓ CVP, ↑ CO Improves postop renal function Decreases respiratory failure and AF Decreases LOS Decreases mortality
Blais DM. Nesiritide Compared with Milrinone for Cardiac Surgery. Ann Pharmacother 2007;41:502-504. Mentzer RM, et al: Effects of Perioperative Nesiritide in Patients With Left Ventricular Dysfunction Undergoing Cardiac Surgery. The NAPA Trial. J Am Coll Cardiol 2007;49:716-726.
MANAGEMENT OF LEFT HEART FAILURE WITH SECONDARY PULMONARY HYPERTENSION
IN CARDIAC SURGERY PATIENTS
Nesiritide (Natrecor):
• Standard Dilution:
[1.5 mg] [250 ml D5W, D5½S or NS]
• Loading dose:
2 mcg/kg over 20 min
• Followed by 0.01 mcg/kg/min
• Continuous infusion x 48 hours
GUIDELINES FOR MANAGEMENT OF PULMONARY HYPERTENSION IN CARDIAC SURGERY PATIENTS
Selective pulmonary vasodilatation:
• Right heart failure resistant to therapy
• Pre-existing pulmonary hypertension
* Inhaled Nitric Oxide (iNO)
* Inhaled Prostacyclin (iPGI2)
* Inhaled Iloprost
* Sildenafil
Sidebotham D, et al: Cardiothoracic critical care. Butterworth-Heinemann, Philadelphia 2007;24:374-382.
GUIDELINES FOR MANAGEMENT OF PULMONARY HYPERTENSION IN CARDIAC SURGERY PATIENTS
Inhaled Nitric Oxide (iNO):
• Usual dose: 5 - 40 ppm • Selective pulmonary vasodilator • Does not cause systemic hypotension • Distributed only to ventilated portions of the lungs • Requires accurate gas delivery system to monitor NO and NO2 • May cause methemoglobinemia • May cause rebound pulmonary hypertension • Expensive
Sidebotham D, et al: Cardiothoracic critical care. Butterworth-Heinemann, Philadelphia 2007;24:374-382.
GUIDELINES FOR MANAGEMENT OF PULMONARY HYPERTENSION IN CARDIAC SURGERY PATIENTS
Inhaled prostacyclin (iPGI2):
• Usual dose: 5 - 50 ng/kg/min • Short-acting selective pulmonary vasodilator • Equally effective as iNO • Does not cause systemic hypotension • Distributed only to ventilated portions of the lungs • May cause thrombocytopenia • Does not cause rebound pulmonary hypertension • Inexpensive
Sidebotham D, et al: Cardiothoracic critical care. Butterworth-Heinemann, Philadelphia 2007;24:374-382.
GUIDELINES FOR MANAGEMENT OF PULMONARY HYPERTENSION IN CARDIAC SURGERY PATIENTS
Inhaled prostacyclin (iPGI2):
• Usual starting dose: 50 ng/kg/min • Weaning (3-4 days): 25-10-5-3 ng/kg/min • Selective pulmonary vasodilator • Does not cause systemic hypotension • Equally effective as iNO • Prolonged use is not associated with systemic effects • Readily available in most hospitals • Inexpensive
Lowson SM, et al: Inhaled prostacyclin for the treatment of pulmonary hypertension after cardiac surgery. Crit Care Med 2002; 30:2762-2764.
GUIDELINES FOR MANAGEMENT OF PULMONARY HYPERTENSION IN CARDIAC SURGERY PATIENTS
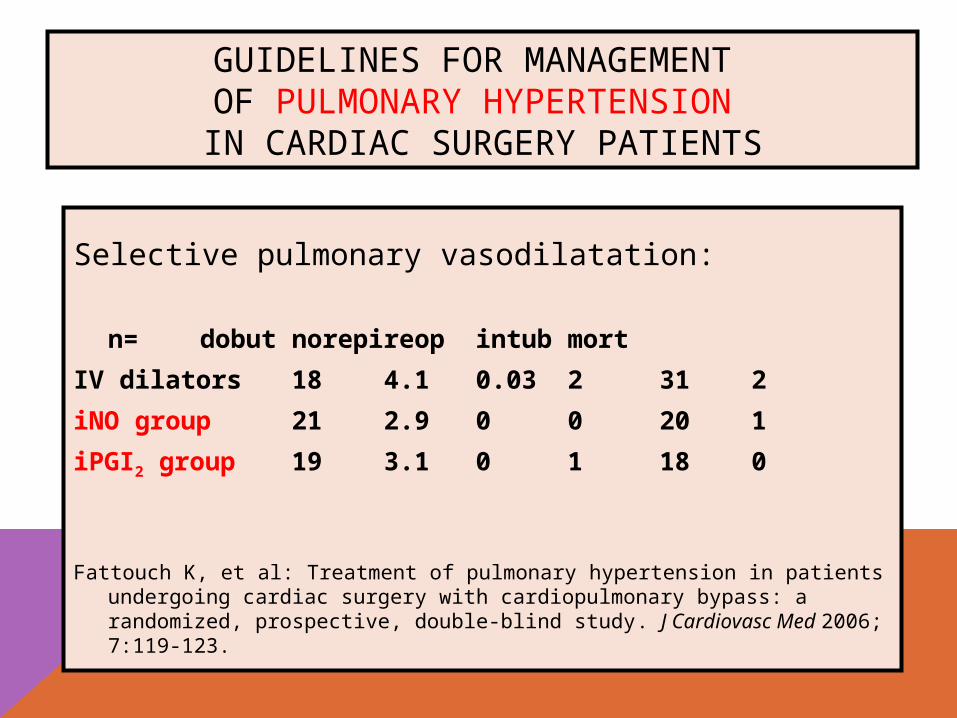
Selective pulmonary vasodilatation:
n= dobut norepi reop intub mort
IV dilators 18 4.1 0.03 2 31 2
iNO group 21 2.9 0 0 20 1
iPGI2 group 19 3.1 0 1 18 0
Fattouch K, et al: Treatment of pulmonary hypertension in patients undergoing cardiac surgery with cardiopulmonary bypass: a randomized, prospective, double-blind study. J Cardiovasc Med 2006; 7:119-123.
GUIDELINES FOR MANAGEMENT OF PULMONARY HYPERTENSION IN CARDIAC SURGERY PATIENTS
Inhaled prostacyclin (iPGI2):
• Equally effective as iNO
• Neither iPGI2 nor its metabolites have toxic effects
• Possible thrombocytopenia but does not increase risk of bleeding
• Easy administration
• Inexpensive
Fattouch K, et al: Treatment of pulmonary hypertension in patients undergoing cardiac surgery with cardiopulmonary bypass: a randomized, prospective, double-blind study. J Cardiovasc Med 2006; 7:119-123.
GUIDELINES FOR MANAGEMENT OF PULMONARY HYPERTENSION IN CARDIAC SURGERY PATIENTS
Inhaled iloprost:
• Usual dose: 12 - 20 mcg q 4-6 hr
• Intermittent nebulization
• Longer half-life selective pulmonary vasodilator
• Equally effective as iNO
• Does not cause systemic hypotension
• May cause thrombocytopenia
• Does not cause rebound pulmonary hypertension
• Intermittent nebulization requires periodic interruption of PEEP
Sidebotham D, et al: Cardiothoracic critical care. Butterworth-Heinemann, Philadelphia 2007;24:374-382.
GUIDELINES FOR MANAGEMENT OF PULMONARY HYPERTENSION IN CARDIAC SURGERY PATIENTS
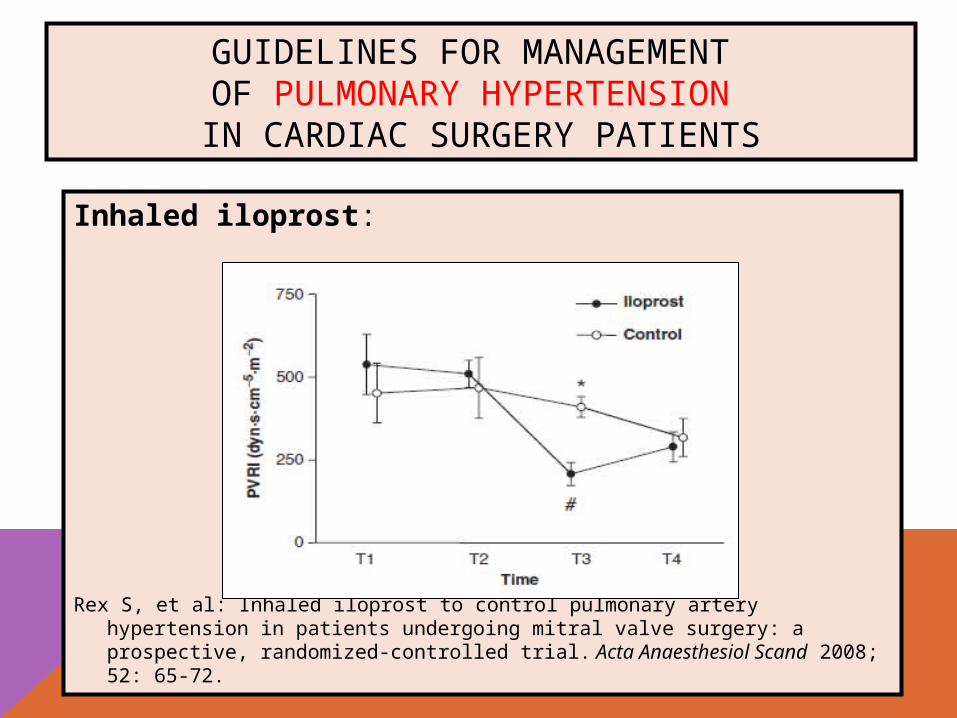
Inhaled iloprost:
Rex S, et al: Inhaled iloprost to control pulmonary artery hypertension in patients undergoing mitral valve surgery: a prospective, randomized-controlled trial. Acta Anaesthesiol Scand 2008; 52: 65-72.
GUIDELINES FOR MANAGEMENT OF PULMONARY HYPERTENSION IN CARDIAC SURGERY PATIENTS
Sildenafil:
• Equally effective as iNO
• Increases cardiac output
• Does not increase wedge pressure
• Oral or IV administration
• Inexpensive
Michelakis E, et al: Oral Sildenafil is an effective and specific pulmonary vasodilator in patients with pulmonary arterial hypertension. Comparison with inhaled nitric oxide. Circulation 2002;105:2398-2403.
GUIDELINES FOR MANAGEMENT OF PULMONARY HYPERTENSION IN CARDIAC SURGERY PATIENTS
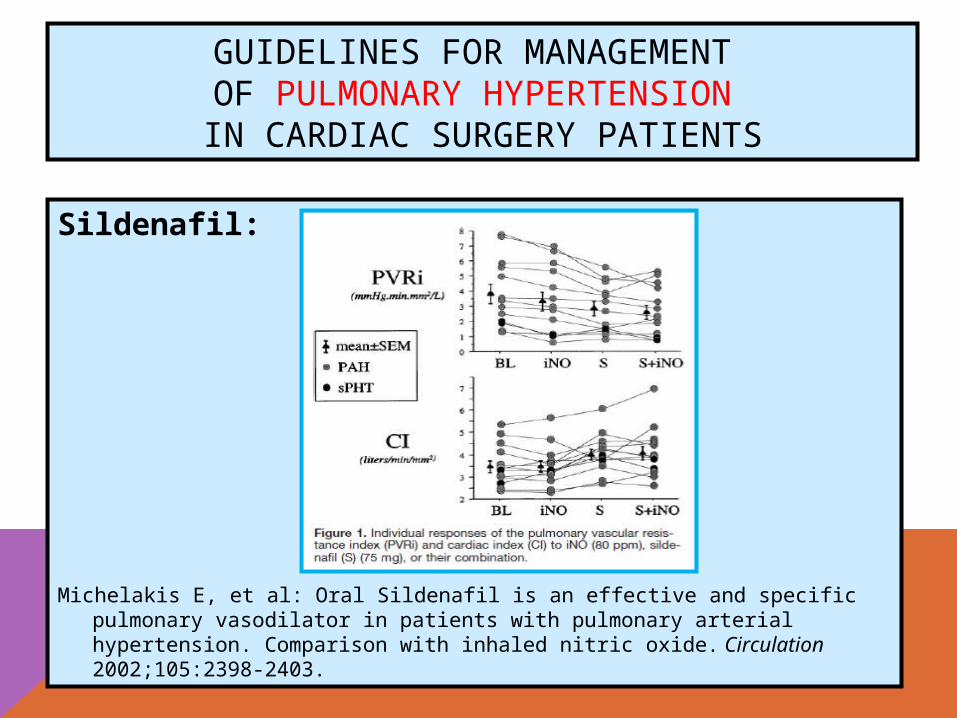
Sildenafil:
Michelakis E, et al: Oral Sildenafil is an effective and specific pulmonary vasodilator in patients with pulmonary arterial hypertension. Comparison with inhaled nitric oxide. Circulation 2002;105:2398-2403.
GUIDELINES FOR MANAGEMENT OF PULMONARY HYPERTENSION IN CARDIAC SURGERY PATIENTS
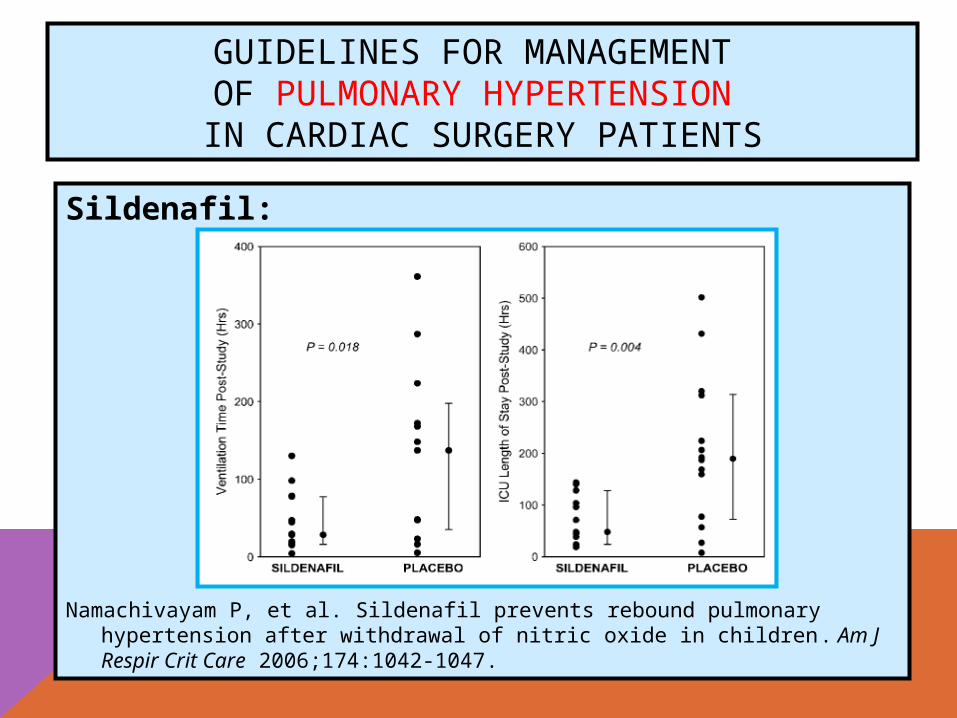
Sildenafil:
Namachivayam P, et al. Sildenafil prevents rebound pulmonary hypertension after withdrawal of nitric oxide in children. Am J Respir Crit Care 2006;174:1042-1047.
GUIDELINES FOR MANAGEMENT OF PULMONARY HYPERTENSION IN CARDIAC SURGERY PATIENTS
Sildenafil:
• Initial dose: 50-75 mg PO 10-30 min before induction of anesthesia
• Maintenance dose: 25 mg BID - 50 mg TID
• Pediatric dose: 0.4 mg/kg before discontinuing iNO
Shim JK, et al. Effect of oral sildenafil citrate on intraoperative hemodynamics in patients with pulmonary hypertension undergoing valvular heart surgery. J Thorac Cardiovasc Surg 2006;132:1420-1425.
Trachte AL, et al: Oral sildenafil reduces pulmonary hypertension after cardiac surgery. Ann Thorac Surg 2005;79:194-197.




























