Embed Size (px)
DESCRIPTION
Citation preview

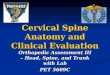
Occiput
PRA625






Occipitofrontalis

Semispinalis Capitis

Suboccipitals


Cranial manipulation
• Developed mid 1930’s
• Controversy
• Cottom
• Three Hypothesis– Dysfunction dural tension– CSF circulation– Stress and pressure

Technique
• Saggital suture spread
• Cranial universal
• Parietal lift



HW
• Read the article by Flynn et al
“The audible pop is not necessary for successful spinal HV manipulation in individuals with low back pain”



Cervical Spine

Cervical Spine
• Most vulnerable site for injury
• Common area everyday complaints and articular dysfunction
• Tri-planar motion
• Restoration of joint mobility

• 7 cervical vertebral segments
• 3rd, 4th, 5th and 6th typical vertebrae
• 1st, 2nd and 7th atypical vertebrae


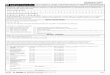
Cervical Vertebrae
• Seven vertebrae (C1-C7) are the smallest, lightest vertebrae
• C3-C6 are distinguished with an oval body, short spinous processes, and large, triangular vertebral foramina
• Each transverse process contains a transverse foramen



Cervical Vertebrae
Table 7.2

Cervical Vertebrae: The Atlas (C1)
• The atlas – Has no body and no spinous process– Consists of anterior and posterior arches, and
two lateral masses– The superior surface of lateral masses
articulate with the occipital condyles

Cervical Vertebrae: The Atlas (C1)
Figure 7.16a, b

Cervical Vertebrae: The Axis (C2)
• The axis has a body, spine, and vertebral arches as do other cervical vertebrae
Figure 7.16c

Cervical Vertebrae: The Axis (C2)
• Unique to the axis is the dens, or odontoid process, which projects superiorly from the body and is cradled in the anterior arch of the atlas
Figure 7.16c

Cervical Vertebrae: The Axis (C2)
• The dens is a pivot for the rotation of the atlas
Figure 7.16c

Biomechanics
• Cervical spine has numerous articulations
• Cervical spine – lordotic curve



• Cervical spine motion
• Rotation contributes to the greatest disc degeneration


• Cervical spine provides different motion characteristics
• Occipitoatlantal complex (C0-C1)
• Atlantoaxial complex (C1-C2)

• Greatest ROM occurs the middle of the cervical at the level of C5-C6 during flexion and extension
• Facet joints lie 45 degrees to the ventral and motion involves a coupled movement along both the X and Y axes
Rash,PJ and Burke RK. Kinesiology and Applied Anatomy. 1974
Bergman, DH and Peterson, TF. Chiropractic Technique. 2nd ed. 2002.

What is the coupled physiological effect of the cervical spine with left lateral flexion? (Hint: think facet, VB, Disc, SP)

• Lateral bending produces concomitant PA rotation, with spinous movements to the contralateral side of lateral flexion
• Coupling movement actually decrease gradually from C2-C7 as the incline of the facet joints
Bergman, DH and Peterson, TF. Chiropractic Technique. 2nd ed. 2002.

Biomechanics of Cervical Injury
Mechanism Structures Affected
• Flexion or axial compressive loading
• Posterior column elements
• Capsular ligaments• Supraspinous Lig• Interspinous Lig• Erector spinae gp• Trapezius muscle

Biomechanics of Cervical Injury
Mechanism Structures Affected
• Lateral flexion • Nerve root• Dorsal sleeve• Brachial plexus• Scalene muscles

Biomechanics of Cervical Injury
Mechanism Structures Affected
• Extension or axial rotation
• Anterior column elements
• ALL• Outer annulus of
disk• Apophyseal joints• SCM

Indications for manipulations
• Proper patient selection enhances the efficiency of CMT and minimizes the risk
• Complete H & P• Radiographic studies• A Pt with a sign of VBI or carotid artery
disease should have a vascular examination and Doppler studies

• H & P, neurological, orthopedic and radiography will generally indicate the appropriateness of CMT for the individual patients

• Cervical manipulation overcomes many musculoskeletal complaints essentially by restoring motion to the synovial joints of the spine, altering the existing tension of the myofascia, lengthing connective tissue, disrupting adhesions and relieving muscular hypertonicity

• Spinal manipulative therapy– 2 subcategories HVLA and HALV
• HVLA – involves a very fast movement with a very small amplitude and is usually followed by one or several noises at the articular level (cavitation)
• HALV – involves a big motion, such as flexion of the neck, performed at a slow, repetitive pace, not followed by an audible

• Most specific HVLA adjustments are MONO-VECTOR
• Involve a single vector during a thrust and vector is aligned wit the movement of a single intervertebral segment
• Thrust vector is in the closest direction to the facet-gliding plane
• Specific adjustment

• Zygapophyseal joint locking theory
– Joint fixation is probably multi-factorial and may involve derangement of the posterior articular joints, intra-discal degrangements, muscle spasm, soft tissue fibrosis etc.

Mechanisms of Action in Manipulative Therapy
• HVLA causes changes in the joint capsule tension
• Excites the mechanoreceptors of the synovial joints, primarily the type I and type II
• Type I mechanoreceptors contribute to perception of position and kinesthetic awareness

• Type II mechanoreceptors inhibit pain and exert a phasic (relaxing) effect on motor neurons
• Endogenous opiate release that follows CMT combined with nociceptor suppression at the cord level, also inhibit pain

• Upper cervical complex is critically important in manual therapy because of vascular insult
• Several investigators have reported moderate amounts of kinking of the vertebral arteries during moderate amounts of axial rotation even in individuals with no prior vascular disease

• Chiropractic profession is well aware of the cases of documented VBA infarct following manipulation by various practitioners of manual therapy
• A through practitioner should ALWAYS screen patients for neurovascular disturbances, especially VBAI, to ensure safety and efficacy of the cervical manipulation