Embed Size (px)
Citation preview
Dr/ ABD ALLAH NAZEER. MD.
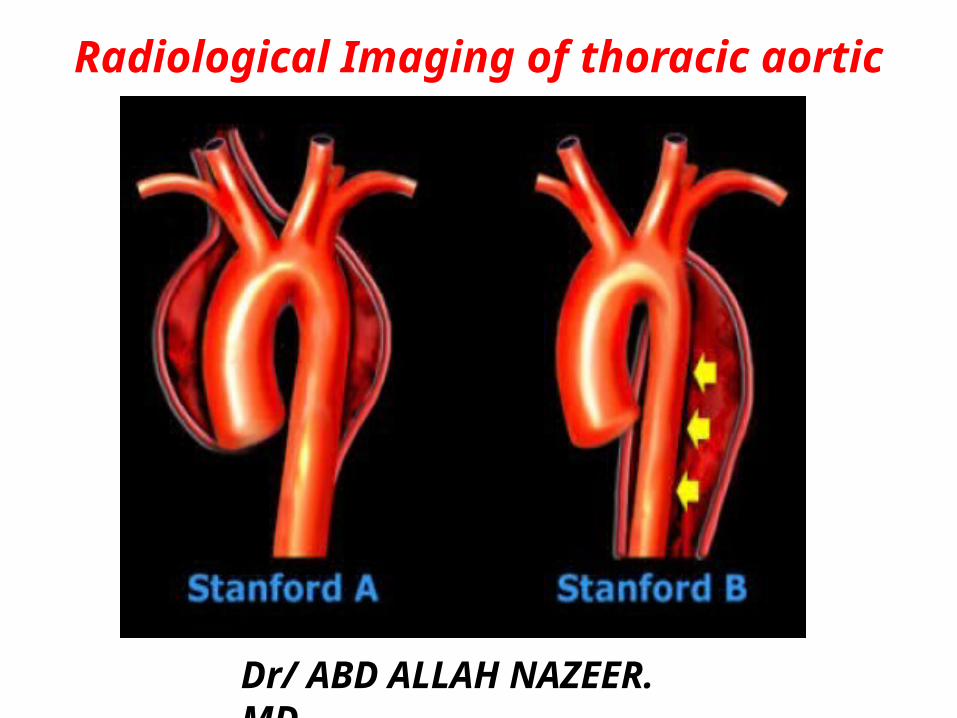
Radiological Imaging of thoracic aortic aneurysm.
Thoracic aortic aneurysms are relatively uncommon compared to abdominal aortic aneurysms. There is a wide range of causes, and the ascending aorta is most commonly affected. CTA and MRA are the modalities of choice to image this condition.TerminologyThe term aneurysm is used when the axial diameter of the thoracic aorta is > 5 cm and when it measures 4-5 cm the term dilatation is used.EpidemiologyMost commonly occur in 50 to 60-year-old age group and incidence is estimated at ~7.5 per 100,000 patient years. There is a male predominance (M:F=3:1).Clinical presentationThoracic aneurysms are often identified incidentally on imaging of the chest. A symptomatic presentation may be due to mass effect on airway or esophagus. Alternatively, they may present due to a complication, including rupture, aorto-bronchial or aorto-oesophageal fistulae.Pseudoaneurysms of the thoracic aorta are usually the result of significant thoracic trauma, both penetrating and blunt, and carry a very high mortality, with 80-90% of patients dying before reaching hospital
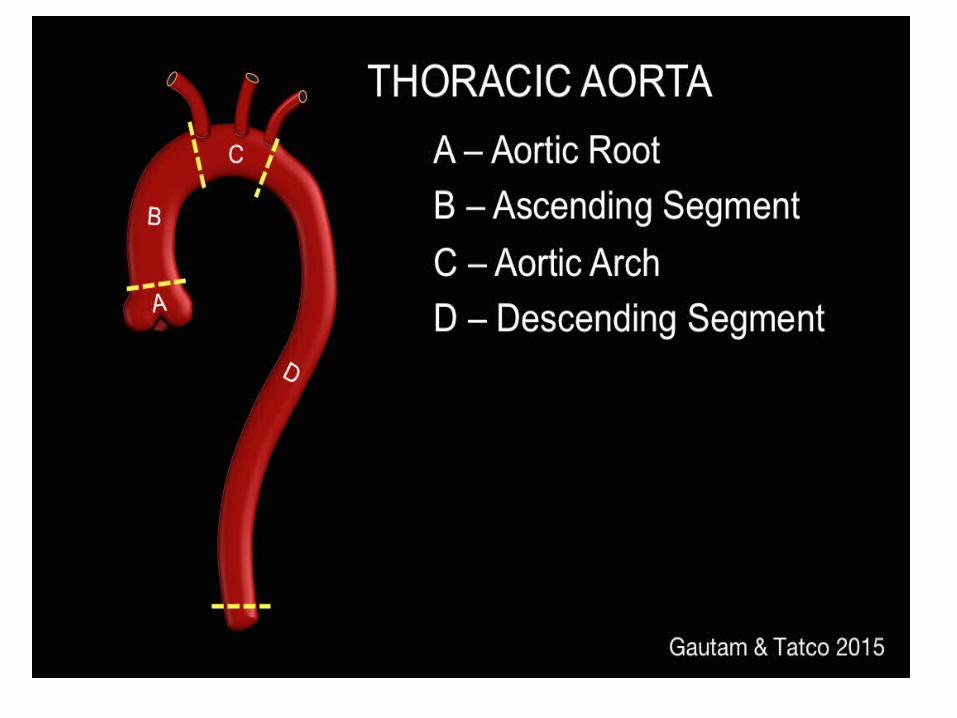
PathologyLocationAneurysmal dilatation can affect any part of the thoracic aorta. Relative frequencies are (with some involving more than one segment):aortic root/ascending aorta: 60%aortic arch: 10%descending aorta: 40%thoracoabdominal segment: 10%
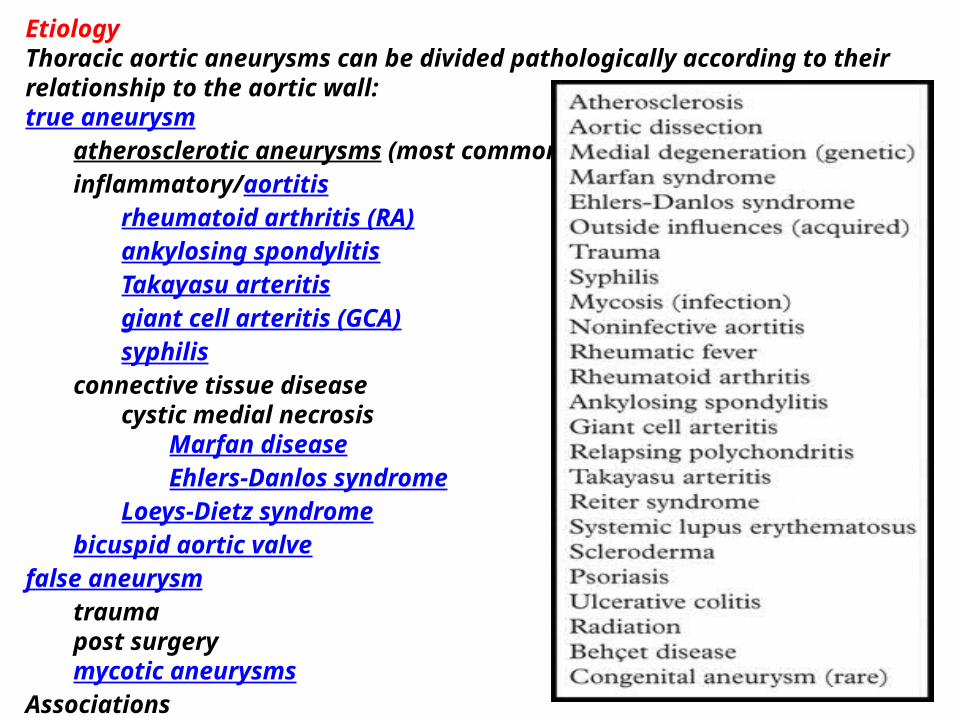
EtiologyThoracic aortic aneurysms can be divided pathologically according to their relationship to the aortic wall:true aneurysm
atherosclerotic aneurysms (most common)inflammatory/aortitis
rheumatoid arthritis (RA)ankylosing spondylitisTakayasu arteritisgiant cell arteritis (GCA)syphilis
connective tissue diseasecystic medial necrosis
Marfan diseaseEhlers-Danlos syndrome
Loeys-Dietz syndromebicuspid aortic valve
false aneurysmtraumapost surgerymycotic aneurysms
Associationsintracranial cerebral aneurysms (~10% prevalence).
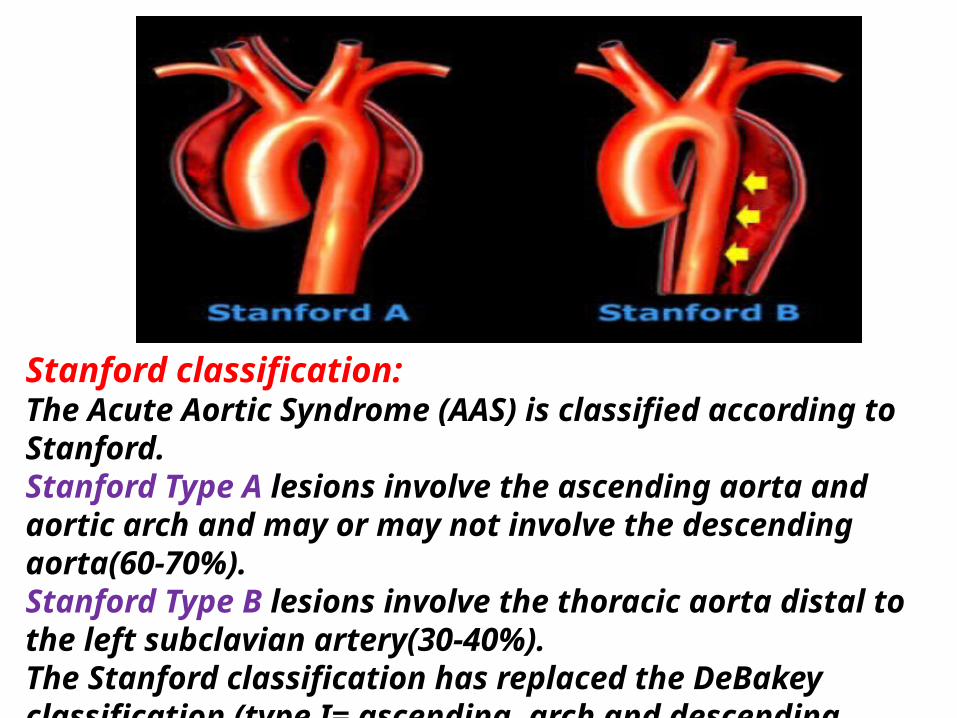
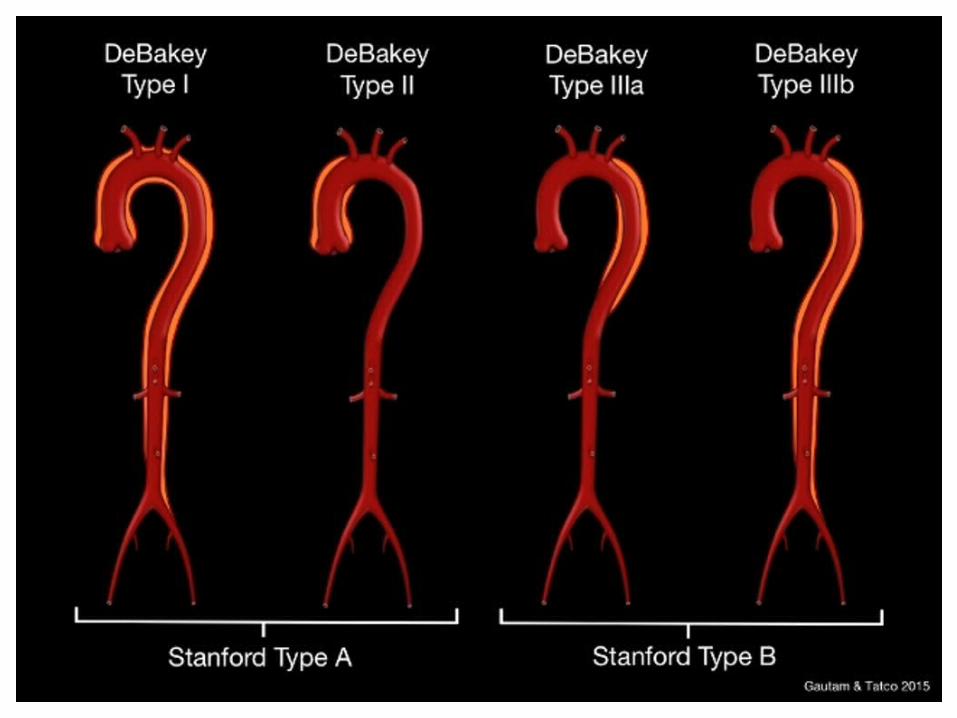
Stanford classification:The Acute Aortic Syndrome (AAS) is classified according to Stanford.Stanford Type A lesions involve the ascending aorta and aortic arch and may or may not involve the descending aorta(60-70%). Stanford Type B lesions involve the thoracic aorta distal to the left subclavian artery(30-40%).The Stanford classification has replaced the DeBakey classification (type I= ascending, arch and descending aorta: type II= only ascending aorta: type III= only descending aorta).
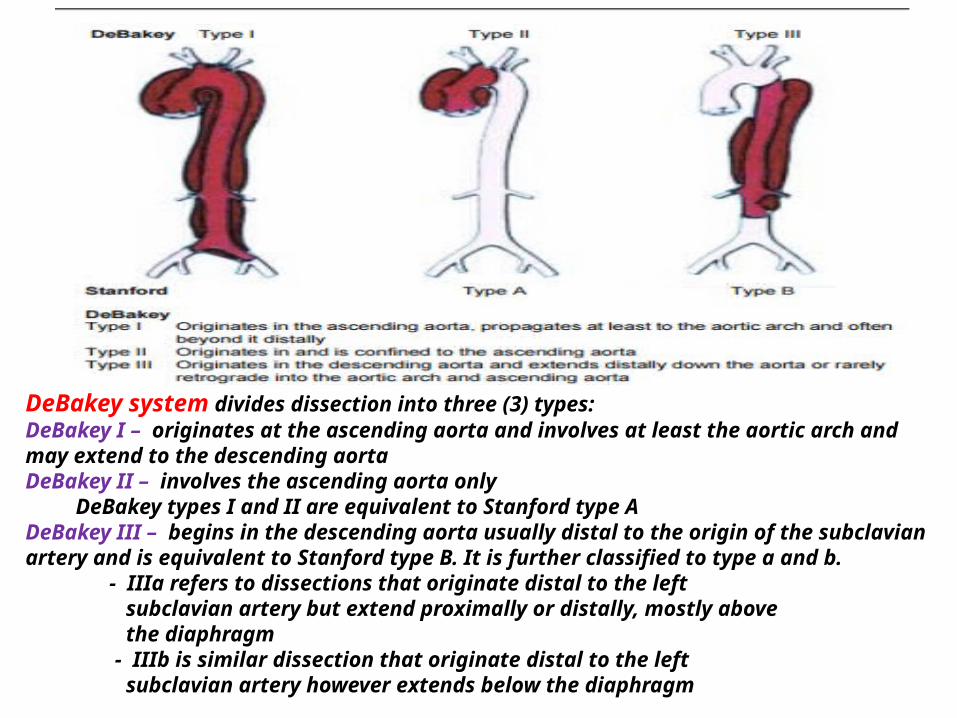
DeBakey system divides dissection into three (3) types:DeBakey I – originates at the ascending aorta and involves at least the aortic arch and may extend to the descending aortaDeBakey II – involves the ascending aorta only DeBakey types I and II are equivalent to Stanford type ADeBakey III – begins in the descending aorta usually distal to the origin of the subclavian artery and is equivalent to Stanford type B. It is further classified to type a and b. - IIIa refers to dissections that originate distal to the left subclavian artery but extend proximally or distally, mostly above the diaphragm - IIIb is similar dissection that originate distal to the left subclavian artery however extends below the diaphragm
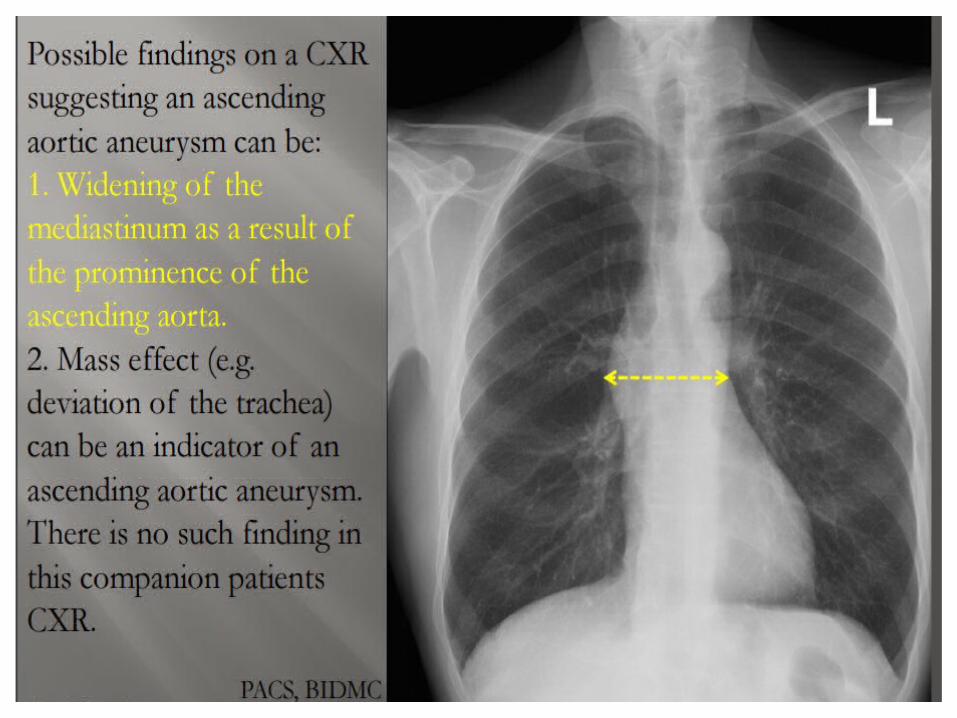
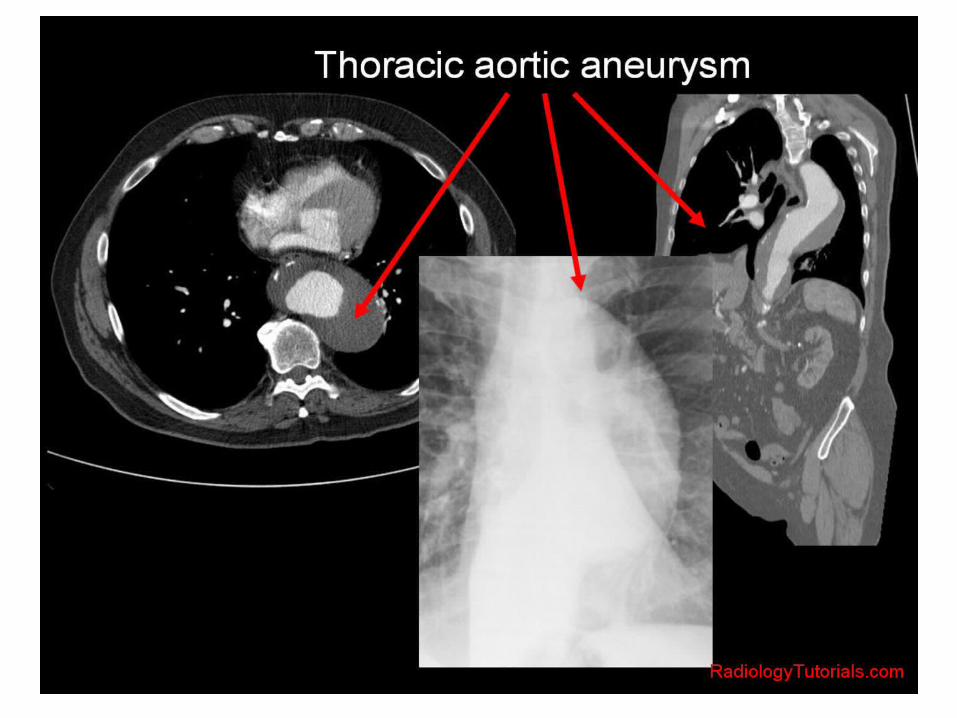
Radiographic featuresThe location and shape of thoracic aortic aneurysms are variable. An aortic aneurysm, as aneurysms elsewhere, can be described as saccular or fusiform. In the case of fusiform dilatation, the term aneurysm should be applied when the diameter is >4 cm.Plain radiographThe thoracic aorta can usually be seen on both frontal and lateral chest radiographs, and aneurysms are often obvious. However, it is difficult to assess size accurately (due to magnification effects and often poor visualization on the side of the artery).Additionally, mediastinal masses may mimic aortic aneurysms.Mural calcification is seen both in atherosclerotic disease as well as various causes of aortitis.UltrasoundUnlike abdominal aneurysms that can usually be readily assessed and monitored with ultrasound, thoracic aortic aneurysms are encased in bone and air making transthoracic ultrasound of no use.Transoesophageal echocardiography can visualize much of the descending aorta, but due to its invasive nature is not routinely used.
CTCTA is the work-horse of aneurysm assessment able to rapidly image the relevant vascular territory with high resolution. It can visualise both the sac and the lumen and detect potential complications.Typically aneurysms appear as dilatations of the lumen. The walls may be thin or thickened by the presence of a mural thrombus (circumferential or more frequently eccentric).Calcified atherosclerotic disease is often identified not only in the wall of an aneurysm but adjacent arteries.If rupture or leak has occurred hematoma/fluid may be seen adjacent to the aorta, in the left pleural cavity or the pericardium.See main article: reporting tips for aortic aneurysms.MRIMRI has the advantage of not requiring ionizing radiation or large volumes of iodinated contrast 2. This is particularly advantageous in young patients with connective tissue disorders. However, there are limitations in patients with pacemakers, and those with reduced renal function (see nephrogenic systemic fibrosis)Acquisitions capable of being reformatted in three dimensions are essential to allow for accurate luminal measurement.Digital subtraction angiography (DSA)Although angiography has long been considered the gold standard for vascular imaging, it has largely been superseded by CTA and MRA, which can obtain 3D volumetric data, and able to assess the extraluminal soft tissues.Angiography is however used during endovascular repair.
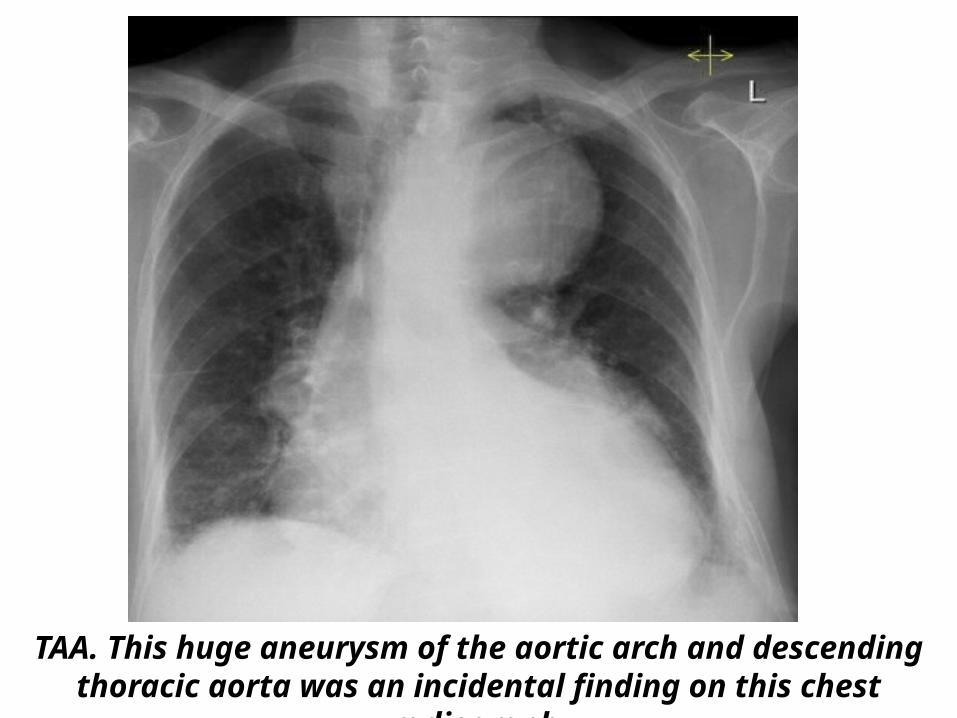
TAA. This huge aneurysm of the aortic arch and descending thoracic aorta was an incidental finding on this chest radiograph
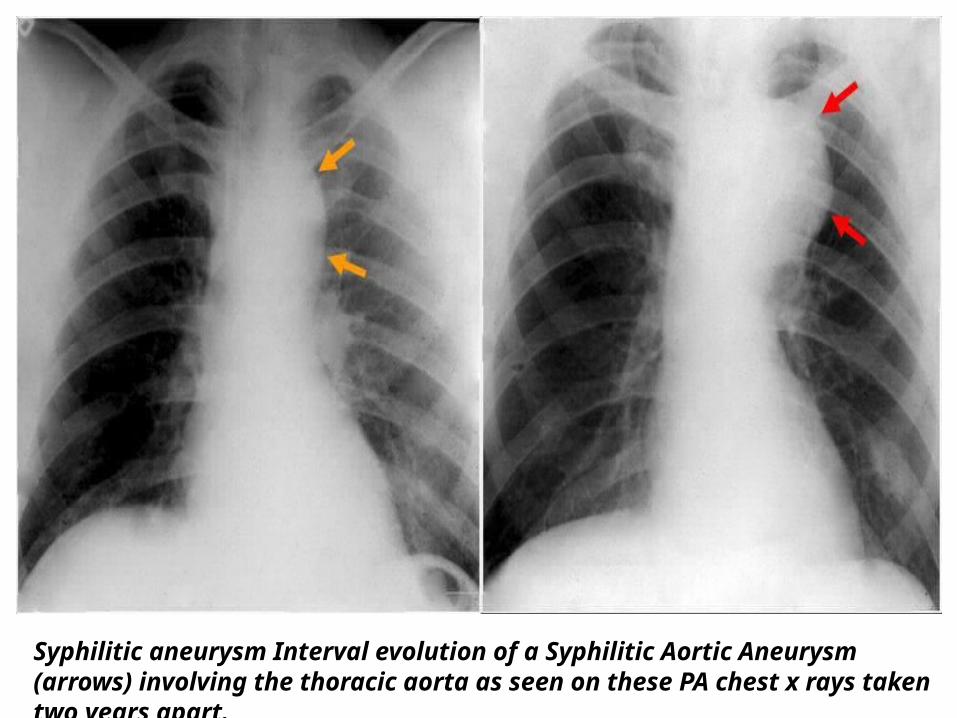
Syphilitic aneurysm Interval evolution of a Syphilitic Aortic Aneurysm (arrows) involving the thoracic aorta as seen on these PA chest x rays taken two years apart.
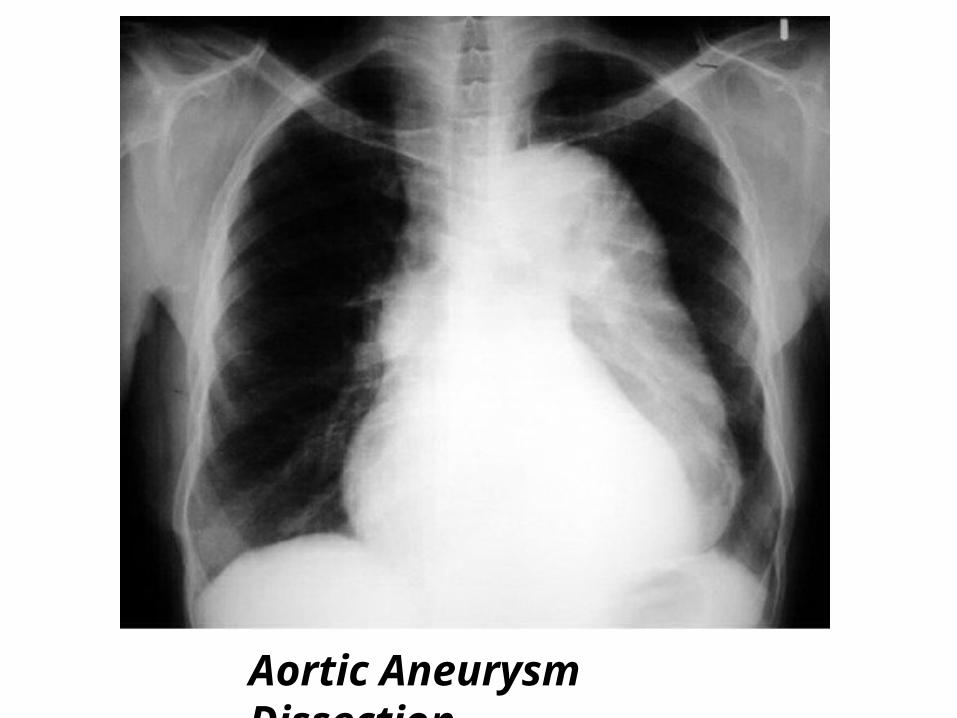
Aortic Aneurysm Dissection.
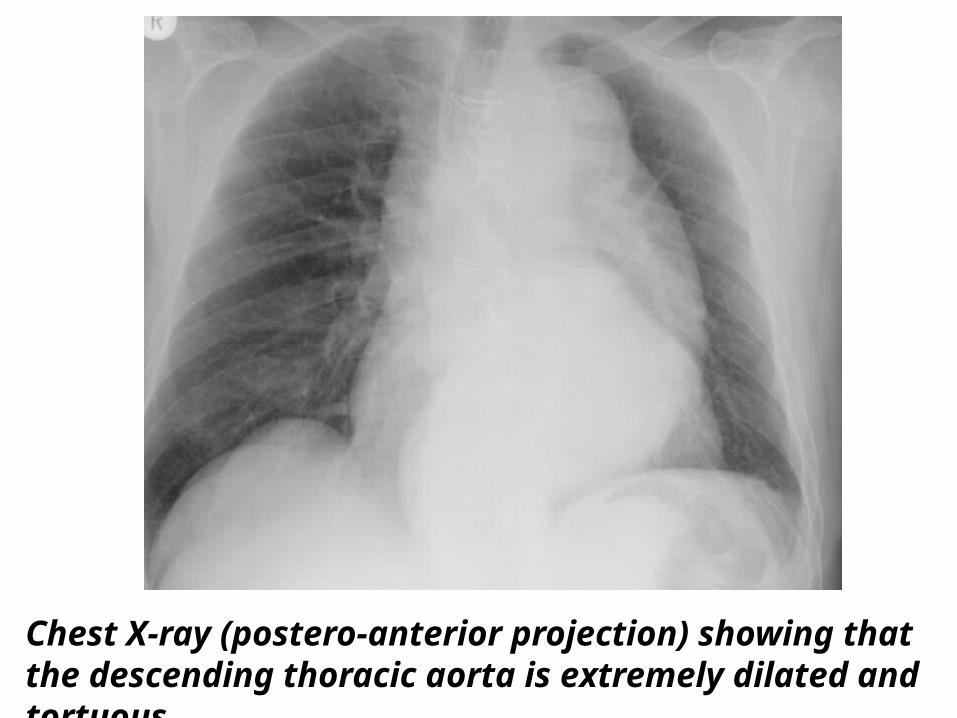
Chest X-ray (postero-anterior projection) showing that the descending thoracic aorta is extremely dilated and tortuous.
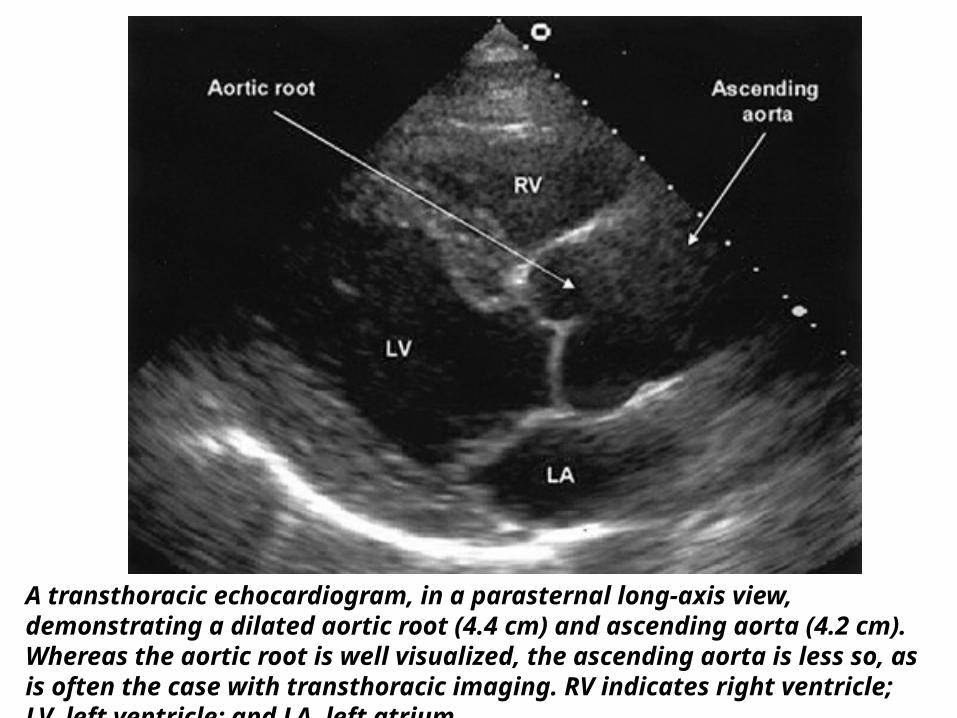
A transthoracic echocardiogram, in a parasternal long-axis view, demonstrating a dilated aortic root (4.4 cm) and ascending aorta (4.2 cm). Whereas the aortic root is well visualized, the ascending aorta is less so, as is often the case with transthoracic imaging. RV indicates right ventricle; LV, left ventricle; and LA, left atrium.
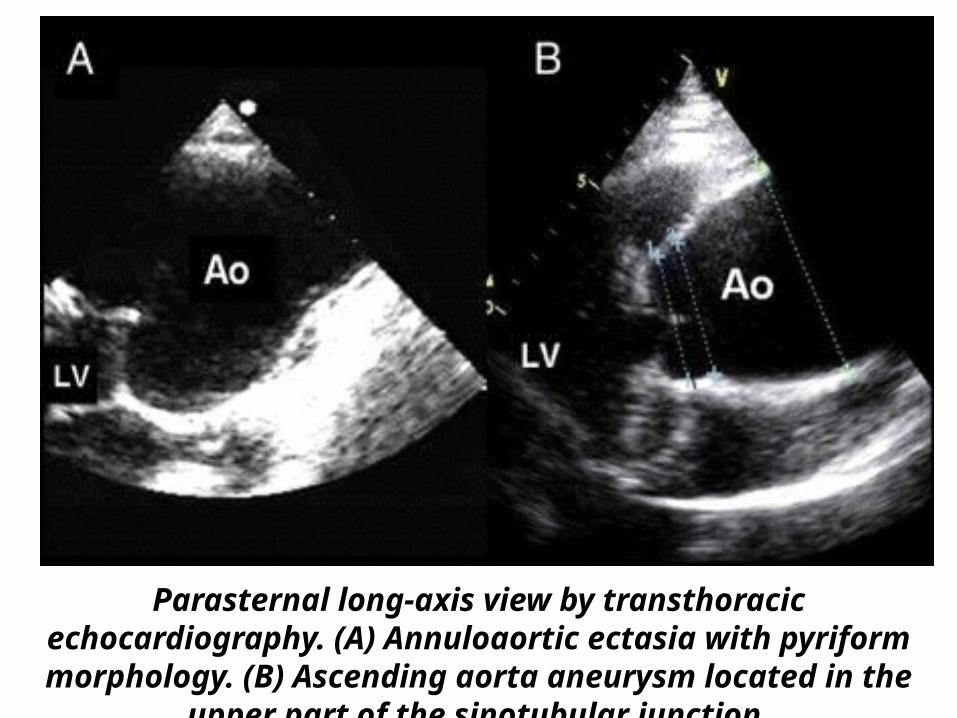
Parasternal long-axis view by transthoracic echocardiography. (A) Annuloaortic ectasia with pyriform morphology. (B) Ascending aorta
aneurysm located in the upper part of the sinotubular junction.
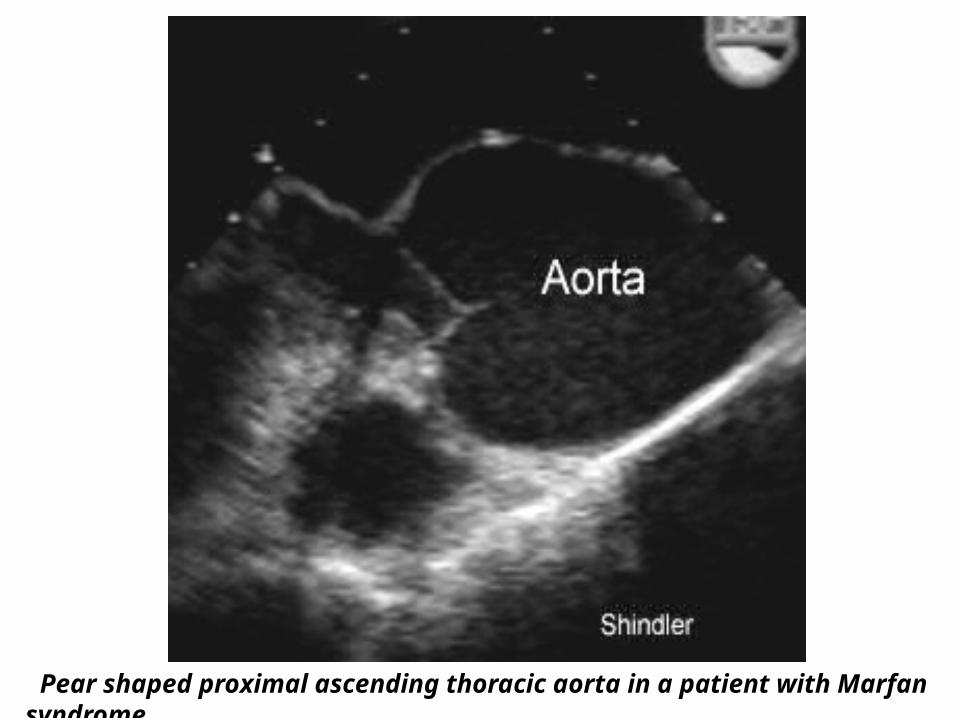
Pear shaped proximal ascending thoracic aorta in a patient with Marfan syndrome.
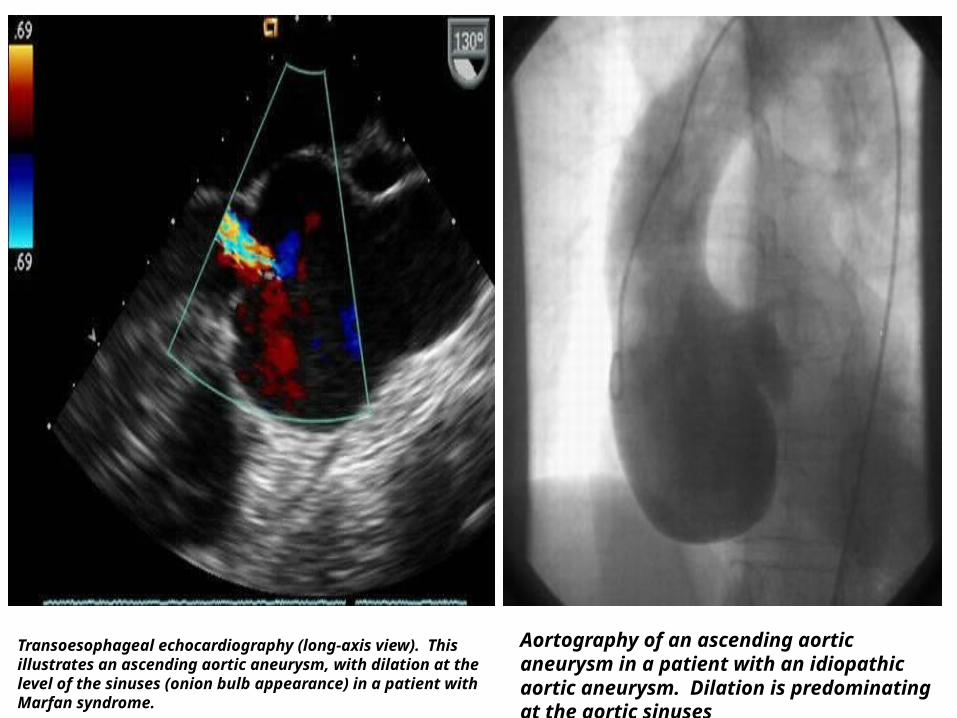
Transoesophageal echocardiography (long-axis view). This illustrates an ascending aortic aneurysm, with dilation at the level of the sinuses (onion bulb appearance) in a patient with Marfan syndrome.
Aortography of an ascending aortic aneurysm in a patient with an idiopathic aortic aneurysm. Dilation is predominating at the aortic sinuses
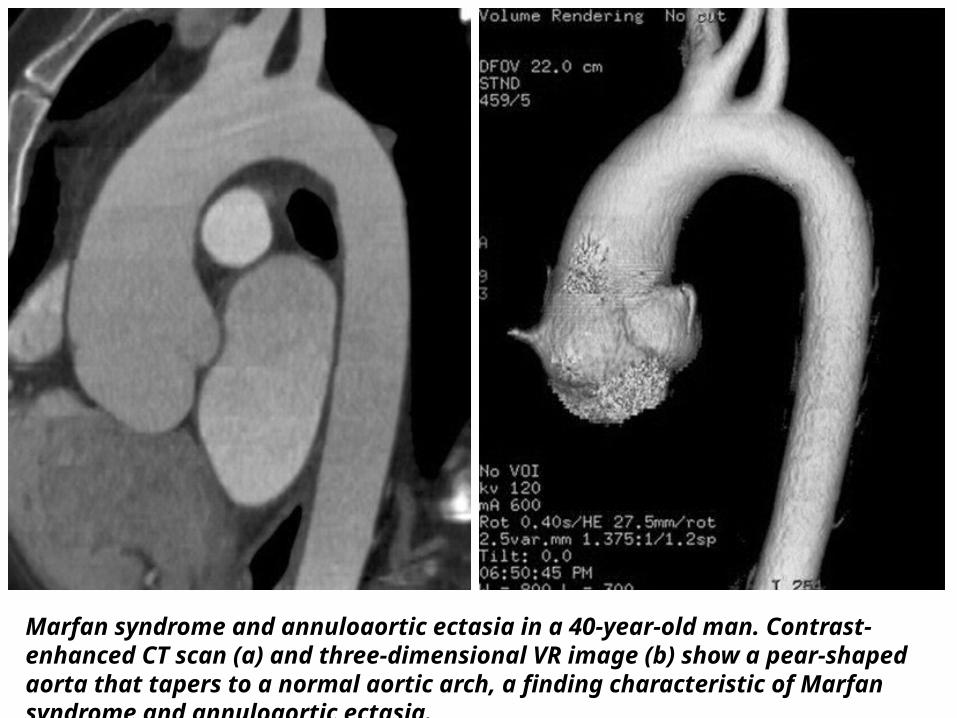
Marfan syndrome and annuloaortic ectasia in a 40-year-old man. Contrast-enhanced CT scan (a) and three-dimensional VR image (b) show a pear-shaped aorta that tapers to a normal aortic arch, a finding characteristic of Marfan syndrome and annuloaortic ectasia.
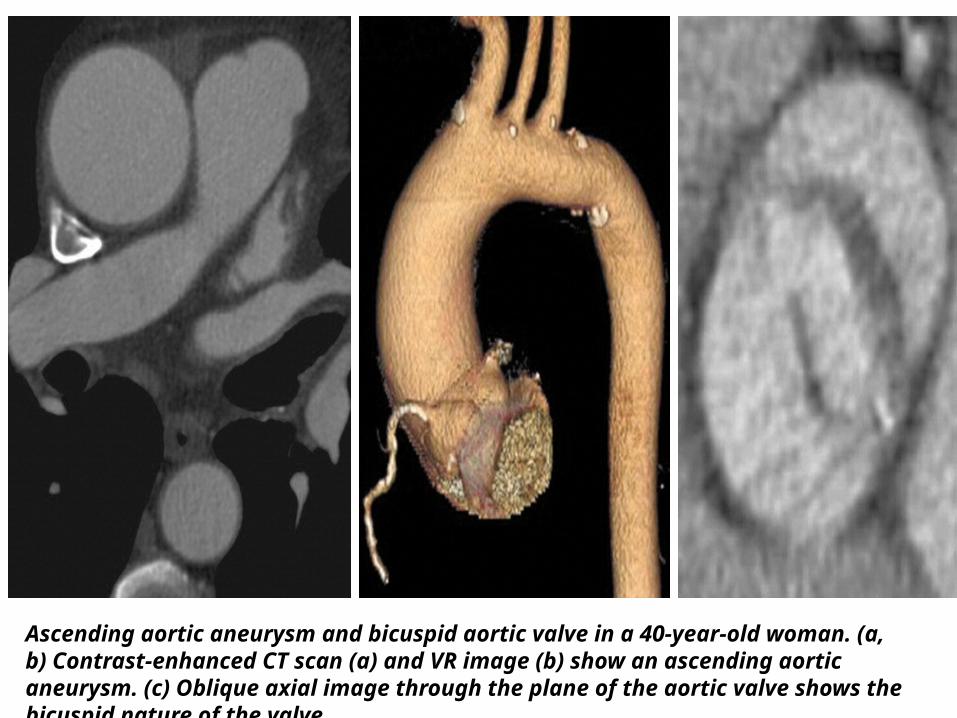
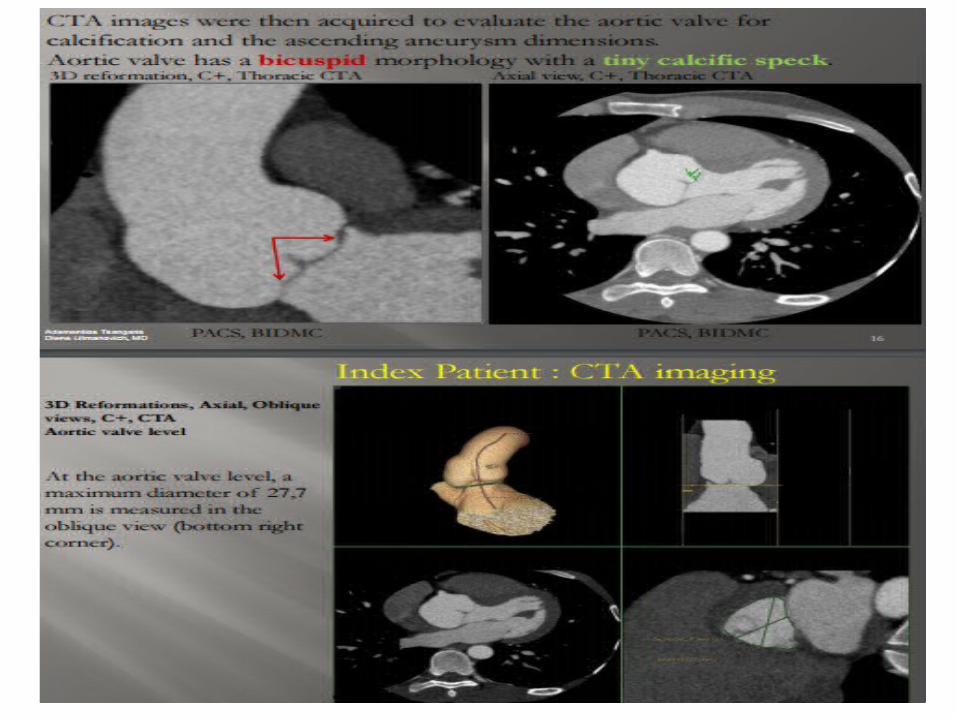
Ascending aortic aneurysm and bicuspid aortic valve in a 40-year-old woman. (a, b) Contrast-enhanced CT scan (a) and VR image (b) show an ascending aortic aneurysm. (c) Oblique axial image through the plane of the aortic valve shows the bicuspid nature of the valve.
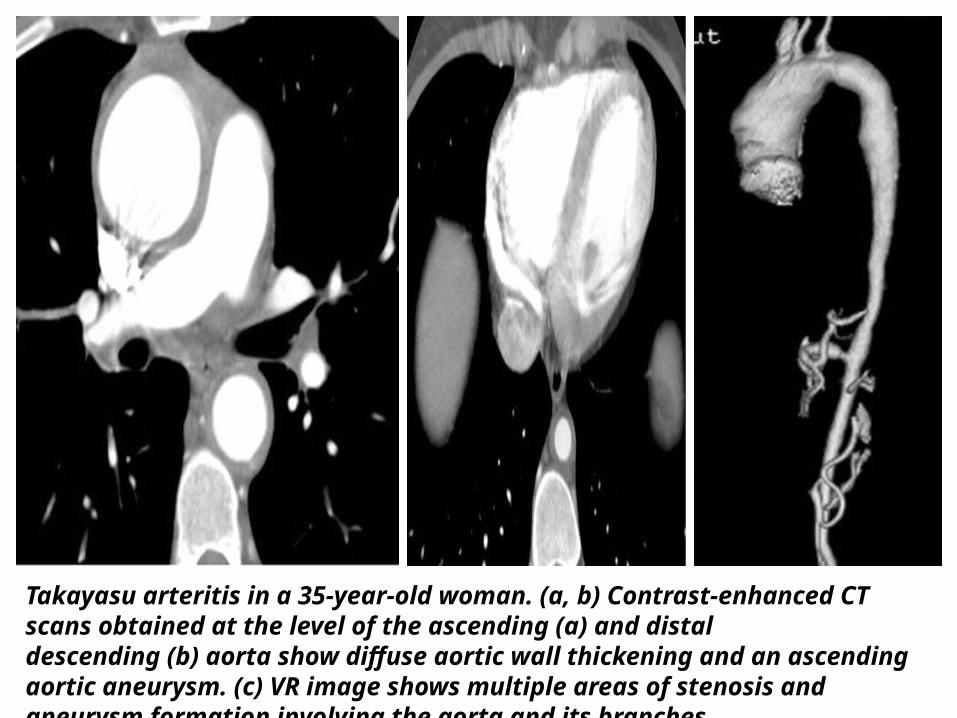
Takayasu arteritis in a 35-year-old woman. (a, b) Contrast-enhanced CT scans obtained at the level of the ascending (a) and distal descending (b) aorta show diffuse aortic wall thickening and an ascending aortic aneurysm. (c) VR image shows multiple areas of stenosis and aneurysm formation involving the aorta and its branches.
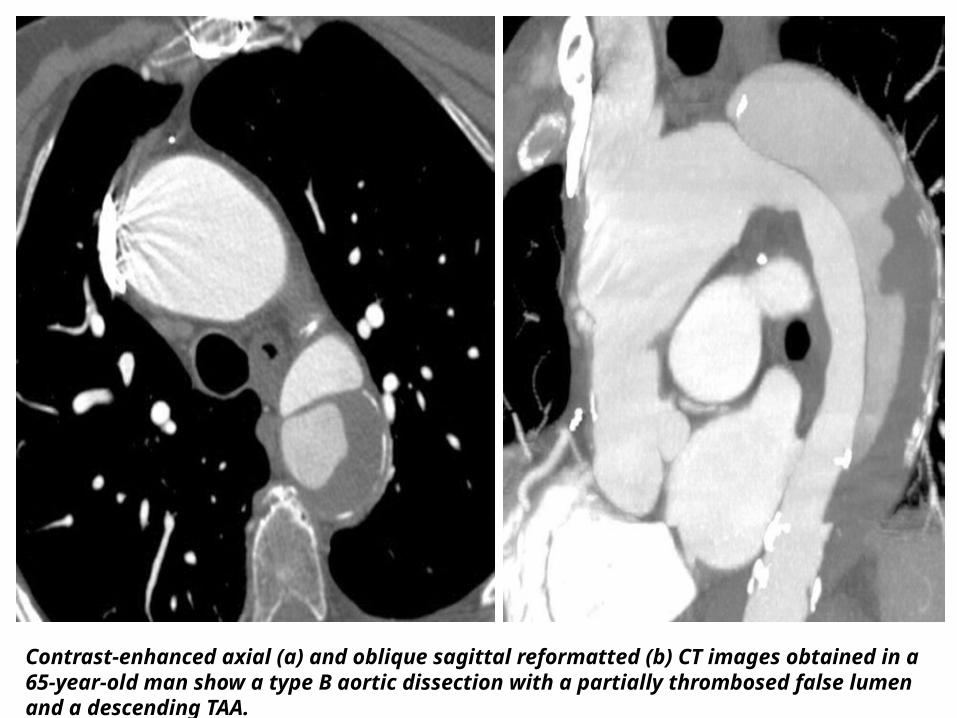
Contrast-enhanced axial (a) and oblique sagittal reformatted (b) CT images obtained in a 65-year-old man show a type B aortic dissection with a partially thrombosed false lumen and a descending TAA.
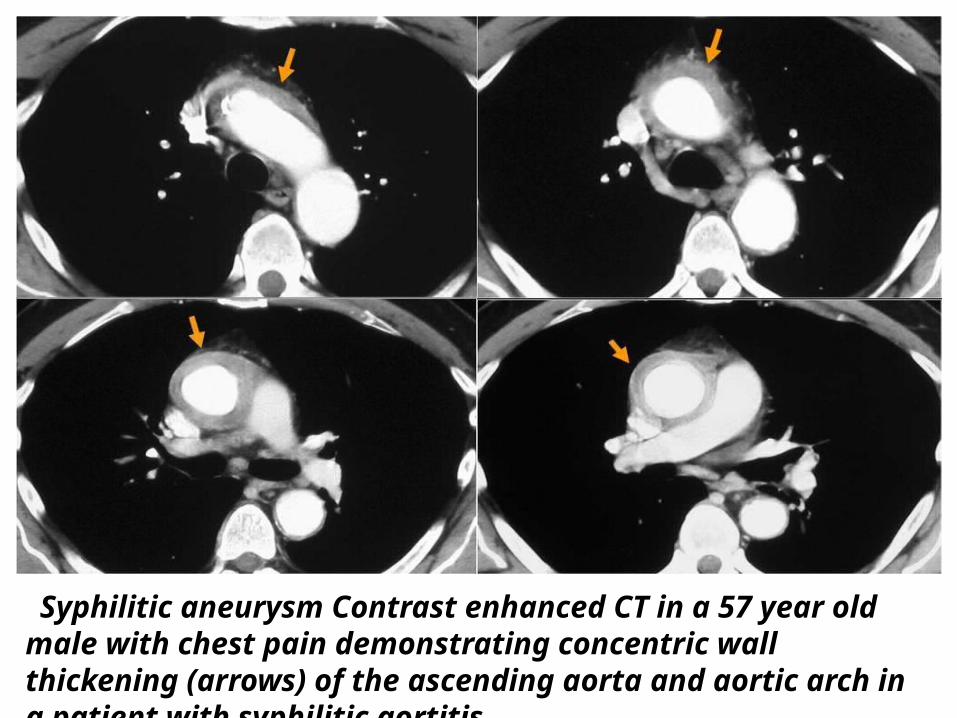
Syphilitic aneurysm Contrast enhanced CT in a 57 year old male with chest pain demonstrating concentric wall thickening (arrows) of the ascending aorta and aortic arch in a patient with syphilitic aortitis.
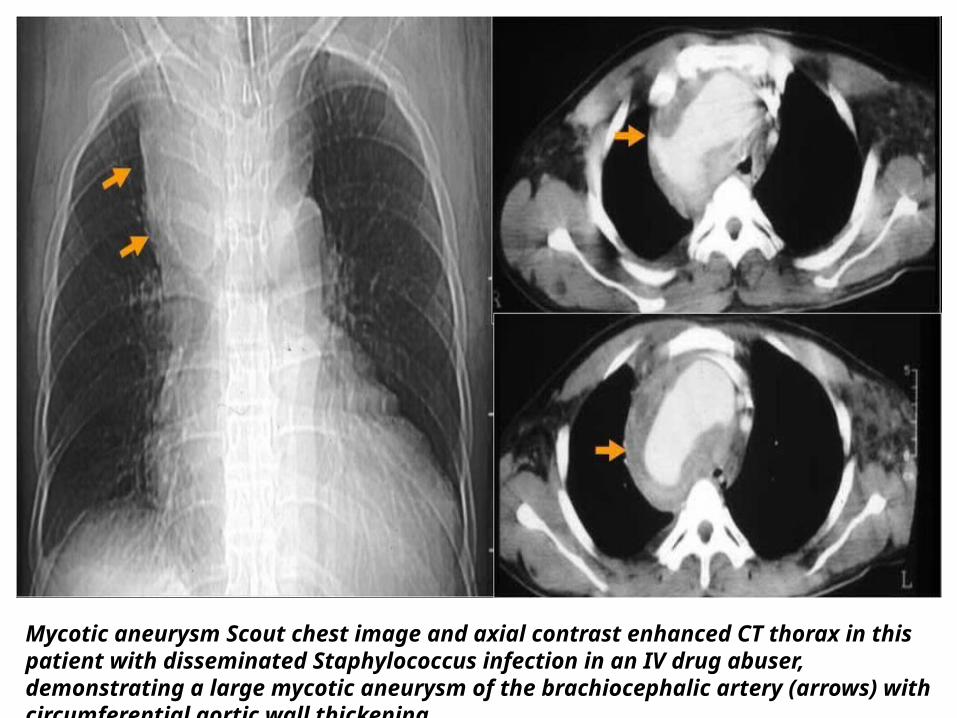
Mycotic aneurysm Scout chest image and axial contrast enhanced CT thorax in this patient with disseminated Staphylococcus infection in an IV drug abuser, demonstrating a large mycotic aneurysm of the brachiocephalic artery (arrows) with circumferential aortic wall thickening.
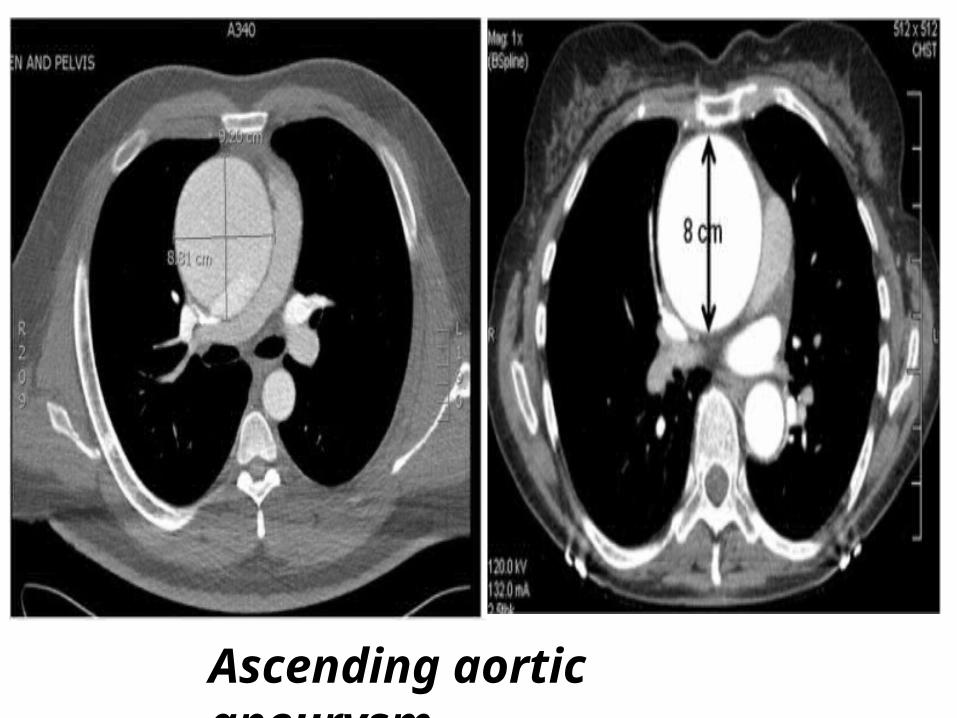
Ascending aortic aneurysm.
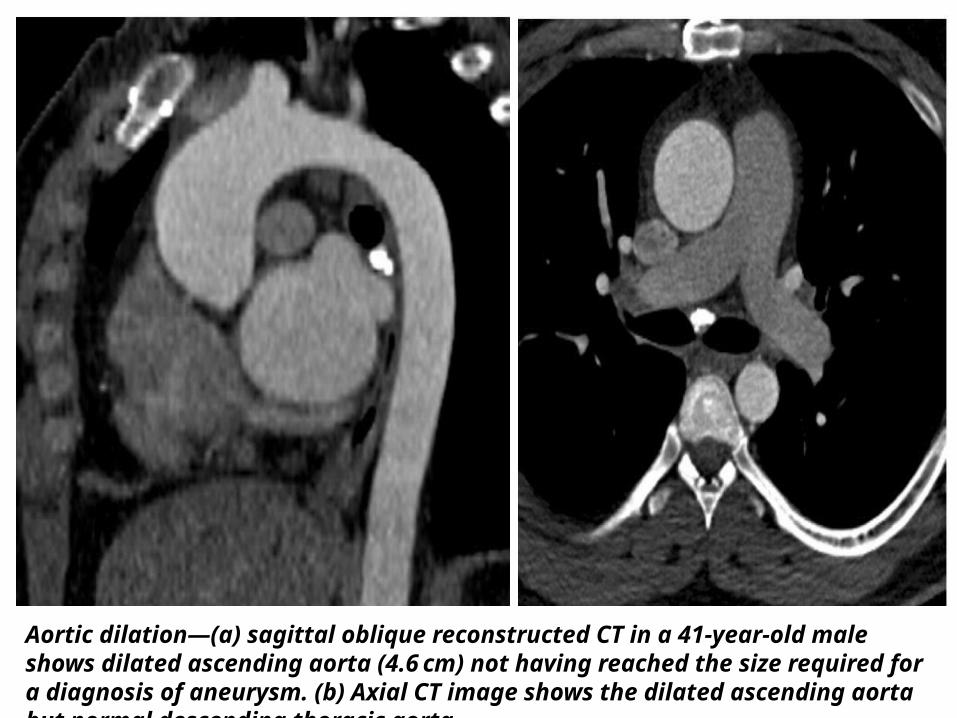
Aortic dilation—(a) sagittal oblique reconstructed CT in a 41-year-old male shows dilated ascending aorta (4.6 cm) not having reached the size required for a diagnosis of aneurysm. (b) Axial CT image shows the dilated ascending aorta but normal descending thoracic aorta.
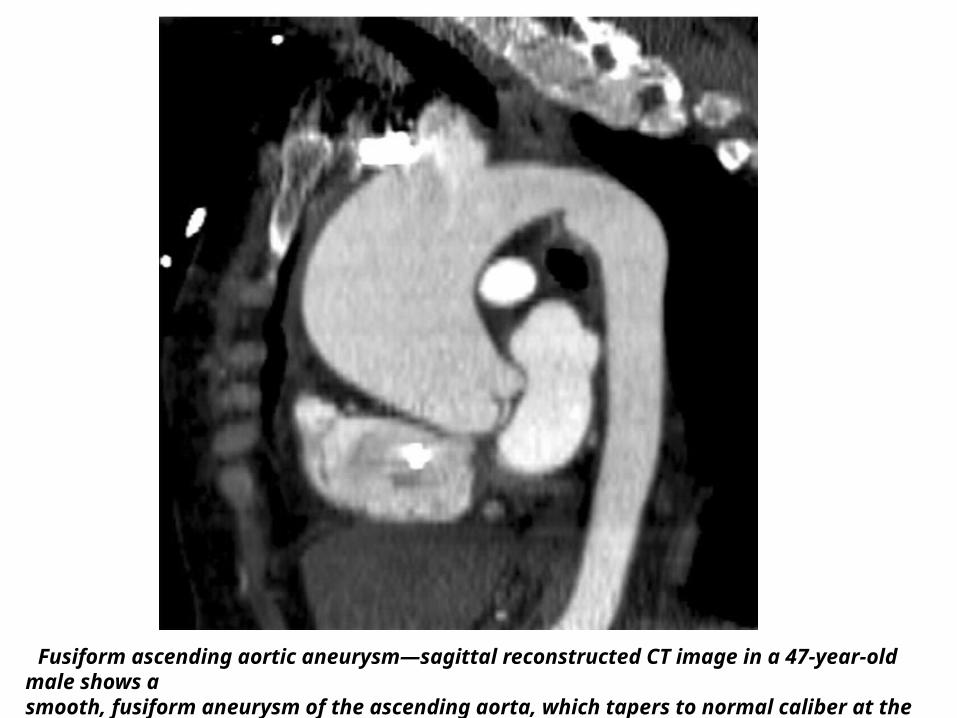
Fusiform ascending aortic aneurysm—sagittal reconstructed CT image in a 47-year-old male shows a smooth, fusiform aneurysm of the ascending aorta, which tapers to normal caliber at the proximal arch.
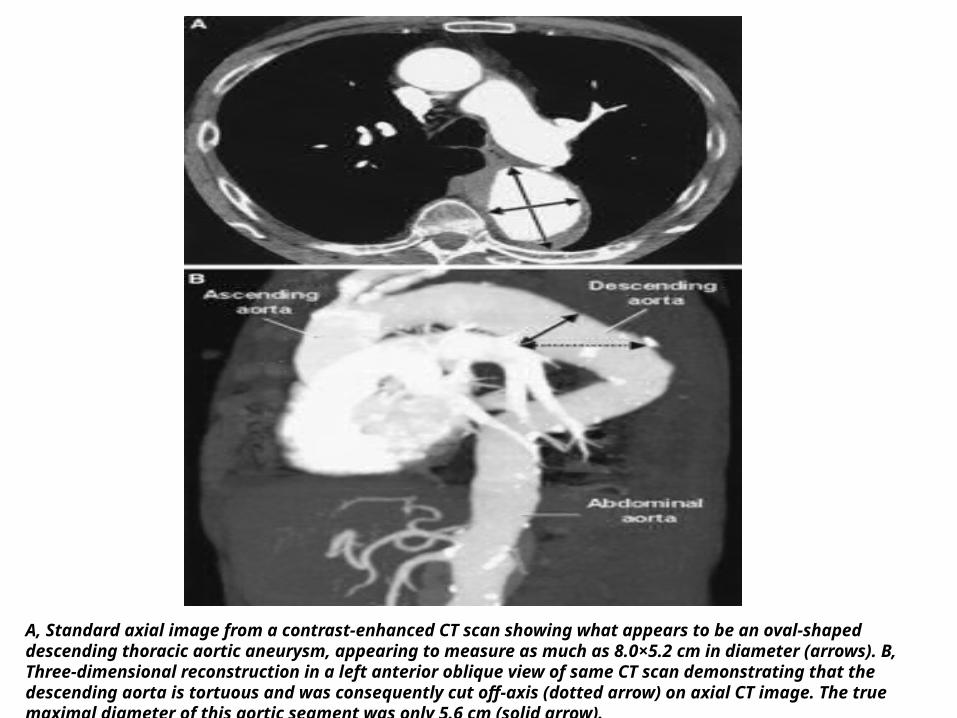
A, Standard axial image from a contrast-enhanced CT scan showing what appears to be an oval-shaped descending thoracic aortic aneurysm, appearing to measure as much as 8.0×5.2 cm in diameter (arrows). B, Three-dimensional reconstruction in a left anterior oblique view of same CT scan demonstrating that the descending aorta is tortuous and was consequently cut off-axis (dotted arrow) on axial CT image. The true maximal diameter of this aortic segment was only 5.6 cm (solid arrow).
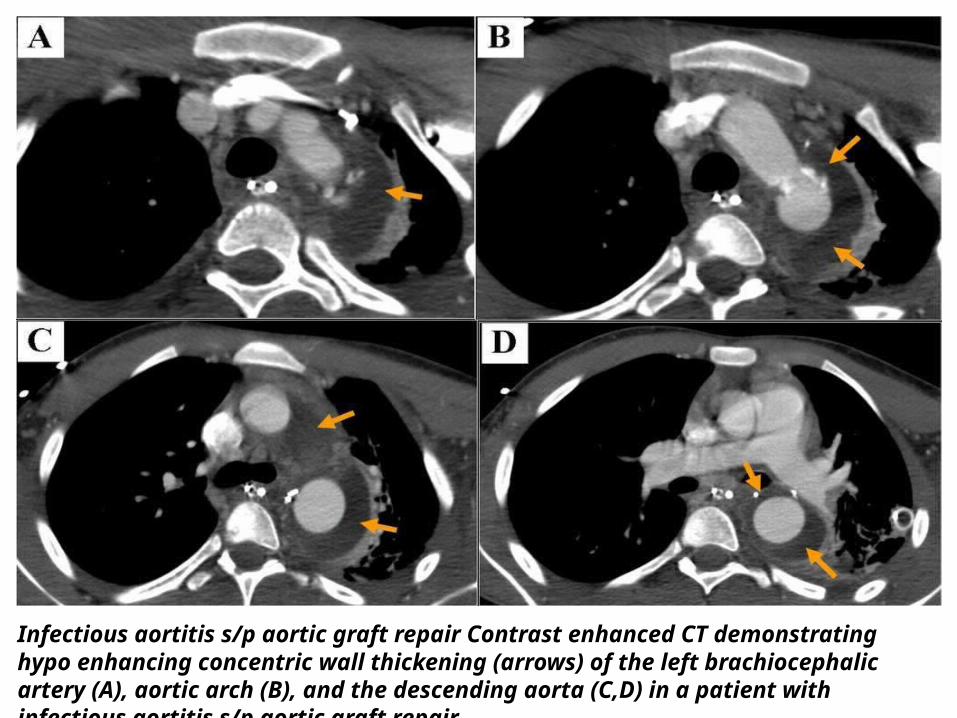
Infectious aortitis s/p aortic graft repair Contrast enhanced CT demonstrating hypo enhancing concentric wall thickening (arrows) of the left brachiocephalic artery (A), aortic arch (B), and the descending aorta (C,D) in a patient with infectious aortitis s/p aortic graft repair
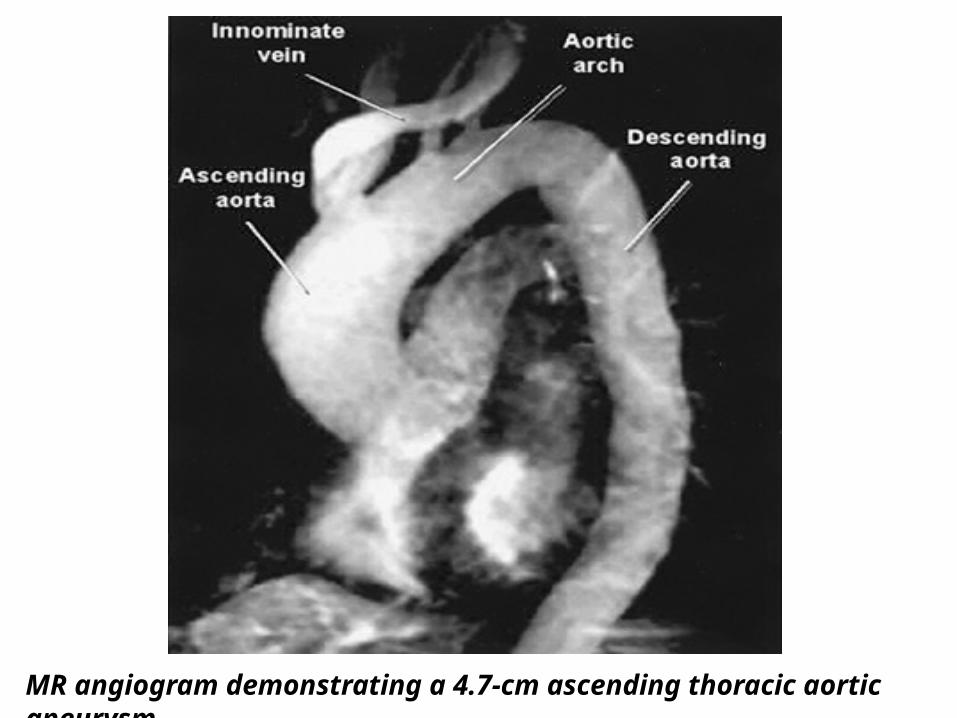
MR angiogram demonstrating a 4.7-cm ascending thoracic aortic aneurysm.
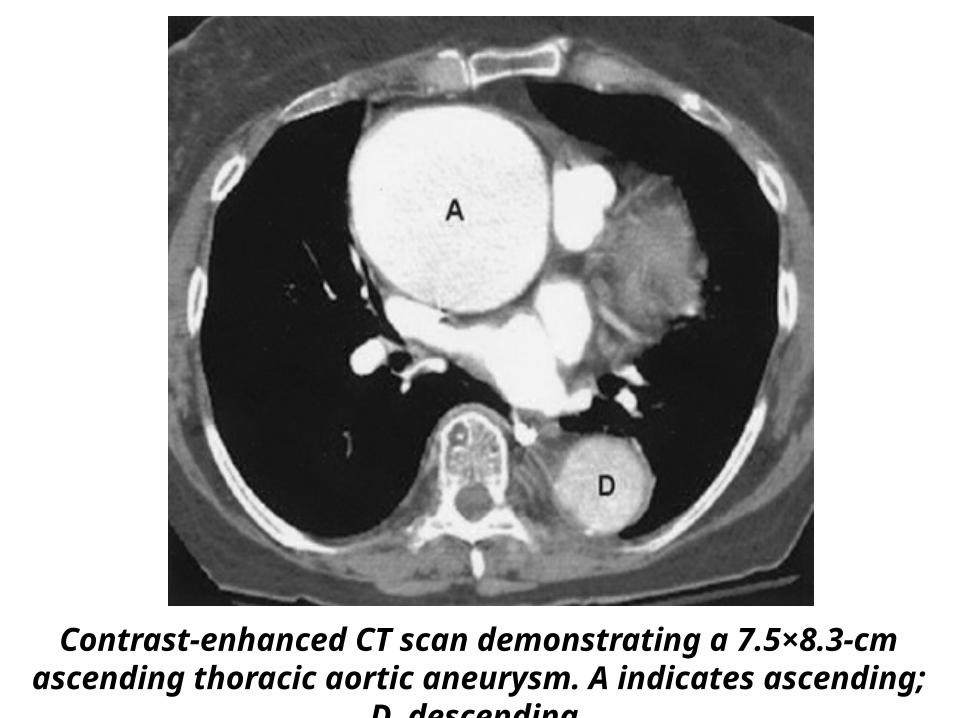
Contrast-enhanced CT scan demonstrating a 7.5×8.3-cm ascending thoracic aortic aneurysm. A indicates ascending; D, descending.
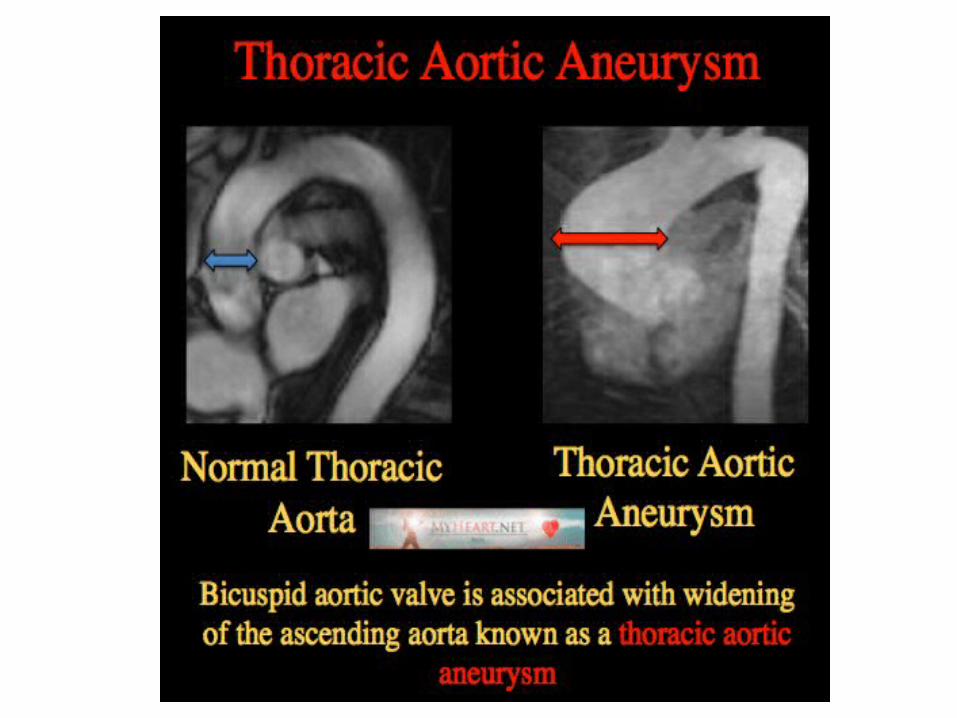
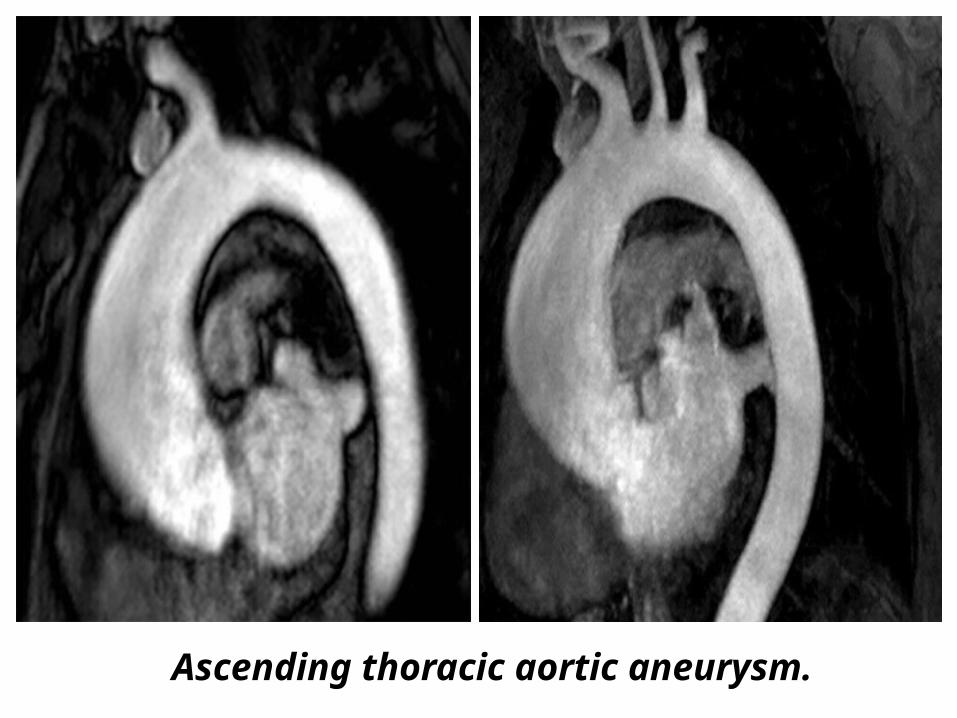
Ascending thoracic aortic aneurysm.
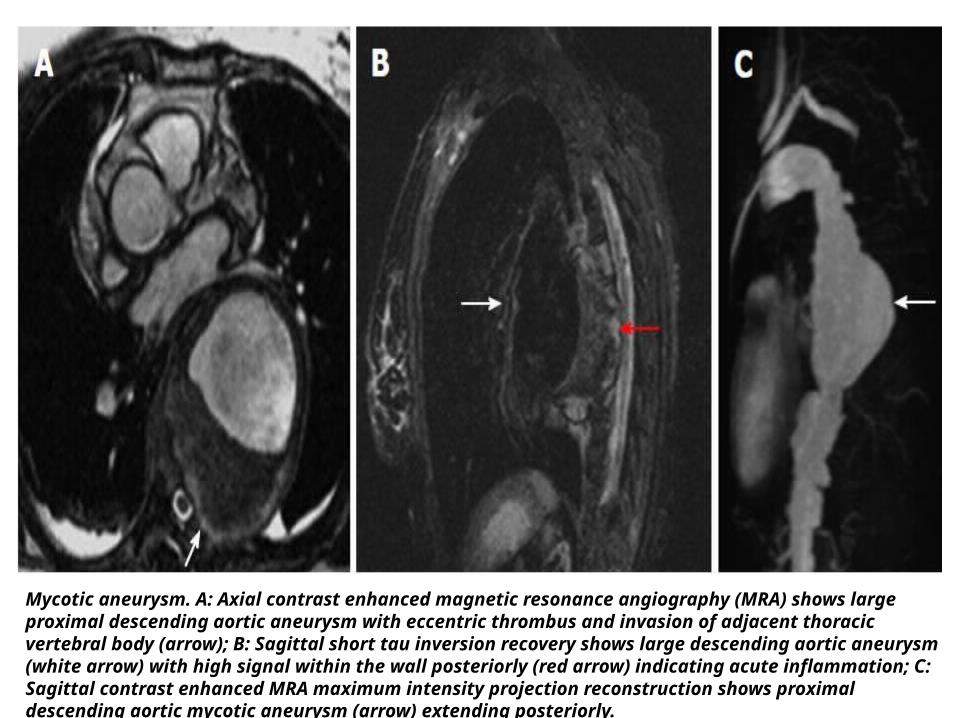
Mycotic aneurysm. A: Axial contrast enhanced magnetic resonance angiography (MRA) shows large proximal descending aortic aneurysm with eccentric thrombus and invasion of adjacent thoracic vertebral body (arrow); B: Sagittal short tau inversion recovery shows large descending aortic aneurysm (white arrow) with high signal within the wall posteriorly (red arrow) indicating acute inflammation; C: Sagittal contrast enhanced MRA maximum intensity projection reconstruction shows proximal descending aortic mycotic aneurysm (arrow) extending posteriorly.
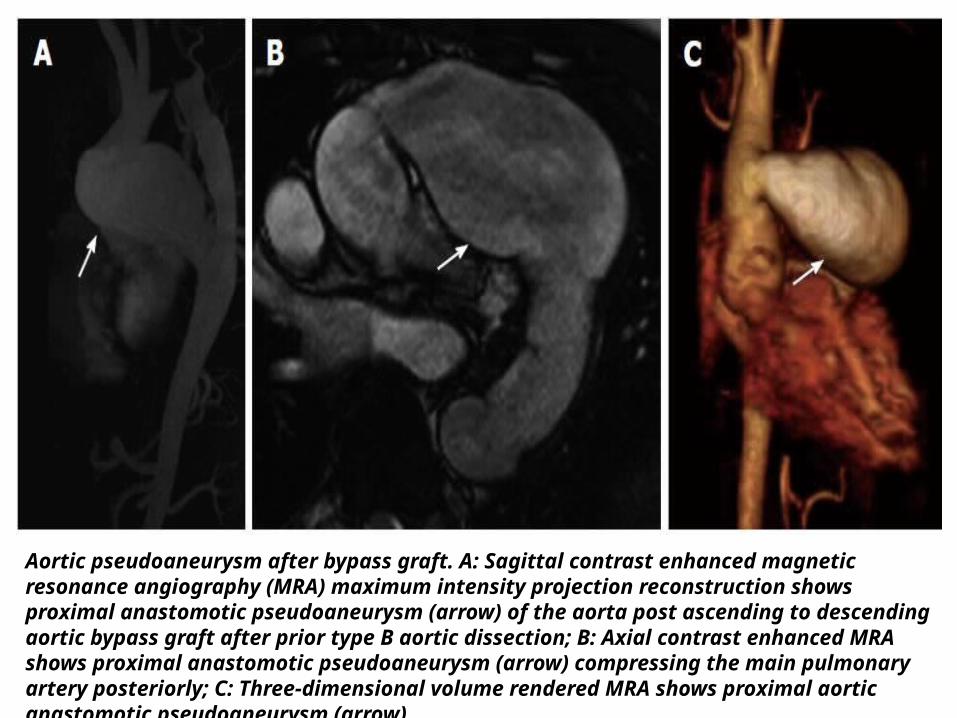
Aortic pseudoaneurysm after bypass graft. A: Sagittal contrast enhanced magnetic resonance angiography (MRA) maximum intensity projection reconstruction shows proximal anastomotic pseudoaneurysm (arrow) of the aorta post ascending to descending aortic bypass graft after prior type B aortic dissection; B: Axial contrast enhanced MRA shows proximal anastomotic pseudoaneurysm (arrow) compressing the main pulmonary artery posteriorly; C: Three-dimensional volume rendered MRA shows proximal aortic anastomotic pseudoaneurysm (arrow).
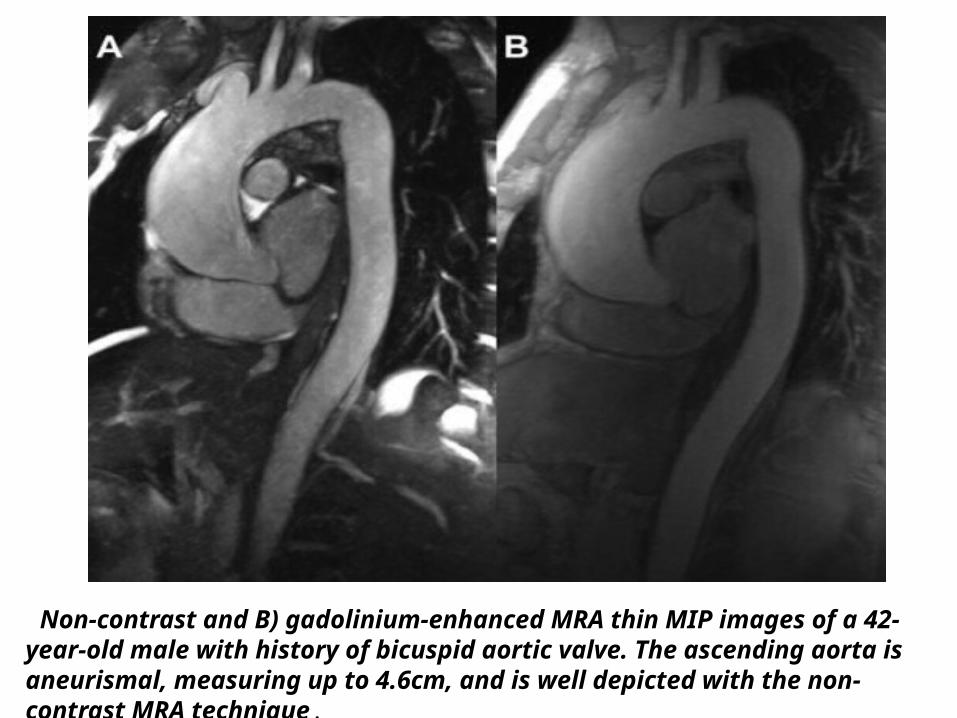
Non-contrast and B) gadolinium-enhanced MRA thin MIP images of a 42-year-old male with history of bicuspid aortic valve. The ascending aorta is aneurismal, measuring up to 4.6cm, and is well depicted with the non-contrast MRA technique.
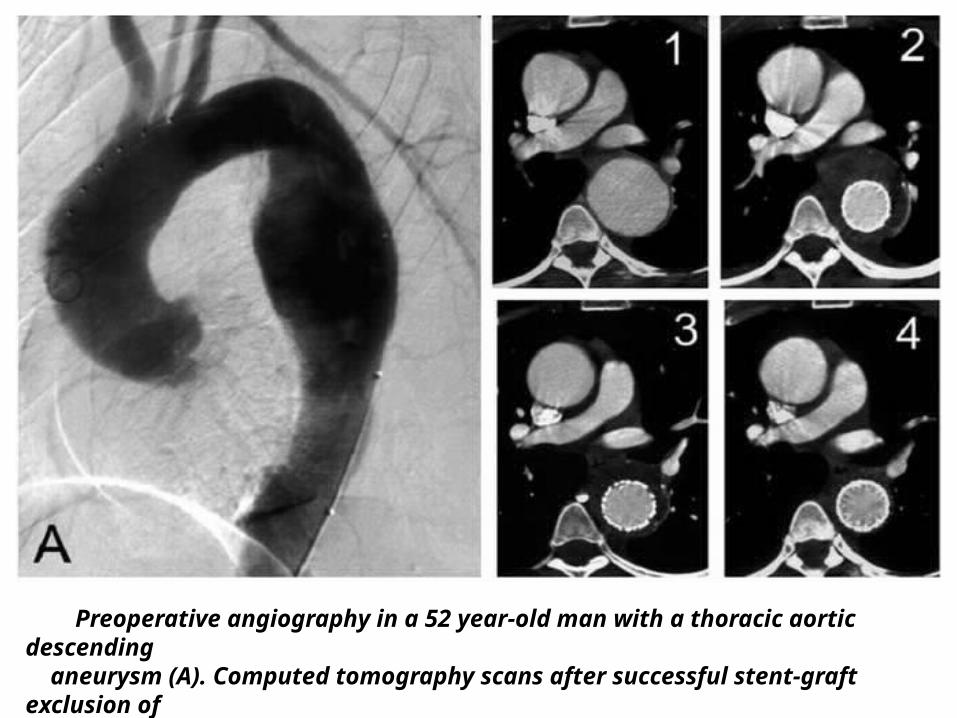
Preoperative angiography in a 52 year-old man with a thoracic aortic descending aneurysm (A). Computed tomography scans after successful stent-graft exclusion of the aneurysm demonstrate continued shrinkage of the periprothetic thrombus mass (1-4).
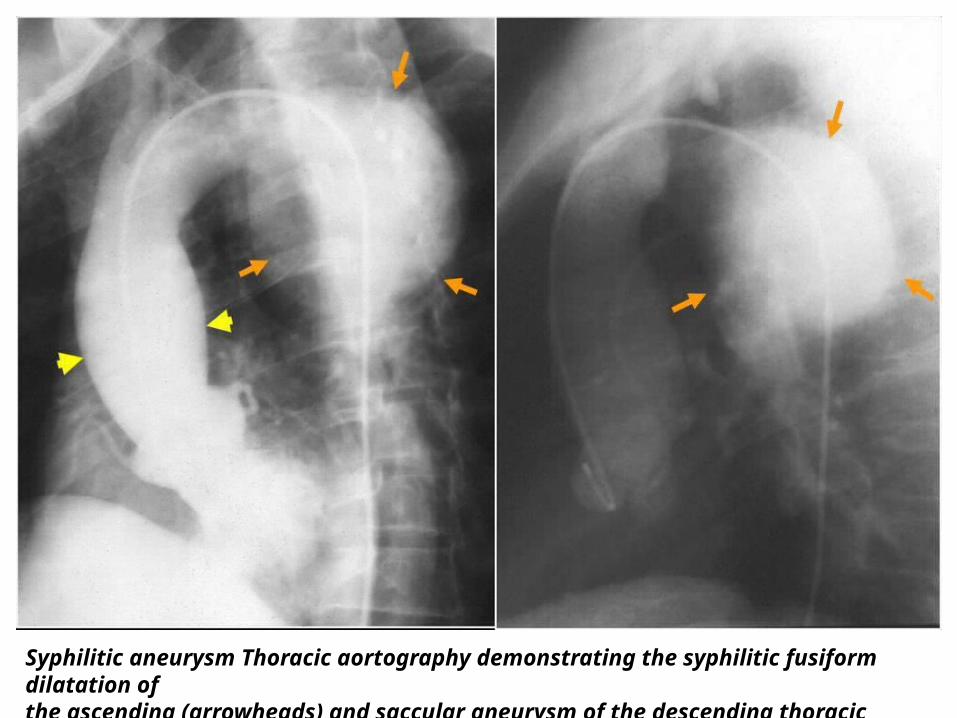
Syphilitic aneurysm Thoracic aortography demonstrating the syphilitic fusiform dilatation of the ascending (arrowheads) and saccular aneurysm of the descending thoracic aorta (arrows).
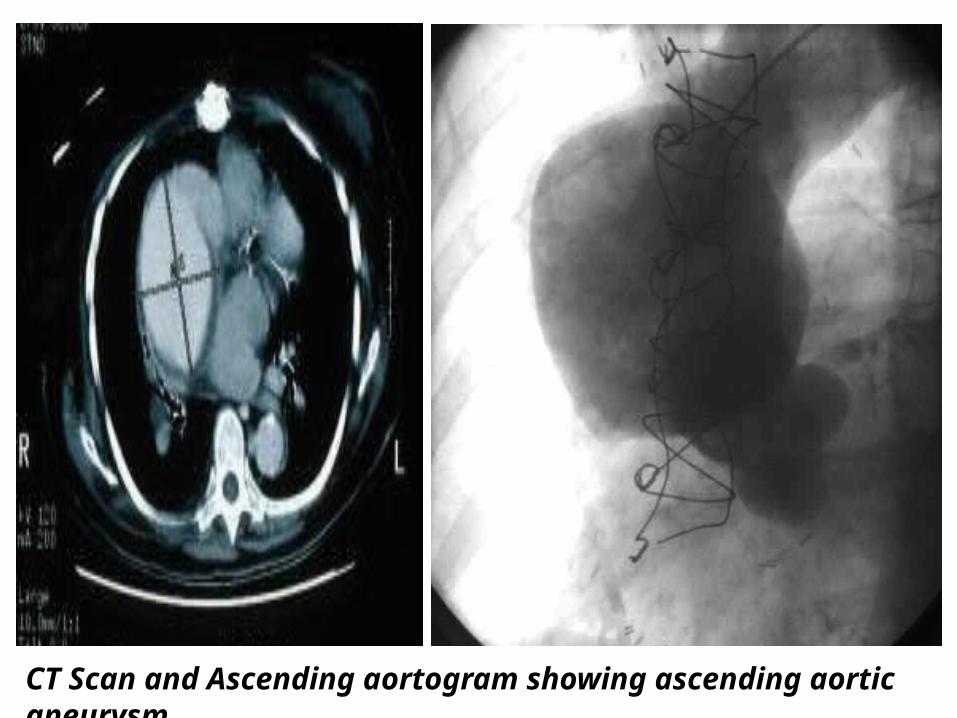
CT Scan and Ascending aortogram showing ascending aortic aneurysm.
Thank You.