Embed Size (px)
DESCRIPTION
Target: UG medical students.
Citation preview
Pulmonary Hypertension
Dr.CSBR.Prasad, M.D.
CSBRP-Dec-2012
Pulmonary Hypertension
Pulmonary BP is only ⅛ of systemic BP
Def: Mean pulmonary arterial pressure
exceeding ¼ of systemic levels is PHT
CSBRP-Dec-2012
Pulmonary Hypertension
Classification:
Primary: Idiopathic, no known cause,
6% - have family history (AD)
Secondary: Structural abnormalities in
cardiopulmonary area
CSBRP-Dec-2012
Pulmonary Hypertension
Classification:
Primary: Idiopathic, no known cause
6% - have family history (AD-vp)
Mutations in BMPR2 (bone morphogenic protein receptor type-2)
CSBRP-Dec-2012
Pulmonary Hypertension
Primary: Idiopathic, Mutations in BMPR2
BMPR2 belongs to TGF-ß receptor superfamily
BMP-BMPR2 signalling play a role in:
- Apoptosis
- Cell proliferation & differentiation
- Embryogenesis
CSBRP-Dec-2012
Pulmonary Hypertension
BMP-BMPR2 signalling in vascular smooth
muscle:
- Inhibits proliferation
- Induces apoptosis
Hence mutations in this gene causes proliferation of
smooth muscle in the vessels
CSBRP-Dec-2012
Pulmonary Hypertension
How this gene gets deleted / rendered
useless?
TWO hit hypothesis:
First hit: genetic loss of one locus
Second hit: Environmental factor
Mutations in the other gene
Environmental factors: disruption of
vasoregualtory mechnisms involving Endothelin,
Prostacyclin synthase or ACE. CSBRP-Dec-2012
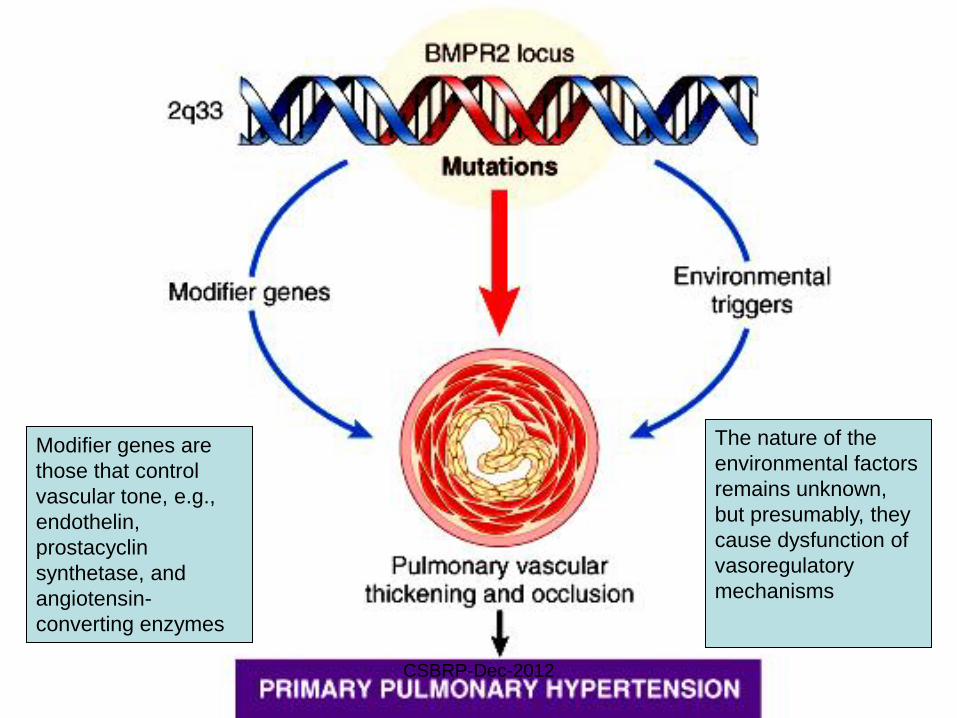
Modifier genes are
those that control
vascular tone, e.g.,
endothelin,
prostacyclin
synthetase, and
angiotensin-
converting enzymes
The nature of the
environmental factors
remains unknown,
but presumably, they
cause dysfunction of
vasoregulatory
mechanisms
CSBRP-Dec-2012
Pulmonary Hypertension
Classification:
Secondary: Structural abnormalities in cardiopulmonary area
• COPD / interstitial lung disease
• Congenital / acquired heart disease
• Recurrent thromboembolism
• Autoimmune diseases
CSBRP-Dec-2012
Pulmonary Hypertension
Secondary: Structural abnormalities in cardiopulmonary area
Endothelial cell dysfunction is produced by the process that initiates the disorder, such as:
The increased shear and mechanical injury associated with left-to-right shunts
The biochemical injury produced by fibrin in thromboembolism
Decreased elaboration of prostacyclin, decreased production of nitric oxide, and increased release of endothelin all promote pulmonary vasoconstriction
CSBRP-Dec-2012
Pulmonary Hypertension
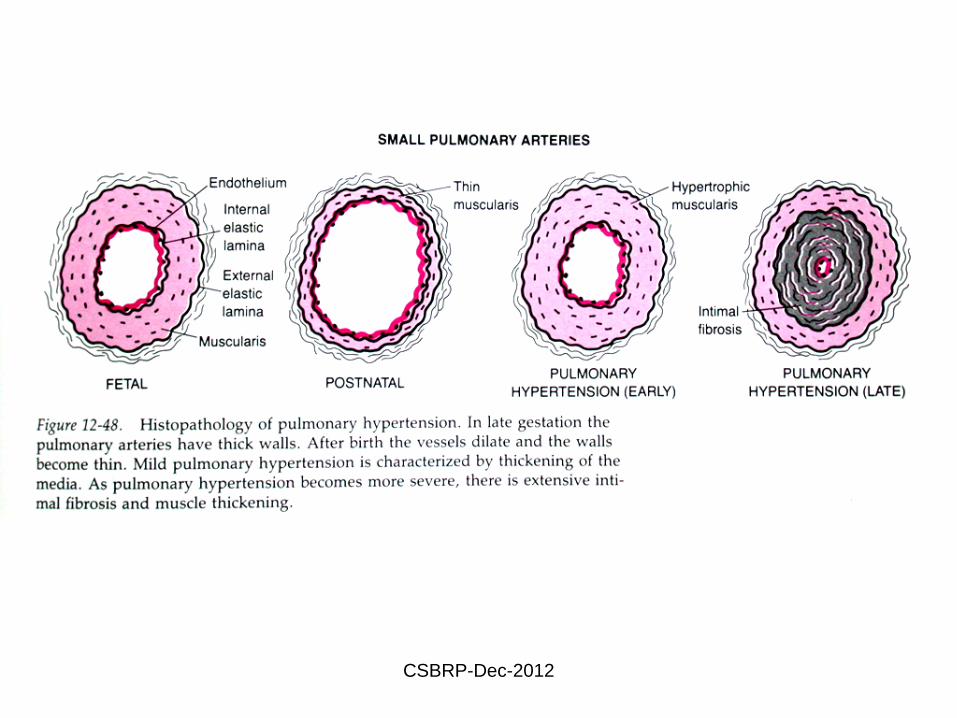
Morphology:
The arterioles and small arteries (40 to 300 µm in diameter) are most prominently affected
1. Medial hypertrophy and
2. Intimal fibrosis
3. Plexogenic pulmonary arteriopathy
CSBRP-Dec-2012
CSBRP-Dec-2012
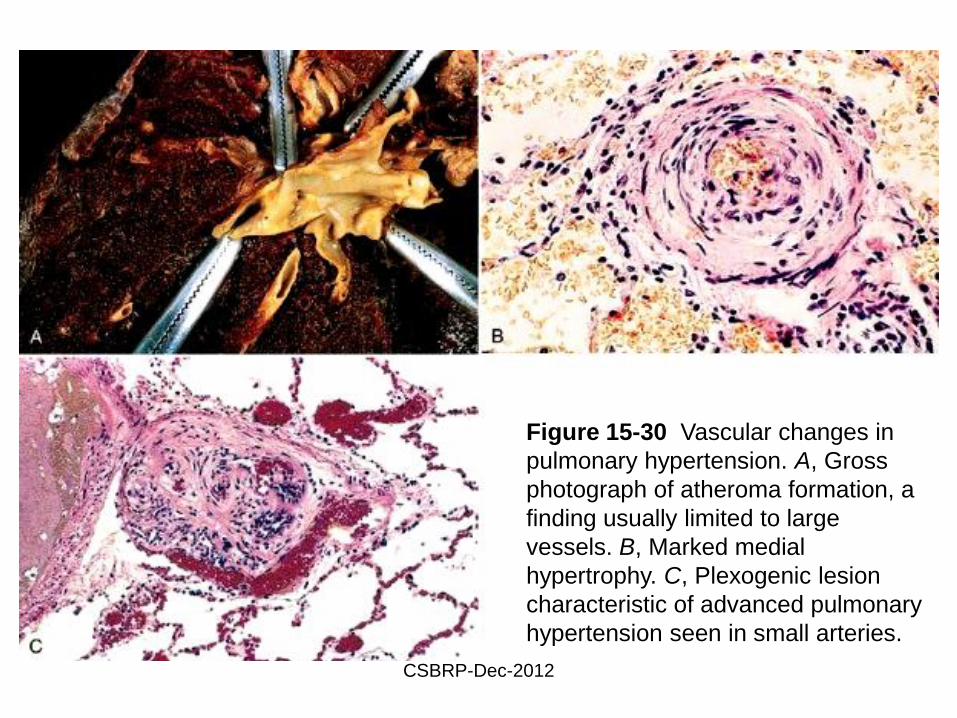
Figure 15-30 Vascular changes in
pulmonary hypertension. A, Gross
photograph of atheroma formation, a
finding usually limited to large
vessels. B, Marked medial
hypertrophy. C, Plexogenic lesion
characteristic of advanced pulmonary
hypertension seen in small arteries.
CSBRP-Dec-2012
Pulmonary Hypertension
Clinical course:
Primary PHT is more common in females
Between 20-40yrs
Dyspnea and fatigue
Chest pain
Cyanosis
RVH
Death: in 2-5yrs in 80% of the patients
due to Cor pulmonale, pneumonia
CSBRP-Dec-2012
E N D
CSBRP-Dec-2012