Embed Size (px)
Citation preview

Rare Headache Syndromes
Moderator: Dr Rohit Bhatia
Presenter: Dr Sucharita Ray

SEARCH STRATEGY:
PubMedGOOGLE SCHOLARHANDBOOK OF CLINICAL NEUROLOGY: Headache; Volume 97International Classification of Headache Disorders 2nd edition (ICHD-2) criteriaT J Schwedt, J P Gladstone, R A Purdy and D W Dodick

Acute
• Subarachnoid hemorrhage
• Cervical artery dissection
• Acute hypertensive crisis
• Ischemic stroke
• Pituitary apoplexy
• Colloid cyst of the third ventricle
• Primary thunderclap headache
• Intracranial infection
Episodic
• Hemiplegic migraine
•Basilar-type migraine
•Cluster headache
•Episodic paroxysmal hemicrania
•SUNCT syndrome
•Chiari malformation
•Trigeminal neuralgia
• Subacute angle-closure glaucoma
•Primary stabbing headache
•Primary headache associated with sexual activity
•Primary cough headache
Chronic
•Giant cell arteritis
•Cerebral venous sinus thrombosis
•Spontaneous intracranial hypotension
• Idiopathic intracranial hypertension
• Intracranial neoplasm
•Sinus headache
•Medication-overuse headache
•Post-traumatic headache
•Cervicogenic headache
•Occipital neuralgia
•Hypnic headache

Miscellaneous Syndromes that are truly rare !!!
Interactive case studies.

CASE 1:A 26-year-old pregnant woman presented with nausea, vomiting, and headache. There was no past medical history of note and she was not taking any medication. O/E she was drowsy and uncooperative. No E/o focal neurology.

CASE 2:A 62-year-old woman presented with a 3-day history of generalized headache of gradual
onset associated with neck stiffness and malaise. On the day of admission, she had awoken covered in blood with no memory of what had happened. She was taking tamoxifen for breast cancer diagnosed 6 months previously for which she had had a mastectomy. On examination, GCS was 14/15 and there was a laceration over theocciput. There was no focal neurological abnormality.

CASE 3:A 19-year-old woman presented with diarrhoea and vomiting, headache and visual
disturbance. She was a smoker and was on OCPs. O/E there was papilloedema and a right VI nerve palsy. She subsequently deteriorated developing bilaterally reduced visual acuity and bilateral VI nerve palsies and then right arm weakness.

CASE 4
A 31-year-old man presented with acute onset headache a/w right arm weakness. There was a past H/O hepatic abscess and hepatic vein thrombosis. O/E he was alert and there was no papilloedema but he had a right CN VI and right-sided pyramidal weakness. He had 2 generalized motor seizures in the ED.

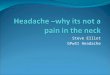
The diagnosis is cerebral venous sinus thrombosis (CVT).A schematic figure of the cerebral venous sinus system is shown in Fig. 2.1.In CVT, the superior sagittal sinus (see Figs. 2.2 and 2.3) and the transversesinuses (see Figs. 2.3 and 2.4) are the most commonly affected followedby the straight sinuses (see Figs. 2.5 and 2.6) and the cavernoussinuses. More than one sinus is usually affected. Thrombosis of theGalenic system (see Fig. 2.6) or isolated involvement of the cortical veinsis infrequent. CVT is often accompanied by raised intracranial pressuresince the dural sinuses contain most of the arachnoid villi and granulationsin which CSF absorption takes place.Occlusion of one of the larger venous sinuses without involvement ofcortical veins or the Galenic venous system generally causes raisedintracranial pressure in the absence of focal neurological signs (


Hence it is important to know that a single clinical phenomenon may have an acute, chronic and episodic presentation. Hence management should be guided by a proper history, observation of the clinical signs and clinical examination to aid in the diagnosis
Still for the most part, certain clinical syndromes can present with some very typical clinical and case scenarios. A knowledge of these signs and symptoms can help clinch the diagnosis at presentation itself.


52 year old female presented with acute onset of headache, 4 to 5 episodes of vomiting, retroorbital pain and blurring of vision in both eyes since early morning.By the time she was rushed to the ER, she was found to be confused about his name and address, was seen to have a BP of 77/43mmHg and was able to count fingers at three feet.Past history was only significant for hypertension





The patient was a 36-year-old retropositive woman with a H/O multiple opportunistic infections, including P carinii and M kanasii pneumonias, cerebral toxoplasmosis, and cryptococcal meningitis. She developed unexplained fever and headache with nuchalrigidity with progressive deterioration of her mental status.
O/E: Cushing response (hypertension with bradycardia), b/l nonreactive and small pupils (1mm), decorticate rigidity and extensor plantar reflexes.
An emergent CT Head was done


The patient was intubated and continued on broad-spectrum antibiotic therapy. An emergency ventriculostomy was performed, which relieved the increased intracranial pressure but clinical improvement was not seen.

POST OPERATIVE CT SCAN

Another ventriculostomy was inserted . Despite appropriate medical therapy, the patient’s neurologic function continued to decline. Two additional ventriculostomiesyielded no clinical benefit. Owing to the absence of cortical activity and poor prognosis, life support was withdrawn,and the patient expired 7 days after last admission



Rare lesions comprising 0.5–1% of primary brain tumors.
Occur in the third to fifth decades of life ,mc site anterior third ventricle> lateral> fourth ventricle>outside ventricular system.
C/F: Headaches are brief, lasting seconds to minutes, and are usually relieved by standing. A well recognized cause of sudden death. Other symptoms include progressive dementia, drop attacks, and spells of transient loss of consciousness. Cyst size does not appear to be a reliable predictor of outcome
Histologically benign, but may obstruct the foramina of Monro to produceacute hydrocephalus. Intermittent foraminal obstruction due to attachment to roof of third ventricle.
Attachment to the third ventricular roof may impart a pendulous character.


24-year-old female c/o left-sided throbbing headaches associated with blurring of vision followed later by development of right-sided hemiparesis and aphasia and later started having right focal motor seizures.Past H/O similar type of headache 12 years back with right sided weakness alternating with left sided weakness Duration of few hours and then reverting back to normal.
Imaging (CT, MRI,MRA), csf lactate serum lactate all were normal
No family history


Hemiplegic migraine was initially described in 1910 as a type of migraine consisting of recurrent headache associated with transient hemiparesis.
AD form of migraine with aura in which some degree of hemiparesis is present during attacksAura typically lasts longer than in migraine with aura and usually comprises visual, sensory, aphasic, and motor symptomsFamily History maybe absent.Two subforms of FHM families exist—pure FHM in 80% and FHM families with cerebellar symptoms in 20%
Responsible gene CACNA1A encoding a neuronal calcium channel, are present in 50% of families with hemiplegic migraine including those with cerebellar signs

A 56-year-old woman c/o 5-year history of daily multiple (upto 5) episodic short-lasting (15-20 seconds each) Attacks occurred up to five times a day and lasted 15–20 s each. The attacks were left-sided, moderately severe and retro-orbital a/w marked tearing and redness of the ipsilateral eye with mild rhinorrhoea but no nausea, photophobia or phonophobia.
No history of migraine nor family history of headache. Clinical examination normal. MRI of the brain was normal.
No particular response to any of the medications ( TCAs/PPnl/ methysergide/ lithium/verapamil, trial of steroids /ergots/triptans/indomethacin, valproate/CBZ)

subtype of the trigeminal autonomic cephalalgias (TACs) . It is characterized by frequent (up to 200/day), strictly unilateral, severe, neuralgiform attacks in the ophthalmic division of the trigeminal nerve which are brief in duration (60 seconds) and occur in association with conjunctival injection and tearingThe diagnosis of SUNCT syndrome is based on operationaldiagnostic criteria (Box 17.1). The differential diagnosis of SUNCT includes trigeminalneuralgia (see Chapter 19), primary stabbing headache(see Chapter 21), paroxysmal hemicrania, and clusterheadache (see Chapter 15 and Fig. 17.1). Clinically similar to trigeminal neuralgia; however, SUNCT isalmost always confined to V1 while trigeminal neuralgia isconfined to V1 in less than 5% of patients. In addition, SUNCTattacks are longer, associated with autonomic symptoms, andhave a refractory period. Secondary causes of SUNCT have been reported with lesionsoccurring most commonly in the pituitary gland, parasellarregion, and posterior fossa. MRI brain with coronal enhanced

images of the pituitary isrequired to rule out a secondary cause. A trial of indomethacin is helpful to exclude an indomethacinresponsiveheadachen Treatment. SUNCT is more refractory to treatment than other primaryheadache disorders. The pharmacologic treatments with reported success in casereports and case series include: anticonvulsants (lamotrigine,gabapentin, carbamazepine, and topiramate), corticosteroids,and intravenous lidocainennn

SUNCT – International Headache Society diagnosticcriteriaA. At least 20 attacks fulfilling criteria B–EB. Attacks of unilateral, orbital, supraorbital or temporal stabbingor pulsating pain lasting 5–240 secondsC. Pain is accompanied by ipsilateral conjunctival injection andlacrimationD. Attacks occur with a frequency from 3 to 200 per dayE. Not attributed to another disorder100100100CPHClusterSUNCT1 hTime