Embed Size (px)
DESCRIPTION
MEDICAL STUDENTS
Citation preview

1
Respiratory Examination
Introduction
W - Wash your hands.I – Introduce yourself (full name and role). Greet the patient with their title and surname, and check you are using their preferred form of address.P - Permission. Explain that you wish to perform a respiratory examination and obtain consent for the examination.E - Expose the necessary parts of the patient. Ideally the patient should be undressed from the waist up taking care to ensure the patient is not cold or unnecessarily embarrassed.R – Reposition the patient. In this examination the patient should be supine and reclined at 45 degrees.
Peripheral ExaminationEnd of the BedThe position of the patientFirst look at the patient from the end of the bed for signs of breathlessnesss or distress. Those with extreme pulmonary dysfunction will often sit up-right. In cases of real distress, they will lean forward, resting their hands on their knees in what is known as the tri-pod position.
It is also important to look at the surrounding environment for sputum pots, nebulisers, peak-flow meters, inhalers or oxygen tubing.

2
Breathing through pursed lips, often seen in cases of emphysema.
Ability to speak. At times, respiratory rates can be so high and/or work of breathing so great that patients are unable to speak in complete sentences. If this occurs, note how many words they can speak (i.e. the fewer words per breath, the worse the problem!).
HandsLook at the hands for clubbing, tar staining and peripheral cyanosis.Examine for tremor and a carbon dioxide retention flap.Palpate the radial pulse to calculate heart rate. At this time also assess respiratory rate and determine the pattern of breathing.
FaceLook at the patient’s eyes and face for signs of Horner’s syndrome or lupus pernio.Inspect the conjunctivae for anaemia.Look at the lips and tongue for central cyanosisLie the patient at 45 degrees and assess JVP.Palpate the cervical, supraclavicular and axillary lymph nodes.Examination of the chest
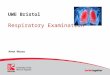
Review of Lung Anatomy:Understanding the pulmonary exam is greatly enhanced by recognizing the relationships between surface structures, the skeleton, and the main lobes of the lung. Realize that this can be difficult as some surface landmarks (eg nipples of the breast) do not always maintain

3
their precise relationship to underlying structures. Nevertheless, surface markers will give you a rough guide to what lies beneath the skin. The pictures below demonstrate these relationships. The multi-colored areas of the lung model identify precise anatomic segments of the various lobes, which cannot be appreciated on examination. Main lobes are outlined in black. The following abbreviations are used: RUL = Right Upper Lobe; LUL = Left Upper Lobe; RML = Right Middle Lobe; RLL = Right Lower Lobe; LLL = Left Lower Lobe.

4

5
Inspection1.look for chest deformity while you are examining the patient “anteriorly” or spine deformity “posteriorly”.

6
These may arise as a result of chronic lung disease (ex.emphysema), occur congenitally, or be otherwise acquired. In any case, they can impair a patient's ability to breathe normally.
a. Barrel chest: chest wall increased anterior-posterior , Associated with emphysema and lung hyperinflation
b. Pectus excavatum: sternum sunken into the chestc. Pectus carinatum - sternum protruding from the chestd. Kyphosis: Causes the patient to be bent forward
e. Scoliosis: Condition where the spine is curved to either the left or right
2.look for skin ,scars , dilated vessels , respiratory distress signs Skin eruption e.g Herpes zoster Nodules (inflammatory, metastatic, lipoma, neurofibroma…) Subcutaneous emphysema Purpuric spots, Vascular spiders, Bruises Prominent blood vessels (arterial in coarctation of aorta and venous in
SVC obstruction)

7
Scars (previous operation, trauma, sterneotomy) Discharging sinuses Lesions of the breasts and enlargement of axillary LNs
.Signs of respiratory distress-
. Pursed-lip breathing - COPD (used to increase end expiratory pressure)
. Accessory muscle use (scalene muscles)
. Diaphragmatic paradox - the diaphragm moves opposite of the normal direction on inspiration
. Any degree of asymmetry or asynchrony of chest expansion
3. Look for respiratory movement:
In female ,it is thoracoabdominal with chest predominant movement.
In male , it is abdominothoracic movement
4. Use of accessory muscles of breathing:
Intercostal indrawing , supraclavicular or intercostal retraction.
PALPATION:
Place the entire palm of each hand first on the superior portion of both hemithoraces and then, gently though firmly, move the hand inferiorly to just below the twelfth rib. Repeat the process moving laterally and subsequently anteriorly; search for rib deformities, nodules, and areas of tenderness. In the face of a history of chest discomfort, ask the patient to point to the area(s) of greatest discomfort. Palpate the area with increasing firmness in an attempt to elicit tenderness and to assess if this maneuver reproduces the patient's symptoms.

8
1. Trachea:The trachea should be checked to see if it is in the normal central position. This means the distance between the trachea and the sternomastoid muscles should be equal on both sides. Slight displacement of the trachea to the right is fairly common in healthy people. Palpate the trachea by placing a finger either side of the trachea and judging whether the distance between it and the sternomastoid tendons are equal on both sides. Before doing this warn the patient that this might be slightly uncomfortable.
Tracheal deviation is indicative of mediastinal displacement to one side, which can be due to:
The trachea is pushed away to other side:
1. pneumothorax “large volume of air in the pleural space”
2. Pleural effusion “Large volumes of fluid in the pleural space”
Trachea is pulled by apical collapse , fibrosis or tumour while it is pushed to other side by air or fluid “if large”.
Cricosternal distance
Measuring the cricosternal distance can help determine if the patient is hyperventilating. A distance of less than three of the patient’s finger-breadths indicates hyperventilation, usually evident as a visible ‘descent’ of the trachea during inspiration (tracheal tug) (Ford et al, 2005).
2.APEX BEAT:
It is the lower most , outer most ,most forceful pulsation.
It is important to check the line, space and character.
Position of the apex beat can confirm or exclude mediastinal displacement (Ford et al, 2005). This is not a reliable sign if there is cardiomegaly (Epstein et al, 2003).
3.CHEST EXPANSION:
Chest expansion must be assessed to determine the depth and quality of movement on each side of the chest. Both sides should be assessed for symmetry. The symmetry and degree of chest expansion can be more accurately evaluated by observing chest movement than by palpating the chest wall (Ford et al, 2005).
Palpation of Respiratory Movements
1. Respiratory movements in the infraclavicular regions

9
2. Respiratory movements at the costal margins
3. Respiratory movements of the lower ribs posteriorly
Signifacance of reduced respiratory movements
Unilateral reduction of chest wall movements:
Pleural effusion/empyema
Pneumothorax
Pulmonary collapse
Pleural or parenchymatous pulmonary fibrosis
Bilateral reduction of chest wall movements:
Bronchial asthma
Emphysema
Diffuse pulmonary fibrosis

10
Method:
Assess chest expansion by putting the fingers of both your hands as far round the chest as possible and then bring your thumbs together in the midline . Ask your patient to take a deep breath and observe whether the distance moved is the same for both thumbs. Your hands should lift symmetrically outward when the patient takes a deep breath . Asymmetric lung expansion, as occur when anything fills the pleural space (e.g. air or fluid), may then be detected as the hand on the affected side will move outward to a lesser degree. thumbs typically separate by approximately 2 to 3 cm.ANT= 2 LEVELS ,POST= 3 LEVELS
4.TACTILE VOCAL FREMITUS:
.Comparison is mandatory in chest examination.
.The anatomical land marks to use are:
Anteriorly= mid-clavicular line
Laterally= mid-axillary line
Posteriorly=above scapula , parascapular “paraspinal”, below scapula

11
Physiological idea:
Normal lung transmits a palpable vibratory sensation to the chest wall as it is a good conductive media for sound.
How to do?
This palpable vibratory sensation is called fremitus. It can be detected by placing the ulnar aspects of both hands firmly against either side of the chest while the patient says the words "Ninety-Nine” whilst physician sense with ulnar aspect of hand for changes in sound conduction. This maneuver is repeated until the entire posterior thorax is covered. The bony aspects of the hands are used as they are particularly sensitive for detecting these vibrations.
Palpate for tactile vocal fremitus by placing the edge or flat of your hand on the chest and asking your patient to say ‘ninety nine’ or forty-four.
. Increased TVF
• Consolidation
• Cavitation
• Collapse with patent main bronchus
.Decreased TVF
• Thick chest wall
• Pleural effusion
• Collapse
• Pleural fibrosis

12
• Pneumothorax
4. Percussion
. Press The last 2 phalanges of your left middle finger firmly on the patient's back on the
area to be percussed and raise the second and fourth fingers off the chest surface; otherwise, both sound and tactile vibrations will be blunted.
.Middle finger ”right” strikes the middle phalanx of the other middle finger.. Use a quick, sharp wrist motion, Allow your hand to swing freely at the wrist (like a catcher throwing a baseball to second base) to strike the finger in contact with the chest wall with the tip of the third finger of the other hand. The best percussion site is between the proximal and distal interphalangeal joints.
.When percussing any one spot, 2 or 3 sharp taps should suffice.
. After you have percussed the left chest, move your hands across and repeat the same procedure on the right side.
. Percuss the posterior, lateral, and anterior chest wall in such a manner that the long axis of the percussed finger is roughly parallel to the ribs. Compare one side to the other.
.In general percussion in 5 or so different locations should cover one hemi-thorax.
.If you detect any abnormality on one side, it's a good idea to slide your hands across to the other for comparison.
Cut your nails

13
Percussion :Anterior Chest
1. Start percussion by tapping directly in the middle of both clavicles.
2.. Percuss from side to side and top to bottom using the pattern shown in the illustration away from bones and midline.
3. Compare one side to the other looking for asymmetry.
4. Note the location and quality of the percussion sounds you hear.
5. The finger on the chest should always be placed in the intercostal space, and there is no need to percuss more heavily than is necessary as this can be distressing for the patient.
6. Normal dullness is caused by liver on right midclavicular line”6th” , heart on left midclavicular line”4th intercostals space” ,andSpleen on left midaxillary line “9th,10th,11th”.

14
Percussion: Posterior Chest In general, percussion is limited to the posterior lung fields.
Ask the patient to cross their hands in front of their chest, grasping the opposite shoulder with each hand. This will help to pull the scapulae laterally, away from the percussion field.
Avoid bones and midline-Work down the "alley" that exists between the scapula and vertebral column.
Percuss from side to side and top to bottom using this pattern. Omit the areas
covered by the scapulae. Compare one side to the other looking for asymmetry.
Note the location and quality of the percussion sounds you hear. Find the level of the diaphragmatic dullness on both sides.
you will develop a sense of where the normal lung should end by simply looking at the chest.

15
A. What is "Speed percussion" ?
It help to accentuate the difference between dull and resonant areas. During this technique, the examiner moves their left (i.e. the non-percussing) hand at a

16
constant rate down the patient's back, tapping on it continuously as it progresses towards the bottom of the thorax. This tends to make the point of inflection (i.e. change from resonant to dull) more pronounced.
B. What is Diaphragmatic Excursion?1. Find the level of the diaphragmatic dullness on both sides. 2. Ask the patient to inspire deeply. 3. The level of dullness (diaphragmatic excursion) should go down 3-5cm symmetrically. 4. Decreased or asymmetric diaphragmatic excursion may indicate paralysis or
emphysema.
C. Tidal percussion:
1. It is used to differentiate supra-diaphragmatic from infra-diaphragmatic dullness.2. While the patient seated find the upper level of dullness3. Ask the patient to take deep inspiration and to hold it then percuss again.4. If the note becomes resonant à infra-diaphragmatic cause.5. If there is no change of the note à supra-diaphragmatic cause as pleural effusion.
THE PURPOSE:
The purpose of percussion is to determine if the area under the percussed finger is air filled (sounding resonant like a drum), fluid filled (a dull sound) or solid (a flat sound). If the normal air-filled tissue has been displaced by fluid (e.g. pleural effusion) or infiltrated with white cells and bacteria (e.g. pneumonia), percussion will generate a deadened tone. Alternatively, processes that lead to chronic (e.g. emphysema) or acute (e.g. pneumothorax) air trapping in the lung or pleural space, respectively, will produce hyper-resonant (i.e. more drum-like) notes on percussion.
Stony dull------ 1. pleural effusion
2. pleural fibrosis

17
Dull “impaired percussion note”
1. Consolidation “pneumonia, cancer, embolism”
2. Collapse
Auscultation:
Keys to performing a sensitive yet thorough exam:
o Explain what you're doing (" why) before doing it .o Expose the minimum amount of skin necessary .o Examining lungs of female patients:
Expose the chest only to the extent needed. For lung exam, you can listen to the anterior fields by exposing only the top part of the breasts .`
Enlist patient's assistance, asking them to raise their breast to a position that enhances your ability to listen to the heart
o Don't rush, act in a callous fashion, or cause pain o PLEASE... don't examine body parts thru gown as:
It reflects Poor technique You'll miss things You'll lose points on scored exams .
Anatomical areas to remember :
.Lower lobes occupy the bottom 3/4 of the posterior fields
.Right middle lobe heard in right axilla
.Lingula in left axilla

18
. Upper lobes in the anterior chest and at the top 1/4 of the posterior fields.
This can be quite helpful in trying to pin down the location of pathologic processes that may be restricted by anatomic boundaries (e.g. pneumonia).
Technique of Auscultation
“ The chest is ausculted with the diaphragm”
1. Put on your stethoscope so that the ear pieces are directed away from you. Adjust the head of the scope so that the diaphragm is engaged. If you're not sure, scratch lightly on the diaphragm, which should produce a noise. If not, twist the head and try again. Gently rub the head of the stethoscope on your shirt so that it is not too cold prior to placing it on the patient's skin.
2. While the patient relaxed and breathes normally with mouth open, auscultate the lungs, making sure to auscultate the apices and middle and lower lung fields posteriorly, laterally and anteriorly.
3. The upper aspect of the posterior fields are examined first. Listen over one spot and then move the stethoscope to the same position on the opposite side and repeat. This again makes use of one lung as a source of comparison for the other.
4. The entire posterior chest can be covered by listening in roughly 4 places on each side. Of course, if you hear something abnormal, you'll need to listen in more places.
5. Alternate and compare both sides at each site.
6. Listen to at least one complete respiratory cycle at each site.

19
7. First listen with quiet respiration. If breath sounds are inaudible, then have him take deep breaths.
8. The lingula and right middle lobes can be examined while you are still standing
behind the patient.
9. Then, move around to the front and listen to the anterior fields in the same fashion IF
NOT STARTED BY IT. This is generally done while the patient is still sitting upright. Asking female patients to lie down will allow their breasts to fall away laterally, which may make this part of the examination easier
A few additional things worth noting.
1. Ask the patient to take slow, deep breaths through their mouths while you are performing your exam. This forces the patient to move greater volumes of air with each breath, increasing the duration, intensity, and thus detectability of any abnormal breath sounds that might be present.
2. Sometimes it's helpful to have the patient cough a few times prior to beginning auscultation. This clears airway secretions and opens small atelectatic (i.e. collapsed) areas at the lung bases.
3. If the patient cannot sit up (e.g. in cases of neurologic disease, post-operative states, etc.), auscultation can be performed while the patient is lying on their side.

20
What can you expect to hear?
• Note the intensity of breath sounds and make a comparison with the opposite side. • Assess length of inspiration and expiration. Listen for a pause between inspiration,
expiration and the quality of pitch of the sound • Also compare the intensity of breath sounds between upper and lower chest in
upright position. Compare the intensity of breath sounds from dependent to top lung in the decubitus position.
.Note the presence or absence of adventitious sounds.
IN SUMMARY;1. EQUALITY OF ENTRY OF BREATHING SOUNDS IN BOTH SIDES2. TYPE OF BREATHING 3. ADDED SOUNDS “CREPITATION,RHONCHI,PLEURAL RUB”
IN NORMAL LUNG The normal breath sounds heard over the lung are vesicular breathing. The vesicular breathing is heard over the lungs, lower pitched and softer than
bronchial breathing. Expiration is shorter (I > E) and there is no pause between inspiration and expiration.
The breath sounds are symmetrical and louder in intensity in bases compared to apices in erect position and dependent lung areas in decubitus position.
No adventitious sounds are heard. The breath sounds heard over the tracheobronchial tree are called bronchial
breathing. The only place where tracheobronchial trees are close to chest wall without
surrounding lung tissue are trachea, right sternoclavicular joints and posterior right interscapular space. These are the sites where bronchial breathing can be normally heard. In all other places there is lung tissue and vesicular breathing is heard.
The bronchial breath sounds have a higher pitch, louder, inspiration and expiration are equal and there is a pause between inspiration and expiration.
A prolonged expiratory phase (E > I) indicates airway narrowing, as in: Bronchial asthma. Chronic bronchitis

21
Bronchial breathing may be heard in pathological conditions as: Consolidation Collapse with patent large airways Compressed lung by a large pl effusion or a tension pneumothorax Pulmonary fibrosis Cavitation
Voice Transmission Tests: are only used in special situations. All these tests become abnormal in consolidation to confirm bronchial breathing. They include
Bronchophony Whispered Pectoriloquy Egophony
Voice sounds- Bronchophony1. Ask the patient to say "ninety-nine“ or 44 in arabic several times in a normal voice.2. Auscultate several symmetrical areas over each lung.
3.The sounds you hear should be muffled and indistinct. Louder, clearer sounds are called bronchophony
Whispered Pectoriloquy
1. Ask the patient to whisper "ninety-nine“ or 44 in arabic several times. 2. Auscultate several symmetrical areas over each lung.
3.You should hear only faint sounds or nothing at all. If you hear the sounds clearly this is referred to as whispered pectoriloquy.
Egophony1. Ask the patient to say "ee" continuously. 2. Auscultate several symmetrical areas over each lung. 3. You should hear a muffled "ee" sound. If you hear an "ay" sound this is referred to as
"E -> A" or egophony.
4. Egophony (British: Aegophony) is an increased resonance of voice sounds heard when auscultating the lungs, often caused by lung consolidation and fibrosis.
5. It is due to enhanced transmission of high-frequency noise across fluid, such as in abnormal lung tissue, with lower frequencies filtered out. It results in a high-pitched nasal or bleating quality in the affected person's voice.

22
Adventitious sounds
Crepitations: types Rhonchi: sibilant and sonorous Pleural rub
Wheezes are whistling-type noises produced during expiration (and sometimes inspiration) when air is forced through airways narrowed by bronchoconstriction, secretions, and/or associated mucosal edema. As this most commonly occurs in association with diffuse processes that affect all lobes of the lung (e.g. asthma and emphysema) it is frequently audible in all fields. In cases of significant bronchoconstriction, the expiratory phase of respiration (relative to inspiration) becomes noticeably prolonged. The greater the difference, the worse the obstruction. Occasionally, focal wheezing can occur when airway narrowing if restricted to a single anatomic area, as might occur with an obstructing tumor or bronchoconstriction induced by pneumonia. Wheezing heard only on inspiration is referred to as stridor and is associated with mechanical obstruction at the level of the trachea/upper airway. This may be best appreciated by placing your stethescope directly on top of the trachea.
Note when the wheezes occur and if there is a change after a deep breath or cough. Also note if the wheezes are monophonic (suggesting obstruction of one airway) or polyphonic (suggesting generalized obstruction of airways).Conditions:asthmaCHFchronic bronchitis

23
COPDpulmonary oedema
Rales (a.k.a. crackles) are scratchy sounds that occur in association with processes that cause fluid to accumulate within the alveolar and interstitial spaces. The sound is similar to that produced by rubbing strands of hair together close to your ear. Pulmonary edema is probably the most common cause, at least in the older adult population, and results in symmetric findings. This tends to occur first in the most dependent portions of the lower lobes and extend from the bases towards the apices as disease progresses. Pneumonia, on the other hand, can result in discrete areas of alveolar filling, and therefore produce crackles restricted to a specific region of the lung. Very distinct, diffuse, dry-sounding crackles, similar to the noise produced when separating pieces of velcro, are caused by pulmonary fibrosis, a relatively uncommon condition. Crepitations are present in all sorts of conditions, and really are non-specific. Crepitations are usually divided into 'coarse' and 'fine', and may occur during inspiration or expiration
Auscultation over the same region should help to distinguish between these possibilities, as consolidation generates bronchial breath sounds while an effusion is associated with a relative absence of sound. Similarly, fremitus will be increased over consolidation and

24
decreased over an effusion. As such, it may be necessary to repeat certain aspects of the exam, using one finding to confirm the significance of another.
The mechanical basis of crackles: Small airways open during inspiration and collapse duringexpiration causing the crackling sounds. Another explanation for crackles is that air bubblesthrough secretions or incompletely closed airways during expiration.Conditions:ARDSasthmabronchiectasischronic bronchitisconsolidationearly CHFinterstitial lung diseasepulmonary oedema
Pleural Rub Pleural rubs are creaking or brushing sounds produced when the pleural surfaces are inflamed or roughened and rub against each other. They may be discontinuous or continuous sounds.They can usually be localized a particular place on the chest wall and are heard during both the inspiratory and expiratory phases.Conditions:pleural effusion
pneumothorax
3 types of lesions