Embed Size (px)
Citation preview
Peripheral Blood Stem Cells Transplantation
(PBSCT)
Dr. AG Almosewi
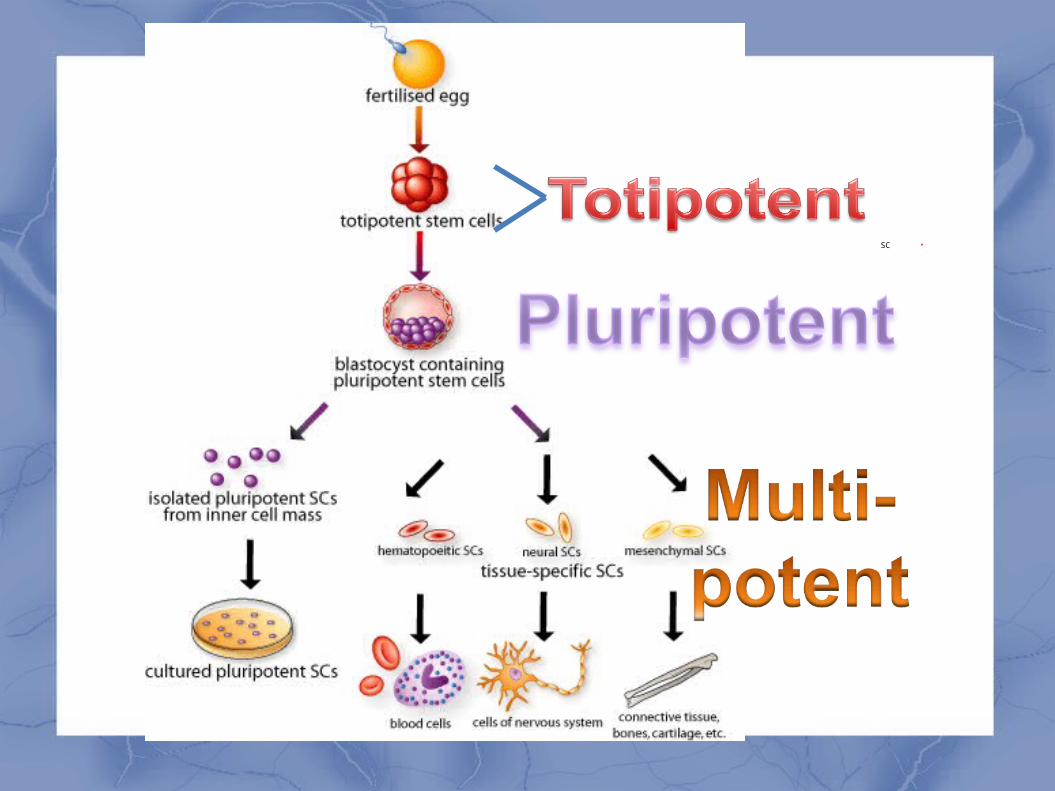
Stem Cell – Definition
A cell that has the ability to continuously divide and differentiate (develop) into various other kind(s) of cells/tissues
SC
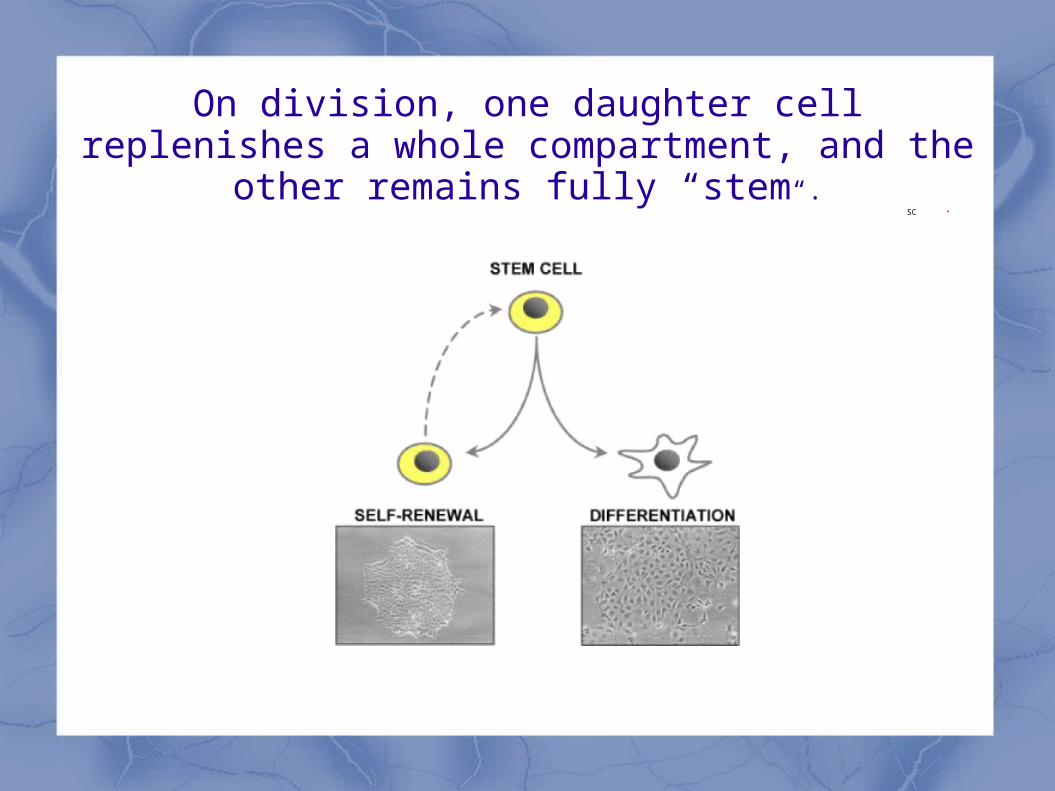
On division, one daughter cell replenishes a whole compartment, and the other remains fully “stem“.
SC
HSCT
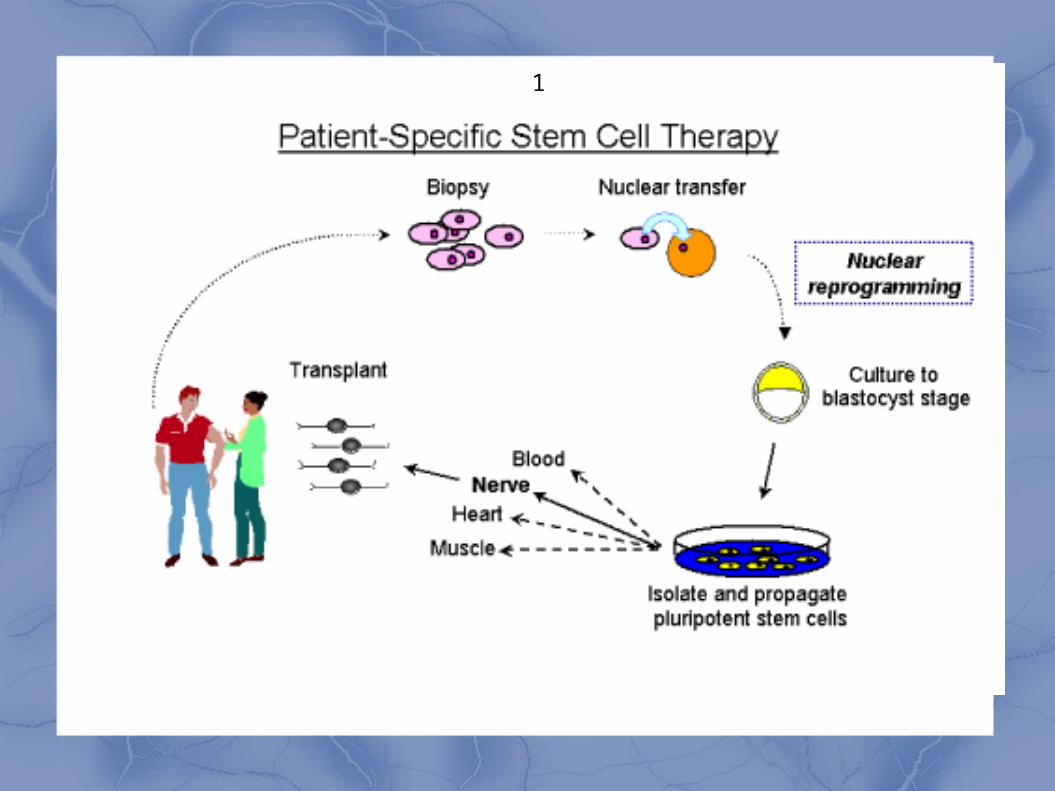
Intravenous infusion of autologous or allogeneic stem cells collected from bone marrow, peripheral blood, or umbilical cord blood to reestablish hematopoietic function in patients whose bone marrow or immune system is damaged or defective.
Why is Stem Cell Research So Important ?
Stem cells can replace diseased or damaged cells
Stem cells allow us to study development and genetics
Stem cells can be used to test different substances (drugs and chemicals)
Stem Cell ApplicationsStem Cell Applications
Tissue repair
- nerve, heart, muscle, organ, skin
Cancers
Autoimmune diseases
- diabetes, rheumatoid arthritis, MS
G
1
Indications
eliminate a bone marrow infiltrative process, such as leukemia,
correct congenital immunodeficiency disorders.
allow patients with cancer to receive higher doses of chemotherapy than bone marrow can usually tolerate;
replacement of marrow progenitors for the purpose of making normal red cells (eg, in hemoglobinopathies)
making corrective enzymes (eg, in storage disorders),
and mediating tissue repair (eg, in epidermolysis bullosa).
Transplant considered in patients with severe AID
Life-threatening disease
Disease of major morbidity (diffuse Scleroderma)
unresponsive to standard therapy (Systemic Lupus)
Early in progressive relapse (Multiple Sclerosis)
Thalassemia - An 80% disease-free survival rate is achieved after allogenic HSCT
Sickle cell anemia - Sickle cell anemia is potentially curable with allogenic HSCT
tolerance
Induction of solid organ graft tolerance
In living donor solid organ transplants
liver
Kidney
Pancreatic islet cell
The use of HSCT to mediate tissue repair
Injection of stem cells into area of dead heart muscle
regenerates viable muscle Injection of stem cells promotes formation of new blood
vessels in injured heart muscle The PROTECT-CAD bone marrow mononuclear cells
were injected directly into ischemic myocardium in patients with refractory myocardial ischemia. The 6-month follow-up showed improvement in exercise time and left ventricular function.
Peripheral blood stem cell transplantation(PBSCT) is the most common transplanta-tion procedure performed in medicine
Its clinical introduction in 1986 replaced BM asa stem-cell source to approximately 100%inthe autologous and to approximately 75%inthe allogeneic transplantation setting
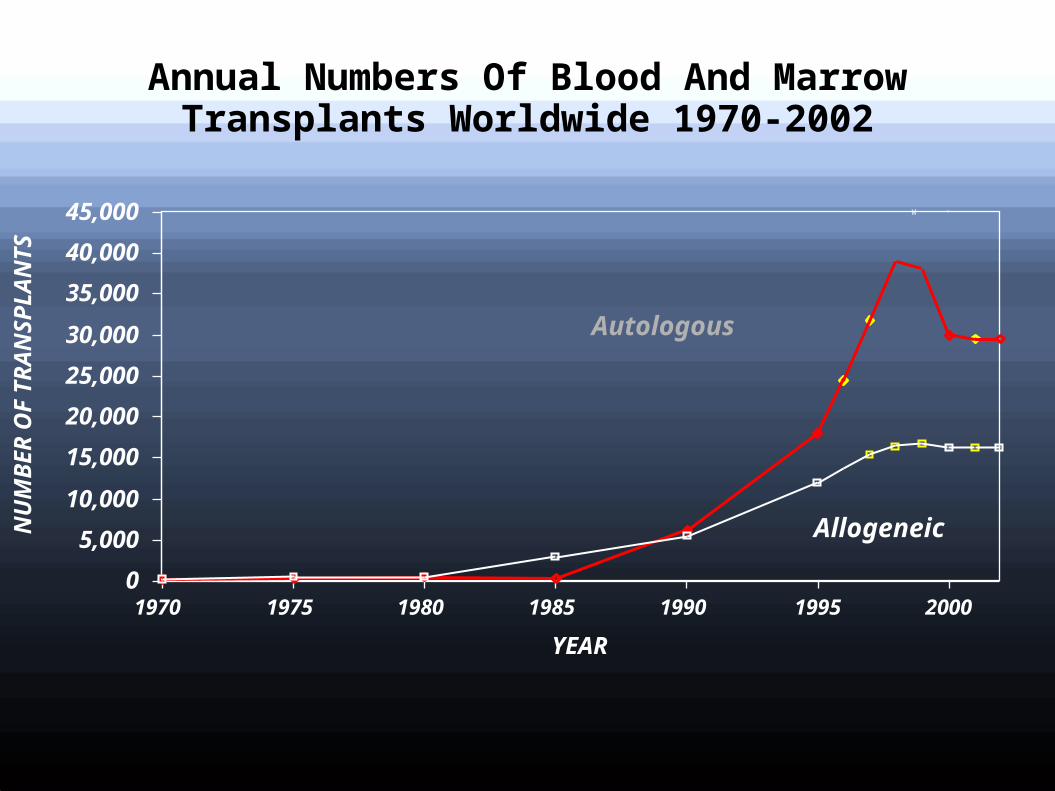
Annual Numbers Of Blood And Marrow Transplants Worldwide 1970-2002
W
NU
MB
ER
OF
TR
AN
SP
LA
NT
S
YEAR
1970 1975 1980 1985 1990 1995
Autologous
Allogeneic
20000
5,000
10,000
15,000
20,000
25,000
30,000
35,000
40,000
45,000
Until about 20 years ago, the only way to collect the stem cells was to have the patient or donor undergo as many as 50–100 BM aspirations .
The discovery that stem cells could be collected from the bloodstream by giving a patient or donor injections of stem cell growth factors such as Neupogen , this has become the standard method.
It is rarely necessary to use the old method of direct bone marrow harvesting from the pelvic bone .
Methods of Collecting Stem Cells from the Blood Stream (PBSC)
1) giving growth factors alone . 2) giving growth factors with chemotherapy.
Mobilization by growth factors alone
The white cell growth factors ( filgrastim (Neupogen) at 10 mcg/kg/d ) used to stimulate the release of stem cells from the bone marrow into the bloodstream. ”
Mozobil (plerixafor),
The injections are given daily for three or more days. Stem cells are usually collected on the 4thor 5th day after starting the injections.
The collections and injections will continue daily until sufficient stem cells are obtained
Chemotherapy plus growth factors.
Following chemotherapy for stem cell mobilization, a white cell growth factor is given by injection under the skin daily for approximately ten days.(can be done at home ot outpatientclin
Once the number of stem cells in the blood stream is high enough, they will be collected over 2–5 days, while the patient is still receiving the growth factor injections.
Harvesting Procedure
By leukapheresis The apheresis procedure will last 3–4 hours
each day for 1 to 5 days. Apheresis is usually done as an outpatient procedure.
After collection, the peripheral blood is taken to the processing laboratory, where blood cells are prepared for freezing (cryopreservation).
Excellent function of stem cells is retained for at least 10 years.
a minimum number of stem cells to safely complete a transplant is 2 million CD34+ cells per kilogram of body weight .
In situations where a sufficient number of blood stem cells cannot be harvested, patients may qualify for use of Mozobil .

Tansplantation
The previously collected stem cells will be given back, into the bloodstream one to two days after administration of the highdose chemotherapy. This procedure is often referred to as the transplant .
The transplant takes place in the patient’s room. ( as BT)
GVHD prophylaxis : tacrolimus or cyclosporine and methotrexate
Engrafment
SCs take 10–14 days to produce new blood cells in substantial numbers.Growth factors may be given .
The patients may remain in the hospital until the white blood cell counts reach a level safe enough for the patient to be discharged.
recovery
The average time in the hospital for the chemotherapy, transplant, and recovery is approximately 3 weeks . ( some centers have nearby facilities and some allow sleep at home)
Patients usually cannot resume normal activities or return to full-time work for up to three to six months after the transplant .
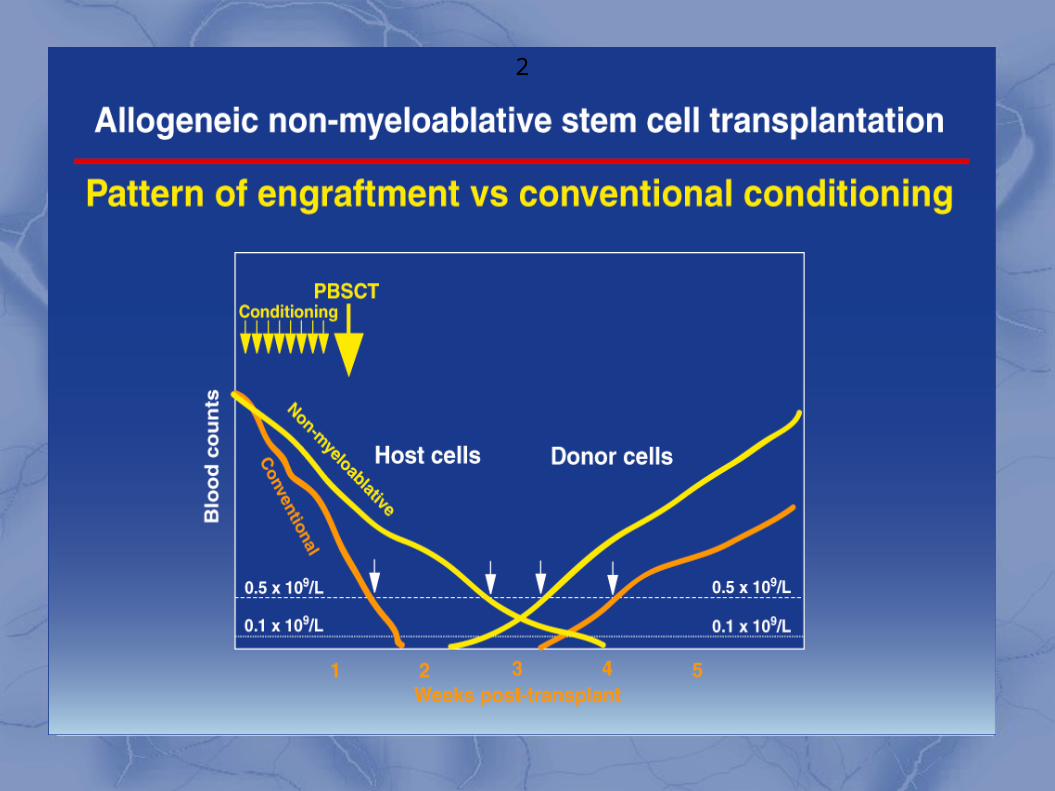
Nonmyeloablative stem cell transplantation (NST)
(NST) is increasingly used in older patients
Nonmyeloablative conditioning: fludarabine , busulfan Myeloablative conditioning : cyclophosphamide
fractionated total body irradiation (TBI) or oral busulfan and cyclophosphamide .
Overall survival was improved in the NST group at 1 year , and 2 years . The nonrelapse mortality rate was lower for NST patients , but the relapse rate was higher
Nonmyeloablative Stem Cell Transplants as
Immunotherapy• “Mini transplants”: less cytoablative
therapy– host/donor marrow chimerism prominent
– low level GVHD•if chimerism present .
– reduction in immunosuppression– donor lymphocyte infusion– high remission re-induction rate– lower mortality/morbidity
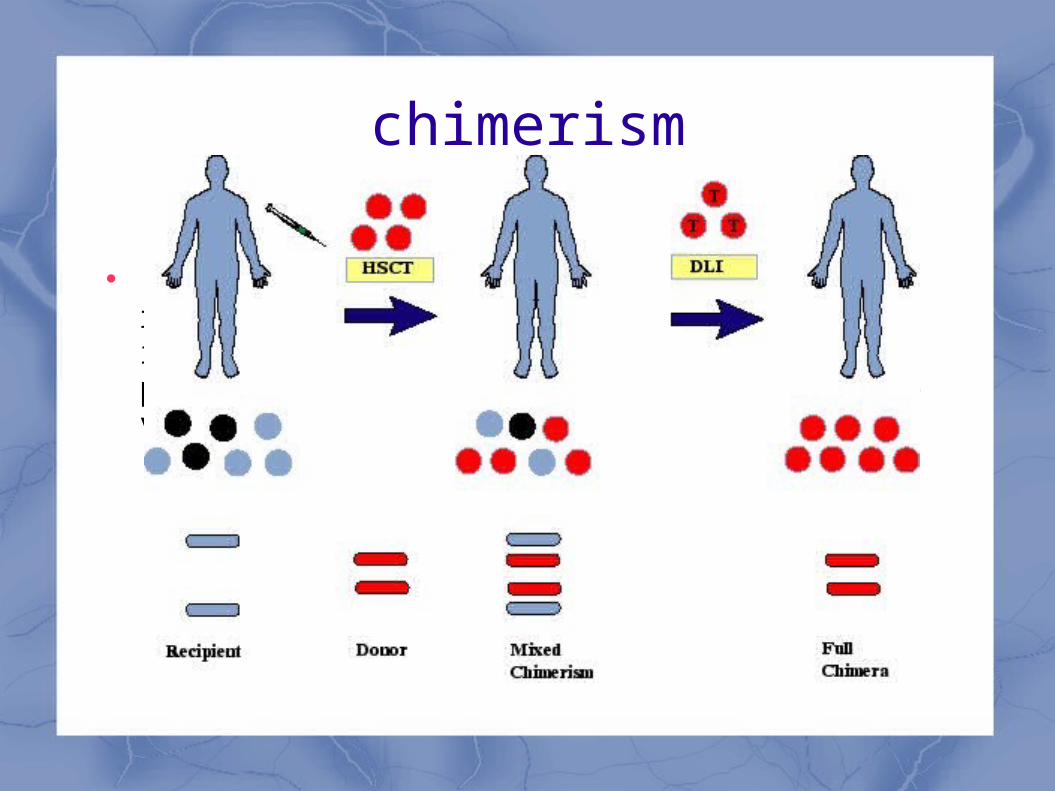
chimerism
Although mixed chimerism reduces the risk of graft-versus-host disease(GVHD), it may also lead to tumor tolerance, potentially abolishing a beneficial graft-versus-malignancy (GVM) effect.
Q
2
2
Peripheral blood HSCT grafts, have
a greater number of CD34+ progenitor → faster marrow recovery (8-10 days for neutrophil and 10-12 days for platelet recovery) → . decreased mortality and early hospital
discharges.
more T cells → higher graft-versus-tumor or graft-versus-leukemia effect and results in decreased relapse rates and increased incidence of GVHD , but ( There was no significant difference between PBSCT and BMT in the cumulative incidence of grades II-IV acute GVHD at100 days after transplantation,
Peripheral blood HSCT
PBSCT have recently been the predominant source of HSCT grafts secondary to the :
nonsurgical method of collection, graft availability, and faster engraftment time.
Peripheral blood HSCT versus bone marrow HSCT
meta-analysis : leukemia Peripheral blood HSCT was
associated with decreased leukemia relapse rates, better overall survival, and increased chronic GVHD
Peripheral blood HSCT versus bone marrow HSCT
A long-term follow-up for hematological malignancy
both 2- and 10-year overall survival was superior with peripheral blood HSCT.[
Manipulation of Stem Cell Grafts
The removal of red blood cells from the donor graft prevents hemolysis in the recipient of ABO-incompatible allogenic transplants
T-cell depletion in the allogenic transplantation setting : reduce or eliminate the possibility that graft versus host disease (GVHD) will develop , but (associated with increase in engraftment failure in up to 10% and higher relapse rates
Recent discovery
Yamanaka factors Transcription factors that can reprogram
differentiated cells into pluripotents,termed inducible pluripotent (iPS)
A human can donate a small amount of blood or tissue, which can be transformed into his or her own iPS cells. These iPS cells can then be differentiated into any tissue in the body.
Since the iPS cells can expand in tissue culture, they can also be efficiently modified by techniques such as gene therapy .
Thanks