Embed Size (px)
Citation preview
Mubarak M Abdelkerimubarak M Abdelkerim
Trauma FellowTrauma Fellow
Hemodynamic Instability in Patients with Pelvic Fractures

Objectives:
Epidemiology & Relevance Anatomical Review Classification Systems Hemorrhage Control Management
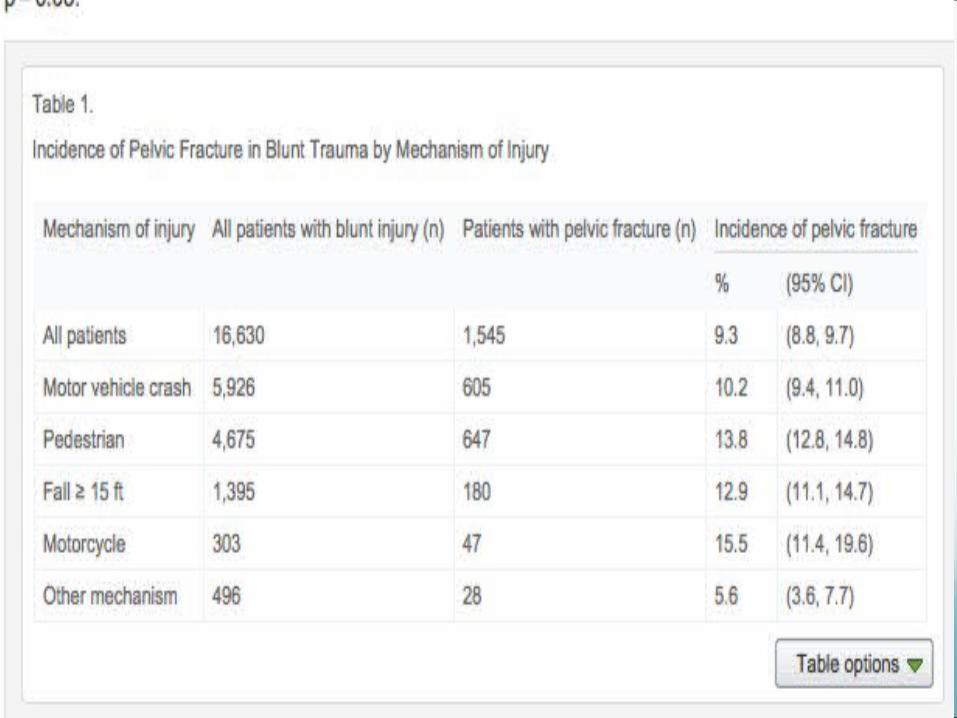
Pelvic Fractures: Epidemiology ~3% of all fractures in ED
50-60% secondary to MVA Motorcycle crashes ~15% Car vs. pedestrian ~15% Falls 10-30% Crush injuries ~5%
Mortality 6-10%; Inc’s to ~50% in unstable pt Tends to occur in setting of multi-system injury
therefore often other serious injuries Complications:
Hemorrhage, neurological injury, deformity, GU injury, GI injury
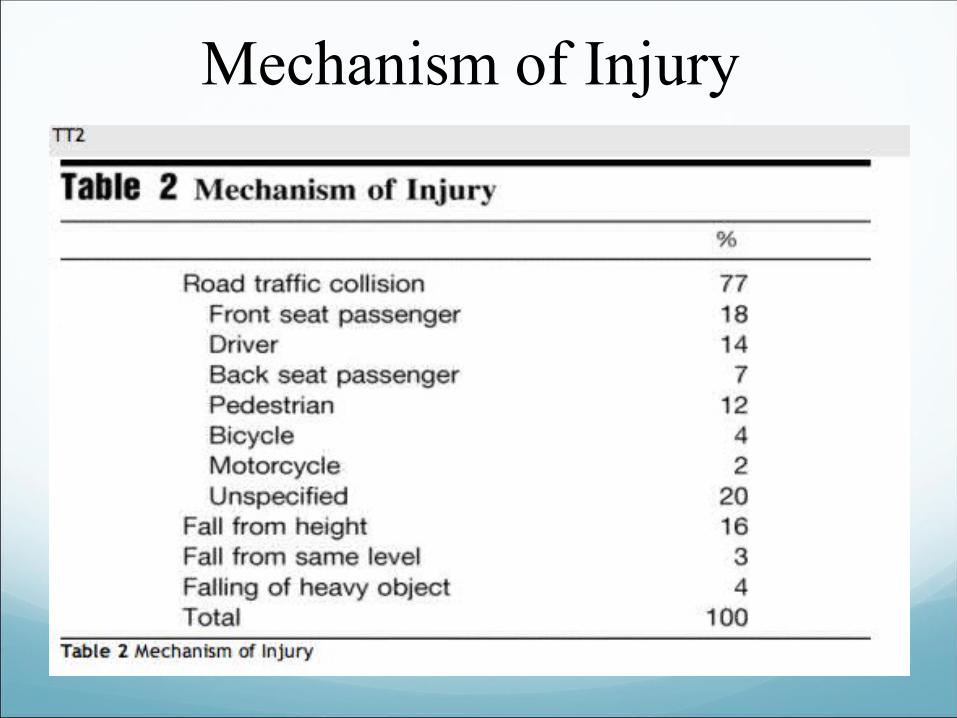
Mechanism of Injury
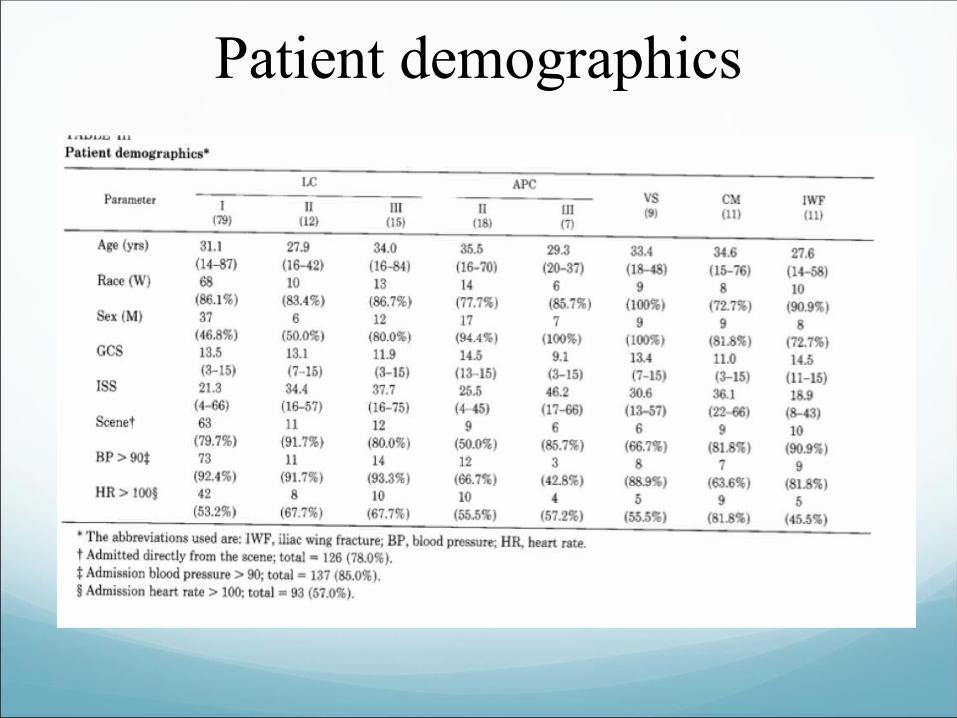
Patient demographics
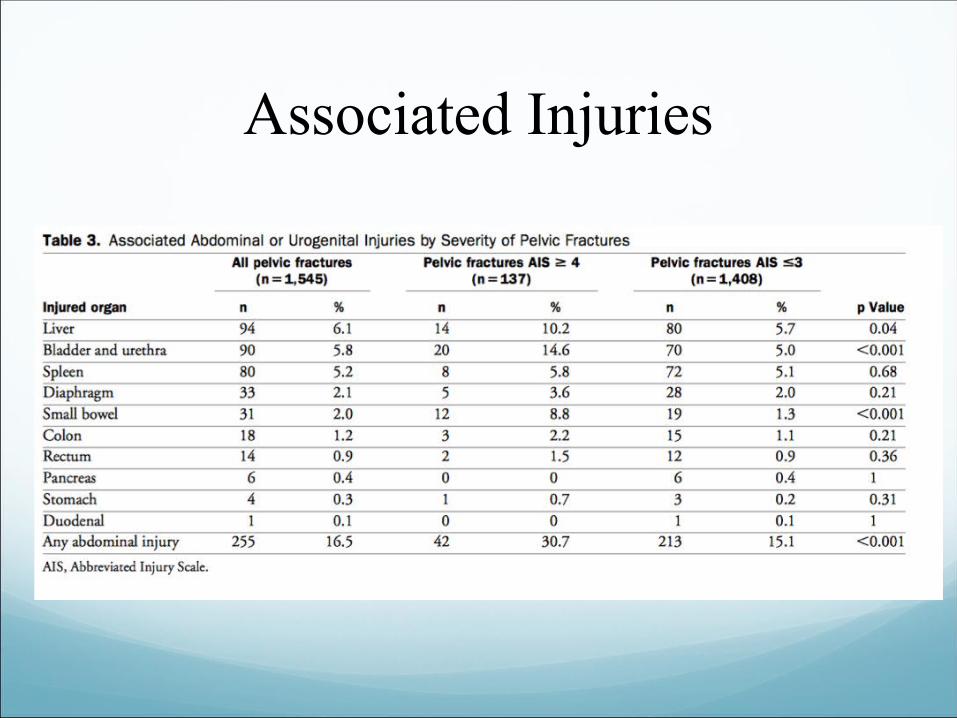
Associated Injuries
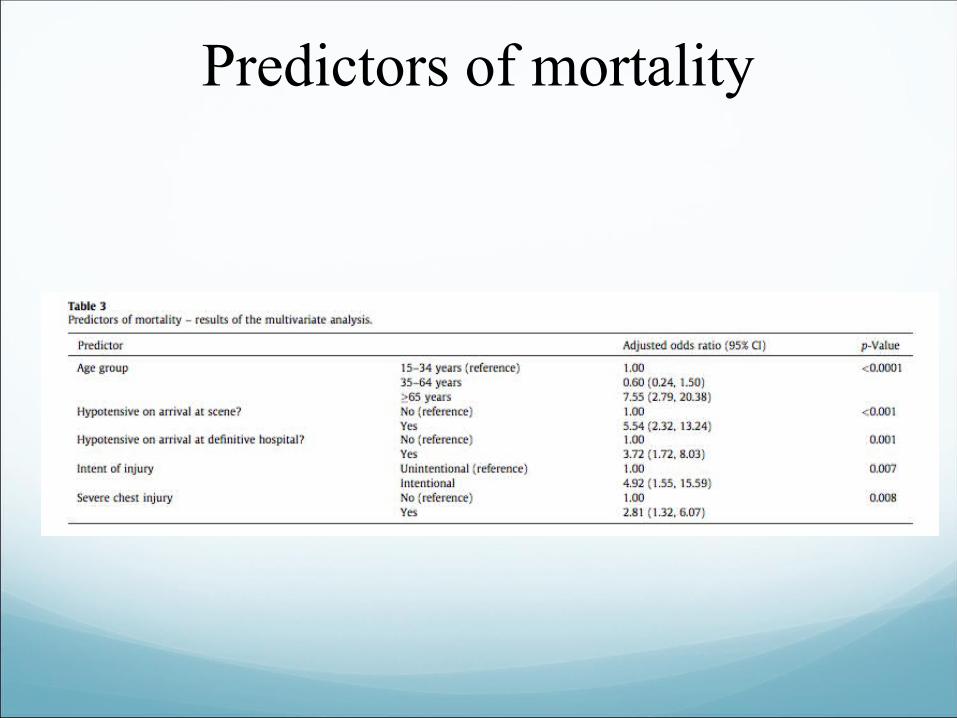
Predictors of mortality
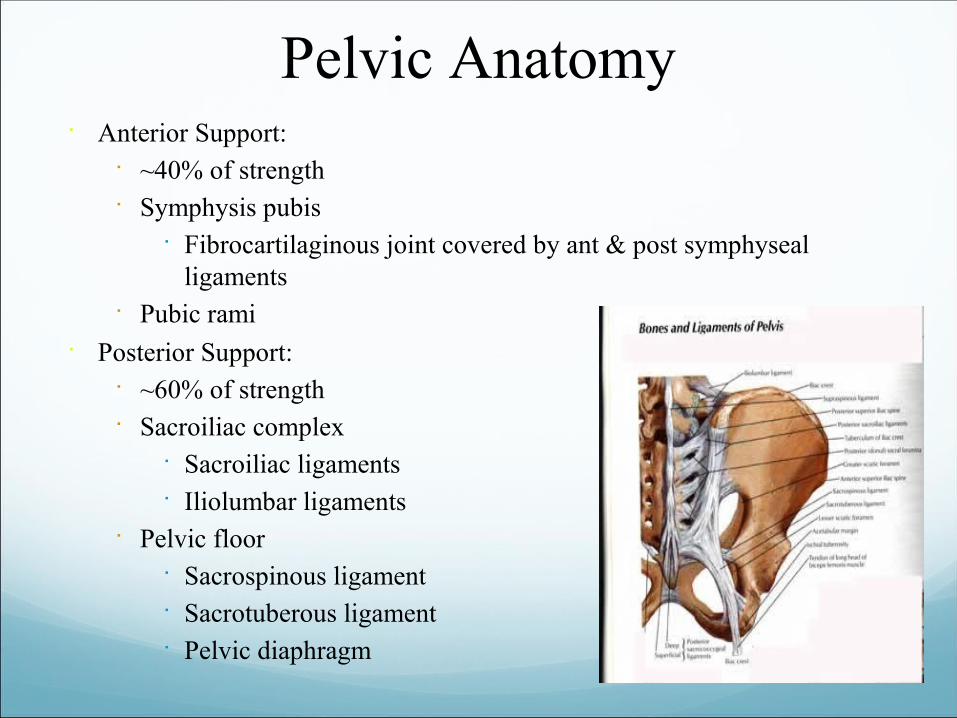
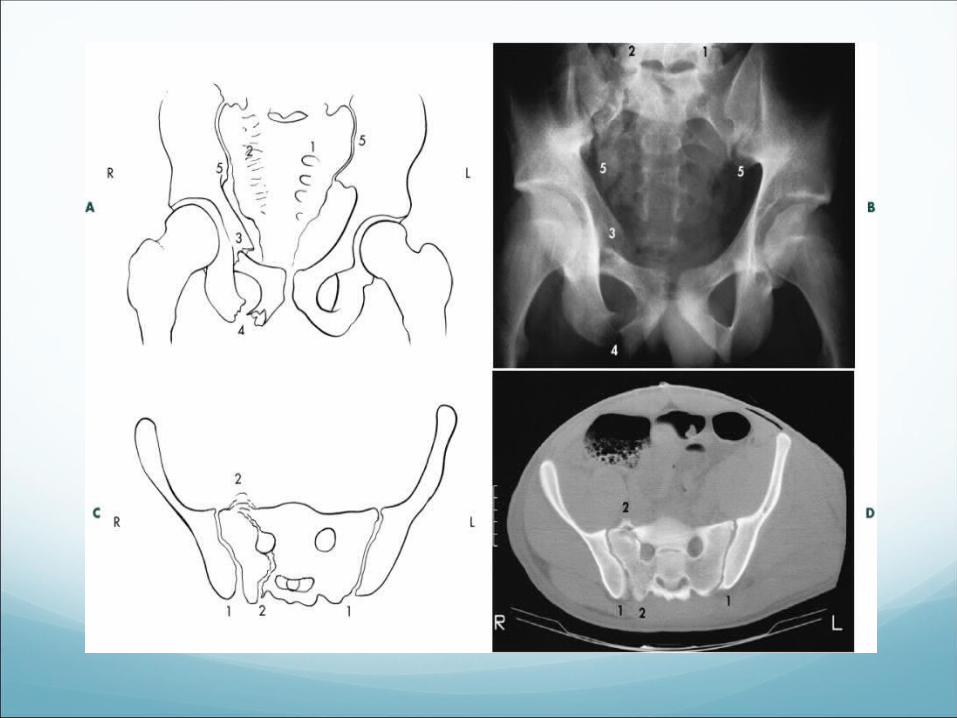
Pelvic Anatomy Anterior Support:
~40% of strength Symphysis pubis
Fibrocartilaginous joint covered by ant & post symphyseal ligaments
Pubic rami Posterior Support:
~60% of strength Sacroiliac complex
Sacroiliac ligaments Iliolumbar ligaments
Pelvic floor Sacrospinous ligament Sacrotuberous ligament Pelvic diaphragm
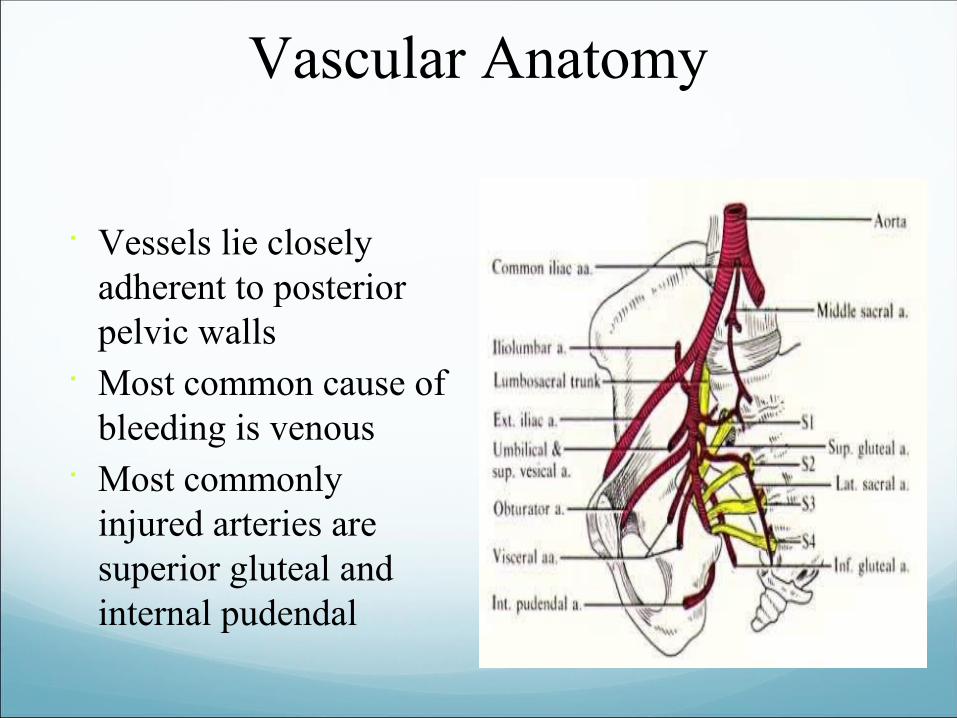
Vascular Anatomy
Vessels lie closely adherent to posterior pelvic walls
Most common cause of bleeding is venous
Most commonly injured arteries are superior gluteal and internal pudendal
History & Physical ABC’s & initial stabilization AMPLE Hx
Most important feature is mechanism Destot’s sign:
Hematoma above inguinal ligament or scrotum Grey-Turner’s sign Earle’s sign:
Presence of bony prominence, palpable hematoma, or tender # line on DRE
Blood at urethral meatus / vaginal introitus Examine pelvis only once
Sensitivity of exam 93% vs. 87% for AP pelvis Gonzalez et al. J Am Coll Surg. 2002; 194: 121-5
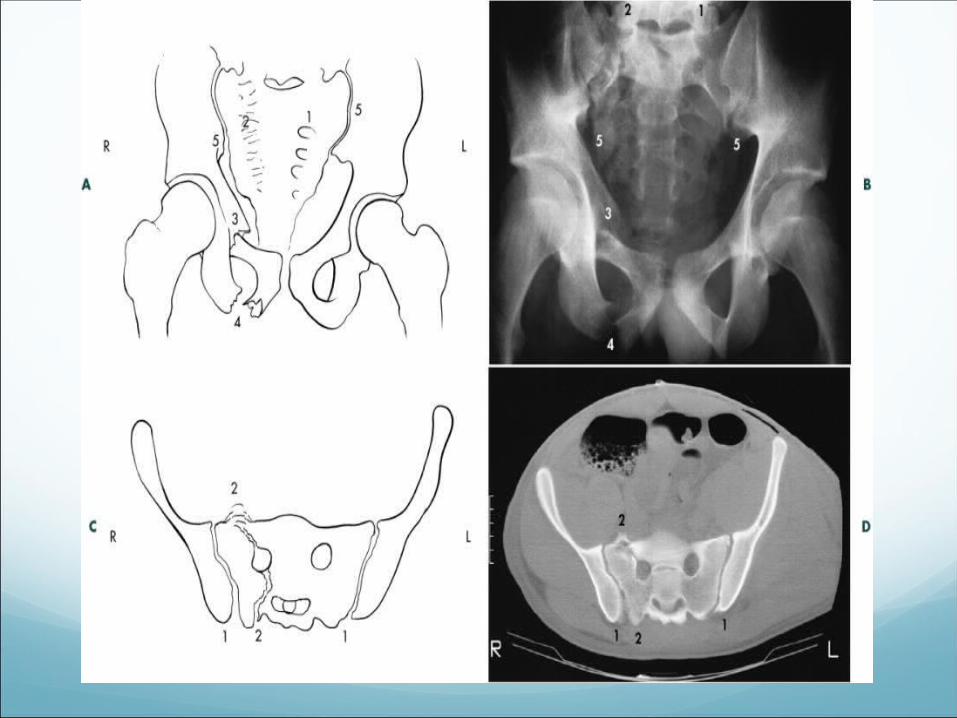
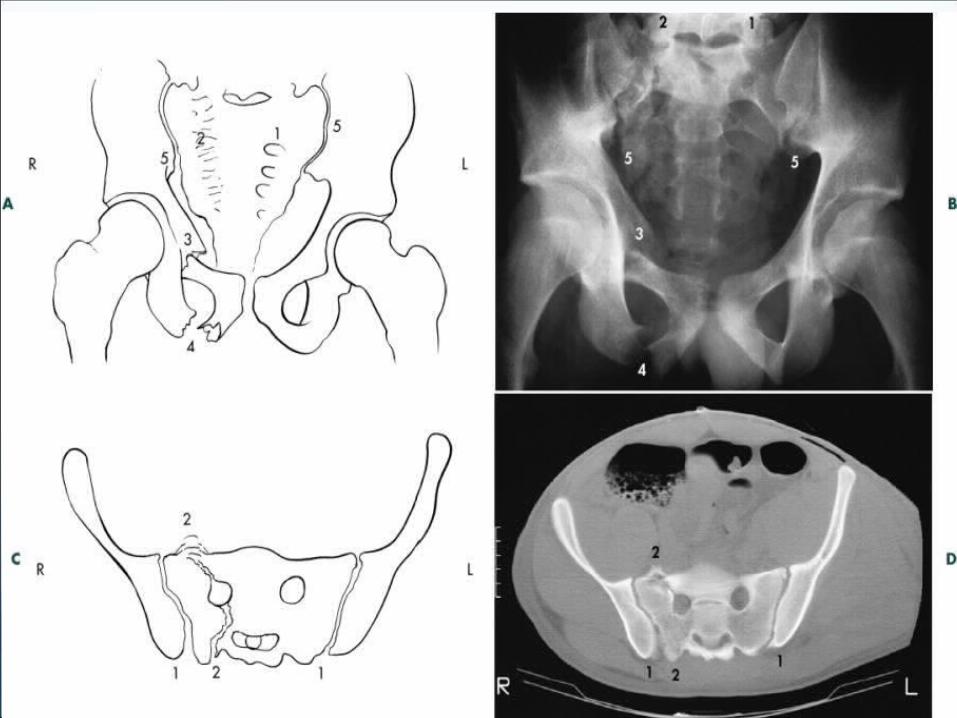
Imaging Plain films
AP Inlet view / Outlet view Judet view (oblique)
AP alone ~90% sensitive; combined w/ inlet / outlet views ~94% sensitive
Limited in ability to clearly delineate posterior injuries Pelvic films are NOT necessary in pts with normal physical exam +
GCS >13 At least one study shows clinical exam reliable in EtOH
Gonzalez et al. J Am Coll Surg. 2002; 194: 121-5
CT scans Evaluates extent of posterior injury better Superior imaging of sacrum and acetabulum More detailed info about associated injuries
FAST/CT/Total Body CT
• Initial clinical experience with a 64-MDCT whole-body scanner in an emergency department: better time management and diagnostic quality
• Rieger, Michael MD; Czermak, Benedikt MD; El Attal, Rene MD; Sumann, Günther MD; Jaschke, Werner MD; Freund, Martin MD
• Journal of Trauma volume 66-3 march 2007 648-657
Classification Systems: Most common are Tile and Young systems Tile Classification system:
Advantages Comprehensive Predicts need for operative intervention
Disadvantages Does NOT predict morbidity or mortality
Young Classification System: Advantages
Based on mechanism of injury predicts associated injury Estimates mortality
Disadvantages Excludes more minor injuries
Classifications and the Risk of Bleeding
• Young-Burgess classification has less inter and inter-observer reliability
• It is well correlated with the mechanism, the amount of energy, the concomitant injuries and transfusion requirements
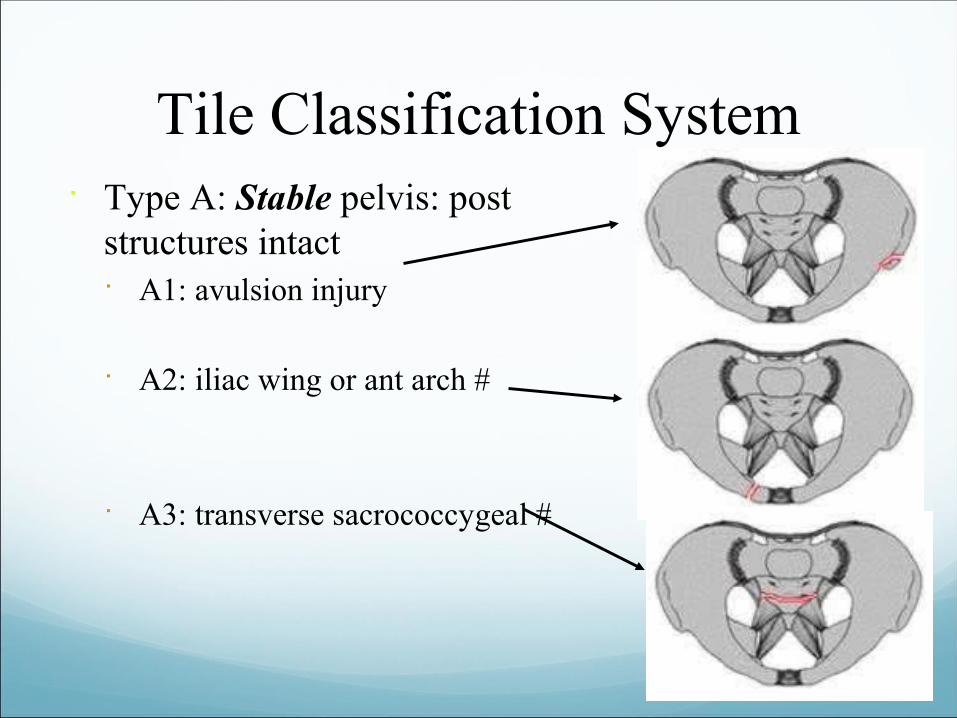
Tile Classification System Type A: Stable pelvis: post
structures intact A1: avulsion injury
A2: iliac wing or ant arch #
A3: transverse sacrococcygeal #
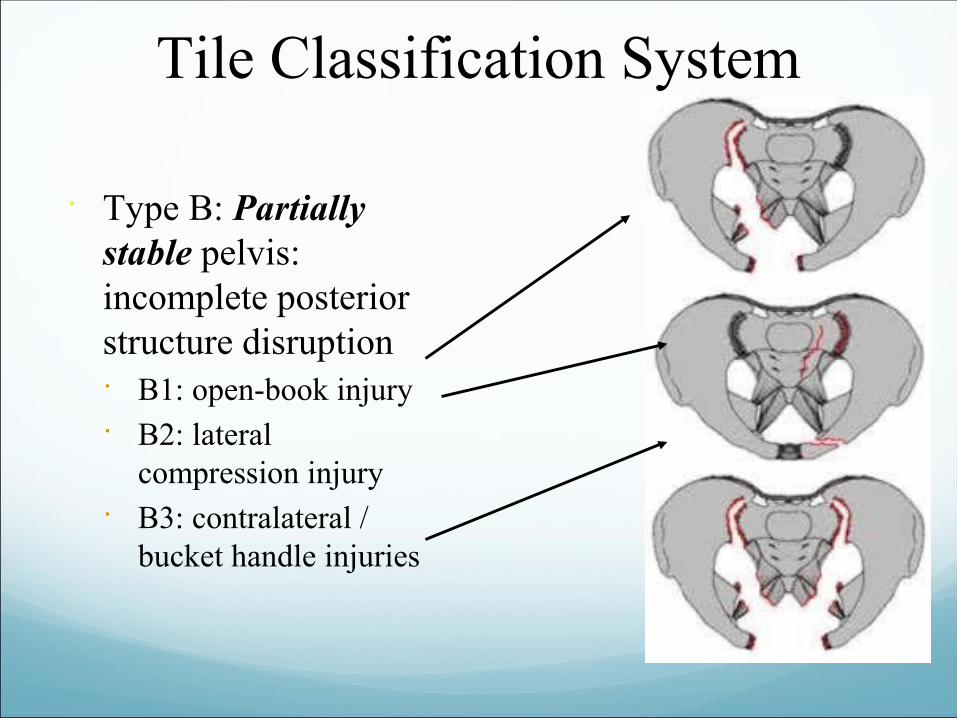
Tile Classification System
Type B: Partially stable pelvis: incomplete posterior structure disruption B1: open-book injury B2: lateral
compression injury B3: contralateral /
bucket handle injuries
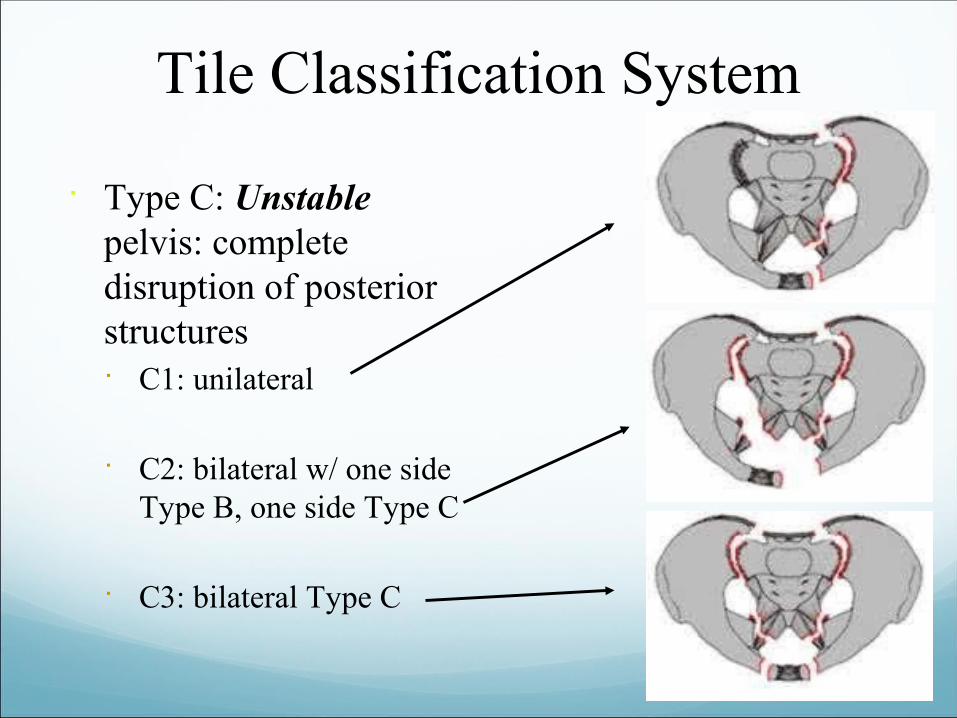
Tile Classification System
Type C: Unstable pelvis: complete disruption of posterior structures C1: unilateral
C2: bilateral w/ one side Type B, one side Type C
C3: bilateral Type C
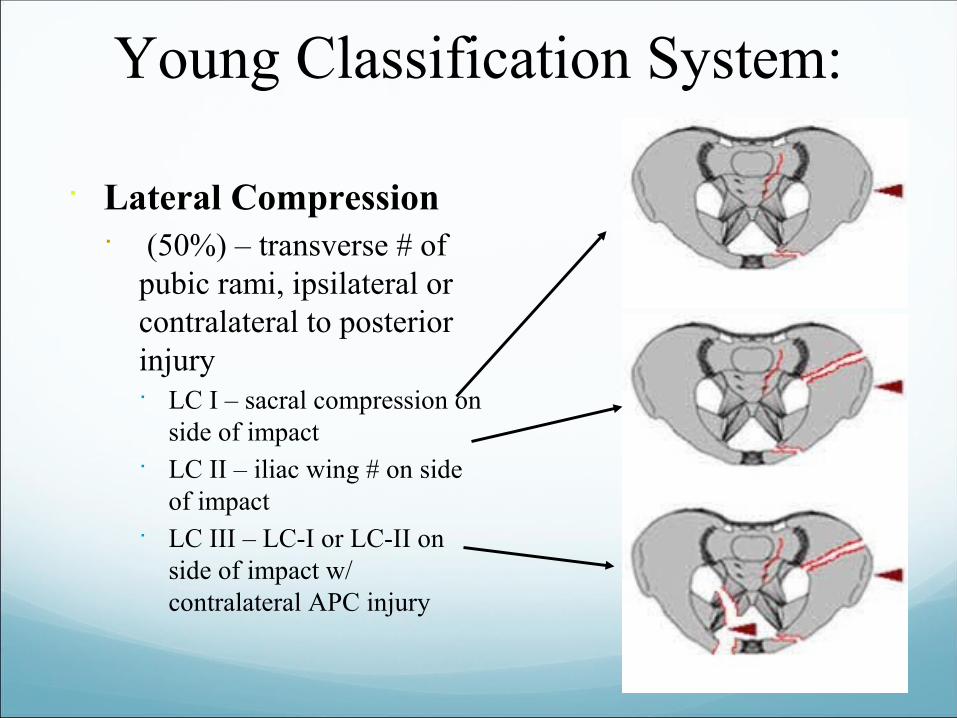
Young Classification System:
Lateral Compression (50%) – transverse # of
pubic rami, ipsilateral or contralateral to posterior injury LC I – sacral compression on
side of impact LC II – iliac wing # on side
of impact LC III – LC-I or LC-II on
side of impact w/ contralateral APC injury
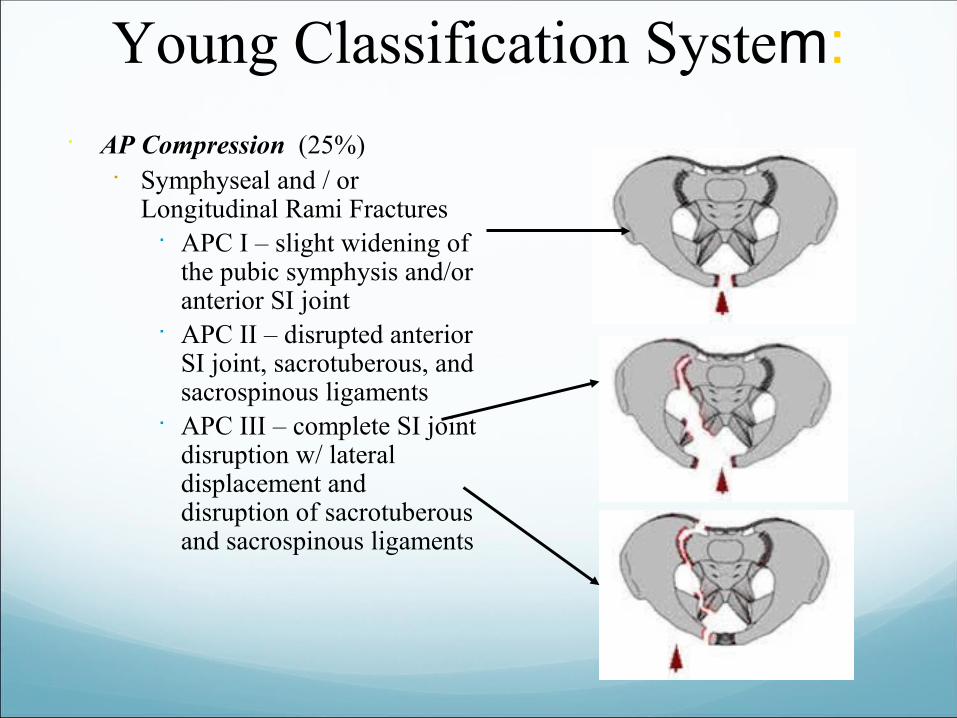
Young Classification System:
AP Compression (25%) Symphyseal and / or
Longitudinal Rami Fractures APC I – slight widening of
the pubic symphysis and/or anterior SI joint
APC II – disrupted anterior SI joint, sacrotuberous, and sacrospinous ligaments
APC III – complete SI joint disruption w/ lateral displacement and disruption of sacrotuberous and sacrospinous ligaments
Young Classification System: Vertical Shear (5%)
Symphyseal diastasis or vertical displacement anteriorly and posteriorly
Combined Mechanism Combination of injury patterns
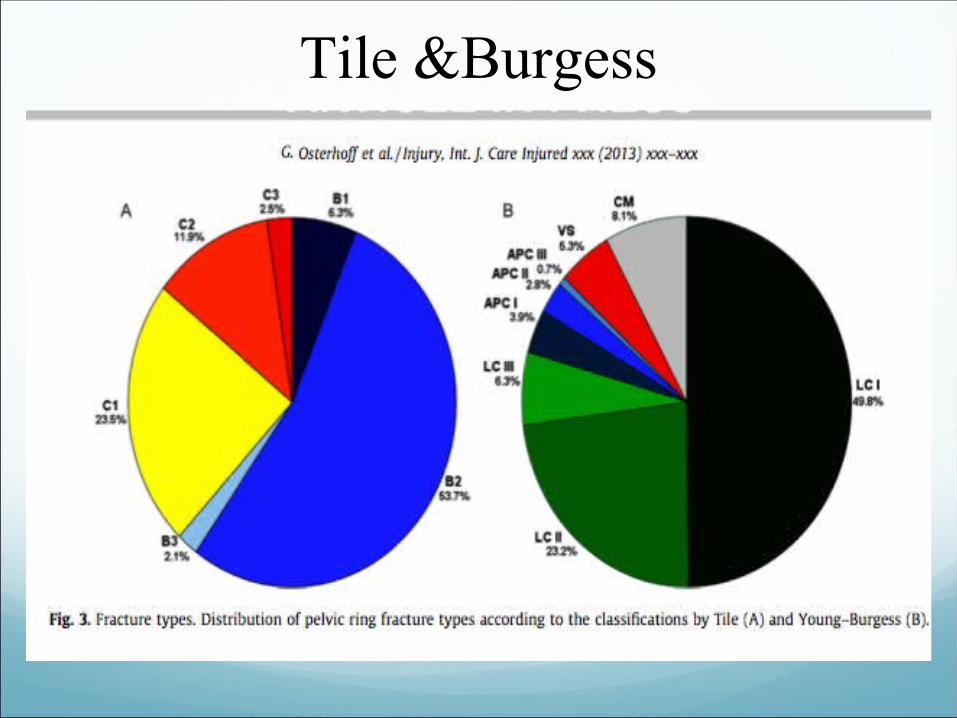
Tile &Burgess
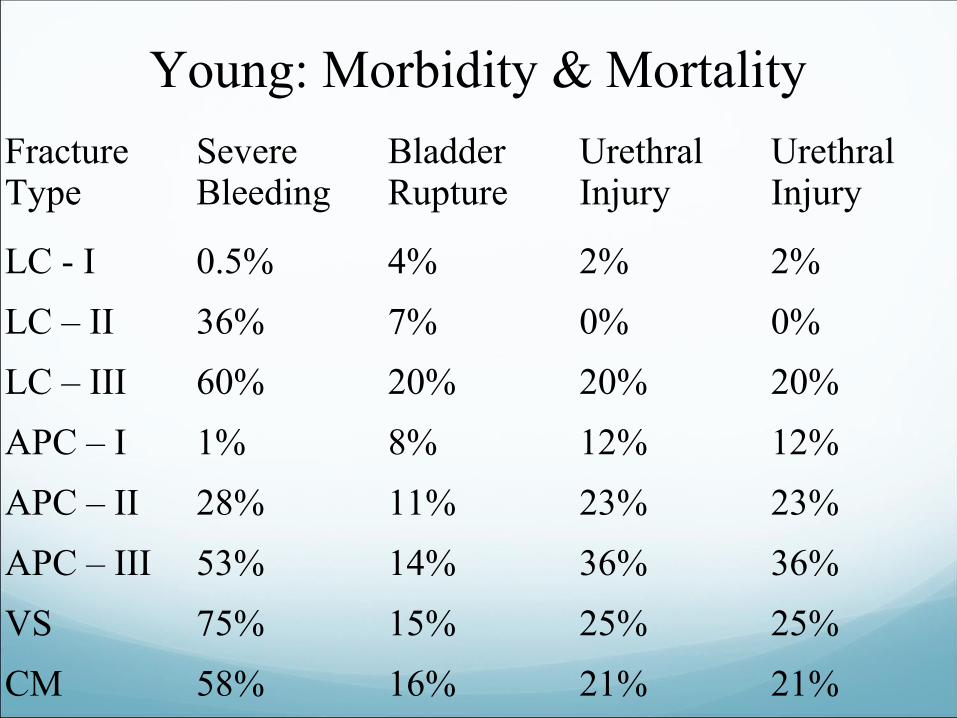
Young: Morbidity & Mortality
Fracture Type
Severe Bleeding
Bladder Rupture
Urethral Injury
Urethral Injury
LC - I 0.5% 4% 2% 2%
LC – II 36% 7% 0% 0%
LC – III 60% 20% 20% 20%
APC – I 1% 8% 12% 12%
APC – II 28% 11% 23% 23%
APC – III 53% 14% 36% 36%
VS 75% 15% 25% 25%
CM 58% 16% 21% 21%
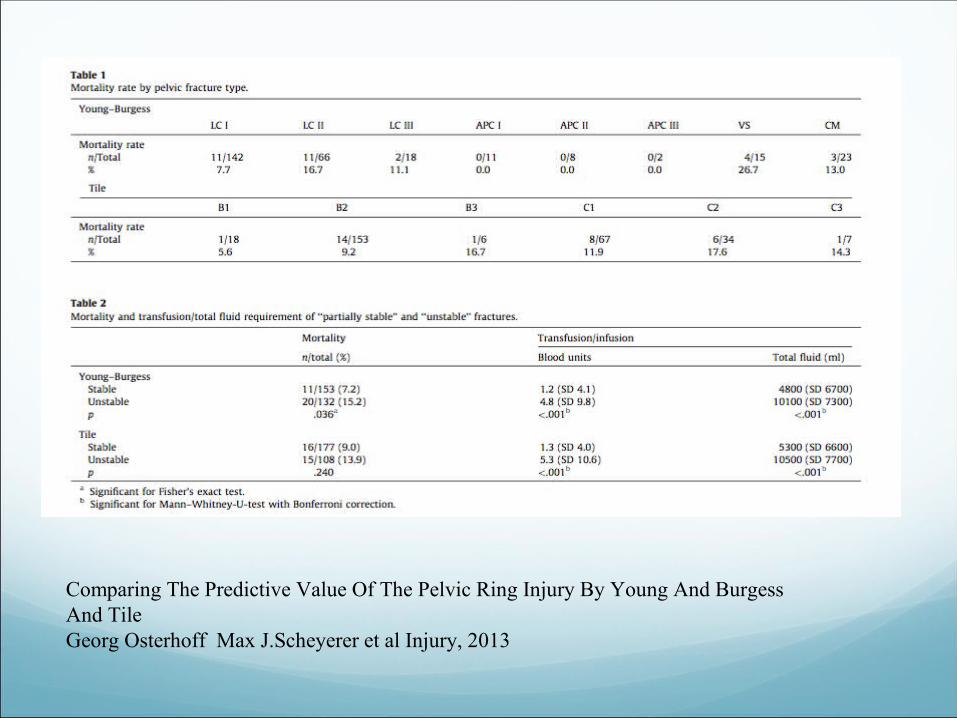
Comparing The Predictive Value Of The Pelvic Ring Injury By Young And Burgess And TileGeorg Osterhoff Max J.Scheyerer et al Injury, 2013
Immediate Action
• During primary survey pelvic binders should be used despite the fact there is no conclusive evidence from the literature to support these binders decrease the need for transfusion, embolization and improve mortality rates but they decrease the pelvic volume.
• Prolonged use can cause trochanteric ulcers, also the secondary survey is difficult while the binder is on.
Chesser T.J,Cross AM,(the use of pelvic binders in the emergent management of potential pelvic trauma Injury2012,43:667-9
Ghaemmaghami V,Sperry J.Friese R,et al .effects of early use of external pelvic compression on transfusion requirements and mortality in pelvic fractures.American Journal of surgery 2007:204:935-9.
Sources Of Bleeding
• Arteries,veins,cancellous bone
• Retroperitoneal haematoma - up to 4 liters mostly from venous plexus and cancellous fractured bone
• Damage control resuscitation is to keep the patient hypotensive and prevent (coagulopathy,acidosis and hypothermia)
• Permissive resuscitation is to keep SBP at 90 mmhg and thus preventing excessive exsanguination and at the same time organs are perfused
• Several questions need to be answered since there is no evidence supporting this strategy
Resuscitation
• Packed RBCS,FFP and platelets
• The optimal ratio of these components is still under research
• Supporting the fibrinolytic system is achieved by giving tranexamic acid
• Military application of TXA in trauma emergency,Archives Of Surgery 2012:147:113-9
Physical Exam
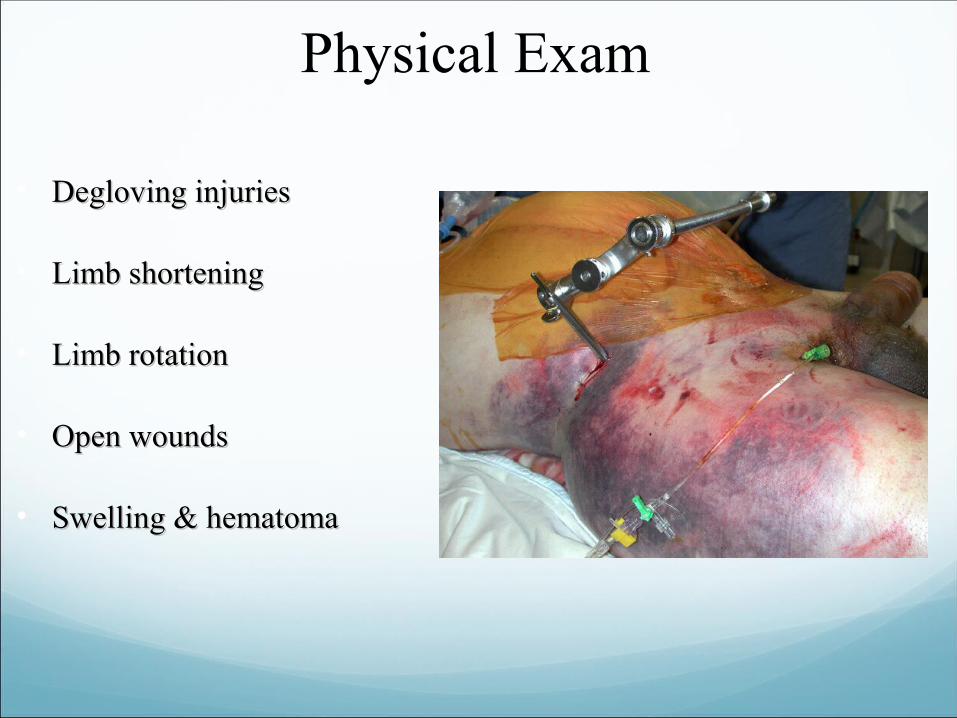
• Degloving injuriesDegloving injuries
• Limb shorteningLimb shortening
• Limb rotationLimb rotation
• Open woundsOpen wounds
• Swelling & hematomaSwelling & hematoma
Clinical Tips
• Presence of blood in the urethra
• Bleeding per vagina
• Edema of the labia
• Leak of urine from the rectum
Management Stable vs Unstable patient Stable pt:
Conservative Tx (bed rest slow wt bearing) Tile: A1, A2, A3 (coccyx #’s only) Young: APC – I, LC – I, some LC – II
Unstable pt: Tile B & C / Young APC & VS = high energy injuries Require surgical management Timing & methods for stabilization controversial
Management: Unstable Patient ABC’s, resuscitation Evaluate for site(s) of blood loss
FAST, CT Laparotomy if indicated
Options for patients not requiring laparotomy: Sheet around pelvis. External fixator. Early ORIF Angiographic embolization
Early antibiotics for open # (cefazolin & gent)
The Risk of Bleeding
• Metz et al demonstrated that APC are associated with posterior bleeding and LC with anterior bleeding.
• ISS and the associated injuries and not the fracture type have been found to represent a better mortality predictor
• the extravasation of iv contrast and the size of pelvic haematoma have been correlated to bleeding and the need for angiography
• Associated Injuries and Not Fracture Instability Predict Mortality in Pelvic Fractures: A Prospective Study of 100 Patients
• Lunsjo, Karl MD, PhD; Tadros, Ayman FRCS; Hauggaard, Anders MD; Blomgren, Rolf MD; Kopke, John MD; Abu-Zidan, Fikri M. MD, FRCS, PhD,-Journal of TraumaVol62(3)March 2007-pages 687-691.
Imaging
• Plain pelvis and chest radiographs ,FAST, selective CT(ATLS)
• Total body CT with split-dose IV contrast
• The effects of this approach comported to the conventional ATLS protocol has not been established
• Several studies have shown that time spent in CT is not a prohibiting factor in patient management in modern trauma centers and have emphasized the efficiency of total body CT
• Wumbte,Quaisser C,Balling et al.(Whole-body CT- improves trauma care in patients requiring surgery after multiple trauma )Emergency Medicine Journal: 2009:66:648-57.
Pelvic Ring Injuries
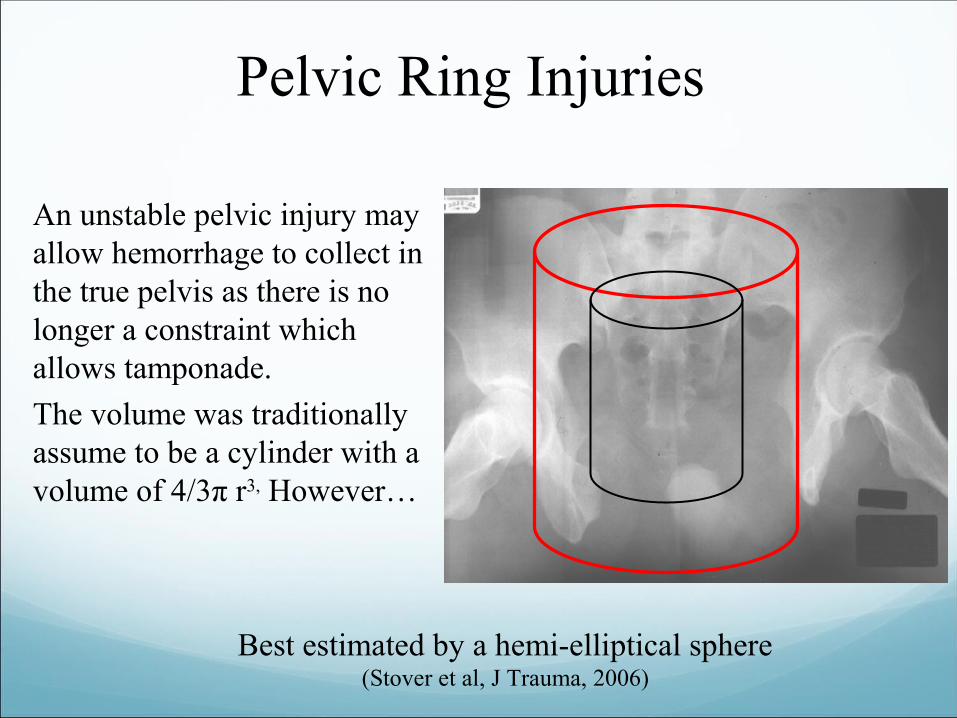
An unstable pelvic injury may allow hemorrhage to collect in the true pelvis as there is no longer a constraint which allows tamponade.
The volume was traditionally assume to be a cylinder with a volume of 4/3π r3, However…
Best estimated by a hemi-elliptical sphere(Stover et al, J Trauma, 2006)
Defining Pelvic Stability?
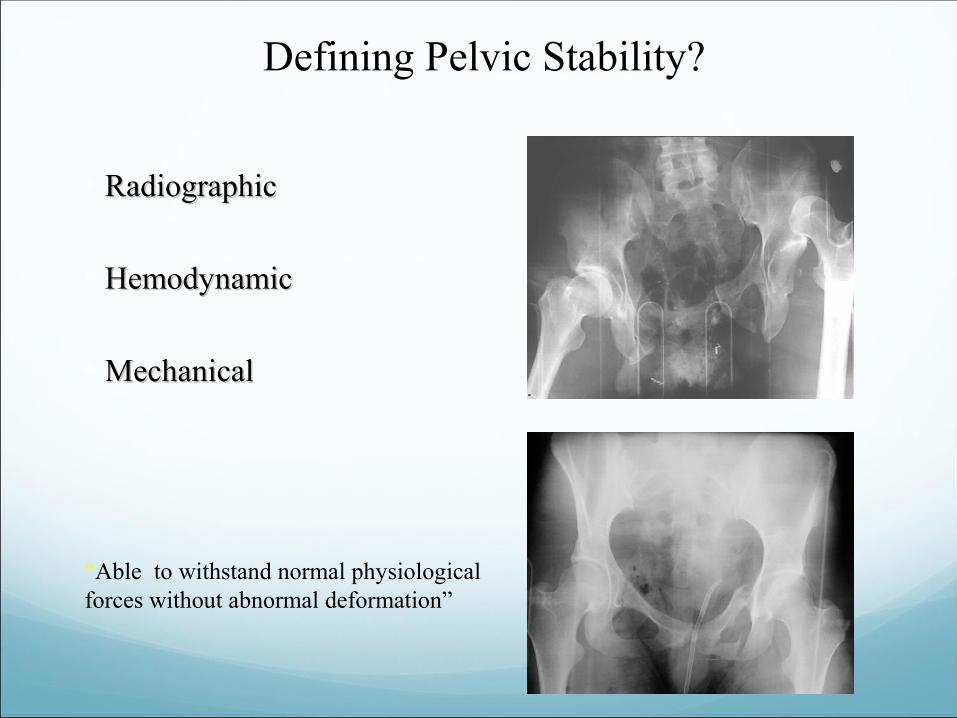
• RadiographicRadiographic
• HemodynamicHemodynamic
• MechanicalMechanical
“Able to withstand normal physiological forces without abnormal deformation”
Radiographic Signs of Instability
• Sacroiliac displacement of 5 mm in any Sacroiliac displacement of 5 mm in any planeplane
• Posterior fracture gap (rather than Posterior fracture gap (rather than impaction)impaction)
• Avulsion of fifth lumbar transverse Avulsion of fifth lumbar transverse process, lateral border of sacrum process, lateral border of sacrum (sacrotuberous ligament), or ischial spine (sacrotuberous ligament), or ischial spine (sacrospinous ligament)(sacrospinous ligament)
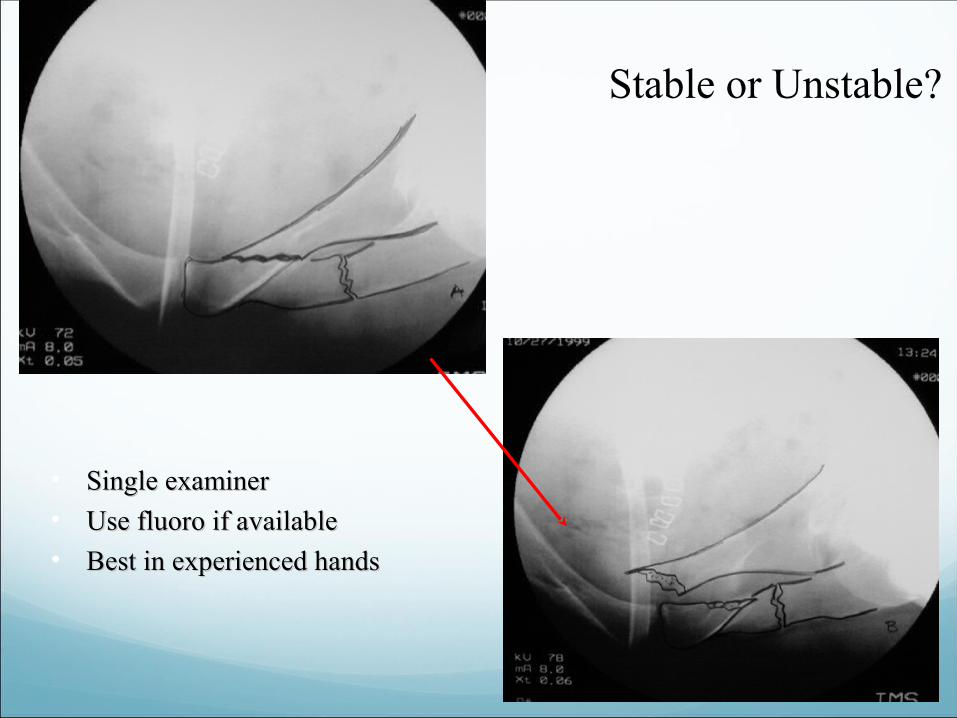
Stable or Unstable?
• Single examinerSingle examiner• Use fluoro if availableUse fluoro if available• Best in experienced handsBest in experienced hands
• External fixator device to the iliac crest easy to apply, but there is a risk of infection
• Pelvic c-clamp on the posterior ilium in the SIJ creates a tamponade effect (?Iliac fractures)
• Injuries to the superior gluteal neuromuscular bundle
• Internal fixation superior but time consuming (extremis)
• Direct surgical control theoretically easy - uncontrolled circumferential stitching and clip application with inadequate visualization may lead to iatrogenic nerve injuries
• Pelvic angiography and embolization
Shock VS Hemodynamic Instability
• Definitions ConfusingDefinitions Confusing
• Potentially based on multiple factors & measuresPotentially based on multiple factors & measures
• Lactate Lactate
• Base DeficitBase Deficit
• SBP < 90 mmHgSBP < 90 mmHg
• Ongoing drop in HematocritOngoing drop in Hematocrit
• Response to fluid challengeResponse to fluid challenge
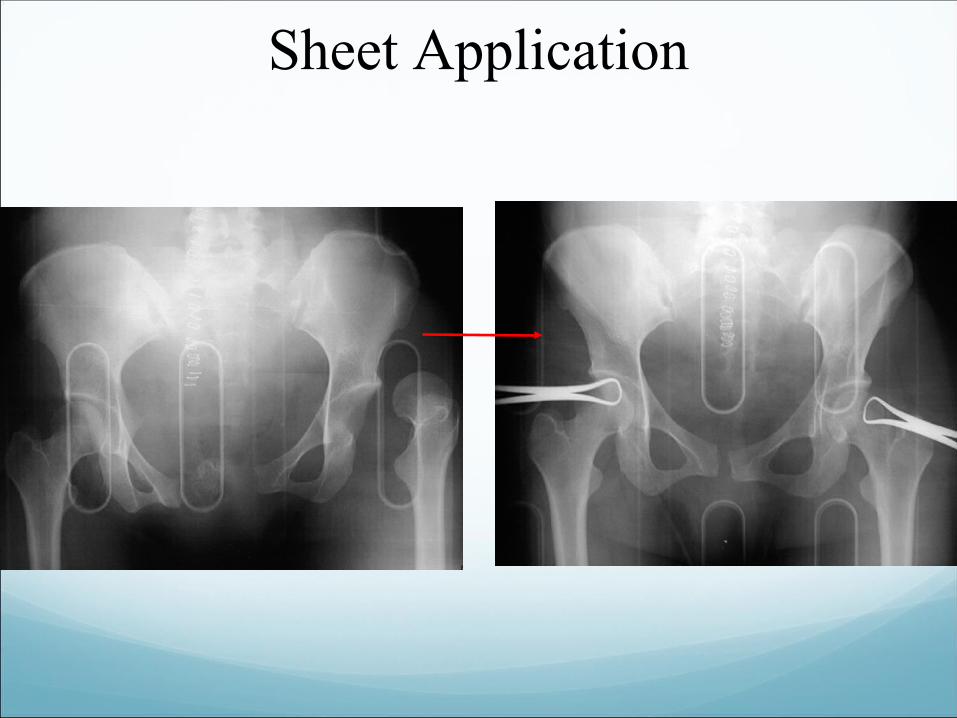
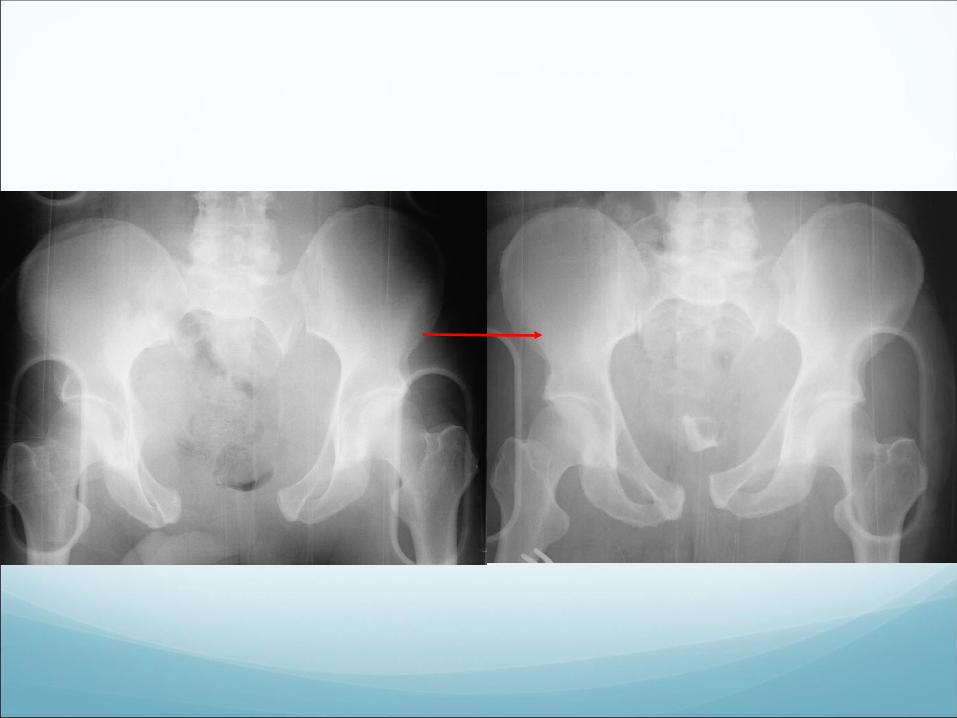
Sheet Application
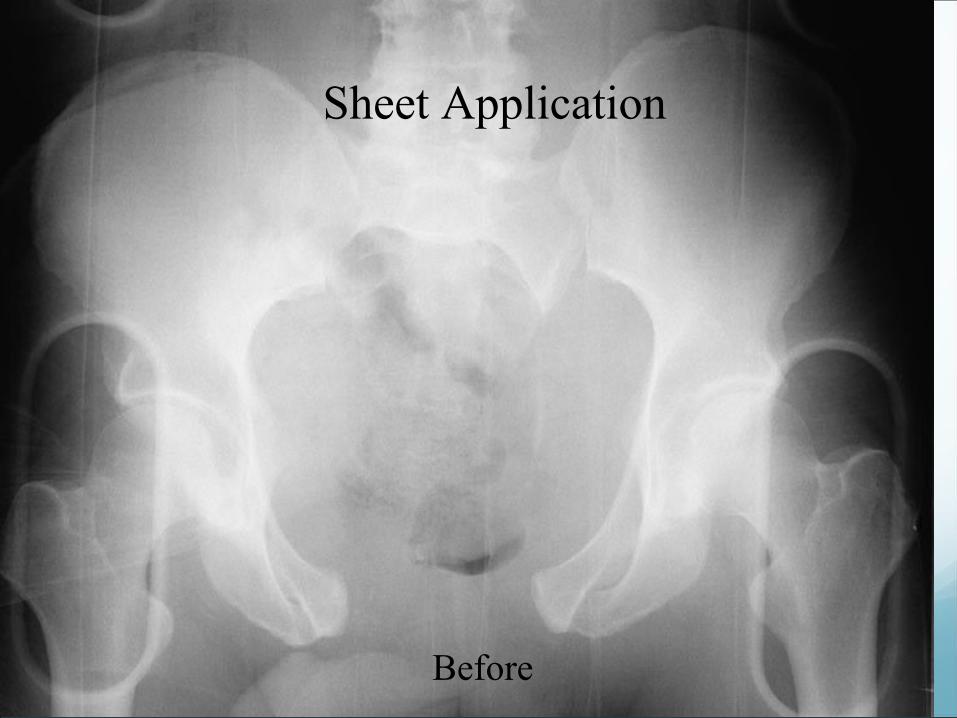
Sheet Application
Before

After
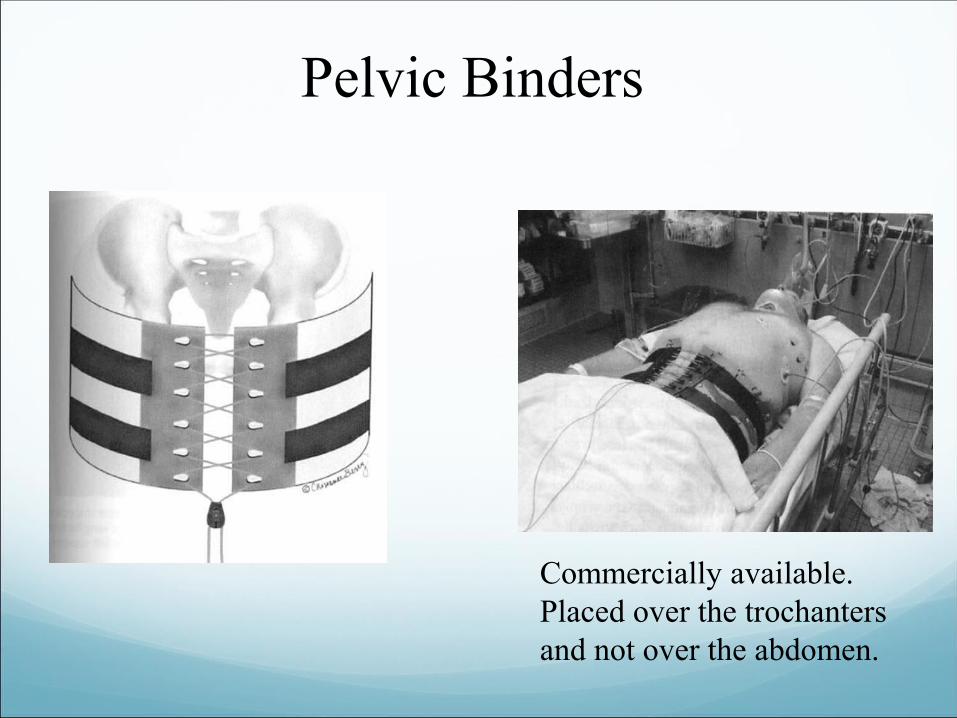
Pelvic Binders
Commercially available.Placed over the trochanters and not over the abdomen.
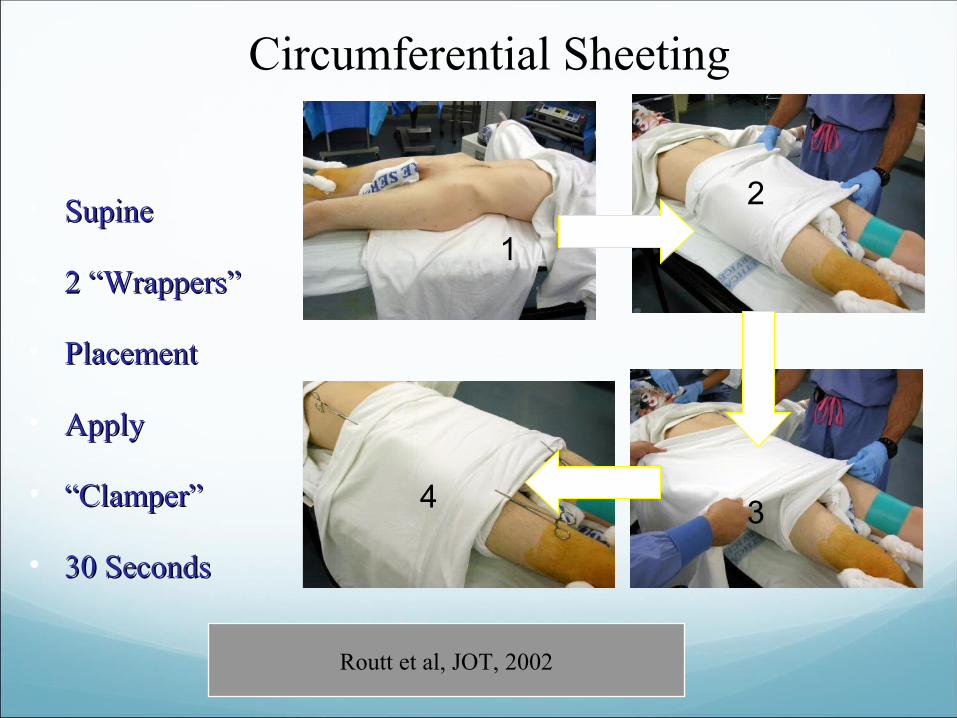
Circumferential Sheeting
• SupineSupine
• 2 2 “Wrappers”“Wrappers”
• PlacementPlacement
• ApplyApply
• ““Clamper”Clamper”
• 30 Seconds30 Seconds
1
2
34
Routt et al, JOT, 2002
Indications for External Fixation
• Resuscitative Resuscitative (hemorrhage control, (hemorrhage control, stability)stability)
• To decrease pain in To decrease pain in polytraumatized patients?polytraumatized patients?
• As an adjunct to ORIFAs an adjunct to ORIF
• Definitive treatment (Rare!)Definitive treatment (Rare!)• Distraction frameDistraction frame• CanCan’t ORIF the pelvis’t ORIF the pelvis
Theoretical and a marginal indication, but there is literature support
Barei, D. P.; Shafer, B. L.; Beingessner, D. M.; Gardner, M. J.; Nork, S. E.; and Routt, M. L.: The impact of open reduction internal fixation on acute pain management in unstable pelvic ring injuries. J Trauma, 68(4): 949-53, 2010.
External Fixation
LocationLocation
AIIS
ASIS
C-clamp
Clinical Application
Resuscitative
Augmentative
Definitive
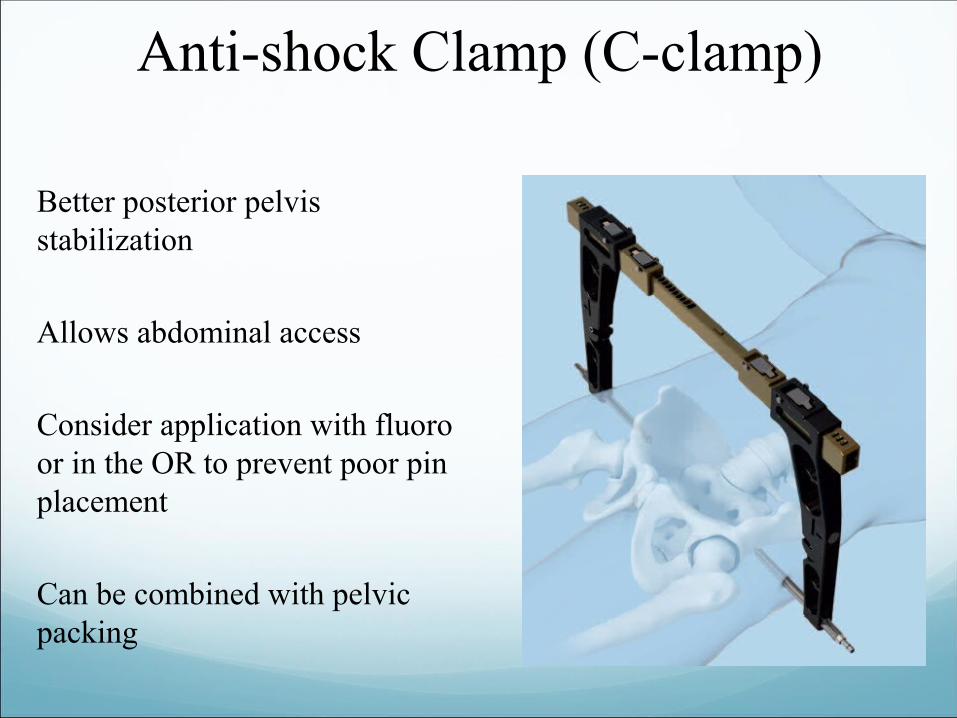
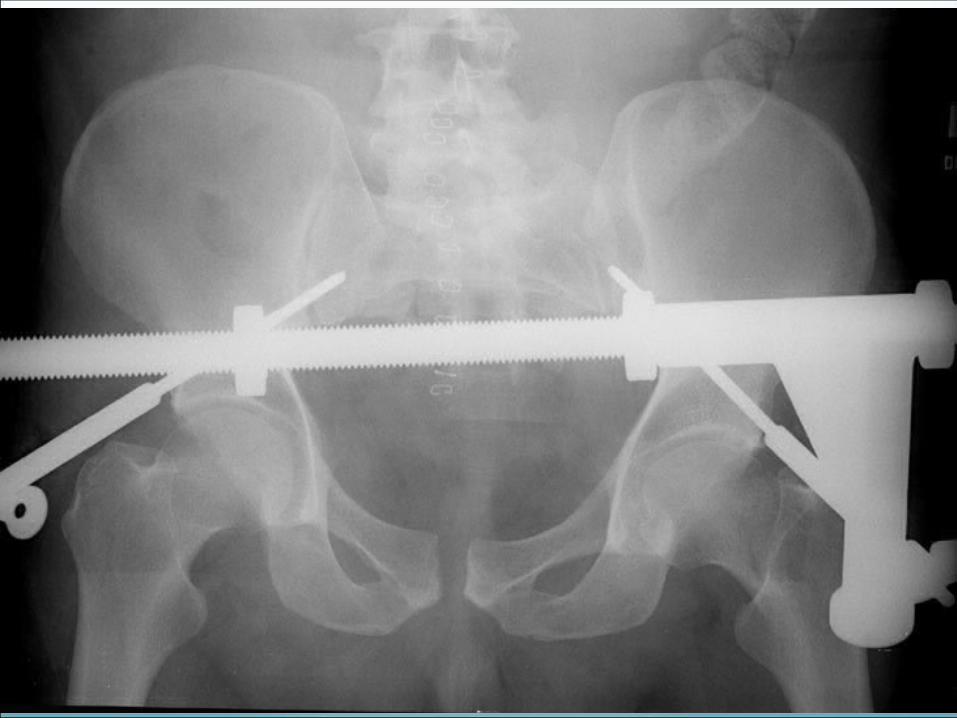
Anti-shock Clamp (C-clamp)
Better posterior pelvis stabilization
Allows abdominal access
Consider application with fluoro or in the OR to prevent poor pin placement
Can be combined with pelvic packing




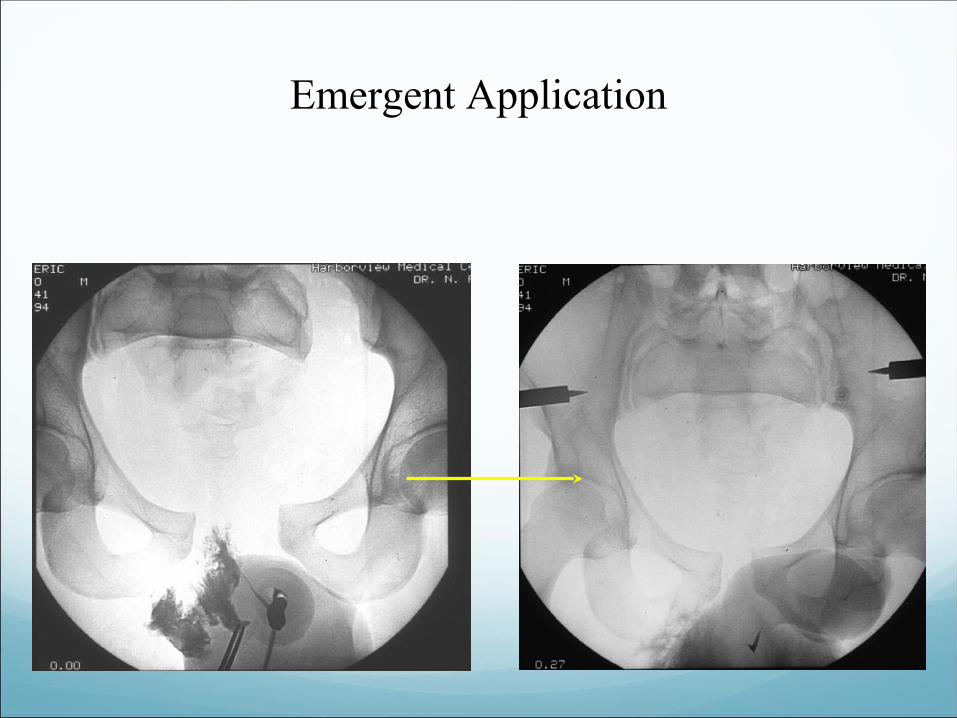
Emergent Application
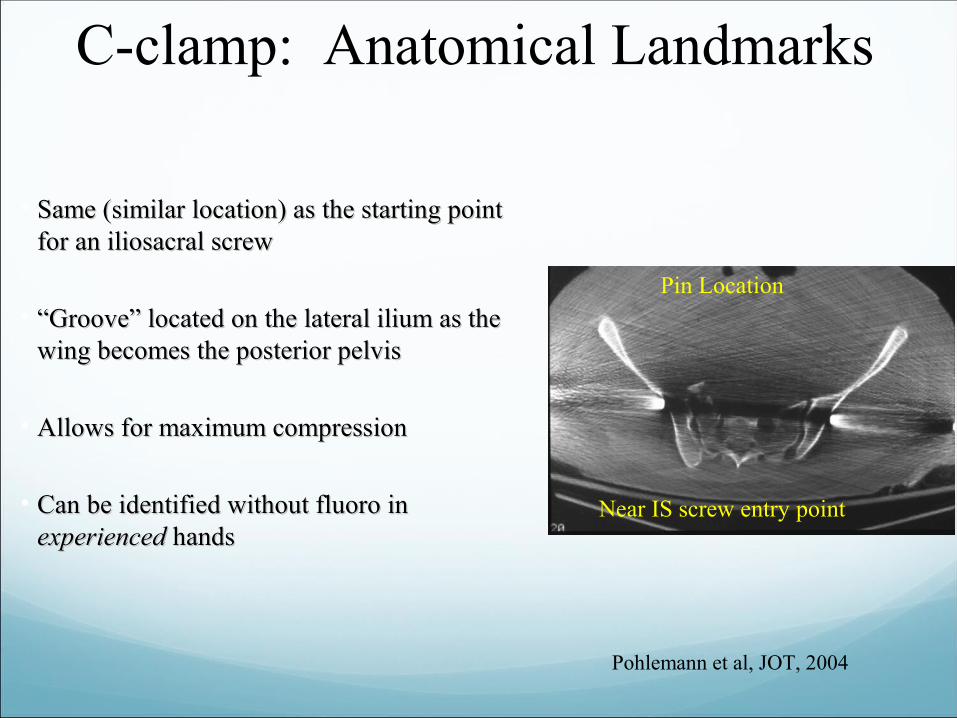
C-clamp: Anatomical Landmarks
• Same (similar location) as the starting point Same (similar location) as the starting point for an iliosacral screwfor an iliosacral screw
• ““Groove” located on the lateral ilium as the Groove” located on the lateral ilium as the wing becomes the posterior pelviswing becomes the posterior pelvis
• Allows for maximum compressionAllows for maximum compression
• Can be identified without fluoro in Can be identified without fluoro in experiencedexperienced hands hands
Pohlemann et al, JOT, 2004
Pin Location
Near IS screw entry point
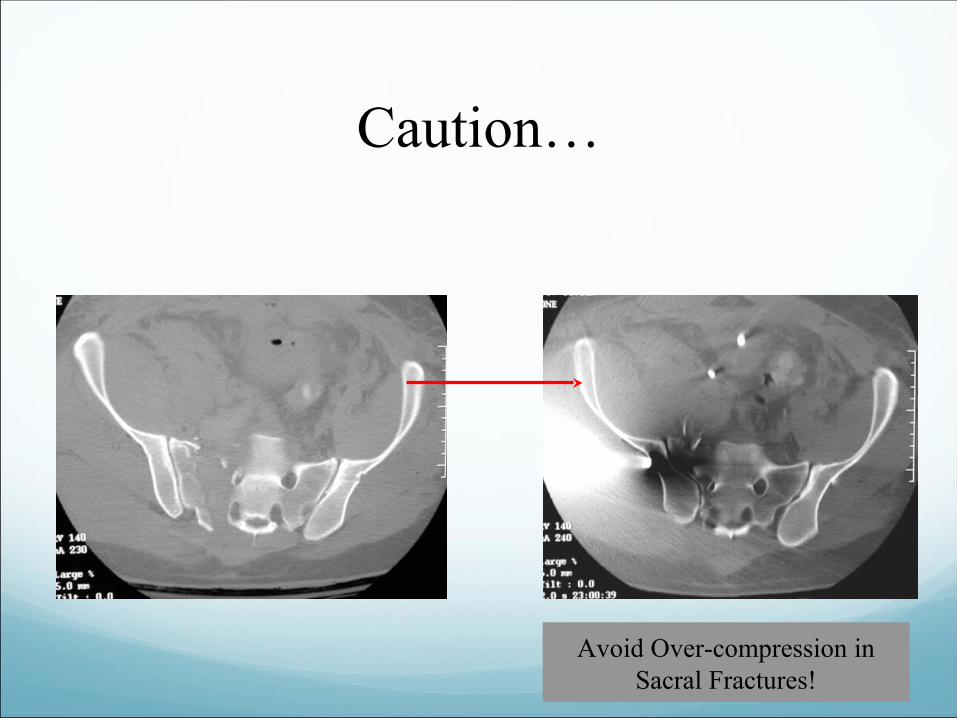
Avoid Over-compression in Sacral Fractures!
Caution…
Control Of Bleeding
•The use of a sacroiliac screw has been reported by Gardner as having a resuscitation role (the anti-shock iliosacral screw-Journal Of Orthopaedic Trauma 2010-24:e86-9)
•The best means to control haemorrhage after skeletal stabilization is a subject of a vivid debate!!!!!
•According to Gullinane DC, and co-workers in their systemic review (Journal Of Trauma 2011:71:1850-68) arterial embolization should be strongly recommended:
Role of Angio
•Valuable for arterial onlyValuable for arterial only
•Estimated at 5-15%Estimated at 5-15%
•Timing (early vs late?)Timing (early vs late?)
•Institution dependentInstitution dependent
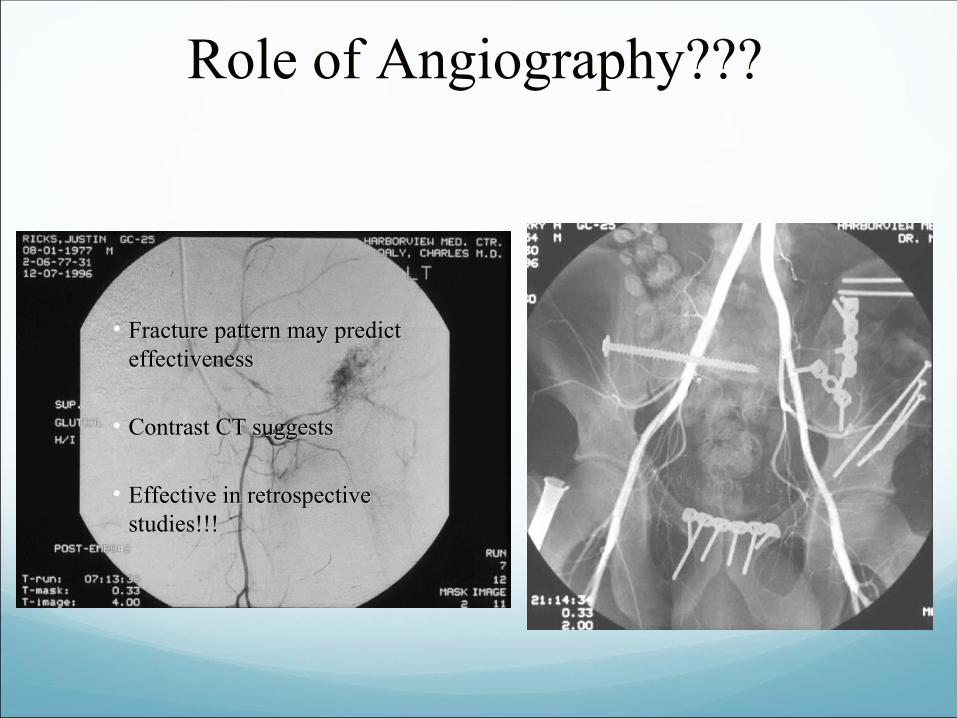
Role of Angiography???
• Fracture pattern may predict Fracture pattern may predict effectivenesseffectiveness
• Contrast CT suggestsContrast CT suggests
• Effective in retrospective Effective in retrospective studies!!!studies!!!
Complications of AE
Gluteal claudication
Pelvic Necrosis
Renal failure
Although effective in controlling bleeding (arterial)but published series didn’t show decrease in necessity for blood product resuscitation
Clay C Burley 2011 American College of Surgeons
Preperitoneal Pelvic Packing
In Europe (PPP/EF),
2011,Clay C Burlew et al (75 out of 1,245) concluded that this method eliminates the question of OR and IR.
Concurrent operations can be done fixed
Less than 15% require angio-embolization
AE should be complementary procedure for life threatening haemorrhage control following PPP/EF
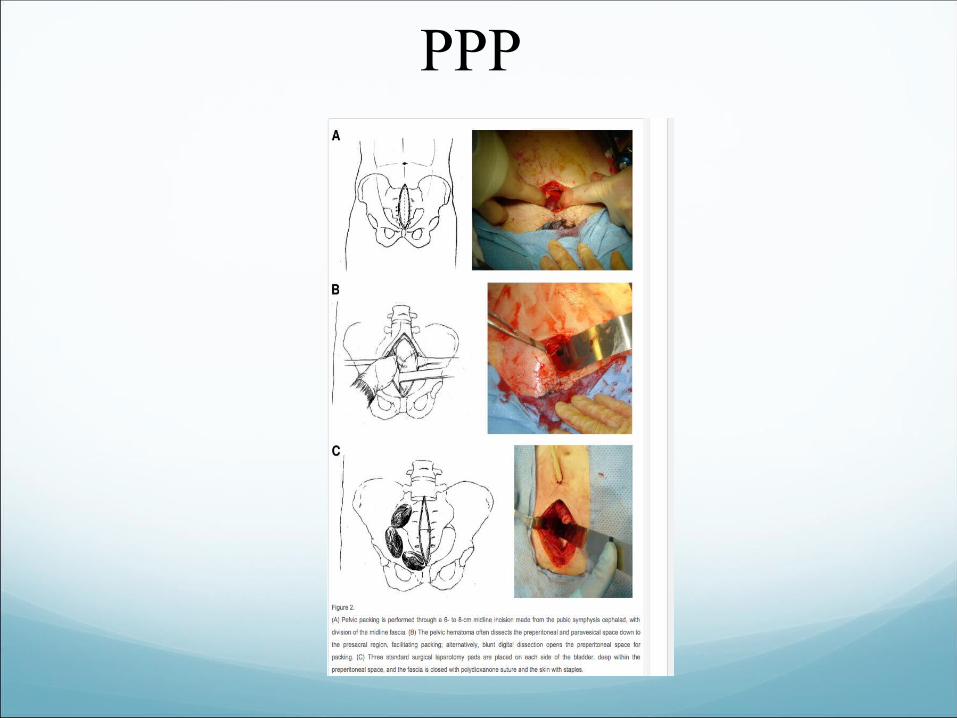
PPP
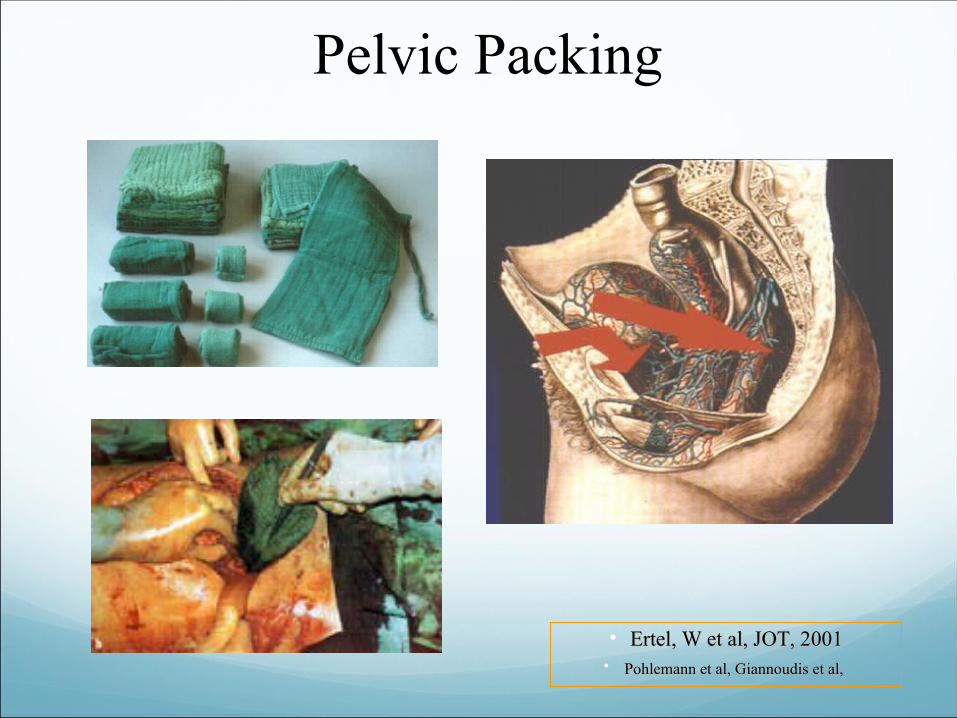
Pelvic Packing
• Ertel, W et al, JOT, 2001Ertel, W et al, JOT, 2001• Pohlemann et al, Giannoudis et al,Pohlemann et al, Giannoudis et al,
Summary
• Play well with others (general surgery, urology, interventional Play well with others (general surgery, urology, interventional radiology, neurosurgery)radiology, neurosurgery)
• Understand the fracture patternUnderstand the fracture pattern
• Do something (sheet, binder, ex fix, c-clamp) call OR/IR .Do something (sheet, binder, ex fix, c-clamp) call OR/IR .
• Combine knowledge of the fracture, the patients condition, and the Combine knowledge of the fracture, the patients condition, and the physical exam to decide next stepsphysical exam to decide next steps














![Clinical Study Dialysis Complications in AKI Patients ...downloads.hindawi.com/journals/bmri/2014/153626.pdf · management of haemodynamically unstable patients with AKI [ , ]. Its](https://img.pdfslide.net/doc/110x75/5ed3b21e7f3dc53cc40caeae/clinical-study-dialysis-complications-in-aki-patients-management-of-haemodynamically.jpg)