Embed Size (px)
DESCRIPTION
thumb deformity and hypoplasia
Citation preview

Thumb Hypoplasia
Ashraf Abdelaziz MD
Lecturer of orthopedic surgery
Hand and reconstructive surgery
Alzhraa University Hospital
Al-Azhar university
2014

Review
Introduction
Classification
Clinical Examination
Management

Introduction
Congenital thumb hypoplasia
frequently associated with partial or
complete absence of the radius
Epidemiology
◦ 4.6% of congenital deformities consist of
thumb hypoplasia
◦ 1/100,000 live births
Male = female

Bilateral involvement in 60% of patients
The right thumb is more affected
Associated anomalies
◦ > 80% of patients have
associated anomalies including;
VACTERL syndrome
Holt-Oram syndrome
Thrombocytopenia absent radius (TAR)
Fanconi anemia

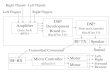
Classification (modified)Blauth classification 1967
I Minimal shortening and narrowing
II
Web space narrowing
Hypoplastic intrinsic thenar muscles
MCP joint instability
A: uniaxial B: Multiaxial
III
A
Type II +extrinsic tendon abnormalities,
Hypoplastic metacarpal , and stable
carpometacarpal
B
Type II + extrinsic tendon abnormalities, Partial
metacarpal aplasia , and unstable
carpometacarpal
IV Floating thumb
V Absent thumb


Buck-Gramcko incorporated soft-tissue
abnormalities in his classification of thumb
hypoplasia.
Lister subdivided Blauth grade II into IIA
and IIB, based on the stability of the MCP
joint; uniaxial or multiaxial.
The importance of Lister’s modification is
that with grade IIA, the MCP joint can be
reconstructed,

The most common type of thumb hypoplasia is type V
Buck-Gramcko modification of the Blauth classification
Hand Clin 1990

Type III B

Type III B

Type IV

Clinical examination
Careful upper limb examination
Passive motion of all joints.
Assessment of laxity of the collateral ligaments
of the interphalangeal (IP) joint and MCP .

Inspection
Extrinsic tendon abnormalities
Hypoplasia of thenar musculature
Absence of skin creases indicate tendon abnormalities
Excessive abduction of MCP joint
◦ Range of motion and instability
Ulnar collateral ligament laxity
Web-space tightness
◦ Evaluation for associated anomalies is essential.

Radiographs
◦ recommended views
bilateral films of hand, wrist and forearm

Studies
Labs
◦ Peripheral blood smear and CBC
important to rule out Fanconi anemia
Additional studies
◦ Chromosomal challenge test
detects Fanconi anemia before bone marrow failure

Treatment
Nonoperative
◦ Observation
Type I thumb hypoplasia.
Operative Management of the hypoplastic
thumb is determined by the grade of thumb
hypoplasia.

Opposition tendon transfer (Opponensplasty)
Type I hypoplasia with insufficient thumb abduction
Release of first web space, Opponensplasty,
and Stabilization of MCP joint
Type II and IIIA hypoplasia

Opponensplasty
An opponensplasty is the preferred to augment the deficient thenar muscles
The choice of donor tendon and pulley reconstruction is debatable
performed using
Flexor digitorum superficialis(FDS)or
Abductor digiti minimi(ADM).
It is recommended about 1-2 years of age
The ring finger flexor digitorum superficialis (FDS) has
adequate length for both tendon transfer and UCL
reconstruction.


The abductor digiti minimi(ADM)

First web space deepening
usually performed with Z-plasty or V-Y flap
partial release of the insertions of the intrinsic
muscles (ie, first dorsal interosseous, )

Stabilization of MCP joint
Three options
Fusion
Reconstruction of UCL with FDS
Reconstruction of UCL with free tendon graft

A type IIIA also requires transfers to
overcome the extrinsic musculotendinous
abnormalities
Extensor indicis proprius(EIP) is good for
Extension of the thumb.
And reconstruction of the flexor pollicis
longus(FPL).

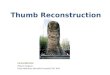
Pollicization
◦ Type IIIB, IV, V hypoplasia
◦ Tips
Plan skin incision to avoid skin grafts
Isolate index finger on its
neurovascular bundles
Detach first dorsal and palmar
interosseous muscles
Removing most index metacarpal and
epiphyseal plate

Stabilize index MCP joint (40°
ABD, 15°EX, and 120° pronation).
Reattach and balance
musculotendinous units
Reconstruct long extensor
tendons
Rebalance flexor tendons

Type V with polydactyl

Summary
Thumb hypoplasia frequently associated with
other anomalies.
Blauth classification with other modifications are
very important for management of thumb
Hypoplasia.
Good clinical examination with lab investigations
are very important before reconstruction.

Thank you