Embed Size (px)
Citation preview

TOF PHYSIOLOGY

HISTORY
Tetralogy of Fallot was first described by Niels Stenson in 1671.
Precise anatomical description by William Hunter at St Georges Hospital Medical School in London in 1784.

Fallot physiology, was defined by Etienne-Louis Fallot in 1888 in his description of L’anatomie pathologique de la maladie bleu.
Term tetralogy of Fallot is attributed to Canadian Maude Abbott in 1924.

Fallot physiology
Systemic venous return unable to reach lungs
Shunted right to left away from pulm circulation VSD essential for this to occur;
Or a common chamber ! PLUS

Obstruction at - RA outlet - i.e Tricuspid atresia - infundibular/valvular Pulmonary stenosis - rarely branch PA stenosis.

FALLOT PHYSIOLOGY SYNDROMES
Tetralogy of Fallot Tricuspid. atresia - PS Single ventricle - PS TGA with VSD – PS DORV – VSD – PS

EPIDEMIOLOGY About 3·5% of all infants born with a congenital heart
disease have tetralogy of Fallot. Corresponding to one in 3600 or 0·28 every 1000
livebirths, with males and females being affected equally. Fyler et al . NE Regional Infant Cardiac Program. 1980
Its precise cause is unknown, as for most congenital heart diseases.
Most cases seem sporadic, although the risk of recurrence in siblings is about 2.5% if there are no other affected first-degree relatives. Nora JJ Nora JJ Am J Med Genet 1988 Am J Med Genet 1988

THE BALTIMORE-WASHINGTON INFANT STUDY. (1981-1989) Ferencz et al.1997
Tof - 0.33 per 1000 live births Fifth most common defect Most common form of cyanotic defect 79.7% had tof with ps 20.3% had tof with pa Tof with ps prevalence 0.26 per 1000 live births with male
predominance.

INDIAN DATA
Bhardwaj et al. Congenital heart disease · October 2014

GENETIC FACTORS
Genetic causes of TOF are heterogeneous: a)Monogenic or polygenic mode of inheritance. b)Autosomal dominant mode of inheritance with reduced
penetrance, c)An autosomal recessive mode of inheritance. Moss & Adams' Heart Disease in infants
Environmental factors: Maternal diabetes [threefold increased risk], Retinoic
acids,Maternal phenylketonuria (PKU), and Trimethadione Edward J et al .Edward J et al .N Engl J Med 1985; 313:837-841N Engl J Med 1985; 313:837-841

GENETIC SYNDROMES AND CHROMOSOMAL ANOMALIES
DiGeorge/Velocardiofacial syndrome
Down syndrome Alagille syndrome Cat's-eye syndrome CHARGE and
VATER/VACTERL associations, Poland syndrome
Goldenhar’s syndrome(oculo-auriculo-vertebral dysplasia). THE BALTIMORE STUDY.
Microdeletion 22q11….seen in8%-23% of TOF patients; 45% of TOF + PA; 65% of those with TOF + APVGoldmuntz et al J Am Coll Goldmuntz et al J Am Coll Cardiol 1998Cardiol 1998

EMBRYOLOGY The aorta and pulmonary artery start as a
single tube the truncus arteriosus which is then divided by the spiral septum.
The spiral septum grows down to and attaches to the ventricular septum which isolates the left and right ventricles as well as isolating the aorta and pulmonary artery.
But in TOF Spiral septum gets shifted over towards the right side of the heart leading to large opening of aorta and small pulmonary artery opening with spiral septum missing ventricular septum with straddling of aorta over malaligned vsd.

ANATOMY ANATOMY
Anterior and cephalad deviation of the infundibular septumAnterior and cephalad deviation of the infundibular septum. .
This results in a malaligned ventricular septal defect (VSD), This results in a malaligned ventricular septal defect (VSD), with the aortic root overriding the defect and leading to with the aortic root overriding the defect and leading to subsequent right ventricular outflow obstruction.subsequent right ventricular outflow obstruction.
VSDVSD is most commonly located in the perimembranous region is most commonly located in the perimembranous region of the septum.of the septum.
The VSD can extend into the muscular septum. The VSD can extend into the muscular septum.
There are rarely other muscular ventricular septal defects. There are rarely other muscular ventricular septal defects. Anderson et al. J thorac Cardiovasc Surg 1981

RVOT OBSTRUCTION
The right ventricular outflow obstruction is often at multiple levels.– The anterior and cephalad deviation of the
infundibular septum results in subvalvular obstruction.– Hypertrophy of muscular bands in this region can
further accentuate subvalvular obstruction.– The pulmonary valve annulus is usually hypoplastic,
although in some instances it is of normal size.– The pulmonary valve itself is frequently bicuspid and
stenotic Van praagh et al .Am J Cardiol 1970

It is common to identify an area of supravalvularr narrowing in the main pulmonary artery at the sinotubular ridge.
There may also be further obstruction at the branch pulmonary arteries.
These may be diffusely hypoplastic or have focal areas of stenosis, most commonly at the proximal branch pulmonary arteries.
Rao et al .Am J Cardiol 1971

Kirklin/Barratt-Boyes Cardiac Surgery

OVERRIDING AORTA
Aorta is displaced to the right over the VSD Aorta is displaced to the right over the VSD rather than the left rather than the left ventricle leading to blood flow from both ventricles into the ventricle leading to blood flow from both ventricles into the aorta.aorta.
The The degree of aortic override of the VSD degree of aortic override of the VSD can vary widely and can vary widely and is one of the major factors used by some groups is one of the major factors used by some groups to to differentiate between TOF and DORV. differentiate between TOF and DORV.
If one defines double outlet right ventricle as the presence If one defines double outlet right ventricle as the presence of aortic/mitral valve fibrous continuity, then the degree of of aortic/mitral valve fibrous continuity, then the degree of override is not relevant to diagnosis. override is not relevant to diagnosis.
If, however, one defines double outlet right ventricle as a If, however, one defines double outlet right ventricle as a condition with greater than 50 percent aortic override, then, by condition with greater than 50 percent aortic override, then, by definition, the degree of aortic override in TOF is limited.definition, the degree of aortic override in TOF is limited.
Moss & Adams' Heart Disease in infants

ASSOCIATED ANOMALIES
Kirklin/Barratt-Boyes Cardiac Surgery

Kirklin/Barratt-Boyes Cardiac SurgeryKirklin/Barratt-Boyes Cardiac Surgery




PATHOPHYSIOLOGY


RV and LV pressures becomes identical

RV and LV pressures becomes identical
There is little or no L to R shunt

RV and LV pressures becomes identical
There is little or no L to R shunt
Hence, VSD is silent

RV and LV pressures becomes identical
There is little or no L to R shunt
Hence, VSD is silent
Right ventricle into pulmonary artery across pulmonic stenosis producing ejection systolic murmur

Hence, the more severe the pulmonary stenosis

Hence, the more severe the pulmonary stenosis
The BIGGER the Left to RIGHT shunt

Hence, the more severe the pulmonary stenosis
The BIGGER the Left to RIGHT shunt
Less flow into the pulmonary artery

Hence, the more severe the pulmonary stenosis
The BIGGER the Left to RIGHT shunt
Less flow into the pulmonary artery
Shorter the ejection systolic murmur

Hence, the more severe the pulmonary stenosis
The BIGGER the Left to RIGHT shunt
Less flow into the pulmonary artery
Shorter the ejection systolic murmur
More cyanosis because of less flow to the lung!

HENCE,
Severity of cyanosis is directly proportional to the severity of pulmonic stenosis.
Intensity of the systolic murmur is inversely related to the severity of pulmonic stenosis.

One of the physiologic characteristics of TOF is that the One of the physiologic characteristics of TOF is that the RVOT obstruction can fluctuate. RVOT obstruction can fluctuate.
An individual with minimal cyanosis can develop a An individual with minimal cyanosis can develop a dynamic increase in right ventricular outflow tract dynamic increase in right ventricular outflow tract obstruction with a subsequent increase in right-to-left obstruction with a subsequent increase in right-to-left shunt and the development of cyanosis. shunt and the development of cyanosis.
These episodes are often referred to as These episodes are often referred to as "TET SPELLS" " or or "HYPERCYANOTIC SPELLS".

Typical spell begins with progressive increase in rate and depth of respiration and culminates in paroxysmal hyperapnea, deepening cyanosis, limpiness, syncope and occasionally in convulsions, CVA and death.
Peak incidence in between second and sixth month of life.
Spells typically initiated by stress of feeding, crying or a bowel movement, particularly after awakening from deep sleep.

Pediatric Cardiology for Practitioners Pediatric Cardiology for Practitioners By Myung K. ParkBy Myung K. Park

5rx5rx

MANAGEMENT OF ANOXIC SPELL1. Calm the baby2. Increase SVR3. Knee chest position4. Humidified O25. Morphine 0.1 -0.2 mg/Kg Subcutaneous6. Correct acidosis – Sodium Bicarb IV7. Inj phenyelphrine8. Propranolol
1. 0.1mg/kg/IV during spells2. 0.5 to 1.0 mg/kg/ 4-6hourly orally
9. Vasopressors:10. Correct anemia

SQUATTING
Postural effects in tetralogy of fallot .Am J Med 15:297,1953

CLINICAL FEATURES
Wide due to variable severity of RV outflow obstruction USGfetal diagnosis Newborn & infants…cyanosis and systolic murmur. Acyanotic TOFrarely CHF unless there is a large PDA
or aortopulmonary collateral arteries
Pregnancy…poorly tolerated … gestational decrease in SVR increases R-L shunt & the labile SVR during labor, delivery leads to abrupt hypoxemia…..high fetal wastage / immature offspring.

EXAMINATION
Cyanosis, Clubbing Prominent a waves in jvp. Arterial pulses …normal in uncomplicated TOF Wide pulse pressure (arterial diastolic runoff)….
aortopulmonary collaterals, palliative surgical shunt or PDA
Accentuated precordial RV impulse S2 single& loud (anterior, dextroposed aorta) S3/S4 are unusual Aortic ejection click

Systolic murmur - crescendo-decrescendo at LUSB. The intensity of the murmur inversely parallels the degree
of pulmonic obstruction. Diastolic murmurs are unusual. TOF with PA- no harsh, obstructive precordial murmurs TOF and APV syndrome - A harsh diastolic murmur, with
a harsh murmur of PS. [Harsh sawing, to-and-fro murmur] Continuous murmurs - PDA, aortopulmonary collaterals,
may be best heard in the back.

ECG
QRS axis … same as that of a normal newborn
RVH…Tall monophasic R in V1 with an abrupt
change to an rS pattern in V2 (Tall R extends into adj
precordial leads in TOF + APV)
Balanced shunt …qR in V5,V6

ECG
ECGECG

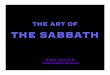
CXR Normal sized heart; [may be large in PA]
Upturned apex; attenuated & concave
left heart border (infundibular and PA
hypoplasia)….boot-shaped heart, or
coeur en sabot
Diminished pulmonary vascularity in
proportion to the degree of cyanosis.
Right atrial enlargement
Right-sided aortic arch (20-25% of
patients) with indentation of leftward-
positioned tracheobronchial shadow.
Absent thymic shadow in the newborn
may indicate associated chromosome
22q11.2 microdeletion (DiGeorge
syndrome).

ECHOCARDIOGRAPHY
2-D echocardiography cornerstone for noninvasive diagnosis. Doppler analysis provides further data regarding
hemodynamic characteristics. The coronary arteries are also readily apparent in PSAX view
slightly superiorly. The origin and course of the left and right coronary arteries
should be determined, paying special attention to whether any vessels take an anterior course across the infundibulum.
Correct definition of the coronary artery anatomy was possible in most patients with a sensitivity of 82%, specificity of 99%, and accuracy of 98.5% in a study by Need et al.


LAD
RCC
NCC
RCA
LCx
Pulm. Valve
MPA
The anomalous LAD crossing the RVOT in TOF is identified when the transducer is swept superiorly in the parasternal short -axis view . This allows visualization of the anomalous LAD that is situated anterior to the RVOT

CARDIAC CATHETERIZATION
With the evolution of noninvasive technology, the indications for diagnostic cardiac catheterization have diminished substantially.
Nonetheless, invasive study to obtain both hemodynamic and anatomic information is, on occasion, helpful prior to deciding on surgical strategy.
Foremost goal …. clarification or better definition of anatomic characteristics, such as pulmonary arterial or coronary arterial anatomy.
Coronary artery anatomy … either by aortic root angio, selective coronary artery injection, or a combination of both. .

Moss & Adams' Heart Disease in infants
A: An ascending aortogram in the LAO projection demonstrates a right anterior descending coronary artery arising from the right coronary artery.
B: A selective left coronary injection shows filling of only the circumflex coronary artery.

COURSE AND COMPLICATIONS
1) Each anoxic spell is potentially fatal2) Polycytemia
1) Cerebrovascular thrombosis3) Anoxic infaction of CNS
1) Neurological complication

CNS COMPLICATIONS
Paradoxic embolus Cerebral thrombosis Cerebral abcess Seizures Hypoxic damage Endocarditis & vegetations Postoperative strokes

NATURAL HISTORY



TREATMENT

TIMING OF SURGERY Infants with very severe RVOT stenosis and those with TOF + PA, with
SaO2<70%, should have surgery within a few weeks after birth.
Infants with moderately severe stenosis and marked cyanosis (SaO2 70–90%)
should have corrective surgery by 2–4 months.
Corrective surgery should be performed in all other infants with tetralogy of Fallot
by 6 months.
Contraindications for repair in early infancyPalliation initially
LAD from RCA crossing infundibulum
Severely hypoplastic PAs
Pulmonary atresia

PALLIATIVE PROCEDURES
Classic BT shunt[1945]…SCAPA on side opposite AA
Modified BT… esp in small infants <6 months…side to side anastomosis
with interposition graft of PTFE or Gore-Tex b/w SCA & PA [on the same
side of AA]
Waterston shunt : Side-side anastomosis of RPA to AA
Potts : Side - side anastomosis of LPA to DA
Waterston/Potts shunts : complications
Excessive PBF HF [20%] & PHTN
Difficulty taking shunt down at time of correction
Distortion of Rt/Lt PA ; Right/Left PA aneurysm

BT shunt-advantages :
(a)low incidence of problems from excess PBF
(b)No pericardial adhesions as pericardium is not entered
(c)Easy to close at time of complete repair..ligating its distal part just proximal to anastomoses with PA
(d)Less distortion of PAs
CENTRAL SHUNT :connecting a short tubular graft of Teflon or GoreTex from the aorta to the MPA.
Advantages vs other shunts: the size of the communication could be controlled by selecting a tube with a diameter appropriate for the patient; branch PAs are not disturbed so that reconstruction is not required at the time of corrective surgery.

BLALOCK TAUSSIG SHUNT
Subclavian artery – Pulmonary artery anastomosis

MODIFIED BLALOCK TAUSSIG SHUNT
Goretex graft

SURGICAL PALLIATION

CLASSIC BT shunt

POTTS SHUNT WATERSTON SHUNT

AIM OF SURGERY
Relieving all possible sources of RVOTO. If possible, pulmonary valve function is preserved by avoiding a
transannular patch. Closure of VSD (dacron patch)
To relieve RVOTOpulmonary valvotomy, the insertion of an outflow tract patch or a transannular patch are often required.
Surgery during early infancy, when the pulmonary annulus is markedly stenotic, frequently requires the insertion of a long and wide transannular patch.
Kirkln JW et al J Thorac Cardiovasc Surg,1992

Consequently, most patients acquire PR as a result of the repair.
PR may be well tolerated by many in the early postoperative years.
But in the long term chronic PR is associated with reduced exercise capacity, RV dilatation, ventricular arrhythmias, and sudden death.


POST REPAIR FOR TOF
Current surgical survival, even for symptomatic infants <3 Current surgical survival, even for symptomatic infants <3 months of age, is excellent. months of age, is excellent.
Hospital and 1-month survival rates of 100% have been Hospital and 1-month survival rates of 100% have been reported. reported.
Earlier age at repair (<1 year of age) did not adversely Earlier age at repair (<1 year of age) did not adversely affect the rate of reintervention; so primary repair should affect the rate of reintervention; so primary repair should be regarded as the preferred management strategy. be regarded as the preferred management strategy.
Twenty-year survival for hospital survivors, irrespective of Twenty-year survival for hospital survivors, irrespective of management strategy, was 98% for patients who have TOF management strategy, was 98% for patients who have TOF with PS and slightly lower for patients with PA, reflecting with PS and slightly lower for patients with PA, reflecting the overall excellent long-term survival of these patients.the overall excellent long-term survival of these patients.

COMPLICATIONS
Residual VSDResidual VSD Pulmonary regurgitationPulmonary regurgitation Residual RVOT obstruction Residual RVOT obstruction RV wall motion abnormalitiesRV wall motion abnormalities RV dysfunction and RHFRV dysfunction and RHF Atrial tachycardiaAtrial tachycardia Ventricular tachycardia (VT)Ventricular tachycardia (VT)

Important findings
Conditions (RVH ON ECG) Important clinical findingsTOF (qrs axis between 90-150 degrees) Long systolic murmur , grade 2-3/6 at
ULSBSoft continuous murmur in neonates with tof with pulmonary atresia Concave main PA segment on cxr Right sided aortic arch on x ray film
DORV with PS (qrs axis > 150 degrees) Resemblance to TOFSystolic murmur along LSB, Grade3-4/6

Important findings
Conditions (LVH ON ECG) Important clinical findingsTricuspid atresia (qrs axis between -30 and -60 degree)
Severe cyanosis Murmur of VSD or PDA Superior QRS axis Boot shaped heart
DORV with PS Resemblance to TOFSystolic murmur along LSB, Grade3-4/6

Important findings
Conditions (BVH ON ECG) Important clinical findingsTGA and PS Moderate cyanosis
No signs of CHF Systolic murmur (of PS ) at ULSB
Single Ventricle and PS Resemblance to TOFSystolic murmur along LSB.

PFO / ASDVSD / PDA
Fallot physiology

PREVALENCETricuspid atresia accounts for 1% to 3% of congenital heart
defects. PATHOLOGY1. The tricuspid valve is absent, and the RV is hypoplastic, with
absence of the inflow portion of the RV. The associated defects such as ASD, VSD, or PDA are necessary for survival.
2. Classified according to the presence or absence of PS and TGA.
The great arteries are normal in 70% & transposed in 30%. Transposition usually appears in the complete form. In 3% of cases, the CCTGA occurs.

h
Heart Disease in Infancy and Childhood , 3rd ed. New York,Macmillan,1978

CLINICAL MANIFESTATIONS
History1. Cyanosis is usually severe from birth. Tachypnea and poor feeding
usually manifest.2. Hypoxic spellsPhysical Examination 1. Cyanosis, either with or without clubbing, is always present.2. A systolic thrill is rarely palpable when associated with PS.3. The S2 is single. A grade 2-3/6 regurgitant systolic murmur of VSD is
usually present at the lower left sternal border. A continuous murmur of PDA isoccasionally present.
4. Hepatomegaly may indicate an inadequate interatrial communication or CHF.

ECG
“Superior” QRS axis (between 0 and -90 degrees) is characteristic. It appears in most patients without TGA .
The “superior” QRS axis is present in only 50% of patients with TGA. LVH is usually present; RAH or combined atrial hypertrophy (CAH) is
common.

CXR
The heart size is normal or slightly increased, with enlargement of the RA and LV.
Pulmonary vascularity decreases in most patients although it may increase in infants with TGA.
Occasionally, the concave PA segment may produce a boot-shaped heart, like the x-ray findings of TOF.

ECHO
Two-dimensional echo readily establishes the diagnosis of tricuspid atresia.
1. Absence of the tricuspid orifice, marked hypoplasia of the RV, and a large LV can be imaged in the apical four-chamber view.
2. The bulging of the atrial septum toward the left and the size of the interatrial communication are easily imaged in the subcostal four-chamber view.
3. Patients with TGA should be examined for possible subaortic stenosis and aortic arch anomalies.

TREATMENT
Medical1. Prostaglandin E1 to maintain the patency of the ductus before planned
cardiac catheterization or cardiacsurgery.2. The Rashkind procedure (balloon atrial septostomy) may be performed
as part of the initial catheterization to improve the RA-to-LA shunt.3. Treatment of CHF is rarely needed in infants with TGA without PS.4. Infants with normally related great arteries and adequate PBF through a
VSD need close monitoring for decreasing oxygen saturation resulting from spontaneous reduction of the VSD.
SurgicalMost infants with tricuspid atresia require a palliative procedure before a
Fontan-type operation can be performed.

Fallot physiology

SINGLE VENTRICLE Occurs in <1% PATHOLOGY Both AV valves are connected to a main, single ventricular chamber
(i.e., double-inlet ventricle), and the main chamber is in turn connected to a rudimentary chamber through the bulboventricular foramen.
One great artery arises from the main chamber, and the other arises from the rudimentary chamber .
The main ventricular chamber has anatomic characteristics of the LV (i.e., double-inlet LV).(80%)
Either D-TGA or L-TGA is present in 85% of cases. Common is double-inlet LV with L-TGA and with the aorta arising
from the rudimentary chamber, occurring in 70% to 75% of cases . The mitral valve is right sided; the tricuspid valve is left sided.
PS or pulmonary atresia is present in about 50% of cases. COA and interrupted aortic arch are also common.

The bulboventricular foramen is frequently obstructive. Anomalies of the AV valves, which include stenosis, in
addition to overriding or straddling, are frequent. In double-inlet RV, either right or left atrial isomerism
and straddling and/or overriding of the AV valves are common.
Most common ventriculoarterial connection is a double outlet from the main chamber.
PS is frequently found.

Physical findings depend on the magnitude of PBF. 1. With increased PBF, physical findings resemble those of
TGA and VSD or even of large VSD: a. Mild cyanosis and CHF with growth retardation are
present in early infancy. b. The S2 is single or narrowly split with a loud P2. A grade
3-4/6 long systolic murmur is audible along the left sternal border.
c. A diastolic murmur of PR may be present along the upper left sternal border as a result of pulmonary hypertension.

2. With decreased PBF, physical findings resemble those of TOF.
a. Moderate to severe cyanosis is present. CHF is not present. Clubbing may be seen in older infants and children.
b. The S2 is loud and single. A grade 2-4/6 ejection systolic murmur may be heard at the upper right or left sternal border

Electrocardiography An unusual ventricular hypertrophy pattern with similar QRS complexes
across most or all precordial leads is common (e.g., RS, rS, QR pattern).
Abnormal Q waves (representing abnormalities in septal depolarization) are also common and take one of the following forms: Q waves in the right precordial leads, no Q waves in any precordial leads, or Q waves in both the right and left precordial leads.
Either first- or second-degree AV block may be present. Arrhythmias occur (e.g., SVT, wandering pacemaker).

CXR
1. With increased PBF the heart size enlarges and the pulmonary vascularity increases.
2. When PBF is normal or decreased, the heart size is normal and the pulmonary vascularity is normal or decreased.
3. A narrow upper mediastinum suggests that TGA may be present.

ECHO
The following anatomic and functional information is important . a. Morphology of the single ventricle (e.g., double-inlet LV? double-
inlet RV?). b. Location of the rudimentary outflow chamber, which is usually left
and anterior. c. Size of the bulboventricular foramen and whether there is an
obstruction at the foramen. d. Presence or absence of D-TGA or L-TGA, stenosis of the
pulmonary or aortic valve, and size of the PAs. e. Anatomy of the AV valves. f. Size of the ASD. g. Associated defects such as COA, interrupted aortic arch, or PDA.

MANAGEMENTMANAGEMENT
• Palliative Procedures – BT shunt , PA banding , DKS operation
• Second stage palliation procedures – bidirectional glenn shunt
• Definitive procedure – fontan operation

DOUBLE OUTLET RIGHT VENTRICLEDOUBLE OUTLET RIGHT VENTRICLE PREVALENCEPREVALENCE DORV occurs in <1% of all congenital heart defects.DORV occurs in <1% of all congenital heart defects.
PATHOLOGYPATHOLOGY 1. Both the aorta and the PA arise from the RV. The only 1. Both the aorta and the PA arise from the RV. The only
outlet from the LV is a large VSD.outlet from the LV is a large VSD. 2. The great arteries usually lie side by side. The aorta is 2. The great arteries usually lie side by side. The aorta is
usually to the right of the PA, although one of the great usually to the right of the PA, although one of the great arteries may be more anterior than the other. arteries may be more anterior than the other.
The aortic and pulmonary valves are at the same level. Conus The aortic and pulmonary valves are at the same level. Conus septum is present between the aorta and the PA. septum is present between the aorta and the PA. There is no There is no fibrous continuity between the semilunar valves and the AV fibrous continuity between the semilunar valves and the AV valves. valves.

3. Classified according to position of VSD and presence or absence of PS
a. SUBAORTIC VSD (TOF type). The VSD is closer to the aortic valve than to the pulmonary valve and lies to the right of the conus septum .
Most common type, (55% to 70%) PS is common, especially the infundibular type, and it occurs in about 50% of patients with this type of DORV
b. SUBPULMONARY VSD (I.E., TAUSSIG-BING ANOMALY). The VSD is closer to the pulmonary valve than to the aortic valve, and it usually lies above the crista supraventricularis and to the left of the conus septum. (10% to 30% )
c. DOUBLY COMMITTED VSD. The VSD is closely related to both semilunar valves and is usually above the crista supraventricularis (<5% of cases).
d. REMOTE OR NONCOMMITTED VSD. The VSD is clearly away from the semilunar valves (about 10% of cases). It most commonly represents the AV canal-typeVSD

FALLOT-TYPE DOUBLE-OUTLET RIGHT FALLOT-TYPE DOUBLE-OUTLET RIGHT VENTRICLE WITH PULMONARY STENOSISVENTRICLE WITH PULMONARY STENOSIS
Even though the VSD is subaortic, in the presence of PS (i.e., Fallot Even though the VSD is subaortic, in the presence of PS (i.e., Fallot type), some desaturated blood goes to the aorta. This causes cyanosis type), some desaturated blood goes to the aorta. This causes cyanosis and a decrease in PBF.and a decrease in PBF.
Clinical pictures resemble those of TOFClinical pictures resemble those of TOF 1. Growth retardation, cyanosis, and clubbing are all common. 1. Growth retardation, cyanosis, and clubbing are all common. The S2 is loud and single. The S2 is loud and single. A grade 2-4/6 ejection systolic murmur along the left sternal border is A grade 2-4/6 ejection systolic murmur along the left sternal border is
present, either with or without a systolic thrill.present, either with or without a systolic thrill. 2. The ECG shows RAD, RAH, RVH, or RBBB. First-degree AV 2. The ECG shows RAD, RAH, RVH, or RBBB. First-degree AV
block is frequent.block is frequent. 3. Chest x-ray images show normal heart size with an upturned apex. 3. Chest x-ray images show normal heart size with an upturned apex.
Pulmonary vascularity is decreasedPulmonary vascularity is decreased

ECHO
In the parasternal short-axis view, a “ DOUBLE CIRCLE,” rather than the normal “circle and sausage” appearance of the great arteries, may be seen.
Either the great arteries are side by side with the aorta to the right, or the aorta is anterior and slightly to the right of the PA.
Differentiation of DORV from TOF with a marked Differentiation of DORV from TOF with a marked overriding of the aorta or from TGA is necessary. There is overriding of the aorta or from TGA is necessary. There is mitral-semilunar continuity in TOF and TGA (i.e., mitral-mitral-semilunar continuity in TOF and TGA (i.e., mitral-aortic continuity in TOF, and mitral-pulmonary continuity aortic continuity in TOF, and mitral-pulmonary continuity in TGA), but no mitral-semilunar continuity is present in in TGA), but no mitral-semilunar continuity is present in DORV.DORV.

MANAGEMENT
Palliative Procedures 1. PA banding for symptomatic infants with increased PBF
and CHF is occasionally performed.. 2. For infants with the Taussig-Bing type, enlarging the
interatrial communication is important for better mixing and for decompressing the LA, which causes pulmonary venous congestion.
Balloon atrial septostomy or blade atrial septostomy should be considered.
3. In infants with PS and decreased PBF with cyanosis, a systemic-to-PA shunt procedure is needed.

Definitive Surgeries – Definitive Surgeries – An intraventricular tunnel between the VSD and the aorta, in addition An intraventricular tunnel between the VSD and the aorta, in addition
to relief of PS by a patch graft, is carried out between 6 months and 2 to relief of PS by a patch graft, is carried out between 6 months and 2 years of age.years of age.
If preoperative studies indicate the need for a homograft valved If preoperative studies indicate the need for a homograft valved extracardiac conduit, the corrective repair is deferred until age 4 or 5 extracardiac conduit, the corrective repair is deferred until age 4 or 5 years, with a shunt operation performed in infancy.years, with a shunt operation performed in infancy.

TETRALOGY OF FALLOT WITH PULMONARY ATRESIA
PREVALENCE -15% to 20% of patients with TOF. PATHOLOGY Resembles that of TOF in all respects except for the
presence of pulmonary atresia, the extreme form of right ventricular outflow tract obstruction. The atresia may be at the infundibular or valvular level.
2. The PBF is most commonly mediated through a PDA (70%) and less commonly through multiple systemic collaterals MAPCA’s (30%).
The ductus is small and long and arises from the left aortic arch at an acute angle (instead of the normal oblique junction) and courses downward (“vertical” ductus)

3. PA anomalies are common in the form of hypoplasia, nonconfluence, and abnormal distribution.
a. The central PA is hypoplastic in most patients with TOF b. The central PAs are confluent in 85% of patients; they
are nonconfluent in 15%. Confluent PAs are usually found in patients with PDA (70%).
c. Among patients with confluent PAs, 50% have incomplete arborization (distribution) of one or both PAs. About 80% of patients with nonconfluent PAs have incomplete arborization

CLINICAL MANIFESTATIONS
Cyanotic at birth. The degree of cyanosis depends on patency of ductus and systemic collateral arteries .
Murmur cannot be heard. However, a faint, continuous murmur may be audible from the PDA or
collaterals. The S2 is loud and single. A systolic click is occasionally present.
ECG - RAD and RVH. CXR- normal heart size. The heart often appears as a boot-shaped
silhouette and the pulmonary vascularity is markedly decreased (i.e., “black” lung field).
Echo studies show all the anatomic findings of TOF plus the absence of a direct connection between the RV and the PA. The small branch PAs and “vertical ductus” are well imaged from a high parasternal or suprasternal transducer position.

NATURAL HISTORY Most neonates who have this condition die during the first 2 years of
life; However, infants with extensive collaterals may survive for a long
time, perhaps for more than 15 years.

MANAGEMENTMANAGEMENT
Pediatric Cardiology for Practitioners By Myung K. Park

TETRALOGY OF FALLOT WITH ABSENT TETRALOGY OF FALLOT WITH ABSENT PULMONARY VALVEPULMONARY VALVE
2% of patients with TOF PATHOLOGY AND PATHOPHYSIOLOGY The pulmonary valve leaflets are either completely absent or have an
uneven rim of rudimentary valve tissue present. The annulus of the valve is stenotic and displaced distally.
A massive aneurysmal dilatation of the PAs is present. The massive PA aneurysm results from severe pulmonary
regurgitation (PR) and an associated increase in RV stroke volume. The aneurysmal PAs compress anteriorly the lower end of the developing trachea and bronchi throughout fetal life, producing hypoplasia of the compressed airways.
This produces signs of airway obstruction and respiratory distress during infancy.

CLINICAL MANIFESTATIONSCLINICAL MANIFESTATIONS
1. Mild cyanosis may be present as a result of a bidirectional shunt during the newborn period when the pulmonary vascular resistance is relatively high. Cyanosis disappears, and signs of CHF may develop, after the newborn period.
2. A to-and-fro murmur (with “sawing-wood” sound) at the upper and mid-left sternal borders - characteristic .This murmur occurs because of mild PS and free PR. The S2 is loud and single.
The RV hyperactivity is palpable.

The ECG shows RAD and RVH.The ECG shows RAD and RVH. Chest x-ray images reveal a noticeably dilated main PA Chest x-ray images reveal a noticeably dilated main PA
and hilar PAs. The heart size is either normal or mildly and hilar PAs. The heart size is either normal or mildly enlarged, and pulmonary vascular markings may be enlarged, and pulmonary vascular markings may be slightly increased. slightly increased.
Echo reveals a large, subaortic VSD with overriding of Echo reveals a large, subaortic VSD with overriding of the aorta, distally displaced pulmonary annulus and the aorta, distally displaced pulmonary annulus and gigantic aneurysm of the PA and its branches.gigantic aneurysm of the PA and its branches.
Doppler studies reveal evidence of stenosis at the annulus Doppler studies reveal evidence of stenosis at the annulus and PR. and PR.

NATURAL HISTORY 1. More than 75% of infants with severe pulmonary
complications (e.g., atelectasis, pneumonia) die during infancy if treated only medically.
2. Infants who survive infancy without serious pulmonary problems do well for 5 to 20 years and have fewer respiratory symptoms during childhood.
They become symptomatic later and die from intractable right-sided heart failure.
Management is early surgical repair.

ConclusionsConclusions
Tetralogy of Fallot is the most common form of cyanotic Tetralogy of Fallot is the most common form of cyanotic congenital heart disease, and one of the first to be successfully congenital heart disease, and one of the first to be successfully repaired by congenital heart surgeons. repaired by congenital heart surgeons.
Since the first procedures in the 1950s, advances in the Since the first procedures in the 1950s, advances in the diagnosis, perioperative and surgical treatment, and diagnosis, perioperative and surgical treatment, and postoperative care have been such that almost all those born with postoperative care have been such that almost all those born with tetralogy of Fallot can now expect to survive to adulthood.tetralogy of Fallot can now expect to survive to adulthood.
The care of children with tetralogy of Fallot and their transition The care of children with tetralogy of Fallot and their transition to adult life has been a success of modern medicine.to adult life has been a success of modern medicine.
Most of them now survive early repair and have an essentially Most of them now survive early repair and have an essentially normal childhood.normal childhood.