Embed Size (px)
Citation preview
VIRAL CONJUCTIVITISSITI MARIAM BINTI MOHD HAMZAH
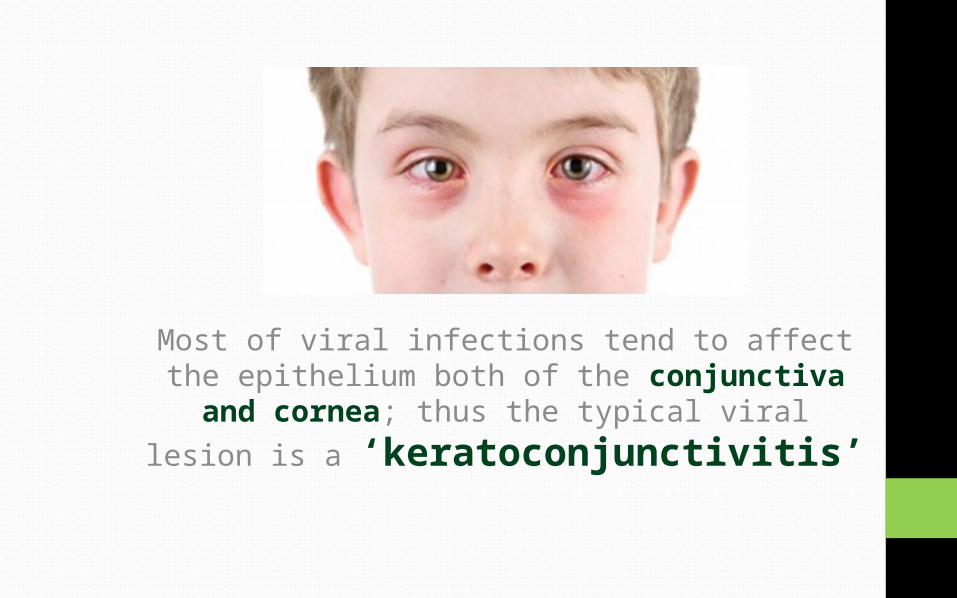
Most of viral infections tend to affect the epithelium both of the conjunctiva and cornea; thus the typical viral lesion is a
‘keratoconjunctivitis’
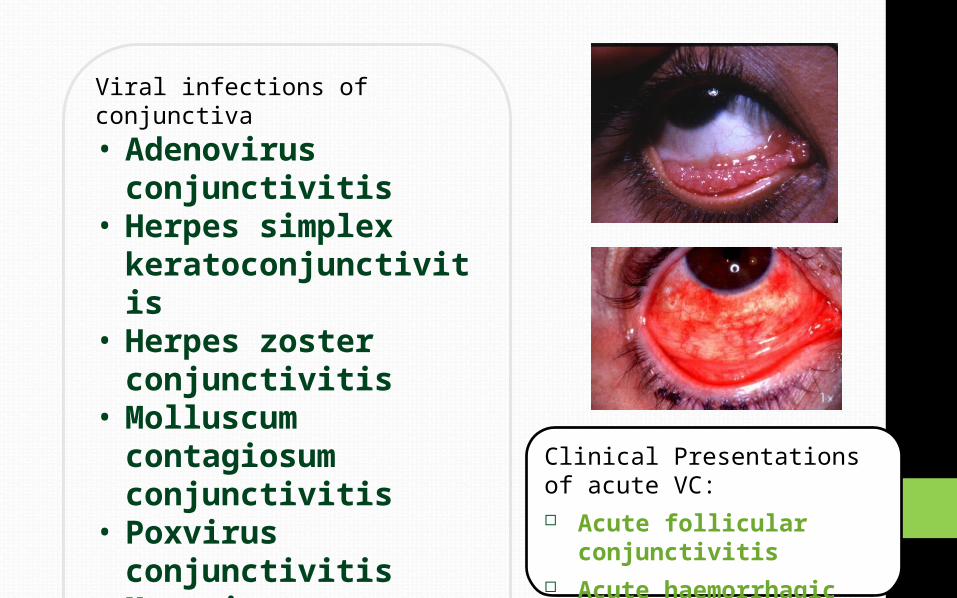
Viral infections of conjunctiva• Adenovirus
conjunctivitis• Herpes simplex
keratoconjunctivitis
• Herpes zoster conjunctivitis
• Molluscum contagiosum conjunctivitis
• Poxvirus conjunctivitis
• Myxovirus conjunctivitis
• Parammyxovirus conjunctivitis
• ARBOR virus conjunctivitis
Clinical Presentations of acute VC: Acute follicular
conjunctivitis Acute haemorrhagic
conjunctivitis
Adenoviral Conjunctivitis• Adenoviruses are the commonest causes of viral
conjunctivitis• Non-enveloped, double stranded DNA viruses, which replicate
within the nucleus of host cells. General reservoir is only human.
Type of adenoviral conjunctivitis• Epidemic keratoconjunctivitis (EKC)• Nonspecific acute follicular conjunctivitis• Pharyngoconjunctival fever (PCF)• Chronic relapsing adenoviral conjunctivitis
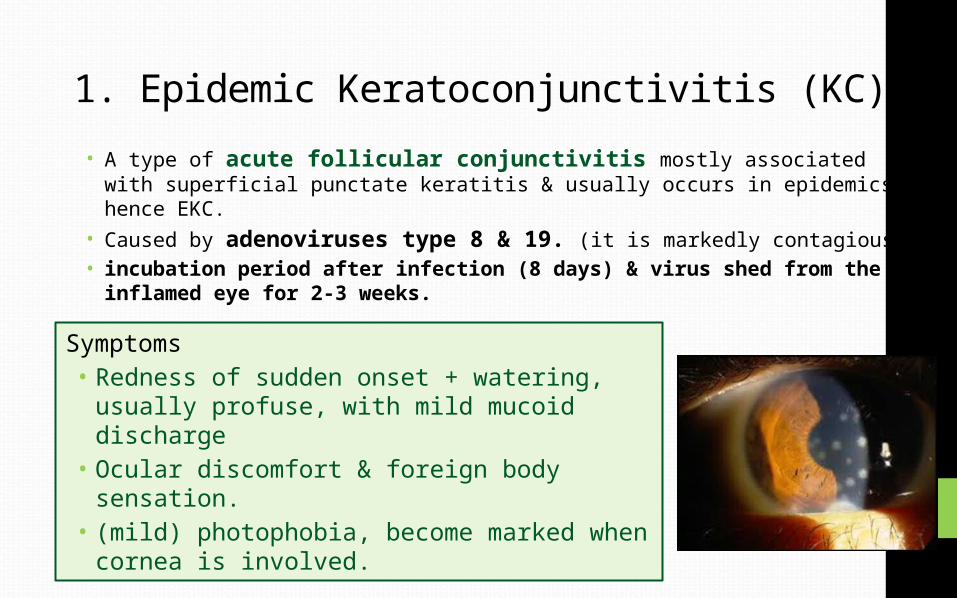
1. Epidemic Keratoconjunctivitis (KC)• A type of acute follicular conjunctivitis mostly associated with
superficial punctate keratitis & usually occurs in epidemics, hence EKC.• Caused by adenoviruses type 8 & 19. (it is markedly contagious)• incubation period after infection (8 days) & virus shed from the
inflamed eye for 2-3 weeks.
Symptoms• Redness of sudden onset + watering,
usually profuse, with mild mucoid discharge• Ocular discomfort & foreign body sensation.• (mild) photophobia, become marked when
cornea is involved.
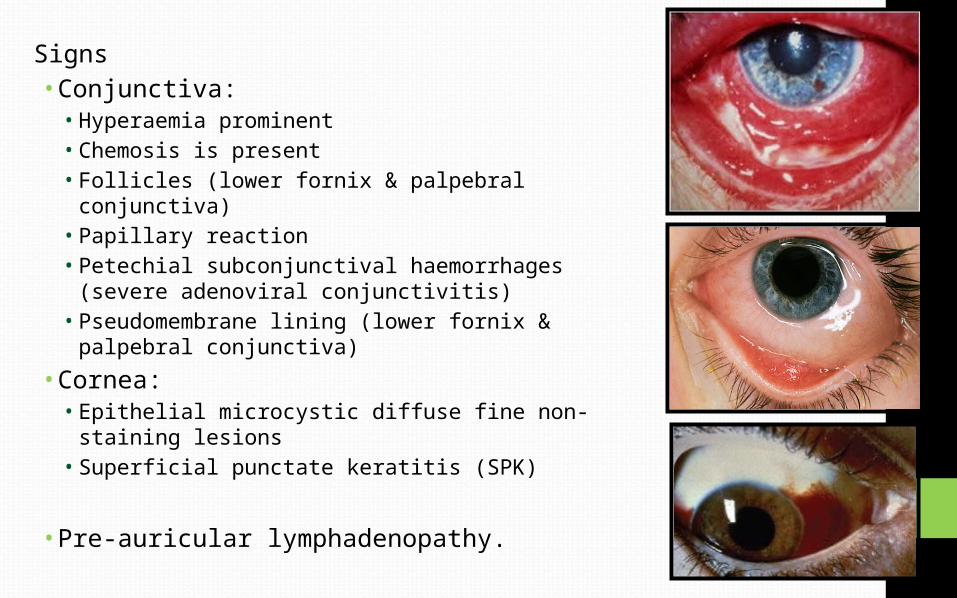
Signs• Conjunctiva:• Hyperaemia prominent• Chemosis is present• Follicles (lower fornix & palpebral conjunctiva)• Papillary reaction• Petechial subconjunctival haemorrhages (severe
adenoviral conjunctivitis)• Pseudomembrane lining (lower fornix &
palpebral conjunctiva)• Cornea:• Epithelial microcystic diffuse fine non-staining
lesions• Superficial punctate keratitis (SPK)
• Pre-auricular lymphadenopathy.
TreatmentI. Supportive treatment for amelioration of symptoms is the
only treatment required and includes:• Cold compresses, and sun glasses to decrease glare,• Decongestant and lubricant tear drops to decrease
discomfortII. Topical antibiotics; to prevent superadded bacterial
infectionsPrevention of spread of infection to the contacts- Highly contagious and patients may be infectious for up to
11 days after onset
Transmission usually occurs• From eyes to fingers to eyes• Tonometers, contact lenses and eye drops
2. Nonspecific Acute Follicular Conjunctivitis• Most common form of acute follicular conjunctivitis• Caused by adenovirus serotypes 1 to 11 & 19• Milder form of acute follicular conjunctivitis.• Treatment similar as EKC
3.Pharyngoconjunctival Fever (PCF)• adenoviral infection commonly associated with
subtypes 3 & 7.• PCF primarily affect children & appears in
epidemic form• Treatment is similar as EKCClinical features• Acute follicular conjunctivitis,
associated with pharyngitis.• Fever & pre-auricular
lymphadenopathy.• Cornea : superficial punctate
keratitis. (30%)
Acute Herpetic Conjunctivitis
• Always an accompaniment of the ‘primary herpetic infection’, mainly occur in children and adolescents.
• Commonly caused by herpes simplex virus type 1 and spreads by kissing or other close personal contacts.• HSV type 2 associated with genital infections, may also involve
the eyes in adults as well as children, though rarely.
• Treatment• Usually self limiting• Topical antiviral drugs control the infection effectively and
prevent recurrences• Supportive measures are similar with EKC
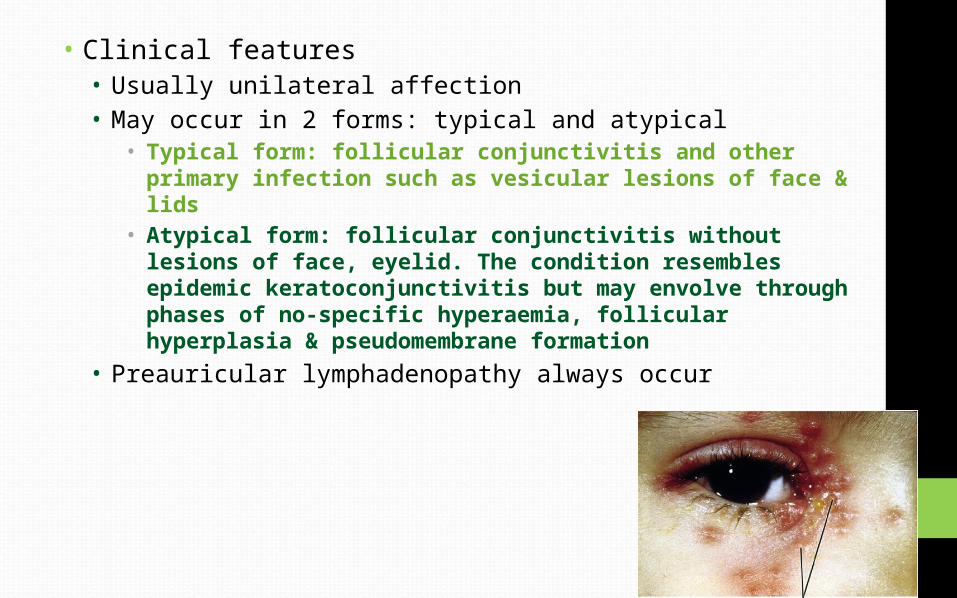
• Clinical features• Usually unilateral affection• May occur in 2 forms: typical and atypical
• Typical form: follicular conjunctivitis and other primary infection such as vesicular lesions of face & lids
• Atypical form: follicular conjunctivitis without lesions of face, eyelid. The condition resembles epidemic keratoconjunctivitis but may envolve through phases of no-specific hyperaemia, follicular hyperplasia & pseudomembrane formation
• Preauricular lymphadenopathy always occur
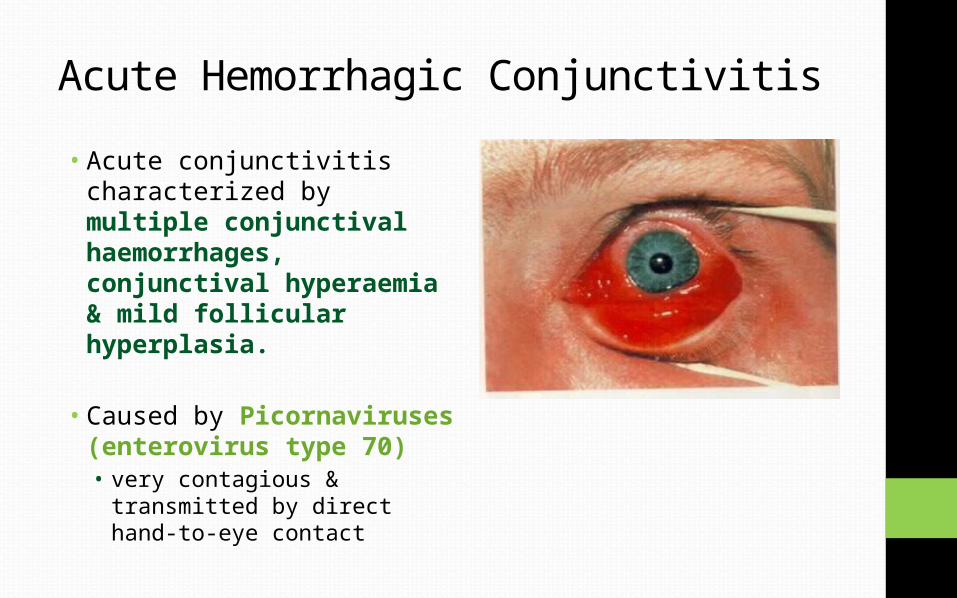
Acute Hemorrhagic Conjunctivitis• Acute conjunctivitis
characterized by multiple conjunctival haemorrhages, conjunctival hyperaemia & mild follicular hyperplasia.
• Caused by Picornaviruses (enterovirus type 70)• very contagious & transmitted
by direct hand-to-eye contact
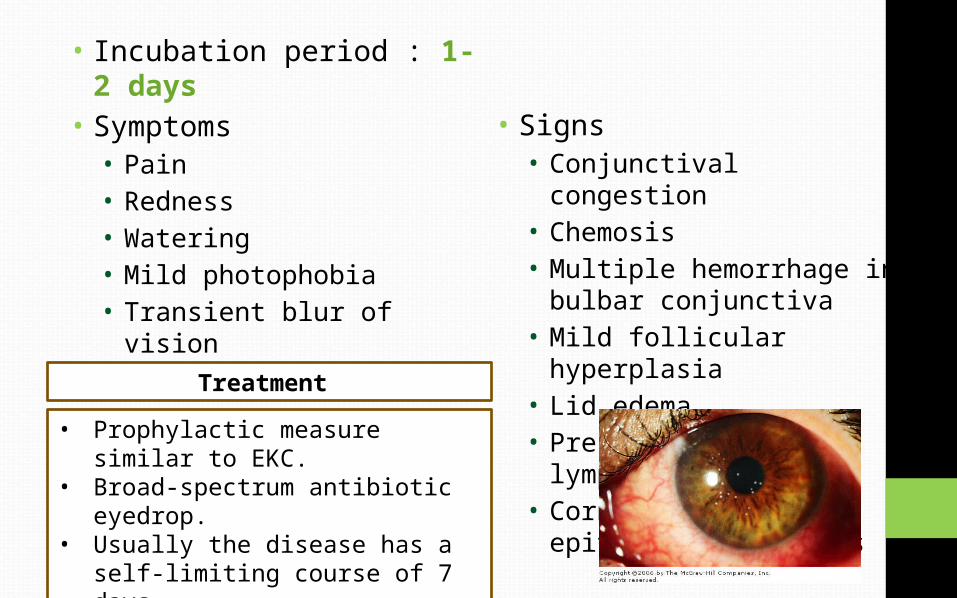
• Incubation period : 1-2 days
• Symptoms• Pain• Redness• Watering• Mild photophobia• Transient blur of vision• Lid swelling
• Signs• Conjunctival congestion• Chemosis• Multiple hemorrhage in
bulbar conjunctiva • Mild follicular hyperplasia• Lid edema• Pre-auricular
lymphadenopathy• Corneal sign : fine
epithelial keratitis
• Prophylactic measure similar to EKC.
• Broad-spectrum antibiotic eyedrop.
• Usually the disease has a self-limiting course of 7 days.
• Supportive measure same as EKC.
Treatment
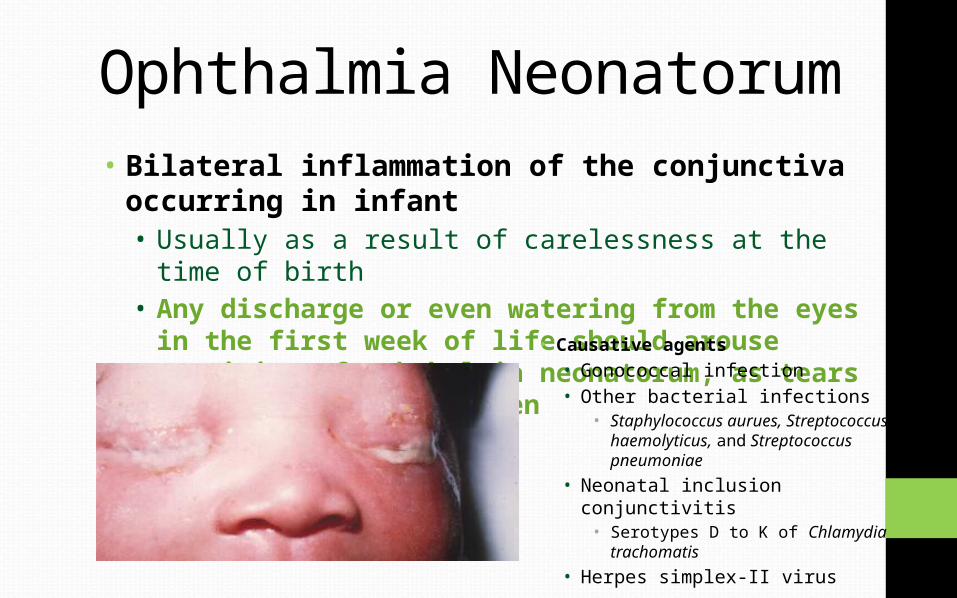
Ophthalmia Neonatorum• Bilateral inflammation of the conjunctiva
occurring in infant• Usually as a result of carelessness at the time of
birth• Any discharge or even watering from the eyes
in the first week of life should arouse suspicion of ophthalmia neonatorum, as tears are not formed till then
• Causative agents• Gonococcal infection• Other bacterial infections
• Staphylococcus aurues, Streptococcus haemolyticus, and Streptococcus pneumoniae
• Neonatal inclusion conjunctivitis• Serotypes D to K of Chlamydia
trachomatis• Herpes simplex-II virus
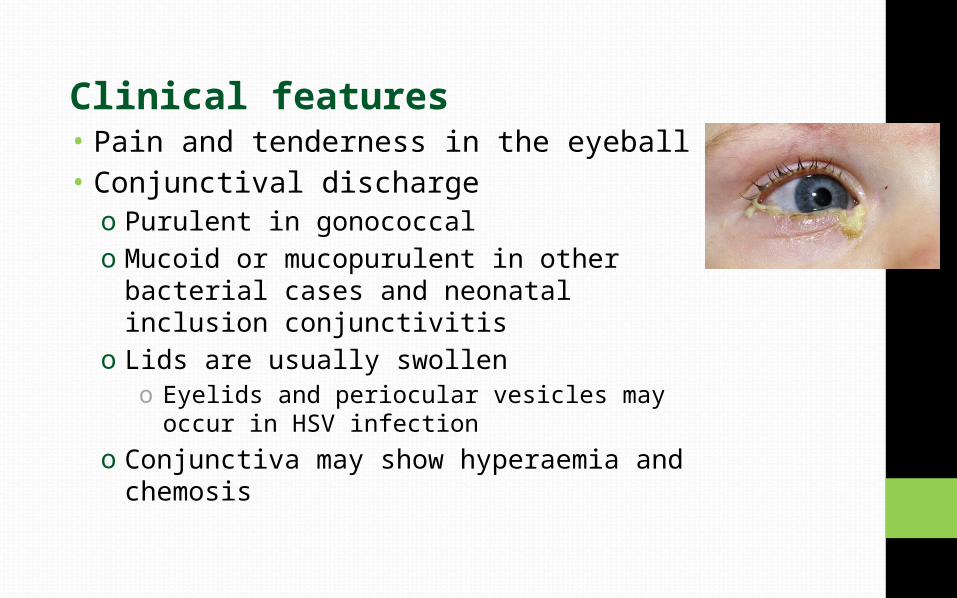
Clinical features• Pain and tenderness in the eyeball• Conjunctival dischargeo Purulent in gonococcal o Mucoid or mucopurulent in other bacterial
cases and neonatal inclusion conjunctivitis
o Lids are usually swolleno Eyelids and periocular vesicles may occur
in HSV infectiono Conjunctiva may show hyperaemia and
chemosis
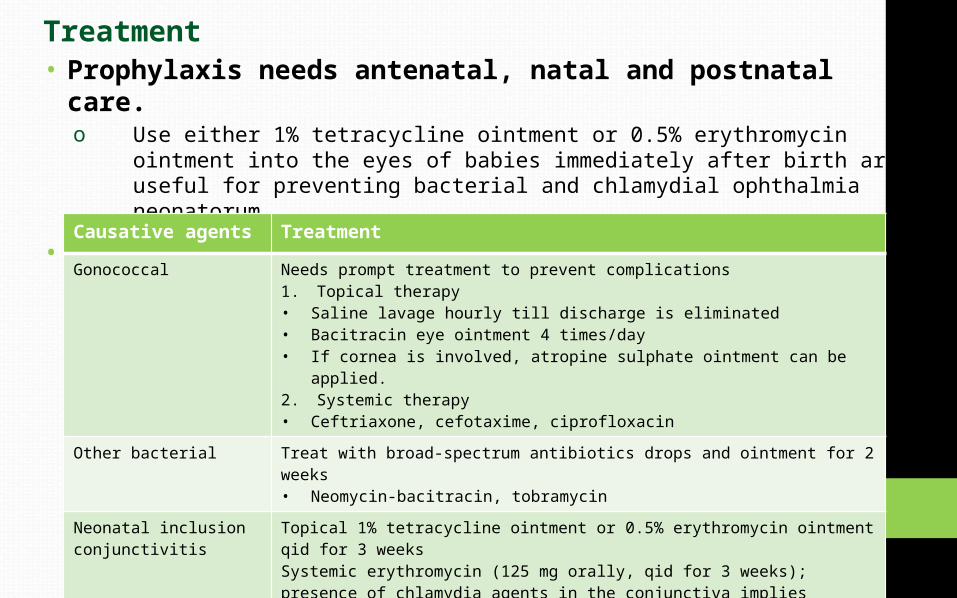
Treatment • Prophylaxis needs antenatal, natal and postnatal care.
o Use either 1% tetracycline ointment or 0.5% erythromycin ointment into the eyes of babies immediately after birth are useful for preventing bacterial and chlamydial ophthalmia neonatorum.
• Curative treatmentCausative agents Treatment
Gonococcal Needs prompt treatment to prevent complications1. Topical therapy• Saline lavage hourly till discharge is eliminated• Bacitracin eye ointment 4 times/day• If cornea is involved, atropine sulphate ointment can be applied.2. Systemic therapy• Ceftriaxone, cefotaxime, ciprofloxacin
Other bacterial Treat with broad-spectrum antibiotics drops and ointment for 2 weeks• Neomycin-bacitracin, tobramycin
Neonatal inclusion conjunctivitis
Topical 1% tetracycline ointment or 0.5% erythromycin ointment qid for 3 weeksSystemic erythromycin (125 mg orally, qid for 3 weeks); presence of chlamydia agents in the conjunctiva implies colonization of URT as well.
Herpes simplex Self-limitingHowever, antiviral drugs may control the infections and prevent the recurrence.


![Viral load in pop [HAConvention15]presented · 2015. 5. 22. · ICVL CVL PVL HIV specialist clinic Viral load ≤500/mL Viral load >500/mL Patients with viral load records Viral load](https://img.pdfslide.net/doc/110x75/6116aca41b670f6ef26fc105/viral-load-in-pop-haconvention15presented-2015-5-22-icvl-cvl-pvl-hiv-specialist.jpg)


























