Embed Size (px)
Citation preview

Viral Infections of SKIN AND MUCOSA I
AAU-MFDept. of
Dermato-venereology

HUMAN HERPESVIRUSES
• Human herpesviruses (HHVs) (family Herpesviridae)are defined by the architecture of the virion,which has: Core containing a linear double-strand DNA• Icosahedral capsid 100–110 nm in diameter composed of 162 capsomers Envelope containing
viral glycoprotein spikes on the surface.• Worldwide, 60–90% of the population is infected with one or more HHVs.

Eight HHVs have been identified:▪ Herpes simplex virus (HSV)-1 (HHV-1)▪ HSV-2 (HHV-2)▪ Varicella-zoster virus ( VzV, or HHV-3)▪ Epstein-Barr virus (EBV, or HHV-4)▪ Cytomegalovirus (CMV, or HHV-5)▪ HHV-6▪ HHV-7▪ HHV-8 (Kaposi sarcoma–associated virus). Primary HHV infections are usually asymptomatic with the exception of VZV, which nearly always presents with symptomatic varicella.

After primary infection, HHVs remain latent in neural or lymphoid cells and reactivate if an adequate immune response does not exist.HHVs are categorized into three groups: Alpha, beta, and gamma Herpesviridae ▪ Alpha Herpesviridae : HSV-1, HSV-2, VZV are characterized by a variable host range, relatively short reproductive cycle, rapid spread in culture, rapid destruction of infected cells, and latentinfection primarily, but not exclusively, of sensory ganglia.

Beta Herpesviridae : CMV has a restricted hostrange and spreads slowly in cultures. Gamma Herpesviridae : EBV, HHV-6, HHV-7,HHV-8, and herpesvirus saimiri are lymphotropic,specific for either T or B lymphocytes.The HHV-8 DNA sequences are closely homologousto minor capsid and tegument protein genes of gamma herpesviridae EBV and herpesvirusSaimiri.

HERPES SIMPLEX VIRUS (HSV) INFECTION
• Whether first-symptomatic or recurrent, may “typically” present clinically with grouped vesicles arising on an erythematous base on keratinized skin
or mucous membrane.• Most HSV infections are “atypical,” with patch(es) of
erythema, small erosions, fissures, or subclinical lesions that shed HSV.
• Once an individual is infected, HSV persists in sensory ganglia for the life of the patient, recurring
with lessening in immunity.

• Age of Onset Most commonly young adults;• range, infancy to senescence.• Etiology HSV-1, HSV-2.• Labialis: HSV-1 (80–90%), HSV-2 (10–20%).• Urogenital: HSV-2 (70–90%), HSV-1 (10–30%).• Herpetic whitlow: <20 years of age usuallyHSV-1; >20 years of age, usually HSV-2.• Neonatal: HSV-2 (70%), HSV-1 (30%).

Transmission
• Most transmission occurs when persons shed virus but lack lesions.
• Usually skin-skin, skin-mucosa, mucosa-skincontact. Herpes gladiatorum transmitted by skin to-skin
contact in wrestlers.• Increased HSV-1 transmission associated with crowded living conditions and lower socioeconomic status

Immunocompromising Factors Predisposing to HSV Reactivation
• HIV/AIDS infection, malignancy(leukemia/lymphoma), transplantation (bone marrow, solid organ), chemotherapy, systemic glucocorticoids, other
immunosuppressive drugs, radiotherapy

PATHOGENESIS
• Primary HSV infection occurs through close contact with a person shedding virus at a peripheral site, mucosal surface, or secretion.
• HSV is inactivated promptly at room temperature;aerosol or fomitic spread unlikely.• Infection occurs via inoculation onto susceptible mucosal surface or break in skin.• After exposure to HSV, the virus replicates in epithelial
cells, causing lysis of infected cells, vesicle formation, and local inflammation.

After primary infection at inoculation site, HSVascends peripheral sensory nerves and enterssensory or autonomic nerve root (vagal) ganglia, where latency is established.• Retrograde transport of HSV among nervesand establishment of latency are not dependent on viral réplication in skin or neurons; neurons can be infected in the absence of symptoms

• Latency can occur after both symptomaticand asymptomatic primary infection.
Periodically, HSV may reactivate from its latent state and virus particles then travel along sensory neurons to skin and mucosal sites to cause recurrent disease episodes.
• Recurrent mucocutaneous shedding can be associated with or without (asymptomatic shedding) lesions; virus can be transmitted to a new host when shedding occurs.







LABORATORY EXAMINATIONS
• Direct Microscopy Tzanck Smear• Optimally, fluid from intact vesicle is smeared
thinly on a microscope slide, dried, and stained with either Wright or Giemsa stain. Positive, if acantholytic keratinocytes or multinucleated giant acantholytic keratinocytes are detected. Positive in 75% of early cases, either primary or recurrent.

Antigen Detection DFA Monoclonal antibodies,specific for HSV-1 and HSV-2 antigens, detect and differentiate HSV antigens on smearfrom lesion. Cultures: Positive HSV cultures from involvedmucocutaneous site or tissue biopsy specimens.Serology• Antibodies to glycoprotein (g)G1 and (g)G2detect and differentiate past HSV-1 and HSV-2infections.

• Primary HSV infection can be documentedby demonstration of seroconversion.• Recurring herpes can be ruled out if seronegative for HSV antibodies.Polymerase Chain Reaction: To determineHSV-DNA sequences in tissue, smears, orsecretion.

DIAGNOSIS:-Clinical suspicion confirmed by viral cultureor antigen detection. Cultures used for diagnosing first-episode infections since antibodies to (g)H1 or (g)G2 may take 2–6 weeks to develop.

MANAGEMENT
• Prevention:- Skin-to-skin contact should be avoided during outbreak of cutaneous HSV infection.
• Topical Antiviral Therapy:-• Approved for herpes labialis; minimal efficacy.• Acyclovir 5% ointment Apply q3h, 6 times daily for 7 days.
Approved for initial genital herpes and limited mucocutaneous HSV infections in immunocompromised individuals.
• Penciclovir 1% cream Apply q2h while awake for recurrent orolabial infection in immunocompetent
individuals.

Oral Antiviral Therapy
• Drugs for oral HSV therapy include acyclovir, valacyclovir, and famciclovir. Valacyclovir, the prodrug of acyclovir, has a better bioavailability and is nearly 85% absorbed after oral administration. Famciclovir is equally effective for cutaneous HSV infections. Antiviral agents more effective in treating primary infections than recurrences

Acyclovir 400 mg 3 times daily or 200 mg 5 times daily for 7–10 daysValacyclovir 1 g twice daily for 7–10 daysFamciclovir 250 mg 3 times daily for 5–10 daysRecurrences Most episodes of recurrent herpes do not benefit from pulse therapy with oralacyclovir. In severe recurrent disease, patients who start therapy at the beginning of the prodrome or within 2 days after onset of lesions may benefit from therapy by shortening and reducing severity of eruption; however, recurrences cannot be prevented.

Chronic suppression:- Decreases frequency of symptomatic recurrences and asymptomatic HSVshedding. After 1 year of continuous daily suppressive therapy, acyclovir shouldbe discontinued to determine the recurrence rate.Acyclovir 400 mg twice dailyValacyclovir 500–1000 mg per dayFamciclovir 250 mg twice daily

Mucocutaneous disease in immunocompromised:-Patients with herpes who do not respond to theindividuals recommended dose of acyclovir may require a higher oral dose of acyclovir,IV acyclovir, or be infected with an acyclovir-resistant HSV strain, requiring IVfoscarnet. Acyclovir 5 mg/kg IV q8h for 7–14 days, or 400 mg 5 times daily for 7–14 daysNeonatal:-Acyclovir 20 mg/kg IV q8h for 14–21 days

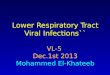
Herpes simplex virus: positive Tzanck smear




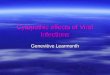
Herpes simplex virusinfection: herpetic whitlow

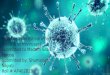
Herpes simplex virus infection: eczema herpeticum on eyelids

VARICELLA ZOSTER VIRUS INFECTIONS
• Varicella zoster virus (VZV) is a human herpesvirus that infects 98% of adult populations.
• Primary VZV infection (varicella or chickenpox) is nearly always symptomatic and characterized by disseminated pruritic vesicles.
• During primary infection, VZV establishes lifelong infection in sensory ganglia.

When immunity to VZV declines, VZV reactivateswithin the nerve cell, traveling down the neuronto the skin, where it erupts in a dermatomal pattern, i.e., herpes zoster (HZ), or shingles.In the immunocompromised host, primary and reactivated VZV infection is often more severe, associated with higher morbidity rates and some mortality. VZV vaccine has reduced the incidence of varicella and herpes zoster.

Age of Onset• Without immunization, 90% of cases occur inchildren <10 years, <5% in persons older than15 years.• With immunization (Varivax), the incidenceis markedly reduced.Etiology• VZV, a herpesvirus.• Structurally similar to other herpesviruses:Lipid envelope surrounding nucleocapsid with icosahedral symmetry.Centrally located double-strand DNA witha molecular weight of 80 million

Transmission• Airborne droplets as well as direct contact• Indirect contact uncommon• Patients are contagious several days beforevaricella exanthem appears and until last cropof vesicles• Crusts are not infectious.• VZV can be aerosolized from skin of individualswith herpes zoster, which is aboutone-third as contagious as varicella, causingvaricella in susceptible contacts.

PATHOGENESIS• In varicella, VZV is thought to enter throughmucosa of upper respiratory tract and oropharynx.• Followed by local replication and primary viremia.• VZV then replicates in cells of reticuloendothelialsystem with subsequent secondary viremia and dissemination to skin and mucous membranes.• Localization of VZV in the basal cell layeris followed by virus replication, ballooningdegeneration of epithelial cells, and accumulationof edema fluid.• Second episodes of varicella have been documentedbut are rare.

LABORATORY EXAMINATIONS
• VZV Antigen Detection DFASmear of vesicle fluid or scraping from ulcer
base/margin: Direct• fluorescent antibody (DFA) test detects VZV specific
antigens.• Viral Cultures: Isolation of virus on viral culture (human fibroblast monolayers) from vesicular
skin lesions, biopsy specimens, cornealscraping, and CSF is possible but more difficultthan for HSV.

Tzanck Smear Cytology of fluid or scrapingfrom base of vesicle or pustule showsboth giant and multinucleated acantholyticepidermal cells (as does that of HSV infections)Serology Seroconversion documents primary VZV infection.

CLINICAL MANIFESTATIONIncubation Period 14 days (range, 10–23 days).Prodrome• Characteristically absent or mild.• Uncommon in children, more common inadults: headache, general aches and pains,severe backache, malaise.• Exanthem appears within 2–3 days. Skin Symptoms Exanthem usually quite pruritic.Skin LesionsIn most children, illness begins with appearanceof exanthem:• Vesicular lesions evident in successivecrops.

• Often single, discrete lesions or scanty in number in children and much more dense in adults.• Initial lesions are papules (often not observed) that may appear as wheals and quickly evolve to vesicles and initially appear as small “drops of water” or “dewdrops on a rose petal”, superficial and thin-walled withsurrounding erythema. • Vesicles become umbilicated and rapidly evolve to pustules and crusts over an 8- to 12-h period.

• With subsequent crops, all stages of evolution may be noted simultaneously, i.e., papules, vesicles, pustules, crusts, i.e., polymorphic.• Crusts fall off in 1–3 weeks, leaving a pink, somewhat depressed base.• Characteristic punched-out permanent scarsmay persist.• Uncommonly, hemorrhage into pustular lesion occurs in otherwise healthy children, i.e., hemorrhagic varicella

Distribution First lesions begin on face and scalp, spreading inferiorly to trunk and extremities.• Most profuse in areas least exposed to pressure,i.e., back between shoulder blades, flanks, axillae, popliteal and anticubital fossae• Density highest on trunk and face, less on extremities• Palms and soles usually sparedMucous Membranes Vesicles (not oftenobserved) and subsequent shallow erosions (2–3 mm)• Most common on palate• Mucosa of nose, conjunctivae, pharynx, larynx,trachea, GI tract, urinary tract, vagina

• ComplicationsSuper infection by methicillin-sensitive S . aureus (MSSA), methicillin-resistant S . aureus (MRSA), or GASImpetigo, furuncles, cellulitis, and gangrene In children 5–11 years of age, the most common complications are varicella encephalitis and Reye syndrome.• In adults, prodromal symptoms are common and may be severe;Exanthem may last for a week or more, with prolonged period of recovery. • The mortality rate in adults was 15 per 50,000 cases (U.S.); 25% of varicella associated deaths did occur in adults.

Primary varicella pneumonia, which presents 1–6 days after appearance of rash, is relatively common in adults: 16% of adults show x-ray evidence of pneumonitis, but only 4% have clinical signs of pneumonitis. Women have a10% risk of severe VZV pneumonitis.VZV encephalitis may also complicate varicellain adults.• Less common complications of varicella include viral arthritis, uveitis, conjunctivitis, carditis, inappropriate antidiuretic hormone syndrome, nephritis, and orchitis.• Maternal varicella during the first trimester ofpregnancy:

Fetus: Fetal varicella syndrome (limb hypoplasia,eye and brain damage, skin lesions) in 2% of exposed fetuses.Neonatal varicella has higher associated incidence of pneumonitis and encephalitis than occurs in older children.• Immunocompromised or glucocorticoid treatedpatients with varicella may manifest dissemination, hepatitis, encephalitis, and hemorrhagic complications.• If varicella occurs at an early age when maternalantibody is still present, an individual canhave a second episode of varicella.

DIAGNOSISUsually made on clinical findings alone.
MANAGEMENTPreventionImmunization VZV immunization is now available (Varivax) and is 80% effective in preventing symptomatic primary VZV infection. Those at high risk for varicella, who should be immunized, include: normal VZV-negative adults, children with leukemia, and immunocompromised individuals (immunosuppressive treatment, HIVinfection, cancer).

Symptomatic therapyLotions Directed at reducing pruritus.Oral antihistamines Application gives short-term relief of pruritus.Caution re antipyretic agents Antipyretic administration is of concern because of a possible link between aspirinand Reye syndrome in children with varicella. Antiviral agentsOtherwise healthy patients If begun within 24 h after onset of varicella, decreases the severity of varicella andreduces secondary cases.Acyclovir 20 mg/kg (800 maximum) four times daily for ∗5 daysValacyclovir Effective but not an approved use; dosing same as for herpes zoster.