Embed Size (px)
Citation preview

http://aja.sagepub.com/Other Dementias
American Journal of Alzheimer's Disease and
http://aja.sagepub.com/content/14/3/181The online version of this article can be found at:
DOI: 10.1177/153331759901400307
1999 14: 181AM J ALZHEIMERS DIS OTHER DEMENJacqueline M. Stolley, Kathleen C. Buckwalter and Harold G. Koenig
Prayer and religious coping for caregivers of persons with Alzheimer's disease and related disorders
Published by:
http://www.sagepublications.com
can be found at:American Journal of Alzheimer's Disease and Other DementiasAdditional services and information for
http://aja.sagepub.com/cgi/alertsEmail Alerts:
http://aja.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://aja.sagepub.com/content/14/3/181.refs.htmlCitations:
What is This?
- May 1, 1999Version of Record >>
at University of Bucharest on January 28, 2013aja.sagepub.comDownloaded from

��������
This study examined the use of prayer and religious cop-ing among caregivers of persons with Alzheimer’s disease(AD) and related disorders. A repeated measures correla-tional design was used, combined with data from a larger,experimental study (NIH, R01-NR-3434). This expansionstudy and secondary analysis added two instruments, theSpringfield Religiosity Schedule (SRS)1 and the JalowiecCoping Scale (JCS)2 to the original study, as well as struc-tured interviews to determine the role of prayer and religiouscoping in the caregiving stress and coping process. A modifi-cation of Lazarus and Folkman’s3 Stress and Coping modelwas used that included religious variables. Results showedthat caregivers (N = 64) used prayer and religious copingfrequently, that they perceived prayer and trusting in God aseffective coping mechanisms, and that internal religiousactivities helped them get through the caregiving situation.Clinical implications are discussed.
�������
Nearly four million Americans suffer fromAlzheimer’s disease and related disorders (ADRD).4
Caring for persons with ADRD is considered more
stressful than other caregiving situations,5,6 and it isimportant to describe the relationship of coping with stressto caregiver outcomes. Prayer and religious coping, twocomponents of spirituality/religiosity, are mechanismsthat may provide ADRD caregivers with the psychologi-cal stamina to endure caregiving responsibilities.
An impressive number of empirical studies have linkedreligiosity and religious coping to various psychologicaland mental health outcomes.7 Religious coping, an activitythat incorporates the use of personal faith and religiousbeliefs, has been identified as important by persons experi-encing stressful situations in general and caregiving in par-ticular.8 Prayer, a private religious activity that impliescommunication with God, is a religious and/or spiritualactivity that has been reported as a means of adapting andreacting to the uncertainty of life events and coping withthem.9-11 A majority of Americans report that prayer is animportant part of their daily lives,10 and caregivers in par-ticular note the importance of prayer in coping with thecaregiving situation.8 Thus, the purpose of this article is toreport results of a study that examined the use of prayer andreligious coping for caregivers of persons with ADRD.The descriptive study was conducted as a first step inbuilding a stress and coping model for caregivers thatincorporates religiosity. Research questions included:
• How frequently are religious activities andprayer used for coping by caregivers over a yearlong study period?
• What is the perceived effectiveness of prayer asa coping mechanism for caregivers? and
• What do caregivers identify as their most helpfulcoping strategy in the caregiving situation?
181American Journal of Alzheimer’s DiseaseVolume 14, Number 3, May/June 1999
������������� � ����� ���������� �������������� �������� ������
� ������������������ ������
Jacqueline M. Stolley, PhD, RN, CSKathleen C. Buckwalter, PhD, RN, FAAN
Harold G. Koenig, MD, MHSc
Jacqueline M. Stolley, PhD, RN, CS, Professor, Trinity College ofNursing, Moline, Illinois.
Kathleen C. Buckwalter, PhD, RN, FAAN, Associate Provost for theHealth Sciences, Professor, College of Nursing, University of Iowa,Iowa City, Iowa.
Harold G. Koenig, MD, MHSc, Associate Professor of Psychiatry ,Assistant Professor of Medicine, Director, Center for the Study ofReligion/Spirituality and Health, Duke University Medical Center,Durham, North Carolina.
at University of Bucharest on January 28, 2013aja.sagepub.comDownloaded from

������ ������������
The framework for this research was a modification ofthe stress and coping paradigm developed by Lazarus andFolkman. In the Lazarus and Folkman model, the individ-ual is faced with a situation or event, appraises the situa-tion or event as irrelevant, benign-positive, or stressful,and mediates the situation or event by drawing on person-al characteristics and resources, initiating coping activi-ties, and mobilizing social support systems. According toLazarus and Folkman,3 caregiver characteristics andresources that mediate the stressor, include such factors ashealth and energy, material resources, and beliefs.Outcomes are related to effectiveness or ineffectiveness ofthe coping mediators and are measured by somatic health,morale, and social functioning.
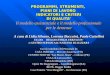
Because the Lazarus and Folkman model is complexand does not specify the role of religiosity in stress andcoping, it was modified to include religiosity as a majorvariable in the paradigm. In the modified model, care-giver characteristics and resources underlie the entirestress and coping process. Religiousness is introduced asa caregiver characteristic and resource, religiosity (orga-nized activity, non-organized activity and intrinsic activ-ity) as a mediator of the stress and coping process, andreligious conservation and/or transformation as out-comes of the coping process. Of particular interest, how-ever, is the role of prayer and religious coping, which aretied to existential beliefs, in coping with the caregivingprocess (Figure 1).
��� � ����� ���������� � �
Analysis of statements made during evaluation of afamily caregiver support group program revealed reli-giosity was a pervasive theme.8 Statements of 31-care-givers were categorized into topics identified asimportant to caregiver support including knowledge ofAD, caregiving problems and strategies, resources, andfeelings. Religiosity was a major coping resourceexpressed by support group members, with prayer iden-tified as a vital source of personal empowerment.
Prayer may be used as a way to accept or find mean-ing in the caregiving situation, or simply asking God ora higher power for strength and support. Use of prayerhas been cited as a mechanism for effective copingamong caregivers, depressed patients, and in olderadults with physical illness and pain.12-14 In fact, stud-ies have shown that 63-95 percent of older adults prayon a daily basis.11,15 More recently, Levin and Taylor10
reported that the use of prayer is strongly correlatedwith age, and that the incidence of daily prayer increas-es with age.
Similarly, Wilson16 found that caregivers turned to spir-ituality for strength when coping with the caregiving situ-ation. Kaye and Robinson17 also found that spiritualitywas an important coping mechanism among wife care-givers of persons with dementia. Compared with non-caregiving wives, dementia caregivers felt closer to Godand used more spiritual behaviors such as prayer and for-giveness to cope. Caregivers also engaged in privateprayer and sought spiritual guidance in making decisionsin their daily lives more often than non caregivers. Findingmeaning, a component of intrinsic religious activity(IRA), was related to lower levels of depression forADRD caregivers in a 1994 study by Farran and col-leagues.18 Moreover, caregivers of persons with ADRDidentified coping activities such as prayer and spiritualguidance as important activities, reporting that the care-giving experience made them feel closer to God.17
��� �����������
Data for this study were obtained from the NationalCaregivers Training Study (NIH, R01-NR-3434), a largemulti-site project testing a psychoeducational model toassist caregivers in caring for persons with ADRD. Twoinstruments, the Springfield Religiosity Schedule (SRS)1
and the Jalowiec Coping Scale (JCS)2 were added to thelarger study to measure religiosity and coping, respec-tively. Completion of the SRS and JCS were optional. Asemi-structured interview was also conducted with 15-randomly selected subjects to determine what copingresources they found most useful and what part religiosi-ty played in the coping process. A repeated measuresdescriptive correlational design was used to examine theassociation between religiosity and coping and variousvariables related to the coping process.
������
The sample consisted of N=64 subjects who complet-ed the entire study period in the National CaregiverTraining Project in Iowa.19 Subjects were caregivers ofdemented elderly and were randomly assigned to thetreatment or comparison groups for a 12-month period.They were recruited from a variety of sources includingGeriatric Assessment Clinics, Alzheimer’s Associationchapters, mental health centers, and recommendationsfrom health care professionals and friends.
A non-respondent questionnaire was sent to subjectswho completed the primary study but did not choose tofill out all of the SRS or the JCS. Results of this surveyshowed that most subjects simply did not want to com-plete another questionnaire. Thus, the optional nature ofthe questionnaires likely explains their non-response.
182 American Journal of Alzheimer’s DiseaseVolume 14, Number 3, May/June 1999
at University of Bucharest on January 28, 2013aja.sagepub.comDownloaded from

183American Journal of Alzheimer’s DiseaseVolume 14, Number 3, May/June 1999
Figure 1. Modified model: Religiosity, coping and caregiving
Caregiver situations and events
1. Cognitive status
2. Problematic behaviors
3. ADL dependents
4. Duration of caregiving
Appraisal
1. Impact
2. Burden
3. Mastery
4. Satisfaction
Coping styles
1. Confrontive
2. Evasive
3. Optimistic
4. Fatalistic
5. Emotive
6. Palliative
7. Supportant
8. Self-reliantOutcomes
1. Somatic health
2. Morale
3. Social functioning
4. Religious conserva-tion or transformation
Social support
1. Guidance
2. Reassurance of worth
3. Social integration
4. Attachment
5. Nuturance
6. Reliable alliance
Religiosity
1. ORA
2. IRA
3. NORA
Caregiver characteristics and resources
1. Health and energy 3. Religiousness 5. Social support and skills2. Material resources 4. Problem solving skills 6. Other (beliefs and commitments)
Med
iato
rs
Shaded area indicates variables under study
at University of Bucharest on January 28, 2013aja.sagepub.comDownloaded from

����� ���������
Initial contact with potential caregiver participantsoccurred during an in-home interview, which was con-ducted by a trained research associate to ensure subjectsmet the following inclusion criteria:
• Be non-paid caregivers;
• Care for an individual diagnosed by a physicianas having ADRD, and who was living in thecommunity;
• Live within two and a half hours of the studysites;
• Provide four or more hours of direct care weekly;
• Had not been exposed to any training based onthe Progressively Lowered Stress Threshold(PLST) model (for the larger study); and
• Had a Global Deterioration score of two orlower (indicating caregivers were cognitivelyintact).
�� �����
After caregivers were admitted to the primary study,they were randomly assigned to the experimental orcomparison group. The Global Deterioration Scale(GDS)20 was administered to the care recipient (for stag-ing disease) and the caregiver (for inclusion criteria).
At the initial interview, caregivers completed an indi-vidualized needs assessment that identified problemsamenable to the intervention. Within two weeks aftersubjects were screened for eligibility, a research associ-ate met with each caregiver. For participants in theexperimental group, the individualized plan of carebased on the Progressively Lowered Stress Threshold(PLST) model21 was presented and practiced. The treat-ment condition (caregiver training) was not central tothis secondary analysis and expansion study. However,although not the focus of this article, an effort wasmade to determine differences in scores between sub-jects in the experimental and comparison groups onreligiosity, and changes in religiousness over time.Procedures for the study reported here were concurrentand identical to those employed in the larger study,except that participants were asked to voluntarily com-plete the SRS at the four data collection points (baseline,three, six, 12-months) and the JCS at the 12-month datacollection point only.
����������
Demographic, descriptive and disease staging dataobtained in the larger study were used for this secondaryanalysis. As noted, the SRS and JCS were added.
��� � � ��
The Springfield Religiosity Schedule (SRS)1 mea-sured the religiosity of caregivers (Baseline, three, six,and 12-months). Items comprising the instrument wereelicited from a variety of scales in existence,22-25 whichhave been widely tested with acceptable reliability andvalidity. The SRS consists of 34-items with Likert-typeanswers. Content validity was provided by a panel ofChristian and Jewish clergy. Reliability was tested bycomputing alphas for data obtained from surveying asample of 836-community-dwelling older adults. Factoranalysis revealed three major factors:
• Organized religious activity (ORA);
• Non-organized religious activity (NORA); and
• Intrinsic religious activity (IRA).
Test-retest reliability after six weeks revealed an over-all agreement of 91.7.1 Total SRS and/or subscale scores(ORA, NORA, IRA) can be used for analysis.
Further analysis using religious coping items and aprayer index can be used.1 The prayer index is calculatedby combining and averaging the scores of two items.Item 17 is “Private prayer is important in my life.” Item20 is a negatively worded item, “Prayer does NOT helpme to cope with difficulties and stress in my life.” Bothare rated on a six point scale ranging from strongly agree(1) to strongly disagree (6). The prayer index results in ascore ranging from 1-6 with higher scores indicatinggreater value for prayer.
Religious coping items include item 15, “While deal-ing with difficult times in my life, I don’t get much per-sonal strength and support from God” and item 20,described previously. The religious coping score resultsfrom combining and averaging answers to these twoitems with scores ranging from 1-6, with higher scoresindicating greater religious coping.
� �
Jalowiec Coping Scale (JCS), revised version2 wasused to measure coping and coping effectiveness. TheJCS is a 60-item, zero to three point rating scale thatassesses eight specific coping styles: emotive, evasive,
184 American Journal of Alzheimer’s DiseaseVolume 14, Number 3, May/June 1999
at University of Bucharest on January 28, 2013aja.sagepub.comDownloaded from

185American Journal of Alzheimer’s DiseaseVolume 14, Number 3, May/June 1999
Table 1. Baseline demographic characteristics
Variable N Percent Mean* SD* Mode* Median*
Gender
Male 16 25
Female 48 75
Total 64 100
Ethnicity
White 64 100
Age (range 35-87 years) 65.6 12.26 78 68
35-45 3 5
46-55 9 14
56-65 11 17
66-75 20 31
76-85 20 31
86 and over 1 2
Total 64 100
Education (range 8 - 23 years) 13.5 3.05 12 12.5
Grade school 2 3
Some high school 4 6
High school graduate 28 44
Some college 12 19
College graduate 11 17
Post college 7 11
Total 64 100
Caregiver relationship to care recipient
Spouse 47 73
Child 11 17
Sibling 0 0
Other relative 5 8
Friend 1 2
Total 64 100
Religious preference
Protestant 35 55
Catholic 12 19
Jewish 0 0
None or other 6 9
Missing 11 17
Total 64 100
* If applicable
at University of Bucharest on January 28, 2013aja.sagepub.comDownloaded from

confrontive, fatalistic, optimistic, palliative, self-reliant,and supportant. Each item is rated separately as to useand effectiveness.
The JCS has been widely used and has ample psycho-metric support as summarized by Jalowiec2 from 12studies. Because of the focus of this study on religiouscoping, as well as the small sample size, only the sum ofJCS item 17’s use and effectiveness scores were used toanswer the research questions, “how frequently is prayerused as a coping mechanism for caregivers over the 12-month study period?” and “What is the effectiveness ofprayer as a coping mechanism for caregivers?”
������ �����������!����
Following signed consent for the larger study, sub-jects were informed of the added tools, (SRS and JCS),and the fact that filling them out was optional. Furtherconsent for the semi-structured interview was implied byreturn of the form describing the interview and request-ing respondents indicate times to be called.
�������
�������� �� ������������
The sample consisted of 64-subjects, including the53-subjects who completed the SRS at least twice duringthe study period (Table 1). T-tests conducted to deter-mine differences in religiosity over time or betweengroups found no statistically significant differences.
����������������� �� ����
To determine how frequently religious activities andprayer were used for coping over the 12-month studyperiod, several descriptive statistics were calculated.Initially, frequencies and percents were computed foranswers to SRS questions 15, 17 and 20. Then, two itemson the SRS were combined and averaged to form aprayer index and religious coping. The frequencies andpercentages illustrating baseline and 12-month data canbe found in Table 2. Of particular interest are theresponses of subjects regarding the use of prayer andreligious coping, along with age differences in thesevariables. Ages were divided into four groups: 35-55years, 56-65 years, 66-75 years, and 76 and over.
Of the 60-items on the JCS, prayer and trusting God(item 17) ranked sixth (when considering ties) in fre-quency of use, with 61 percent (N = 22) of subjects stat-ing that they “often used” this item. Of the 36-subjectswho answered item 17 of the JCS, 61 percent (N = 22)reported they “often used” this coping item. Responses
by age group revealed that 88 percent of subjects age 76and older often prayed and put their trust in God; 67 per-cent of those between ages 66-75; 33 percent of thosebetween ages 56 and 65; and 60 percent of those 35-55years of age. Item 17 was within the four most frequentlycited coping items for persons age 76-years and over.
������������� ��������
To determine the perceived effectiveness of prayer asa coping mechanism, a bivariate correlation (r = .89, p =.01) was calculated between the use score of JCS ques-tion 17 and the associated effectiveness score (N = 35).Thus, a strong, significant relationship between prayeruse and perceived effectiveness was revealed.
� ���������������
Subjects who scored high, moderate and low on SRStotal score were interviewed. In order to determine thosecategories, baseline SRS total scores were summed andquartiles calculated. The lowest quartile were scores of104 and below, indicating low religiosity. The highestquartile included scores of 153 and above, indicatinghigh religiosity. The middle two quartiles, ranging from105 to 152, were considered moderate religiosity. Of the39-subjects who agreed to be interviewed, 15 were ran-domly selected for the telephone interview: five withhigh religiosity; five with moderate religiosity; four withlow religiosity; and one subject who provided no SRSdata at any data point. Subjects were telephoned at a timeconvenient for them, and interviews were tape recordedand transcribed verbatim. The remaining 24-subjectswere telephoned but not formally interviewed.
Subjects were asked the following question:“Throughout your caregiving experience, there havebeen difficult times. What has helped you most to cope?”If the subject did not spontaneously mention spiritual orreligious coping activities, the following question wasasked: “Has your religion or spiritual belief been of helpthrough this experience? Why or why not?” Severalthemes emerged from these interviews. Of particularinterest was the frequency of religious coping activitiesas illustrated by these subjects’ statements reflectingresponses from subjects with high, moderate and lowreligiosity, respectively.
" ������ � � ��
My faith in God. I believe it was more my person-al faith because we couldn’t go to church veryoften due to the inability to handle him outside thehome. It’s relying on Him day by day...At times
186 American Journal of Alzheimer’s DiseaseVolume 14, Number 3, May/June 1999
at University of Bucharest on January 28, 2013aja.sagepub.comDownloaded from

187American Journal of Alzheimer’s DiseaseVolume 14, Number 3, May/June 1999
Table 2. Frequency of prayer: Responses with the value 6, strongly agree or strongly disagree (SRS)
Variable Data point Frequency (percent, rounded) by age in years
35-55 56-65 66-75 76 & over Total
SRS 15 N n(%) N n
(%) N n(%) N n
(%) N n(%)
While dealing with dif-ficult times in my life, Idon’t get much personalstrength and supportfrom God.
Baseline 16 8(50) 13 10
(78) 18 10(56) 22 15
(68) 69 43(62)
12-month 7 5(71) 6 4
(67) 7 5(71) 9 7
(78) 29 21(72)
SRS 17 N n(%) N n
(%) N n(%) N n
(%) N n(%)
Private prayer isimportant in my life.
Baseline 17 9(53) 13 7
(54) 18 8(44) 22 18
(82) 70 42(60)
12-month 7 4(57) 6 3
(50) 7 5(71) 9 7
(78) 29 19(66)
SRS 20 N n(%) N n
(%) N n(%) N n
(%) N n(%)
Prayer does not help meto cope with stress.
Baseline 16 11(69) 13 8
(62) 18 11(61) 22 17
(77) 70 47(68)
12-month 7 6(86) 6 3
(50) 7 5(71) 9 7
(78) 29 21(72)
Prayer index N n(%) N n
(%) N n(%) N n
(%) N n(%)
(#17 + #20)
Baseline 33 20(61) 26 15
(58) 36 19(53) 44 35
(80) 140 89(64)
12-month 14 11(79) 12 6
(50) 14 10(71) 18 14
(78) 58 41(71)
Religious coping N n(%) N n
(%) N n(%) N n
(%) N n(%)
(#15 + #20)
Baseline 32 19(59) 26 18
(69) 36 21(58) 44 32
(73) 139 90(65)
12-month 14 11(79) 12 7
(58) 14 10(71) 18 14
(78) 58 42(72)
at University of Bucharest on January 28, 2013aja.sagepub.comDownloaded from

when I was at my wits end, I would just go in theother room and just say “Lord help me.” (55-year-old, Protestant female).
(My spirituality) most certainly has helped. Mypersonal religiousness, prayer, faith in God,that’s what keeps me going. The church helped,mostly in visiting. It’s hard for some people tocope with it and that’s the hardest part. I guessmoral support an spiritual support is what thechurch gives me (77-year-old Protestant male).
To be real honest, having faith in God helps mecope most and having an opportunity, that’sabout the only place I get anymore is to church. Ifind that is a refuge for me. It gives me timewhere I have to be still and can’t do anything.It’s my private walk with God (that’s mostimportant) Spending time in the word, becausethe word is a source of faith and promise andhope. Knowing that God can get me throughthis, that I’m not alone, and that He sends Hisangels to watch over us and to help us. It justseems that God is there to meet our needs. But itis a private walk with God. And it seems to methat the more you’re taxed, the more you’redrawn closer to God. I believe God gives usgood things and He doesn’t bring calamitiesupon us to teach us lessons or anything else. (53-year-old, Protestant female).
#���������� � � ��
I just pray, God, hold my hand. Gave mestrength to keep going. The church encouragesme by saying they’re praying for me and thistype of thing. Which makes me feel internallybetter. The minister has been supportive. (52-year-old, Protestant female).
I guess I knew I had a source of being there that Icould go to when I was overwhelmed. And itseemed like I could reach down inside for thatstrength that I feel that comes from a God. And Iwould do a lot of praying during the day askingfor patience and asking for understanding andthese seemed to come about. I got a lot of com-fort from going to the church itself and sharingwith many people in the congregation. (60-year-old, Protestant female).
I just turned it over to the good Lord. You’renever given any more than you can handle. And
I had a group of men, young ones, old ones, thesame thing they would say is ‘we’re praying foryou.’ My faith has gotten deeper. Now that I’molder, I can see where the good Lord preparedme for all of these things ahead of time. (79-year-old, Catholic male).
$����� � � ��
The thing (about religion) that helps me the mostis you enter the sanctuary and sit quietly for awhile and I think sitting quietly before the ser-vice probably is the most religious moment ofthe morning. It helped me in my thoughts. Justsome silent prayers. Religion is a private thing.(80-year-old, Protestant male).
I can’t say that it (religion) did help. (79-year-old, Protestant male)
I’ve just made myself realize I have to keeppeace of mind and I have to cope with it. (85-year-old female, no religion).
Religion did not really help. (53-year-old,Catholic female).
The one subject who did not complete the SRS at anydata point gave this reply:
I guess religion and stuff really helped me. Imean I just knew God was helping me. My reli-gion helped me cope. I didn’t go to church, I did-n’t have anybody helping me. I just felt like Godwas watching over me. And every time I cameup against something that I just didn’t think Iwas going to make it, it would just seem likesomebody would just kind of take over andthings would get better and I’d go on and thingswould be okay. (57-year-old female).
Of the remaining 24-subjects whose interviews werenot structured, four spontaneously identified prayer andone identified ORA as coping mechanisms. Twelve sub-jects identified private religiousness and two identifiedORA when asked if their religiosity or spirituality helpedthem cope. Other themes not discussed in this article thatemerged were social support, problem solving, knowl-edge, commitment, material resources, and humor.
� ����� ���� � ��
Characteristics of subjects in this study are consistent
188 American Journal of Alzheimer’s DiseaseVolume 14, Number 3, May/June 1999
at University of Bucharest on January 28, 2013aja.sagepub.comDownloaded from

with those of other studies: Older, female, living with thecare recipient and caring for someone with a diagnosis ofADRD.26-28 The lack of ethnic and religious diversityand higher level of education of this sample reflects per-sons in Iowa, a state with few minorities and one of thehighest literacy rates in the country, as well as aUniversity-related study site where many highly educat-ed people reside.
����������������� �� ����
As noted earlier, prayer is defined as a private reli-gious activity that implies communication with God.Responses to item 15, “While dealing with difficulttimes in my life, I don’t get much personal strength andsupport from God,” in the SRS showed that the majori-ty of subjects strongly disagreed with this statement,with the percentage in disagreement increasing frombaseline to 12-months. All responses reflecting the useof prayer and religious coping increased from baselineto 12-months with the exception of those in the 56 to 65year old group. A similar phenomena was noted forquestions 17 (Private prayer is important in my life)and 20 (Prayer does not help me to cope with stress inmy life). Scores in the 56 to 65-year old group fluctuat-ed during the 12-month study period, particularly foritem 17. The reason for this is impossible to determinefrom the data available, but could be related to the pos-sibility that only those persons who were very religiouscompleted the SRS after baseline. Additionally, subjectattrition could have contributed to selection bias.However, it is entirely possible that varied use of prayeractually did occur during this time of life transitions(e.g. empty nest, grandparenting, and retirement), withless focus on this religious activity.
������
The importance of prayer is apparent for caregiverswho responded to these questions. Using the prayer indexalone, 64 percent of the respondents indicated heavyreliance on prayer. Other research has shown that 63 to 95percent of persons pray on a daily basis.10,11,15 Findingsfrom this study support the powerful function of prayer asa coping mechanism for caregivers as postulated in themodified paradigm, and reported in other studies.8
Age differences in the use of prayer are of interest.Levin and Taylor10 found that 40 percent of persons age18 to 30 pray daily, over 45 percent of persons ages 31 to40, almost 58 percent of persons ages 41 to 60 androughly 73 percent of persons over age 61 pray on a dailybasis. Findings from this study reflect similar results,although the age groupings are not equivalent. Using the
prayer index, 53 percent to 80 percent of persons over66-years of age reported that prayer is important to them.Surprising results are that the younger age caregivers,those 35 to 55-years, also report heavy reliance on prayer(61-79 percent). The lowest reliance on prayer was notedin the 56 to 65 year old age group (50-58 percent). Thereason for the high use of prayer in the youngest agegroup and lower use of prayer for the second age group ispuzzling. However, in most cases, in all age groups, atleast 50 percent of caregiver respondents indicated heavyreliance on prayer throughout the twelve-month caregiv-ing experience. Additionally, the use of prayer increasedfrom baseline to twelve months, perhaps reflecting anincreased use of emotion-focused coping over the dura-tion of a stressor, as has been noted in other caregiverresearch.29 Although prayer is considered a religious cop-ing activity, it has also been conceptualized as an emotion-focused coping activity. With the progressive nature of thedisease and the realization that nothing can be done toreverse ADRD and other dementias, the caregiver mayrely on those activities that are geared toward regulatingtheir emotions rather than solving problems.
Further support for the importance of prayer is thehigh percentage of caregivers who identified prayer as acoping mechanism: 61 percent of the sample stated they“most often used” or “prayed or put your trust in God”for coping. Age differences in response to this questionare similar to those for the prayer index, with the lowestscores obtained in the 56 to 65-year old age group, andthe highest scores in the 76 and over group. Of the 60-items on the JCS, praying or putting trust in God rankedsixth in coping activities, which is quite impressive. Thisresult is stronger than that reported by Parker andBrown,13 who found that prayer was ranked seventh inperceived effectiveness as a coping behavior out of only25 possible responses. The correlation between prayeruse and perceived effectiveness was quite strong, (r =.89), further pointing to the importance of this privatereligious activity for caregivers, particularly for coping.
The frequency of prayer has been studied by oth-ers,9,10,30 although the reasons for prayer are not clearlydelineated in these studies. Results of this study clearlyportray the use of prayer for coping with caregiving as evi-denced by the wording of JCS #17, which asks how oftenprayer and trusting in God were used for coping. Indeed,the study by Whitlach and colleagues indicated that prayerwas a vital source of personal empowerment for care-givers, a finding that is strongly supported by this study.8
������ �� ����
Religious coping is defined as a coping activity thatincorporates the use of personal faith and religious
189American Journal of Alzheimer’s DiseaseVolume 14, Number 3, May/June 1999
at University of Bucharest on January 28, 2013aja.sagepub.comDownloaded from

beliefs. Religious coping has been identified in the faceof a stressful life situation or event,11,31,32 and for care-givers in particular.8,16 Results of this study also illustratereligious coping as an important resource for caregivers.Over the course of the twelve-month study period, 64 to72 percent of the total sample identified religious andspiritual beliefs and activities as coping mechanisms.Age differences in the findings were similar to those forthe prayer index—the youngest and oldest age groupsnamed religious activities for coping.
Answers to the semi-structured interviews support themodified stress and coping paradigm, particularly in rela-tion to prayer and religious coping. Sixteen (41 percent) ofthe subjects who were either formally or informally inter-viewed spontaneously reported religious coping activitiesas most helpful. These religious activities included per-sonal belief systems such as faith and prayer. Less fre-quently, organized religious activity (ORA) wasmentioned as a primary coping activity. Of the subjectswho completed the semi-structured tape-recorded inter-view and spontaneously mentioned religious coping activ-ities, four scored high on religiosity, one scoredmoderately, and one had no data regarding SRS.
The importance of religious coping was reinforcedby the number of persons who mentioned religious cop-ing activities when asked specifically. Thirty nineresponses, representing 20-subjects (51 percent), identi-fied that religious activities were important for coping.Most commonly, private religiousness was identified, acomponent of religiosity that includes not only intrinsicreligious activity (IRA), but also belief systems regard-ing God and religion. ORA was mentioned less frequent-ly, but subjects commented on the importance ofcongregation and clergy support, and church attendance.Only one subject identified non-organized religiousactivity (NORA), watching religious television pro-grams, as a fulfilling coping activity.
Perhaps the most profound religious coping activityidentified by caregivers was prayer. These data are notsurprising in light of the number of subjects of all ageswho reported that they pray frequently and/or use prayerto cope, both in this study and in those conducted by oth-ers.8,10,11,15 Furthermore, caregivers stated that privateprayer by themselves or shared with the care recipient,and prayers said for them by friends and members oftheir religious congregations gave them a sense of peace,strength, and answers to caregiving problems.
Another religious coping mechanism identified bycaregivers was belief and faith in God. Ten of the 15caregivers (66 percent) who completed the semi-struc-tured interview stated that their faith in God, and theirbelief that God was helping them, strongly supportedtheir caregiving efforts. Several respondents said that
God or Christ was with them, not only providingstrength, but also providing answers to caregiving dilem-mas. This finding is particularly important in view ofdata from the Iowa Governors Task Force (1989) inwhich subjects stated that God helped them in their care-giving efforts.19 Moreover, research by Whitlach andcolleagues8 reported the importance of faith and theassistance of the divine in the caregiving process. Thus,the resource of religiousness, coupled with religiouscoping activity, were seen as major components of thecoping process for caregivers. None of the caregiversblamed God for the illness of the care recipient. On thecontrary, subjects who addressed this issue stated that theydid not believe that God was responsible for the disease,but felt that He was available for strength and guidance,conserving or transforming religiousness. It is not surpris-ing that three of the subjects with low religiosity scoresdid not rely on religious coping activities. These subjectsidentified other activities such as learning about the dis-ease and dealing with caregiving as more important.
$ � ��� �
Limitations of this study included the descriptivenature of the design and the use of a primary study forthis expansion study and secondary analysis. Therefore,it is impossible to infer cause and effect. However,because most data for this study were collected at thesame time as the primary study, they likely captured sig-nificant variables simultaneously with the primary study,rather than retrospectively. Additionally, this study isgeneralizable only to the population involved—homecaregivers of ADRD patients within Iowa.
����
Religious coping activities, particularly private activi-ties, were identified as most helpful during the caregiv-ing process. This finding is supported by the majority ofcaregivers who reported that prayer and religious copingactivities were prominent in their lives. While ORA andNORA were found to be helpful, private religious activi-ties such as IRA and beliefs were most helpful. Theresponse of subjects citing religious coping behaviors asmost helpful is impressive and consistent with otherstudies, as well as the modified stress and coping para-digm. Continued testing of this paradigm is recommend-ed with a larger sample size so that multivariate analysiscan be conducted and curvilinear relationships detected.
These findings warrant further investigation anddevelopment of interventions that tap this importantresource. Interventions based on religious coping can becost effective and may diminish many of the negative
190 American Journal of Alzheimer’s DiseaseVolume 14, Number 3, May/June 1999
at University of Bucharest on January 28, 2013aja.sagepub.comDownloaded from

effects of caregiving. By recognizing the potential powerof this resource and incorporating it into care and care-giver support, health professionals can deliver holisticcare, encourage effective coping, assist the client to findmeaning, and serve as a support for clients experiencingreligious transformation.
�����������The larger study from which this study was elicited, was funded by
the National Institutes of Health, R01-NR03434, K.C. Buckwalter, PI.
���������1. Koenig HG, Smiley M, Gonzales JP: Religion, Health, and Aging:A Review and Theoretical Integration. New York: Greenwood Press.1988b.2. Jalowiec A: Jalowiec Coping Scale (revised). Unpublished manu-script. 1987. University of Illinois, Chicago.3. Lazarus RS, Folkman S: Stress, appraisal, and coping. New York:Springer. 1984.4. Evans L, Funkenstein HH, Albert MS, et al: Prevalence ofAlzheimer’s disease in a community population of older persons.JAMA. 1989; 262: 2551-2556.5. Irwin M, Brown M, Pattern T, et al: Neuropeptide Y and naturalkiller cell activity: Findings in depression and Alzheimer caregiverstress. The FASEB Journal. 1991; 5: 3100-3107.6. Schulz R, O’Brien AT, Bookwala J, Fleissner K: Psychiatric andphysical morbidity effects of dementia caregiving: Prevalence, corre-lates, and causes. The Gerontologist. 1995; 35: 771-791.7. Levin JS: Religion and health: Is there an association, is it valid,and is it causal? Social Science Medicine. 1994; 38(11): 1475-1482.8. Whitlatch AM, Meddaugh DI, Langhout KJ: Religiosity amongAlzheimer’s disease caregivers. The American Journal ofAlzheimer’s Disease and Related Disorders & Research. 1992; 7(6):11-20.9. Dossey L: The return of prayer. Alternative Therapies in Healthand Medicine. 1997; 3(6): 10-17.10. Levin JS, Taylor RJ: Age differences in patterns and correlates ofthe frequency of prayer. Gerontologist. 1997; 37(1): 75-88.11. Koenig HG, George, Siegler IC: The use of religion and otheremotion-regulating coping strategies among older adults.Gerontologist. 1988a; 28(3): 303-310.12. Pearlin LI, Mullan JT, Semple SJ, Skaff MM: Caregiving and thestress process: An overview of concepts and their measures.Gerontologist. 1990; 30(5): 583-593.13. Parker GB, Brown LB: Coping behaviors that mediate betweenlife events and depression. Archives of General Psychiatry. 1982; 39:1386-1391.
14. Bearon LB, Koenig HG: Religious cognitions and use of prayer inhealth and illness. The Gerontologist. 1990; 30(2): 249-253.15. Princeton Religion Research Center. 1982 Religion in America.Princeton, NJ: The Gallup Poll. 1982.16. Wilson HS: Family caregiving for a relative with Alzheimer’sdementia: Coping with negative choices. Nursing Research. 1989;38: 94-98.17. Kaye J, Robinson KM: Spirituality among caregivers. Image.1994; 26(3): 218-221.18. Farran CJ, Miller B, Kaufman JE, Davis L: Finding meaning as amoderator of caregiver distress: A comparison of African Americanand White caregivers of persons with dementia. Unpublished manu-script. 1994.19. Iowa Governor’s Task Force on Alzheimer’s Disease and RelatedDisorders Final Report. (1989) Des Moines, Iowa.20. Reisberg B, Ferris SH, deLeon MJ, Crook T: The global deterio-ration scale for assessment of primary degenerative dementia.American Journal of Psychiatry. 1982; 139(9): 1136-1139.21. Hall GR, Buckwalter KC: Progressively lowered stress threshold:A conceptual model for care of adults with Alzheimer’s disease.Archives of Psychiatric Nursing. 1987; 1(6): 399-406.22. Allport GW, Ross JM: Personal religious orientation and prejudice.Journal of Personality and Social Psychology. 1967; 5: 423-443.23. Glock CY, Stark R: Religion and Society in Tension. New York:Rand McNally. 1965.24. Hoge DR: A validated intrinsic religious motivation scale.Journal for the Scientific Study of Religion. 1972; 11: 369-376.25. Paloutzian RF, Ellison CW: Loneliness, spiritual well-being, andquality of life. In Peplau A, Porlman D, (eds): Loneliness: ASourcebook of Current Theory, Research and Therapy. New York:Wiley Inter Science. 1982: 224-237.26. Gwyther L: Research on gender and family caregiving: Implicationsfor clinical practice. In Dwyer JW, Coward RT, (eds.): Gender, Familiesand Elder Care. 1992: 202-218. Newbury Park: Sage. 27. Miller B, Montgomery A: Family caregivers and limitations insocial activity. Research on Aging. 1990; 12: 72-93.28. Pruchno R.A: The effects of help patterns on the mental health ofspouse caregivers. Research on Aging. 1990; 12(1): 57-71.29. Killeen M: The influence of stress and coping on family care-givers’ perceptions of health. International Journal of Aging andHuman Development. 1990; 30(3): 197-211.30. Koenig HG (ed.): Research on Religion and Aging. Westport,Conneticut: Greenwood Press. 1995.31. Conway K: Coping with the stress of medical problems amongblack and white elderly. International Journal of Aging and HumanDevelopment. 1985; 21(1): 39-48.32. Manfredi C, Pickett M: Perceived stressful situations and copingstrategies utilized by the elderly. Journal of Community HealthNursing. 1987; 4(2): 99-110.
191American Journal of Alzheimer’s DiseaseVolume 14, Number 3, May/June 1999
at University of Bucharest on January 28, 2013aja.sagepub.comDownloaded from