Embed Size (px)
Citation preview

Evaluating Lung Nodules in an Endemic Region for
CoccidioidomycosisLung Nodule Conference
Michael W. Peterson, M.D.Valley Medical Foundation
Professor and Chief of MedicineUCSF Fresno

Overview of the Talk
Overview for evaluating lung nodules Challenges applying National
Guidelines in Fresno Evolving tools in the Central Valley

Cancer Death Rates for Men

Cancer Death Rates for Women

Cancer Survival by Stage

The Challenge
56 year old male current smoker with 40 pack years.He has an unintended 10 pound weight loss without other constitutional symptoms.
67 year old woman lifetime nonsmoker who had symptoms of a respiratory infection 3 months agopresents with this chest CT scan. Currently asymptomatic.

Overview of the Talk
Overview for evaluating lung nodulesOverview for evaluating lung nodules Challenges applying National
Guidelines in Fresno Evolving tools in the Central Valley

Clinical Issues Related to Risk
Clinical risk factors (Pretest Probability)– Underlying risk:
• Exposure (tobacco, radon, asbestos)• Age• Gender (male>female)• Presence of chronic lung disease• Personal history of malignancy• First degree relative with lung cancer

Approach to Evaluating Lung Nodules
Clinical risk factors (Pretest Probability) Radiological characteristicsRadiological characteristics Special characteristics

Radiological Criteria: Size
Radiological characteristics– Size: one of the
most important factors in your evaluation
Size Risk
<3 mm 0.2%4-7 mm 0.9%8-20 mm 18%
>20 mm 50%

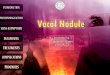
Radiological Criteria: Border, Calcification and Growth
Spiculated border/corona radiata Stippled or eccentric calcification Growth rate

Nodule Demonstrating “Corona Radiata”

Dense Central Calcification = Benign Disease

Clinical Issues Related to Risk
Radiological characteristics– Growth rate: usual doubling time between
20 and 400 days• Three dimensional growth (30% increase in
diameter = doubling volume; volume = r3)• Screening and review has questioned the
“two-year rule”

Nodule Growth Rate
Average doubling times for lung nodules
Radiographic Characteristic Doubling Time
Ground glass 813 days
Ground glass with solid component
457 days
Solid 149 days
Problem: accurate measurements of nodulesDoubling times shorter in smokers
Hasegawa, BMJ, 2000

Solid Nodule

Ground Glass Nodule

Clinical Issues Related to Risk
Clinical risk factors (Pretest Probability) Radiological characteristics Special characteristics Risk stratification

Proposed Guideline: Solid Lung Nodules
Chest. 2013;143(3):840-846

Lung Nodules and Fresno’s “Friend”

Proposed Guideline: Solid Lung Nodules
Chest. 2013;143(3):840-846

Representative Cases: On Line Calculators
56 year old male current smoker with 40 pack years.He has an unintended 10 pound weight loss without other constitutional symptoms.
67 year old woman lifetime nonsmoker who had symptoms of a respiratory infection 3 months agopresents with this chest CT scan. Currently asymptomatic.
Coccidioidomycosis Adenocarcinoma of the lungCoccidioidomycosis Adenocarcinoma of the lung
Calculated Risk 33-75% Calculated Risk 2.5-7.2%Calculated Risk 33-75% Calculated Risk 2.5-7.2%

Analysis of Previous Calculators
Probability of Cancer Coccidioidomycosis CancerAverage 60.8 ± 38.1 59.2 ± 30.7<5 % N: 10 (9%) N: 4 (2%)5-60% N: 38 (35%) N: 92 (48%)>60% N: 62 (56%) N: 96 (50%)
Coccidiodomycosis CancerAverage 25.9 ± 21 52.8 ± 23<5 % N: 18 (16%) N: 3 (2%)5-60% N: 82 (75%) N: 93 (48%)>60% N: 10 (9%) N: 96 (50%)
Coccidiodomycosis CancerAverage 69.5 ± 38 76.6 ± 22.4 <5 % N: 6 (5%) N: 3 (2%)5-60% N: 50 (45%) N: 112 (58%)>60% N: 54 (50%) N: 77 (40%)
Mayo Clinic
Brock Univ.
BayesianModel

Effectiveness of Serology to Differentiate Lung Cancer
from Cocci
Nicola et al., ATS
Sensitivity(95% CI)
Specificity(95% CI)
Positive predictive value
(95% CI)
Negative predictive value
(95% CI)
Coccidioides serology by immunodiffusion
77%(68-84)
93%(89-96)
86%(77-91)
89%(84-92)
Coccidioides serology by complement fixation
51%(42-61)
98%(96-99)
92%(82-96)
79%(74-84)

Differentiation Based on the Radiographic Appearance of the
Lung Nodules Two chest radiologists reviewed chest
CT scans from 302 patients in a blinded fashion. All patients had a biopsy-proven diagnosis of Cocci or Lung cancer
Ronaghi, ACCP 2015

Radiographic Appearance of Nodules
Radiographic Charateristic Cocci Lung Cancer
P-Value
Diameter (cm) 2.9 ± 1.6 4.2 ± 2.5 .0001
Satellite lesions present 59% 14% .001
Chronic Lung Disease present 19% 66% .0001
Solid Density 80% 82% NS
Cavitary Nodule 5% 6% NS
Cavity wall thickness (mm) 4.8 ±2.7 4.4 ± 2.9 NS
Mediastinal adenopathy 57% 62% .035
Ronaghi, ACCP 2015

Project Goal
To develop a calculator that better differentiates nodules due to Cocci

Methods Developed using
302 patients – 192 Lung Cancer and 110 Cocci
Using backward regression – we identified 9 clinical and radiographic variables from 20
Calculated odds ratio for each of the variables for cancer
Odds ratio was used to calculate a numerical value weighted for lung cancer

UCSF – Fresno CalculatorVariable 0 Points 1 Point 2 Points 3 Points 4 Points TotalAge Dx < 50 50-55 55-59 60-64 65+ Gender Male Female Smoking Hx Never Past Current
Occup. Other Construct. Field Work Mechanic Military
Chronic Lung Disease Hx
None Asthma Bronchitis COPD COPD+Asthma
Lung Disease on CT
None/Other Emphysema/Reticular
Nodule Location
RML LLL RLL RUL LUL
Nodule Border-
Smooth Lobulated Spiculated
Family Hx None Asthma/COPD Lung ca
Nodule Size < 2cm >2 cm Total

Results Learning Set (238
patients):– Cocci patients (N =
41): mean score 8.9 (95%CI: 5.1-12.7)
– Lung Cancer (N = 192): mean score 19.6 (95% CI: 14.6-24.6)

Results
We next applied the scoring system to 143 patients who were not included in the learning set
117 patients had lung cancer and 26 patients had Cocci

Results Testing Set (117
patients):– Cocci patients (N =
26): mean score 9.1 (95%CI: 1.7-16.5)
– Lung Cancer (N = 117): mean score 25.2 (95% CI: 15.4-30.0)

Proposed Guideline: Solid Lung Nodules
Chest. 2013;143(3):840-846

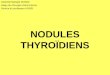
Use of FDG-PET Scanning Principle that malignant lesions have
higher metabolic rates Limitations:
– At least 8 mm in size– Diabetic control– Cost– Best utilized in the moderate risk group– Poor anatomic localization

Combined PET-CT
SUV 4.5

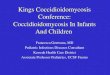
PET CT to Evaluate Lung Nodules
SUV 3.75

PET Activity in Lung Cancer versus Cocci Nodules
SUV 2.5
Lung; published on-line May 7, 2014

FDG-PET for Lung cancer Risk Calculation
Reviewed 70 published studies between Oct 2000 and April 2014 that evaluated nodules by PET
Compared test performance between sites with endemic fungal disease and those in non-endemic regions
SA Deppen et al, JAMA, 2014

Results of the Meta Analysis Overall (70 STUDIES):
– Sensitivity: 89%– Specificity: 75%
Nonendemic regions (60):– Sensitivity: 89%– Specificity: 77%
Endemic regions (10):– Sensitivity: 94%– Specificity: 61%
SA Deppen et al, JAMA, 2014

Conclusions Evaluating lung nodules remains a
challenging exercise for clinicians Guidelines must be interpreted and utilized
within the context of local conditions We have limited tools for differentiating
nodules due to Cocci from lung cancer A multidisciplinary clinic provides us the
opportunity to develop our local guidelines

Future and Ongoing Projects
Refining and testing the nodule prediction tool prospectively
Evaluating the performance of recently developed PCR for Cocci
Development of a tissue and clinical database to share for clinical research
Evaluating the impact of the program on patient quality of life

Acknowledgments CRMC for supporting
the Lung Nodule Clinic Kathy Norkunas, Nurse
Navigator Paul Mills, PhD, MPH Kathy Bilello, MD Karl Van Gundy, MD
Daya Upadhyay, MD Gurpreet Bambra, MD Ali Rashidian, MD Mickey Sachdeva, MD Reza Ronaghi, MD Summer Biomedical
Intern Program