Embed Size (px)
Citation preview
Hypertensive Pulmonary Edema
Sean Collins, MD, MScAssociate ProfessorVanderbilt University
Department of Emergency Medicine
Disclosures
• Consultant: Novartis, Cardiorentis, The Medicines Company, Medtronic
• Research Support: NIH, PCORI, Novartis, Cardiorentis, Trinity
AHF and Elevated BP
Hypertensive Pulmonary Edema
Hypertensive Pulmonary Edema
Scenario
• 75 YO F with h/o HTN and HF with SOB• BP- 180/100 P-80 RR-24 Satn- 84%• Moderate respiratory distress• Diffuse rales; +JVD, trace leg edema• CXR = pulmonary edema; U/S = comet tails• Treatment?
Q: Initial stabilization for this patient may include which of the following?
• a) Non invasive ventilation• b) Sublingual/IV nitrates• c) Dobutamine• d) 1) and 2)• e) All of the above
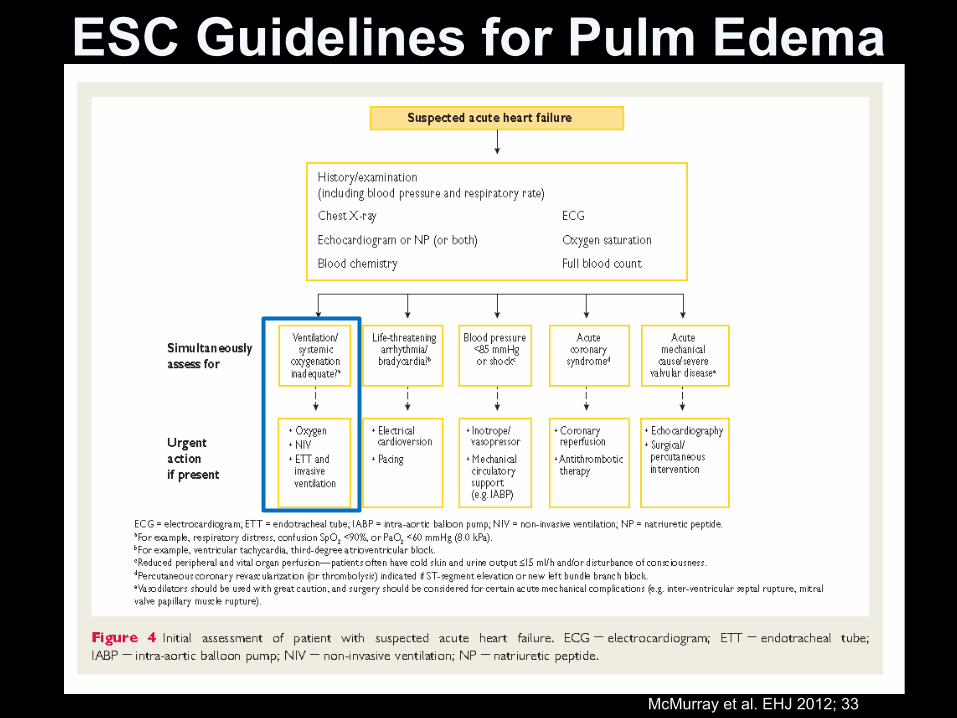
ESC Guidelines for Pulm Edema
McMurray et al. EHJ 2012; 33
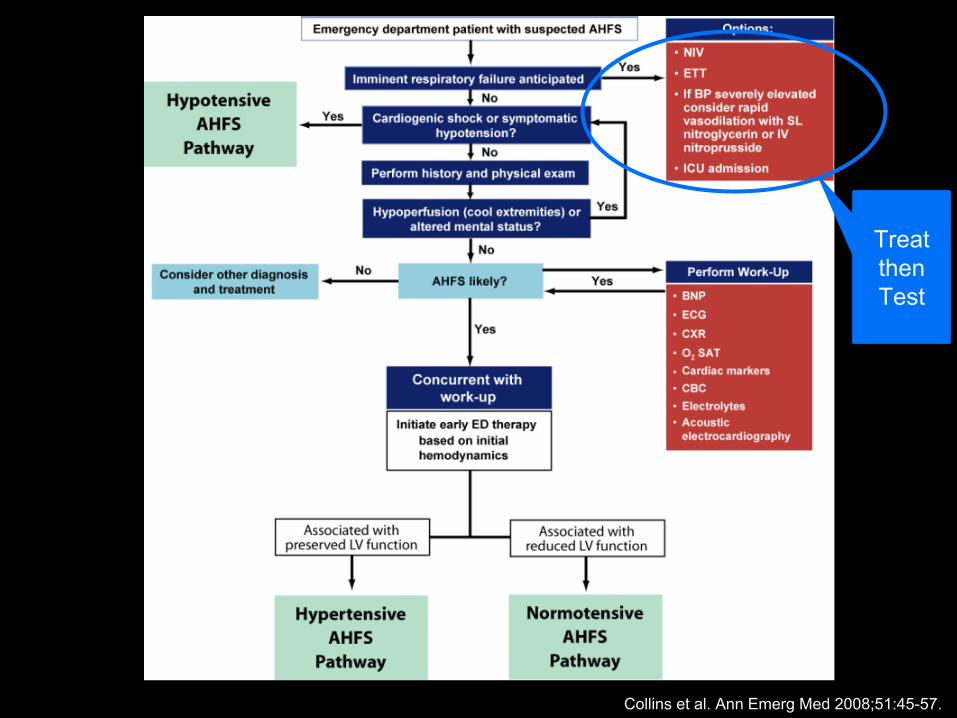
Treat then Test
Collins et al. Ann Emerg Med 2008;51:45-57.
Q: All of the following are true about Non-invasive ventilation except:
• a) It improves acidosis• b) It improves work of breathing• c) It decreases overall mortality • d) It is relatively easy to apply
Non-invasive Ventilation - A Therapy
• Consider if acute respiratory distress– CPAP: continuous positive airway pressure 1,2
• Reduction in need for ETI by 26 %• Trend towards ↑ survival
– BiPAP: bilevel positive airway pressure 3,4,5
• ↓ time to symptom resolution (30 vs. 105 min)• ↓ intubation rate (~ 23 %)
1 Berstein et al. NEJM 1991;325.2 Pang et al. Chest 1998;114.3 Masip et al. Lancet 2000;3564 Levitt MA. J Emerg Med 2001;21.5 Nava et al. Am J Resp Crit Care Med 2003;168
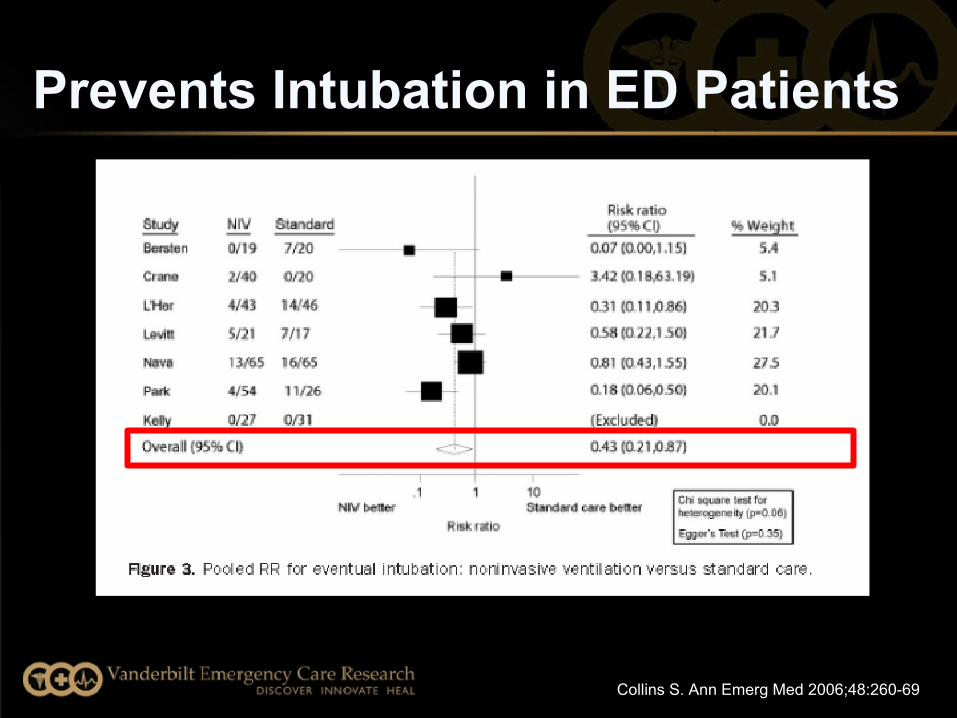
Collins S. Ann Emerg Med 2006;48:260-69
Prevents Intubation in ED Patients
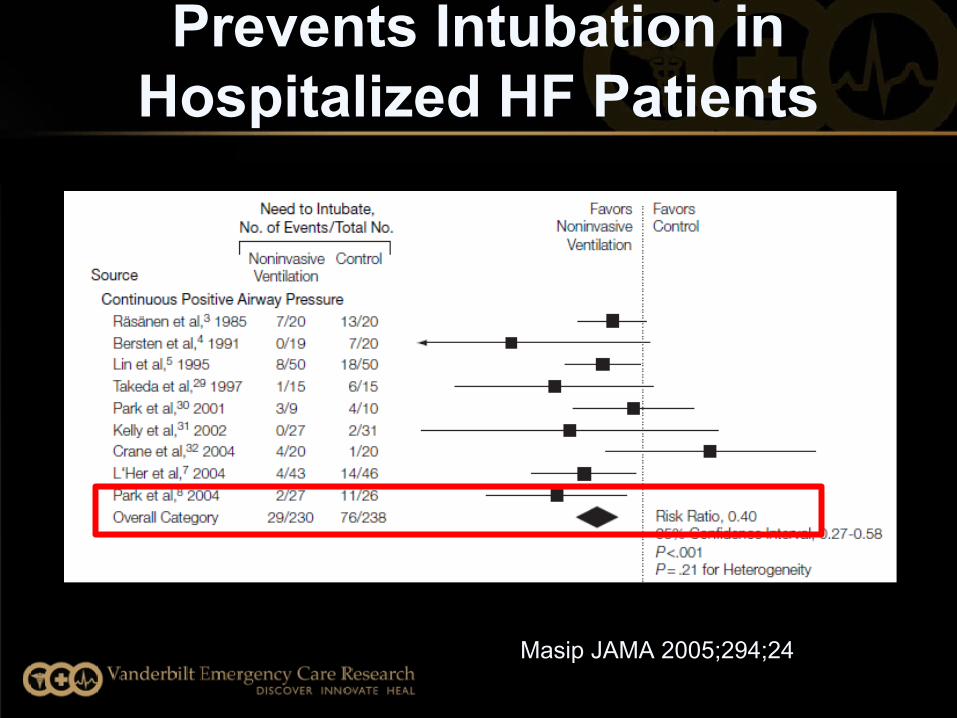
Prevents Intubation in Hospitalized HF Patients
Masip JAMA 2005;294;24
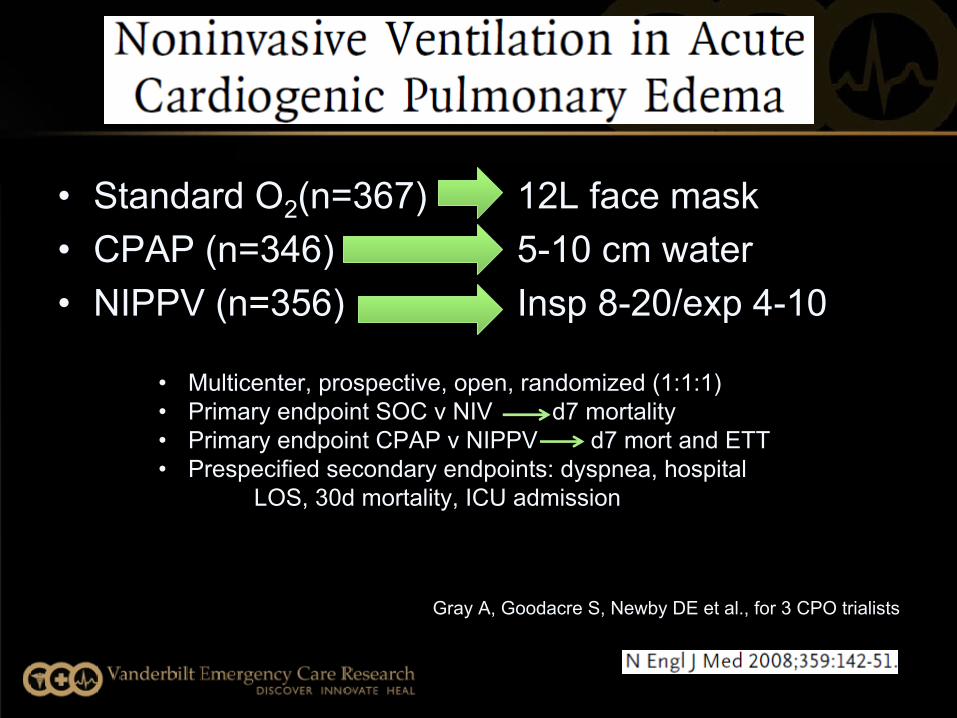
12L face mask 5-10 cm water Insp 8-20/exp 4-10
• Standard O2(n=367)• CPAP (n=346)• NIPPV (n=356)
Gray A, Goodacre S, Newby DE et al., for 3 CPO trialists
• Multicenter, prospective, open, randomized (1:1:1)• Primary endpoint SOC v NIV d7 mortality• Primary endpoint CPAP v NIPPV d7 mort and ETT• Prespecified secondary endpoints: dyspnea, hospital
LOS, 30d mortality, ICU admission
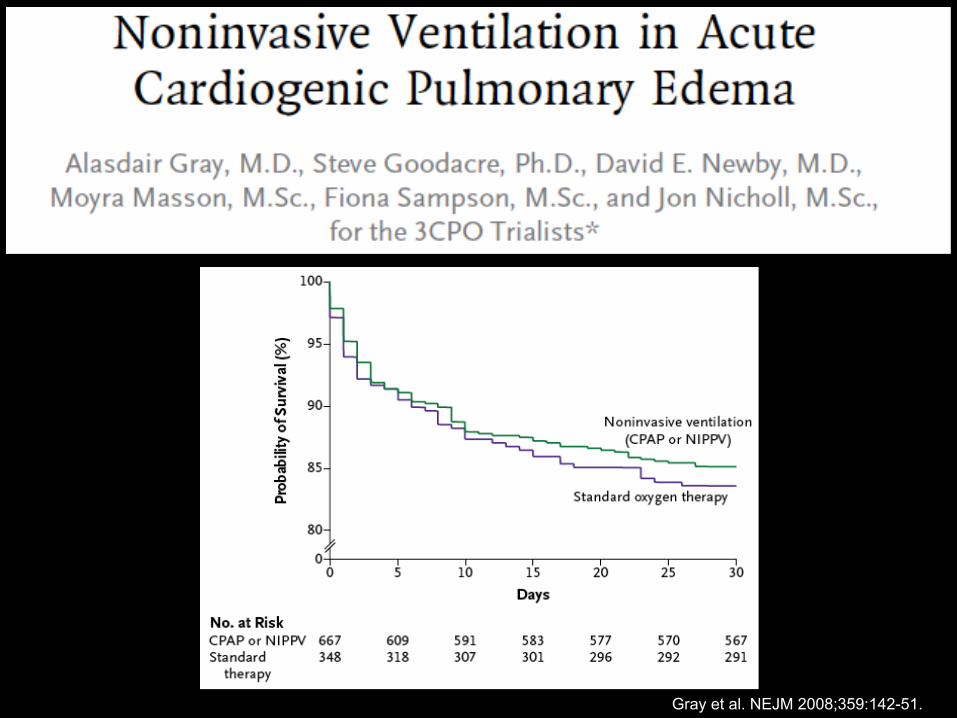
Gray et al. NEJM 2008;359:142-51.
Gray et al. NEJM 2008;359:142-51.
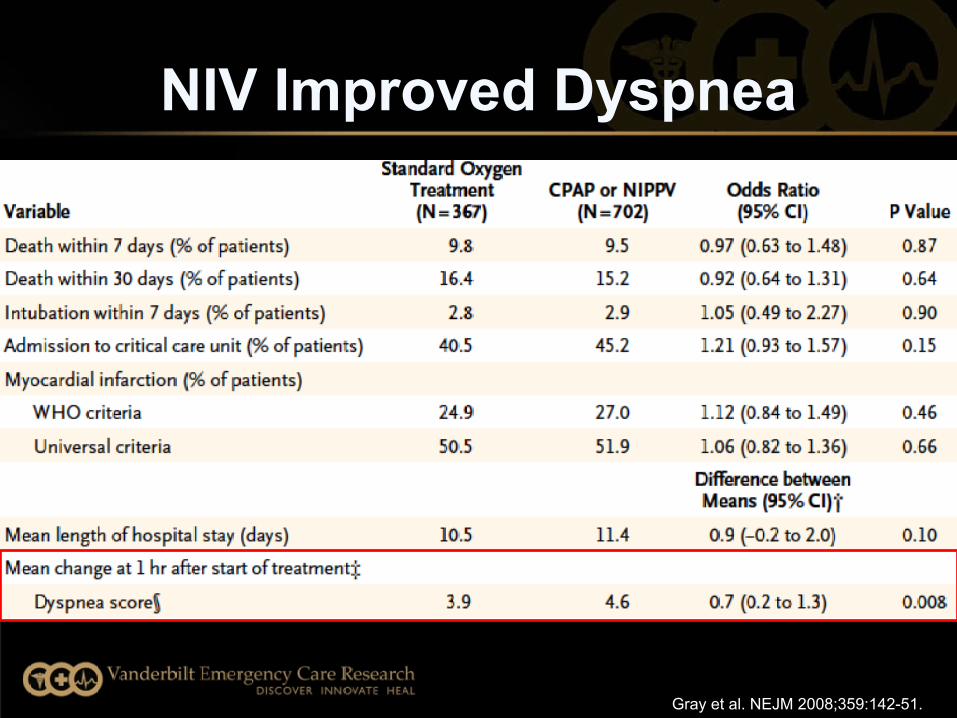
NIV Improved Dyspnea
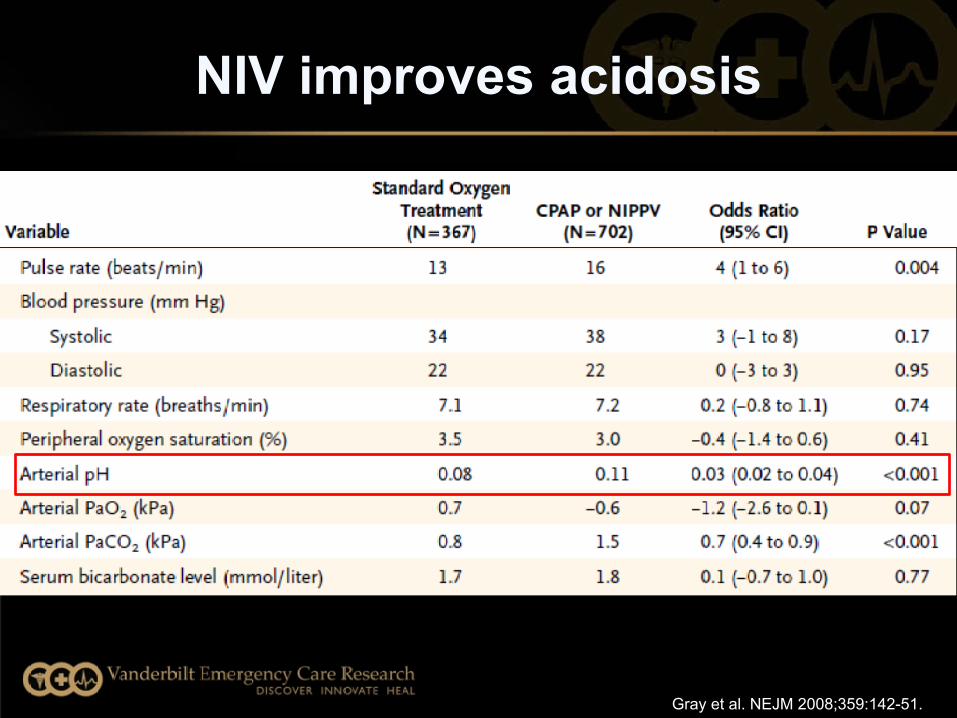
NIV improves acidosis
Gray et al. NEJM 2008;359:142-51.
Gray A, Goodacre S, Newby DE et al., for 3 CPO trialists
• No difference in tracheal intubation (overall rate 2.8%)
• No increase in MI in NIV
• No mortality benefit• Earlier improvement
of dyspnea
Take home points:
-May not save lives-Improves symptoms and resp
distress-Provides time for other therapies
to be started
• Q: T/F: High-dose IV Nitrates have been used safely in the prehospital and ED environment for AHF
• A) True• B) False
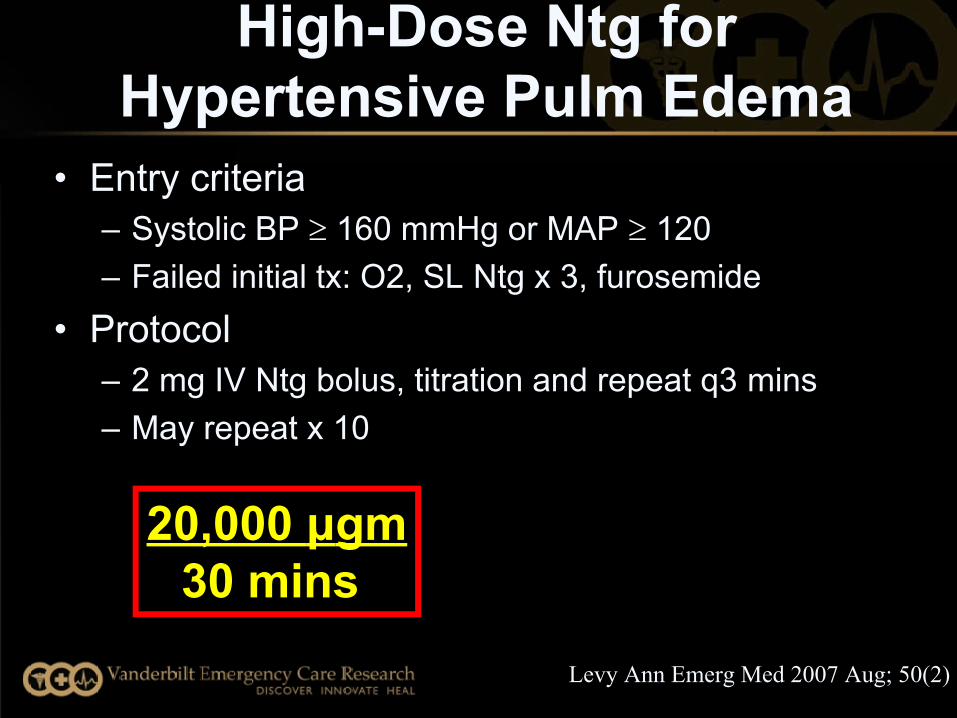
High-Dose Ntg for Hypertensive Pulm Edema
• Entry criteria– Systolic BP 160 mmHg or MAP 120– Failed initial tx: O2, SL Ntg x 3, furosemide
• Protocol– 2 mg IV Ntg bolus, titration and repeat q3 mins– May repeat x 10
Levy Ann Emerg Med 2007 Aug; 50(2)
20,000 μgm30 mins
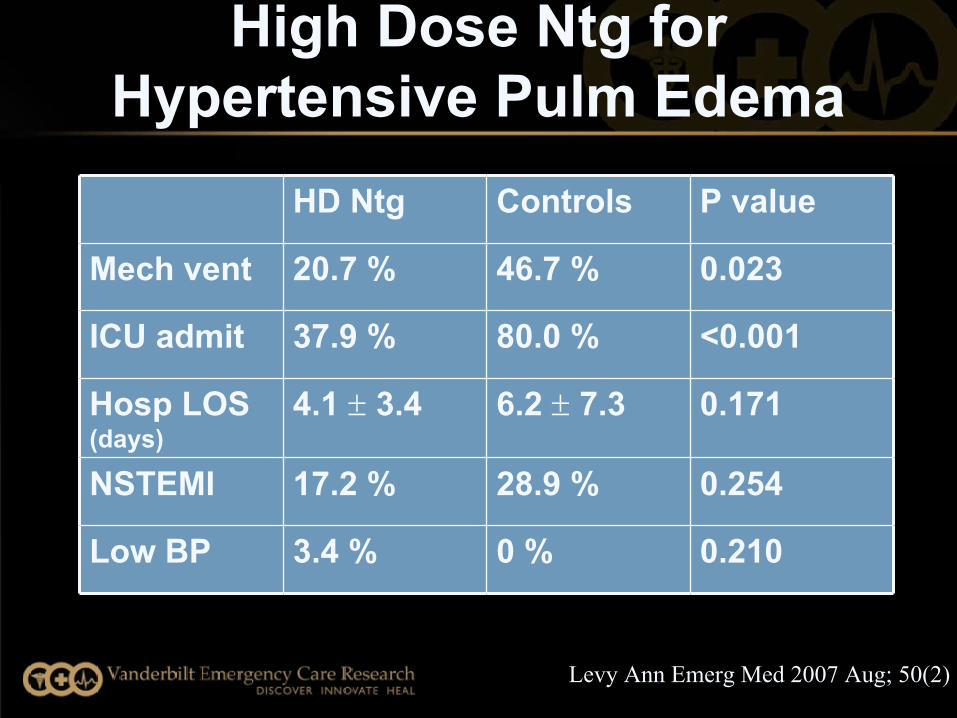
HD Ntg Controls P value
Mech vent 20.7 % 46.7 % 0.023
ICU admit 37.9 % 80.0 % <0.001
Hosp LOS (days)
4.1 3.4 6.2 7.3 0.171
NSTEMI 17.2 % 28.9 % 0.254
Low BP 3.4 % 0 % 0.210
Levy Ann Emerg Med 2007 Aug; 50(2)
High Dose Ntg for Hypertensive Pulm Edema
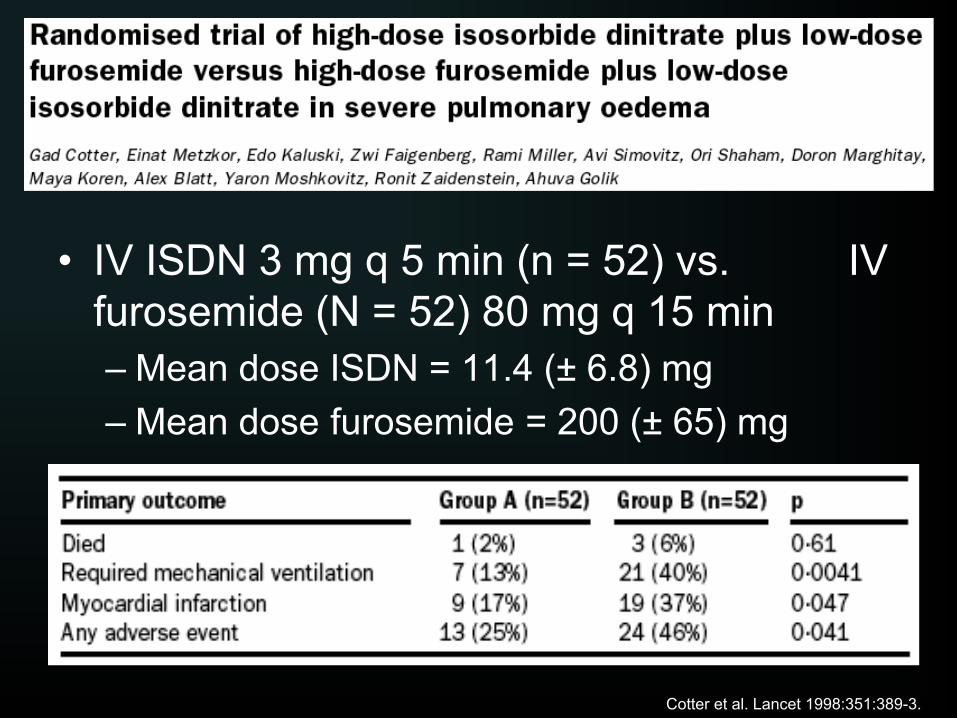
• IV ISDN 3 mg q 5 min (n = 52) vs. IV furosemide (N = 52) 80 mg q 15 min– Mean dose ISDN = 11.4 (± 6.8) mg– Mean dose furosemide = 200 (± 65) mg
Cotter et al. Lancet 1998:351:389-3.
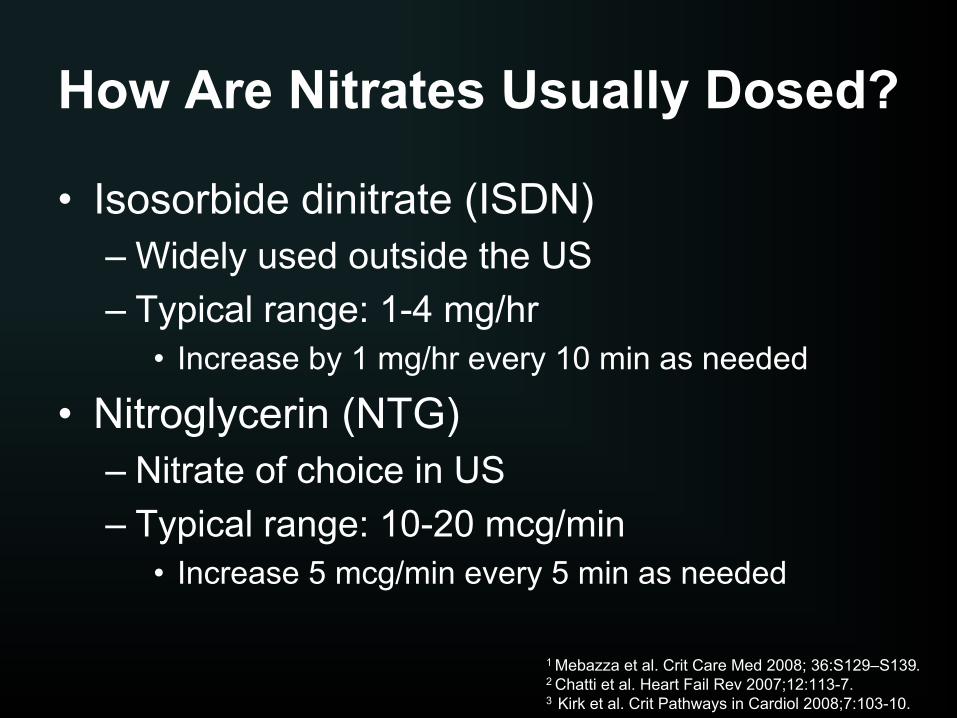
How Are Nitrates Usually Dosed?
• Isosorbide dinitrate (ISDN)– Widely used outside the US– Typical range: 1-4 mg/hr
• Increase by 1 mg/hr every 10 min as needed
• Nitroglycerin (NTG)– Nitrate of choice in US– Typical range: 10-20 mcg/min
• Increase 5 mcg/min every 5 min as needed
1 Mebazza et al. Crit Care Med 2008; 36:S129–S139.2 Chatti et al. Heart Fail Rev 2007;12:113-7.3 Kirk et al. Crit Pathways in Cardiol 2008;7:103-10.
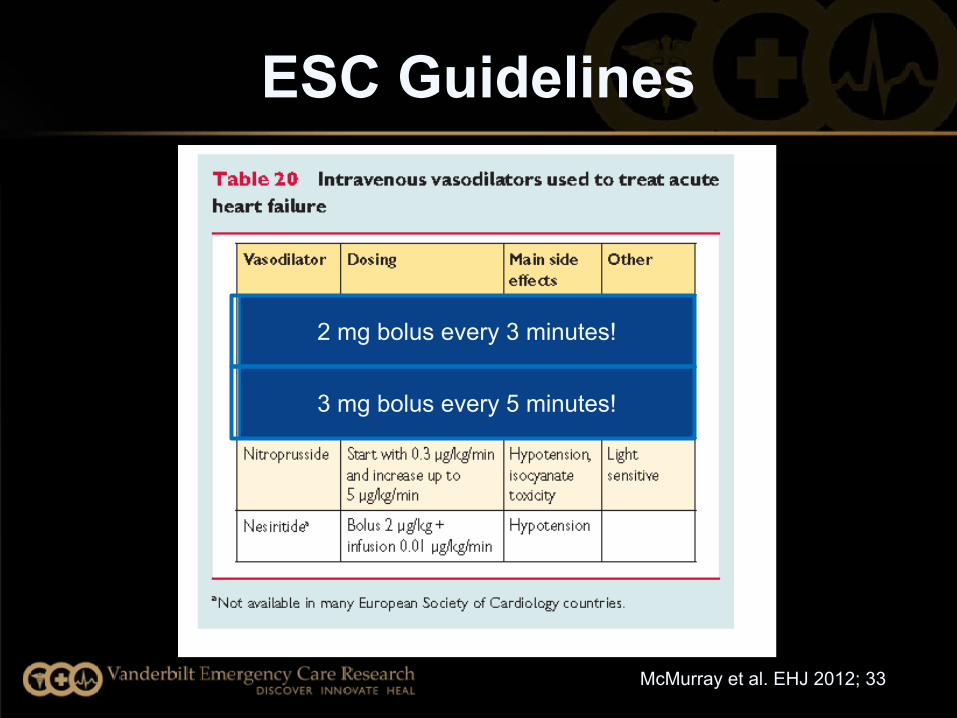
ESC Guidelines
McMurray et al. EHJ 2012; 33
2 mg bolus every 3 minutes!
3 mg bolus every 5 minutes!
PRONTO- IV Calcium Channel Blocker
• Open label, randomized 1:1 (CLV vs. SOC)• Acute Heart Failure (AHF) with SBP ≥ 160 mmHg• Primary objective:
– To evaluate the safety and efficacy of clevidipine vs. SOC IV anti-HTNs in ED AHF with hypertension
Peacock Am Heart J 2014 Apr; 167(4):529-36
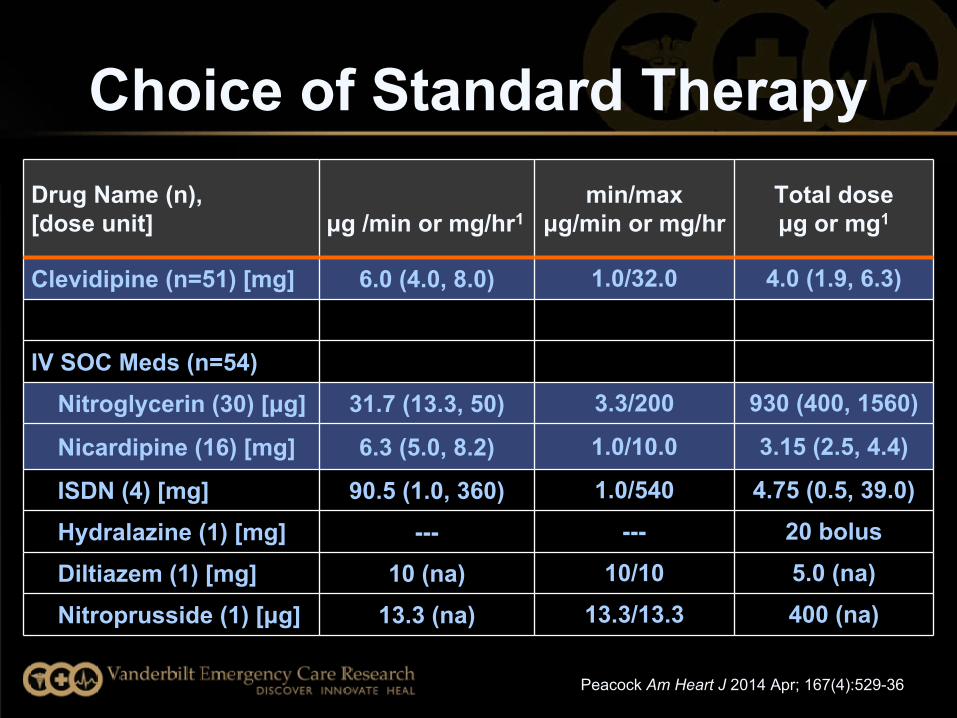
Choice of Standard TherapyDrug Name (n), [dose unit] μg /min or mg/hr1
min/maxμg/min or mg/hr
Total dose μg or mg1
Clevidipine (n=51) [mg] 6.0 (4.0, 8.0) 1.0/32.0 4.0 (1.9, 6.3)
IV SOC Meds (n=54) Nitroglycerin (30) [μg] 31.7 (13.3, 50) 3.3/200 930 (400, 1560)
Nicardipine (16) [mg] 6.3 (5.0, 8.2) 1.0/10.0 3.15 (2.5, 4.4)
ISDN (4) [mg] 90.5 (1.0, 360) 1.0/540 4.75 (0.5, 39.0)
Hydralazine (1) [mg] --- --- 20 bolus
Diltiazem (1) [mg] 10 (na) 10/10 5.0 (na)
Nitroprusside (1) [μg] 13.3 (na) 13.3/13.3 400 (na)
Peacock Am Heart J 2014 Apr; 167(4):529-36
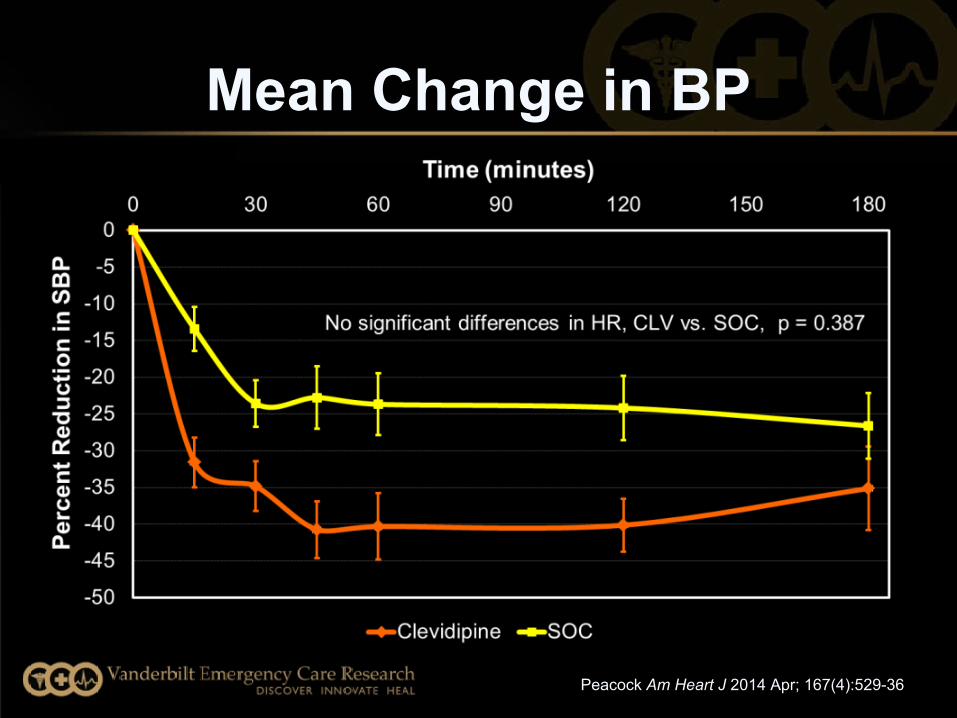
Mean Change in BP
Peacock Am Heart J 2014 Apr; 167(4):529-36
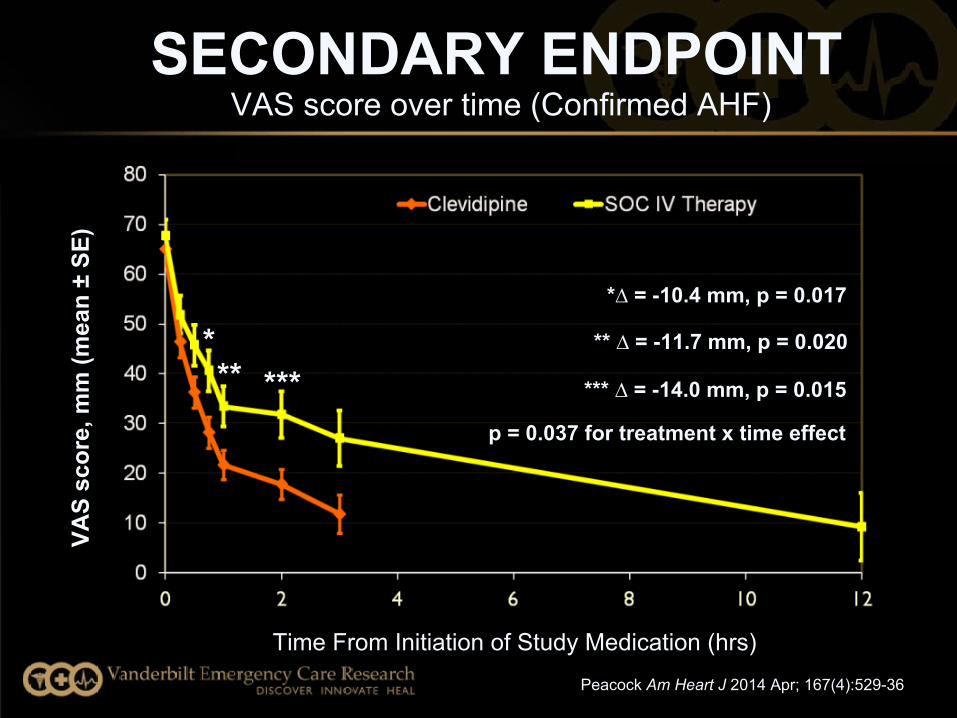
SECONDARY ENDPOINTVAS score over time (Confirmed AHF)
VAS
scor
e, m
m (m
ean
± SE
)
Time From Initiation of Study Medication (hrs)
*** ***
*∆ = -10.4 mm, p = 0.017
** ∆ = -11.7 mm, p = 0.020
*** ∆ = -14.0 mm, p = 0.015
p = 0.037 for treatment x time effect
Peacock Am Heart J 2014 Apr; 167(4):529-36
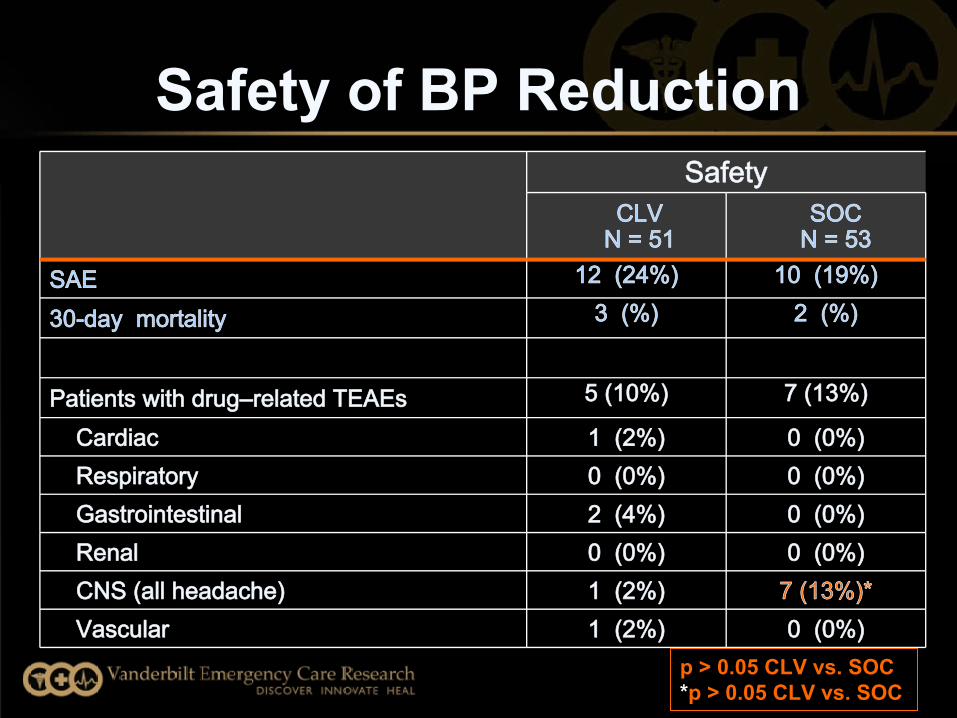
Safety of BP Reduction Safety
CLV N = 51
SOC N = 53
SAE 12 (24%) 10 (19%)
30-day mortality 3 (%) 2 (%)
Patients with drug–related TEAEs 5 (10%) 7 (13%)
Cardiac 1 (2%) 0 (0%) Respiratory 0 (0%) 0 (0%) Gastrointestinal 2 (4%) 0 (0%) Renal 0 (0%) 0 (0%) CNS (all headache) 1 (2%) 7 (13%)* Vascular 1 (2%) 0 (0%)
p > 0.05 CLV vs. SOC*p > 0.05 CLV vs. SOC
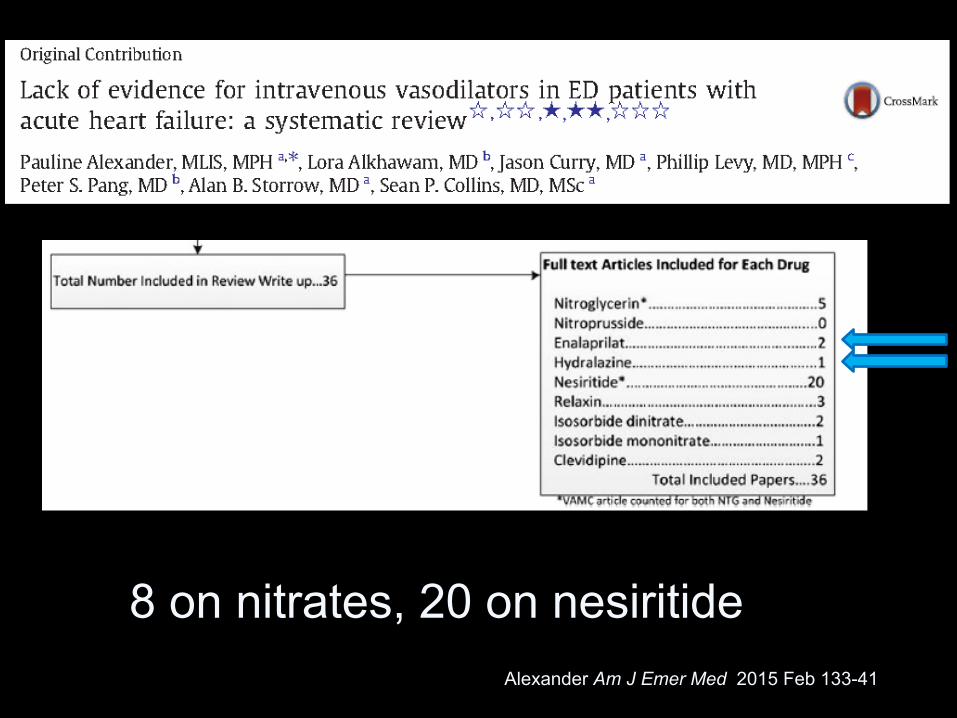
Alexander Am J Emer Med 2015 Feb 133-41
8 on nitrates, 20 on nesiritide
• Hydralazine- 1 study with limitations1
• Enalaprilat - 2 studies- 34 total AHF patients1
• “Evidence Free Zone”
Alexander Am J Emer Med 2015 Feb 133-41
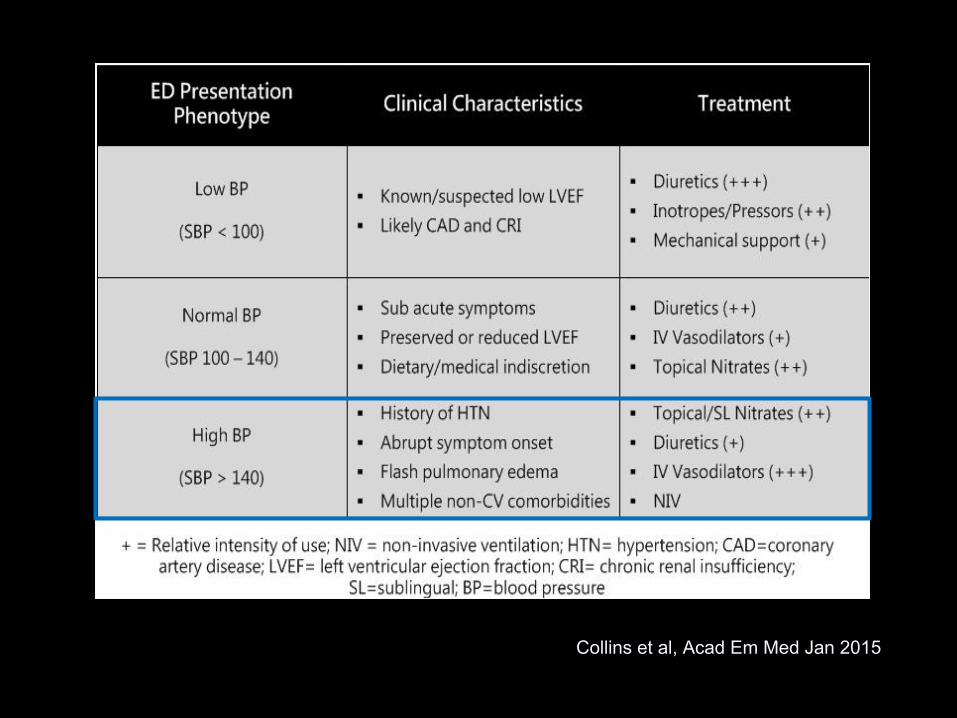
Collins et al, Acad Em Med Jan 2015
Summary: Hypertensive Pulm Edema
• AHF + Significant BP elevation• Early and aggressive treatment improves
symptoms- outcomes??• NIV, Nitrates/vasodilators, Diuretics
• Rapid improvement if hemodynamics addressed early
Thank You