Embed Size (px)
Citation preview

PAEDIATRICSKIN DISORDERS
Richie Chacko
Paediatric & Nonatal Nursing

LISHMANIASIS
• The leishmaniasis are a group of vector-borne protozoan diseases caused bypathogenic Leishmania species which, ifsymptomatic, result in clinicalmanifestations that range from localisedcutaneous ulcers to disseminated lethalinfection. video

Leishmania Parasites and Diseases
SPECIES DISEASE
Leishmania tropica
Leishmania major
Leishmania aethiopica
Leishmania mexicana
Cutaneous leishmaniasis
Leishmania braziliensis Mucocutaneous leishmaniasis
Leishmania donovani
Leishmania infantum
Leishmania chagasi
Visceral leishmaniasis

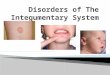
LIFE CYCLE
• The organism is transmitted by the bite of severalspecies of blood-feeding sand flies (Phlebotomus)which carries the promastigote in the anterior gut andpharynx. It gains access to mononuclear phagocyteswhere it transform into amastogotes and divides untilthe infected cell ruptures. The released organismsinfect other cells. The sandfly acquires the organismsduring the blood meal, the amastigotes transform intoflagellate promastigotes and multiply in the gut until theanterior gut and pharynx are packed. Dogs and rodentsare common reservoirs.



SAND FLY

AMASTIGOTES PROMASTIGOTES

ETIOLOGY
• Leishmaniasis is due to protozoan parasites from the Leishmania species. leishmaniasis transmits from bite of an infected called sand fly.

RISK FACTORS
• Geography: India, Bangladesh, South Sudan,Sudan, Brazil, Ethiopia; tropical or subtropicalareas of these countries and regions.
• Socioeconomic Conditions: According tothe World Health Organization (WHO), poverty isa determining factor for the disease.
• Other Infections: children who have weakenedimmune systems are also at increased risk of thiscondition.

CLASSIFICATION
Categorization by clinical disease:• leishmaniasis is divided into 3 primary clinical
forms:1. Cutaneous leishmaniasis: (localized, diffuse
(disseminated), which causes skin sores2. Visceral leishmaniasis: which affects several
internal organs (usually spleen, liver, and bonemarrow).
3. Mucocutaneous leishmaniasis: lead to partial orcomplete destruction of the mucousmembranes found in your nose, throat, andmouth.

Categorization by geographic occurrence:
1. Old World leishmaniasis (causedby Leishmania species found in Africa(ethiopia), Asia, the Middle East, theMediterranean,), which produces cutaneousor visceral disease.
2. New World leishmaniasis (caused byLeishmania species found in Central andSouth America), which produces cutaneous,mucocutaneous, and visceral disease

DISTRIBUTION OF MUCOCUTANEOUS LEISHMANIASIS
• Old World spread ofmucocutaneous leishmaniasis isvia L aethiopica in Ethiopia,Kenya, and Namibia.

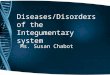
SIGNS AND SYMPTOMS• Cutaneous leishmaniasis :1. Localized cutaneous leishmaniasis: Crusted papules or
ulcers on exposed skin.2. Diffuse (disseminated) cutaneous leishmaniasis:
Multiple, widespread nontender, nonulceratingcutaneous papules and nodules.
3. Leishmaniasis recidivans: Presents as a recurrence oflesions at the site of apparently healed disease yearsafter the original infection.
4. Post–kala-azar dermal leishmaniasis: Developsmonths to years after the patient's recovery fromleishmaniasis, with cutaneous lesions ranging fromhypopigmented macules to erythematous papulesand from nodules to plaques; the lesions may benumerous and persist for decades

• Visceral leishmaniasis
1. Potentially lethal widespread systemicdisease characterized by darkening of theskin as well as fever, weight loss,hepatosplenomegaly, pancytopenia.
2. Nonspecific abdominal tenderness; fever,rigors, fatigue, malaise, nonproductivecough, intermittent diarrhea, headache,arthralgias, myalgias, nausea, adenopathy,transient hepatosplenomegaly

• Mucocutaneous leishmaniasis
1. Excessive tissue obstructing the nares, septalgranulation, and perforation; nose cartilage may be involved, giving rise to external changes known as parrot's beak or camel's nose .
2. Possible presence of granulation, erosion, and ulceration of the palate, uvula, lips, pharynx, and larynx .
3. Gingivitis, periodontitis
4. Localized lymphadenopathy
5. Optical and genital mucosal involvement in severe cases


DIAGNOSISLaboratory diagnosis include the following:
• Isolation, visualization, and culturing of theparasite from infected tissue
• Serologic detection of specific antibodies
• Polymerase chain reaction (PCR) assay forsensitive, rapid diagnosis of Leishmaniaspecies.
• CBC count, coagulation studies, liver function tests, peripheral blood smear
• Measurements of lipase, amylase, gamma globulin, and albumin

COMPLICATIONS
• bleeding
• other infections due to a weakened immune system, which can be life-threatening
• disfigurement

MEDICAL MANAGEMENT
• Liposomal amphotericin B and paromomycincan treat mucocutaneous leishmaniasis.
• Mucocutaneous leishmaniasis diseaseresponds to a 20-day course of sodiumantimony gluconate; amphotericin B may beused to treat advanced or resistant cases.Pentavalent antimony for a course of 4 weekshas also been recommended.

PREVENTION• Wear clothing that covers as much skin as
possible. Long pants, long-sleeved shirtstucked into pants, and high socks arerecommended.
• Use insect repellent on any exposed skin andon the ends of your pants and sleeves.
• Spray indoor sleeping areas with insecticide.
• Sleep on the higher floors of a building. The insects are poor fliers.
• Avoid the outdoors between dusk and dawn.
• Use a bed net tucked into your mattress.

ONYCHOMYCOSIS
• Onychomycosis is a fungal infection ofthe toenails or fingernails that mayinvolve any component of the nail unit,including the matrix, bed, orplate. Onychomycosis can cause pain,discomfort, and disfigurement and mayproduce serious physical andoccupational limitations, as well asreducing quality of life.

ETIOLOGY
• The primary causative dermophytesare Trichophyton rubrum, T. mentagrophytes,and Epidermophyton floccosum.
• Trichophyton rubrum being by far the mostlikely common.

TYPES OF ONYCHOMYCOSIS
• Distal lateral subungualonychomycosis (DLSO)
• White superficial onychomycosis(WSO)
• Proximal subungual onychomycosis(PSO)
• Candidal onychomycosis.

Distal lateral subungualonychomycosis (DLSO)
• Most common
• Fungi invade thehyponychium andgrow in thesubstance of nailplate, causing it tocrumble
• Hyperkeratotic debriscauses nail toseparate from thebed

White superficial onychomycosis(WSO)
• Commonly Trichophytonmentagrophytes
• Nail - white• soft• powdery• not thickened• not separated from thenail bed.

Proximal subungual onychomycosis(PSO)
• CommonlyTrichophyton Rubrum
• Invade the substanceof nail plate, not thesurface
• Hyperkeratotic debriscauses the nail plateto separate from thenail bed

Candidal onychomycosis.
• Almost exclusively inchronicmucocutaneouscandidiasis
• Generally infect allfingernails
• Linear yellow orbrown streaks growand advanceproximally

CLINICAL MANIFESTATION
• Onychomycosis is usually asymptomatic
• interfere with standing, walking, andexercising.
• Paresthesia, pain, discomfort, and loss ofdexterity.
• The nail shows usually yellow-white in color.
• Nail becomes roughened and crumbles easily.


DIAGNOSIS
• Culture – gold standard
• Histological examination by periodic acid-Schiff (PAS) staining – equal to culture

Obtaining specimen
Clip the nail for culture
Subungal debris for culture

–Antibiotics suppress bacterialcontaminants
–Medium turn from yellow to red in 7-14 days – alkaline released bydermatophytes turn phenol (pHindicator) red
• ID the organism
• PAS staining: stain fungal elementspinkish-red

COMPLICATIONS
• Skin injury adjacent to the nail mayallow organisms to colonize, therebyincreasing the risk of infectiouscomplications. Reports ofcomplications with diabetes includecellulitis, osteomyelitis, sepsis, andtissue necrosis.

MEDICAL MANAGEMENT
• Fluconazole (Diflucan): 150-mg dose each
week for 9 months
• Itraconazole (Sporanox): 200 mg/day for
12 weeks for toenails, 6 weeks for
fingernails.“Pulse dosing”: 400 mg/day for
first week of each.
• Terbinafine: 250 mg/day (12 weeks for
toenails, 6 weeks for fingernails)

MECHANICAL REMOVAL
• Surgery: Remove the entire nail or cut theaffected portion, followed by curetting tonormal nail in 7-10 days

DERMATOPHYTOSIS
• Dermatophyte infections are commonworldwide, and dermatophytes are theprevailing causes of fungal infection of theskin, hair, and nails. These infections lead to avariety of clinical manifestations, such as tineapedis, tinea corporis, tinea cruris.

ETIOLOGY
• Dermatophytes are fungi in the generaTrichophyton, Microsporum, andEpidermophyton. Dermatophytesmetabolize and subsist upon keratin in theskin, hair, and nails.

RISK FACTORS
• Age (most common in pre-pubescent children).
• Overcrowding (households or schools).
• Hairdressing salons.
• Use of shared combs.
• Ethnicity.

MAJOR CLINICAL SUBTYPES
• Tinea corporis – Infection of bodysurfaces other than the feet, groin, face,scalp, hair, or beard hair.
• Tinea pedis – Infection of the foot.
• Tinea cruris – Infection of the groin.

TINEA PEDIS
• Tinea pedis (also known as athlete's foot)is the most common dermatophyteinfection. Tinea pedis may manifest as aninterdigital, hyperkeratotic, orvesiculobullous eruption, and rarely as anulcerative skin disorder.

ETIOLOGY
• Tinea pedis usually occurs in adults andadolescents (particularly young men) andis rare prior to puberty Common causesare T. rubrum, T. interdigitale (formerly T.mentagrophytes), and E. floccosum.

CLINICAL FEATURES• Interdigital tinea pedis – Interdigital tinea pedis
manifests as pruritic, erythematous erosions or scalesbetween the toes, especially in the third and fourthdigital interspaces. Associated interdigital fissures maycause pain.
• Hyperkeratotic tinea pedis – Hyperkeratotic tineapedis is characterized by a diffuse hyperkeratoticeruption involving the soles and medial and lateralsurfaces of the feet, There is a variable degree ofunderlying erythema.
• Vesiculobullous (inflammatory) tinea pedis –Vesiculobullous tinea pedis is characterized by apruritic, sometimes painful, vesicular or bullouseruption with underlying erythema . The medial foot isoften affected.


DIAGNOSIS
• The diagnosis is confirmed with the detection of fungi in skin scrapings from an affected area with a potassium hydroxide (KOH) preparation
• A fungal culture is an alternative diagnostic procedure.

TREATMENT• Topical antifungal therapy include azoles,
allylamines, butenafine, ciclopirox, tolnaftate,and amorolfine applied once or twice daily andcontinued for four weeks.
• Hyperkeratotic tinea pedis can benefit fromcombining antifungal treatment with a topicalkeratolytic, such as salicylic acid. Burow's (1%aluminum acetate or 5% aluminum subacetate)wet dressings.
• Placing gauze or cotton between toes may behelpful as an adjunctive measure for patientswith vesiculation.
• Treatment of shoes with antifungal powder, andavoidance of occlusive footwear.

TINEA CORPORIS
• Tinea corporis is a cutaneousdermatophyte infection occurring in sitesother than the feet, groin, face, or hand.

ETIOLOGY
• T. rubrum is the most common causeof tinea corporis. Other notablecauses include T. Interdigitale & T.Tonsurans.

CLINICAL FEATURES
• Tinea corporis often begins as a pruritic, circular or oval, erythematous, scaling patch or plaque that spreads centrifugally. The result is an annular (ringshaped)plaque from which the disease derives its common name (ringworm).
• Pustules occasionally appear, intensely inflammatory.
• Extensive tinea corporis should raise concern for an underlying immune disorder; HIV & Diabetes


DIAGNOSIS
• The diagnosis is confirmed with the detection of fungi in skin scrapings from an affected area with a potassium hydroxide (KOH) preparation
• A fungal culture is an alternative diagnostic procedure.

TREATMENT• Topical antifungal drugs, such as azoles,
allylamines, butenafine, ciclopirox, andtolnaftate once or twice per day for one tothree weeks.
• Topical corticosteroids for inflammation.

TINEA CRURIS
• Tinea cruris (also known as jock itch)is a dermatophyte infection involvingthe crural fold.

ETIOLOGY
• The most common cause is T. rubrum.Other frequent causes include E.floccosum and T. interdigitale
• Common in men than women.
• Predisposing factors include copioussweating, obesity, diabetes, andimmunodeficiency.

CLINICAL FEATURES
• The infection spreads centrifugally, withpartial central clearing and a slightlyelevated, erythematous, sharplydemarcated border that may have tinyvesicles on the proximal medial thigh.
• Infection may spread to the perineumand perianal areas, into the gluteal cleft,or onto the buttocks. In males, thescrotum is typically spared.


DIAGNOSIS
• The diagnosis is confirmed with the detection of fungi in skin scrapings from an affected area with a potassium hydroxide (KOH) preparation
• A fungal culture is an alternative diagnostic procedure.

TREATMENT
• Topical therapy with antifungal agents such as azoles, allylamines, butenafine, ciclopirox, and tolnaftate is effective
• daily use of desiccant powders in the inguinal area and avoidance of tightfitting clothing and noncotton underwear

TINEA CAPITIS
• Tinea capitis, or scalp ringworm, is anexogenous infection caused by thedermatophytes Microsporum .and Trichophyton . These originate from anumber of possible sources children or adults(anthropophilic), animals (zoophilic) or soil(geophilic).

CLINICAL FEATURES• Infection in the hair and scalp skin is
associated with symptoms and signs ofinflammation and hair loss (mainly inprepubertal children). The main signs arescaling and hair loss but acuteinflammation with erythema and pustuleformation can occur..
• tinea capitis can affect nails and skin inother parts of the body (only very rarelythe feet or groins).



DIAGNOSIS
• Scalp scrapings - including hairs and hair fragments.
• Microscopic examination of the infected hairs may provide immediate confirmation of the diagnosis of ringworm .
• Culture may take several weeks. Culture provides precise identification of the species
• Ultraviolet light (Wood's light) Fluorescence is produced by the fungus.

MANAGEMENT
• Topical treatment (usually selenium sulfide orketoconazole shampoo but, occasionally, alsotopical antifungals like terbinafine cream
• Children - griseofulvin (1 month-12 years 15-20 mg/kg, maximum 1 g) once daily or individed doses.
• Fluconazole2-5 mg/kg/day. Weekly treatmentwith 8 mg/kg may be as effective.

COMPLICATIONS
• Severe hair loss.
• Scarring alopecia.
• Psychological impact (ridicule, bullying,isolation, emotional disturbance, familydisruption).
• The main complication is secondary bacterial infection.
• Pain and difficulty with shoes.

PROGNOSIS
• Excellent with good compliance andsubsequent precautions to avoid repeatinfection.

PREVENTION
• Good skin hygiene.
• Good nail hygiene.
• Avoiding prolonged wetting or dampness of the skin and feet.
• Avoiding trainers, which can retain sweat and promote a warm, moist environment.
• Treatment of tinea pedis - helps prevent onychomycosis.[8]
• Wearing clean, loose-fitting underwear.