Embed Size (px)
Citation preview

INTRAOCULAR FOREIGN BODY
PRESENTER DR SANIL SAWANT
MODERATOR DR DEVENDRA VENKATRAMANI
Ocular trauma constitutes one of the important cause of visual loss and subsequent disability.
Penetrating injuries are divided into various subcategories based on specific types of injuries .
Intraocular foreign bodies may complicate penetrating injury
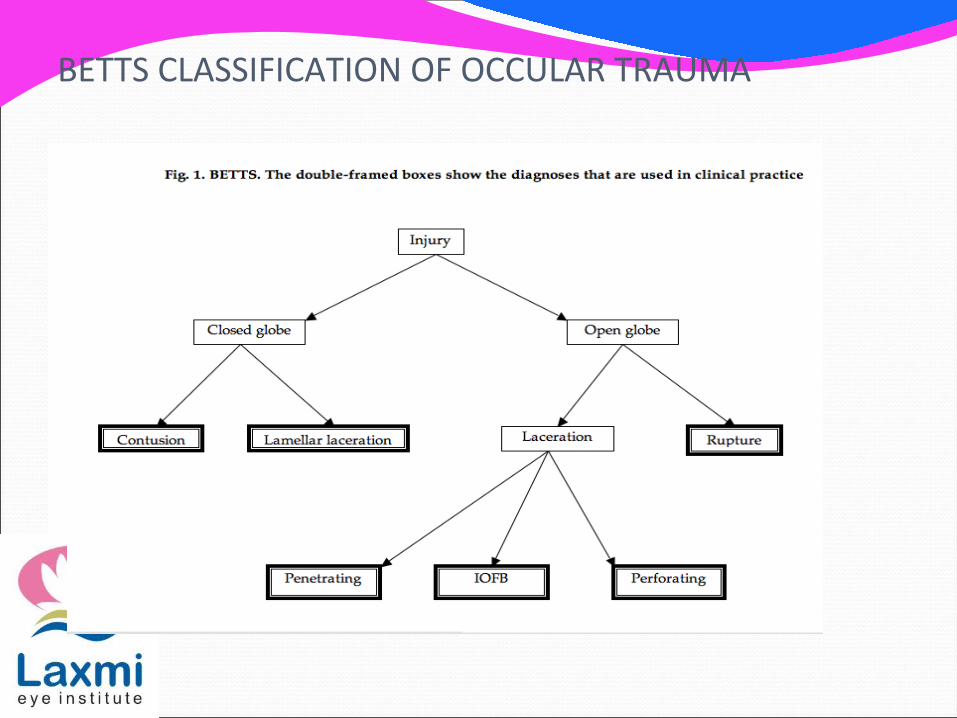
BETTS CLASSIFICATION OF OCCULAR TRAUMA
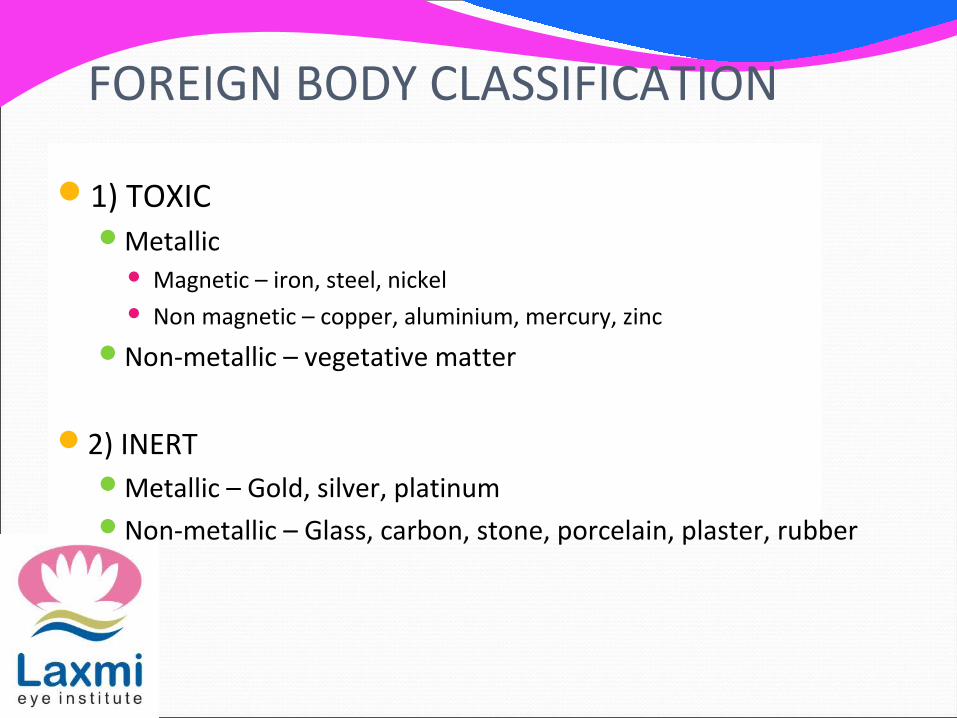
FOREIGN BODY CLASSIFICATION
1) TOXIC Metallic
Magnetic – iron, steel, nickel Non magnetic – copper, aluminium, mercury, zinc
Non-metallic – vegetative matter
2) INERT Metallic – Gold, silver, platinum Non-metallic – Glass, carbon, stone, porcelain, plaster, rubber
MODES OF DAMAGE
Mechanical effects Introduction of infection Reaction of foreign body Post-traumatic iridocyclitis Sympathetic ophthalmitis
MECHANICAL EFFECTS
Depends on the size, velocity and type of foreign body
Foreign bodies greater than 2 mm cause extensive damage
Lesions depends upon the route of entry and the site up to which foreign body has travelled
LOCATIONS OF IOFB 1)Anterior chamber –
Usually sinks in the bottom Tiny foreign body can be visualised only on gonioscopy
2) Iris –In the stroma
3) Posterior chamber – Behind the iris after entering through pupil or making a hole in
the iris
Lens –On anterior surface or inside the lens (either an opaque tract
may be seen in lens or may become cataractous)
Vitreous cavity
Retina , choroid and sclera
Orbital cavity
INTRODUCTION OF INFECTION
Metallic foreign are usually sterile due to heat generated by them
Wood and stones carry a great chance of infection
Usually ends in endophthalmitis and panophthalmitis
REACTION OF FOREIGN BODYInorganic foreign body
No reaction by inert substances which includes glass, porcelain, gold, silver and platinum
Local irritative reaction leading to encapsulation of foreign body occurs with lead and aluminium particles .
Suppurative reaction excited by pure copper, zinc, nickel and mercury particles .
Specific reactions by iron (siderosis) and copper alloys (chalcosis)
SIDEROSIS BULBI Degenerative changes produced by an iron foreign bodyUsually occurs 2 months to 2 years of the injury MECHANISM –
The iron particle undergo electrolytic dissociation by the current of rest and its ions are disseminated throughout the eye.
These ions combine with intracellular protein and produce degenerative changes
Epithelial structures of the eye are most affected
CLINICAL MANIFESTATIONS
Anterior epithelium and capsule of lens are involved first. Rusty deposits are arranged radially in a ring; later cataract develops
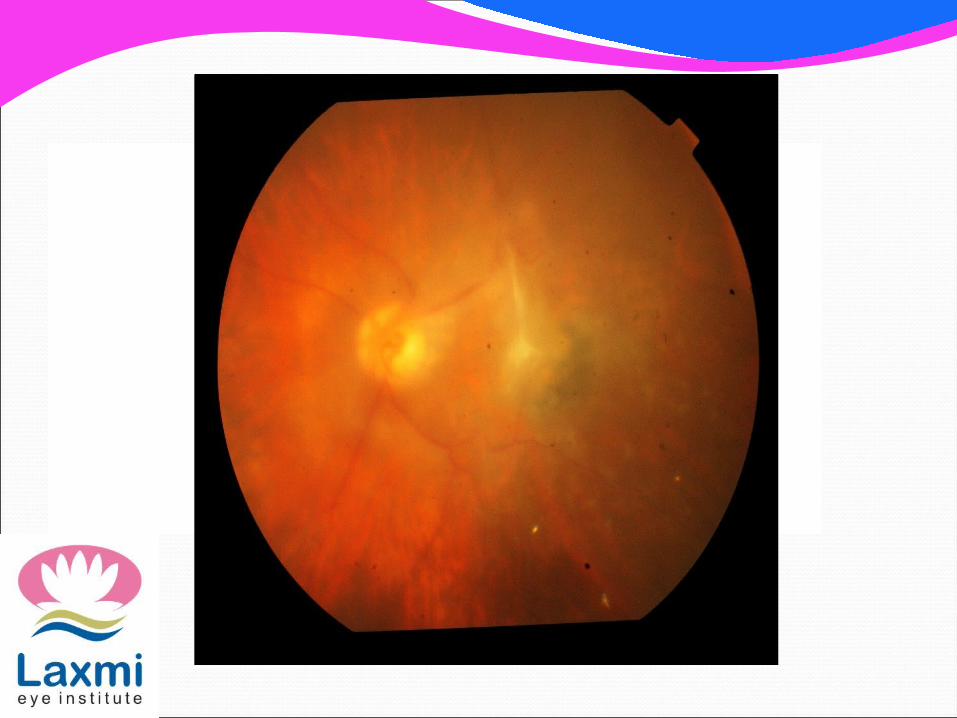
Iris first stained greenish and latter on reddish brown Retinal pigmentary changes can resemble retinitis pigmentosa ERG shows progressive attenuation of b wave over timeSecondary open angle type of glaucoma due to degenerative
changes in trabecular meshwork
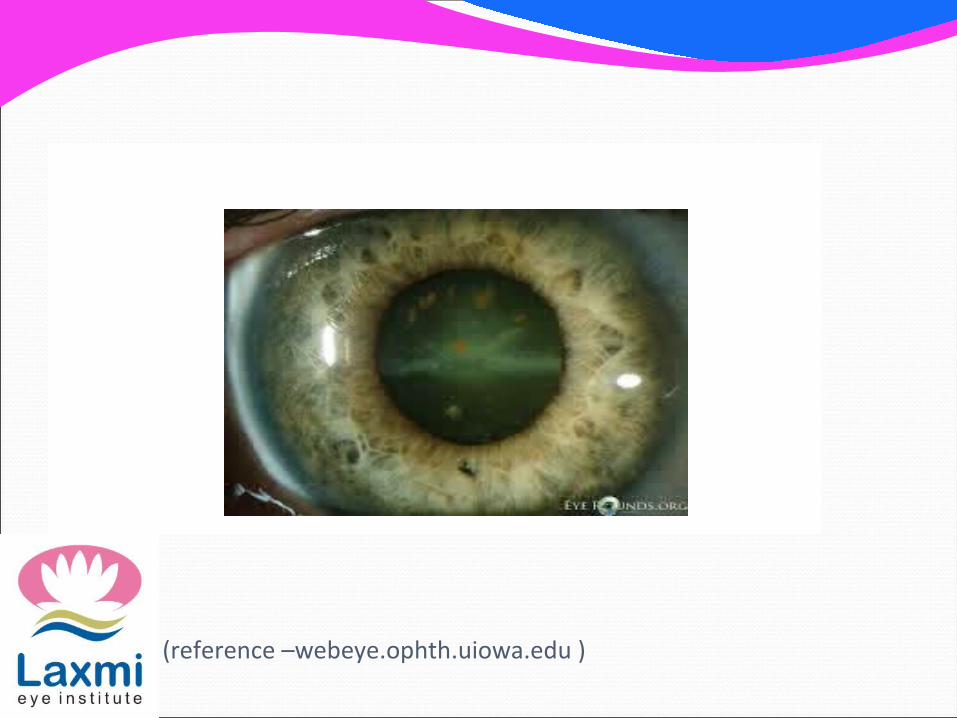
(reference –webeye.ophth.uiowa.edu )
CHALCOSIS
Specific changes produced by alloys of copper in the eye
IOFB with high copper content involves violent endophthalmitis often with progression to phthisis bulbi
Alloys with low copper content like brass and bronze results in chalcosis
CLINICAL MANIFESTATIONS Kayser-Fleischer ring is golden brown ring which occurs
due to deposition of copper under peripheral part of Descemet’s membrane of the cornea
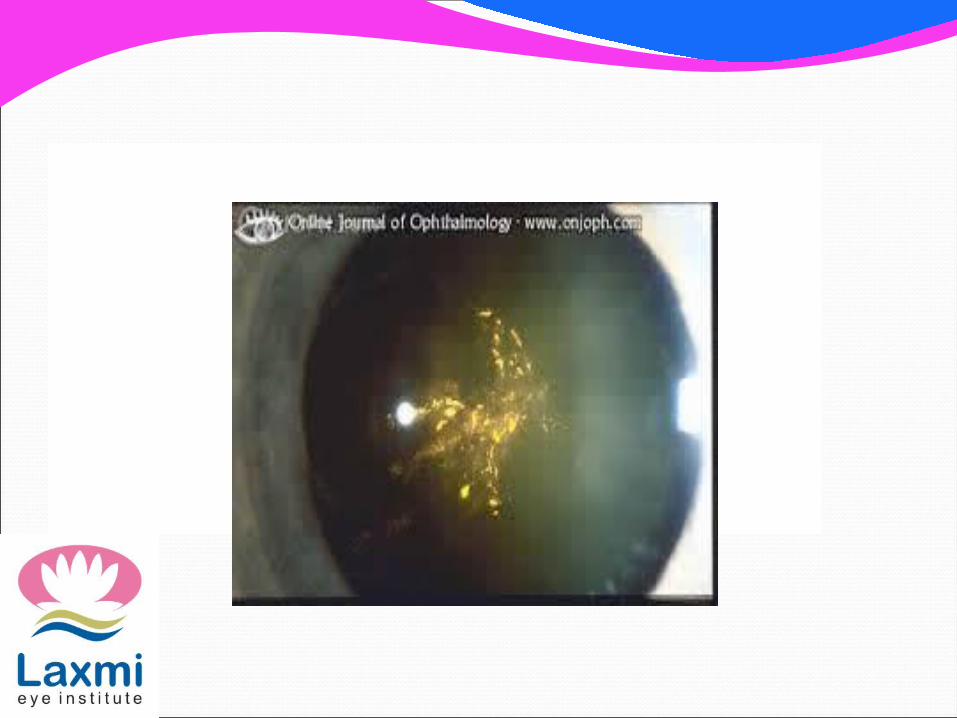
Sunflower cataract produced by deposition of the capsule under posterior capsule of the lens
Brilliant golden green in colourRetina – deposition of golden plaques at the posterior
pole which reflects light with a metallic sheen Degenerative retinopathy does not develop as it is
less retinotoxic compared to iron
REACTION OF ORGANIC FOREIGN BODY
E.g. wood and other vegetative material produce proliferative reaction characterised by formation of giant cells
Caterpillar hair produces ophthalmia nodosum ,which is characterised by severe granulomatous iridocyclitis with nodule formation .
SYMPATHETIC OPHTHALMITIS Serious bilateral granulomatous panuveitis which follows penetrating ocular trauma
Injured eye is exciting eye and fellow eye is sympathizing eye .
A)Predisposing factor
Follows penetrating wound
Wounds in the ciliary region (dangerous zone ) are more prone to it
more common in children than adults
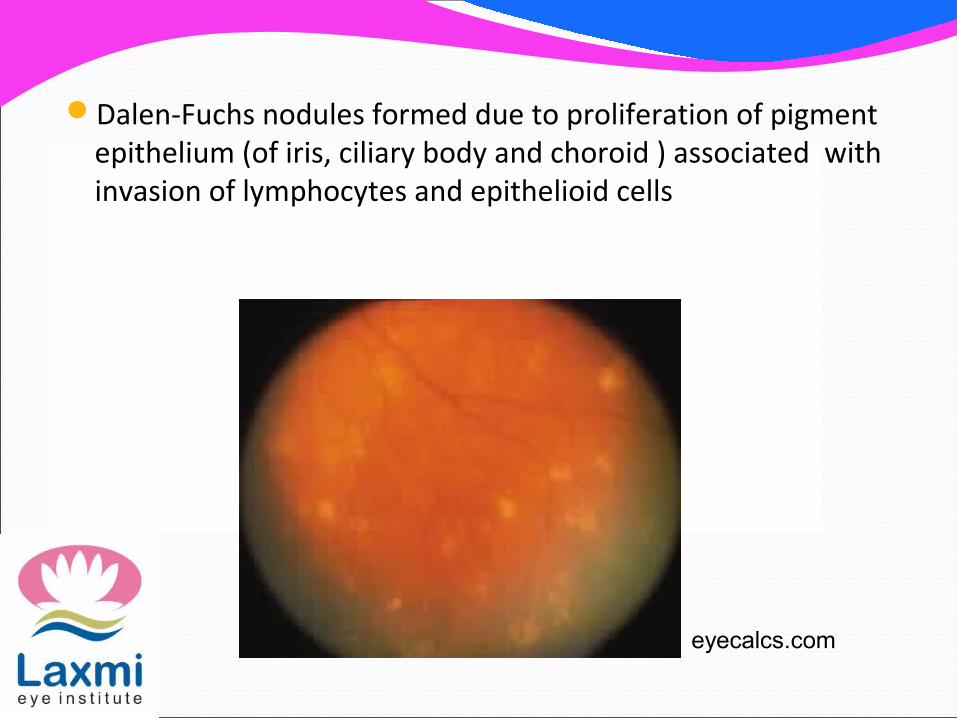
Dalen-Fuchs nodules formed due to proliferation of pigment
epithelium (of iris, ciliary body and choroid ) associated with invasion of lymphocytes and epithelioid cells
eyecalcs.com
CLINICAL PICTURE
1)Exciting ( injured eye ) –Shows clinical feature of persistent low grade plastic uveitis Ciliary congestion , lacrimation and tenderness Keratic precipitates may be present at the back of the cornea 2) Sympathizing ( sound eye ) –Usually involves 4 -8 weeks of injury in the other eye Manifest as acute iridocyclitis
TREATMENT
Prophylaxis meticulous repair of the wound using microsurgical technique
taking great care that uveal tissue is not incarcerated in the wound .
Corticosteroids (topical + sytemic), immunosuppressants
COMPLICATIONS – In Summary Rust ring on cornea at entry point Persistent inflammation Corneal defectsInfection – endophthalmitis Secondary glaucoma Lens damage –traumatic cataractsRetinal/vitreous damage Sympathetic ophthalmia
MANAGEMENT OF RETAINED IOFB
DIAGNOSIS –History – a careful history about the mode of injury may
give clue about the type of IOFBTime elapsed since injury
Ocular examination –A thorough ocular examination including slit lamp examination. Gonioscopy in select cases
SLIT LAMP PHOTOGRAPHY
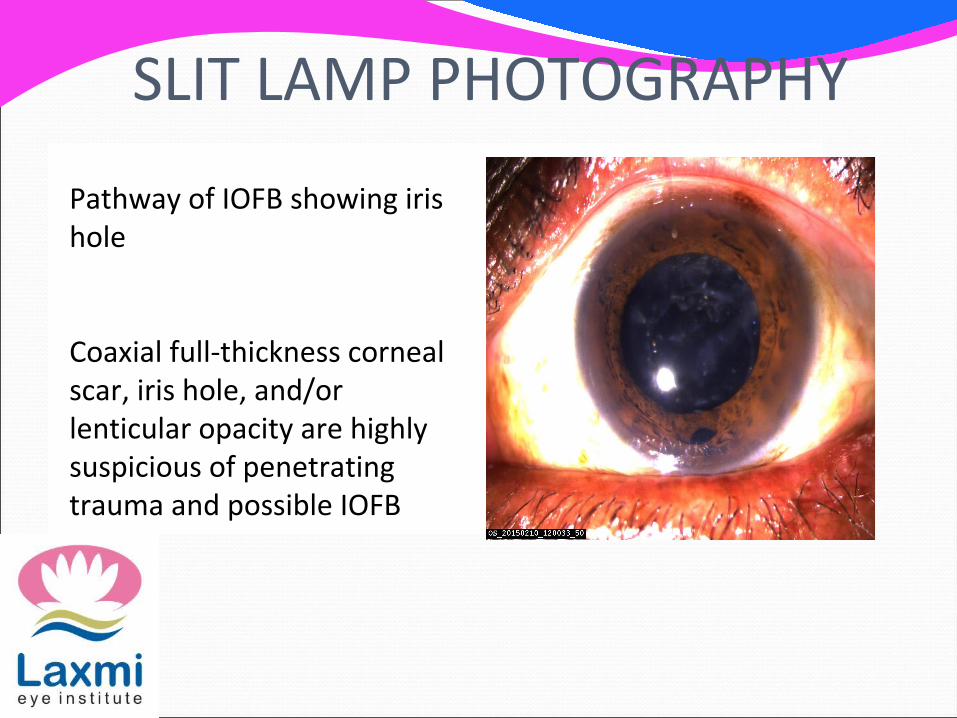
Pathway of IOFB showing iris hole
Coaxial full-thickness corneal scar, iris hole, and/or lenticular opacity are highly suspicious of penetrating trauma and possible IOFB
LOCALISATION OF IOFB
X-RayPlain X rays orbit Anterio-posterior and lateral views
as most foreign bodies are opaque .
Limbal Ring Method–Obsolete Metallic ring of corneal diameter stiched at limbus and x
ray taken in three exposures one while patient looking straight , upwards and downwards .

LIMBAL RING
USG
Features of IOFB on A scan Steeply rising wide echo spike seen
The reflectivity of the spike is extremely high (100% ) which persists on low gain
Sound attenuation is very strong
Features of B scan Appears hyperechoic in contrast to clear vitreousSound attenuation is very strong . IOFB causes shadowing
of ocular and orbital structure behind it .Associated ocular damage like vitreous haemorrhage,
retinal detachment can be assessed
USG localisation can tell position of even radiolucent foreign body
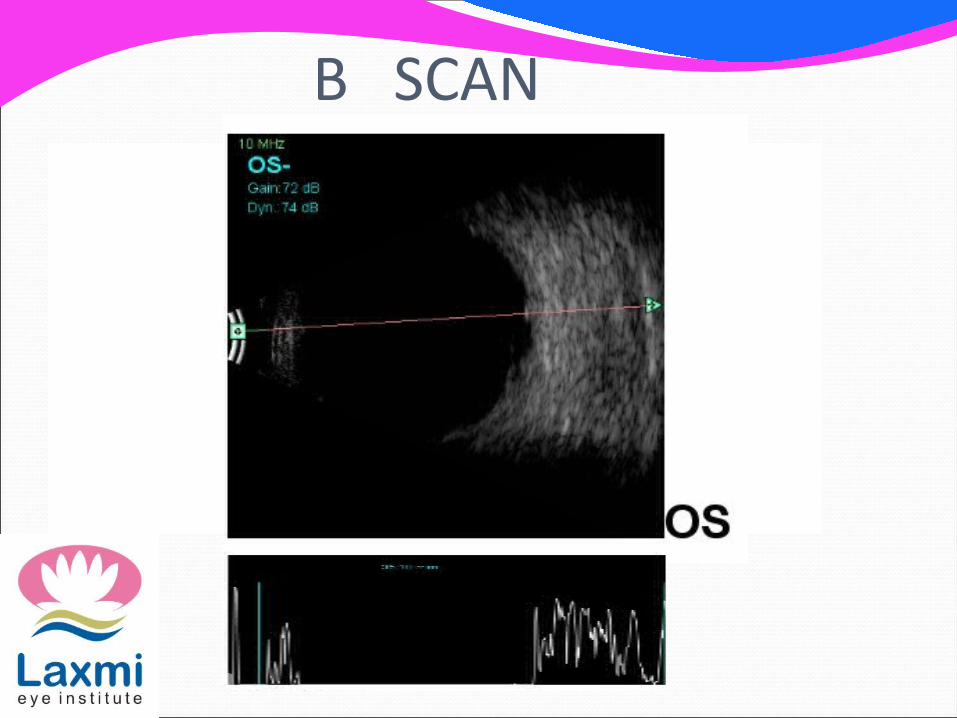
B SCAN
CT SCAN-Best method of localising IOFB Axial and coronal cut of < 1.5 mm are advised
MRI Contraindicated in case of metallic foreign body
MANAGEMENT Requires immediate closure of wound and removal of
IOFB .Delay> 24 hrs produces four fold increase risk of
endophthalmitis and vision lossPrompt removal before encapsulation facilitates removal and
prevents IOFB toxicityEyes should be protected with eye shieldIV broad spectrum antibiotic Tetanus prophylaxis ( Thomson JT et al . Infectious endophthalmitis after retained IOFB . Principles and practice of vitreo retinal surgery . 1993 , 1468-1474 . )
TREATMENT
IOFB should always be removed unless inert, sterile
Foreign body in anterior chamber removed through corresponding corneal incision directed straight towards the foreign body 3 mm incision internal to limbus is taken Magnetic foreign removed with hand held magnet and
nonmagnetic foreign body picked with toothless forceps .Viscoelastic protects delicate structures
Foreign body entangled in iris tissue –Sector iridectomy of part containing magnetic and non
magnetic foreign body .Foreign body in lens
Lens extraction with IOL implant Forceps removal with a pars plana vitrectomy –
Use of intraocular magnet or forceps, via sclerotomy or limbal route in aphakes
PROGNOSIS Depends on
Initial BCVA Time of surgery Initially attached retina Scleral entry site Presence of afferent pupillary defect Mechanism of injury Vitreous hemorrhage
(Akesbi J et al . IOFB of posterior segment : retrospective analysis and management of 57 cases . J Fr Ophtalmol 2011 Nov ;34 (9) 634- 640 .
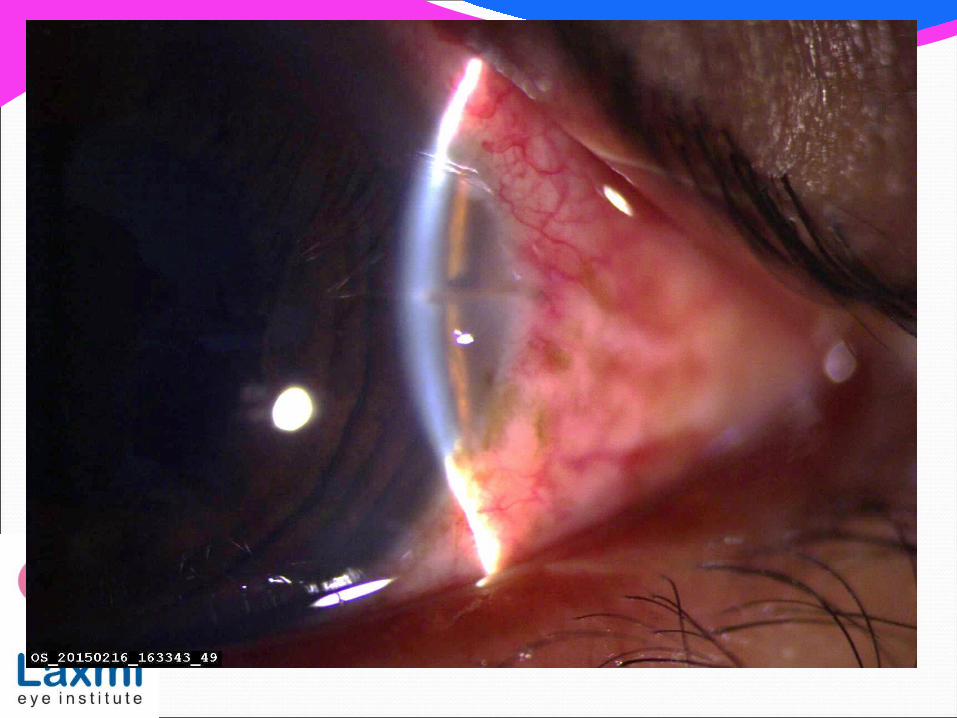
CASE
42 /M came with c/o DOV , pain ,redness in LE since one day
H /O foreign body (steel) particle entry in LE one day back
BCVA RE: 6/9, LE: HM


THANK YOU








![25-Gauge Vitrectomy in Open Eye Injury with Retained ...erior segment intraocular foreign bodies: visual results and ... [12] V. Mester and F. Kuhn, “Ferrous intraocular foreign](https://img.pdfslide.net/doc/110x75/60fc947980b8f13aeb33a84c/25-gauge-vitrectomy-in-open-eye-injury-with-retained-erior-segment-intraocular.jpg)