Embed Size (px)
Citation preview

Moving to a Person Centred Integrated
Acute - Subacute Community Service
Presentation Transfer of Care Conference
22 June 2015
Jenny Collins – Austin Health
Austin Health
• One of Victoria’s largest tertiary health services
• Major academic medical centre providing health services, health
professional education and research
• Austin Health operates 980 beds across acute, sub-acute and
mental health with an annual operating budget of more than $700
million.
• Employing >7,900 people across the Austin Hospital, Heidelberg
Repatriation Hospital (HRH) and the Royal Talbot Rehabilitation
Centre (RTRC).
• Broad catchment serving a population of approx 1.2 million
people
Austin Health
• During 2013-14, Austin Health completed 95,142 inpatient
admissions,177,027 outpatient attendances and 75,366
emergency attendances.
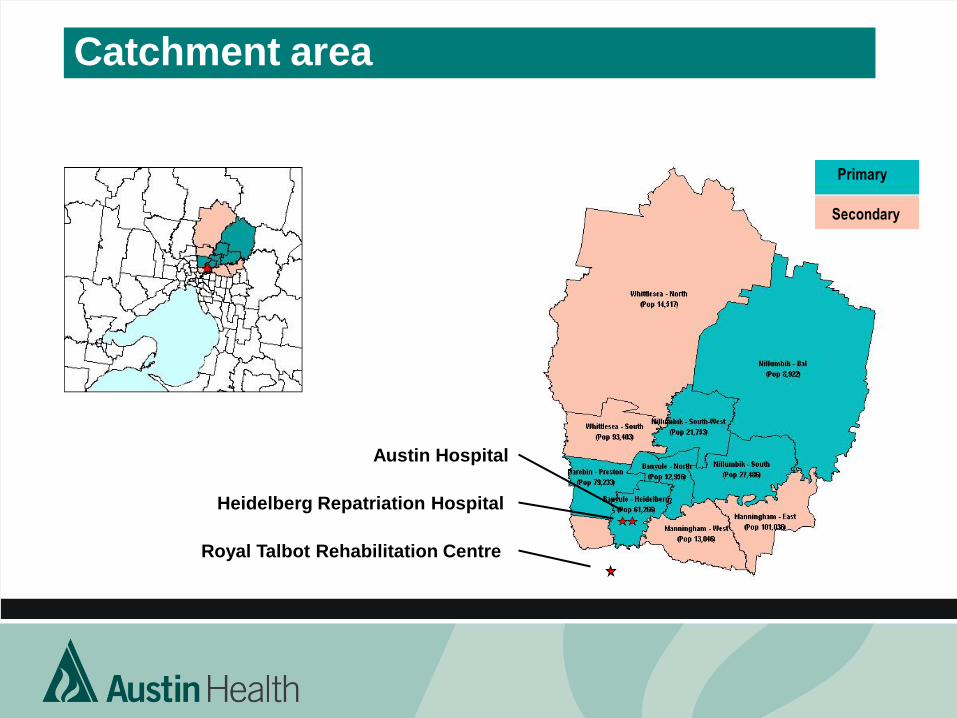
Catchment area
Austin Hospital
Heidelberg Repatriation Hospital
Royal Talbot Rehabilitation Centre
Primary
Secondary
What Are Health Independence Programs
• Deliver health care to support transition from hospital
to home.
• Prevent need for a hospital presentation or stay, with
some people accessing these services directly from
the community.
• Client Centred and integrated delivery of services.
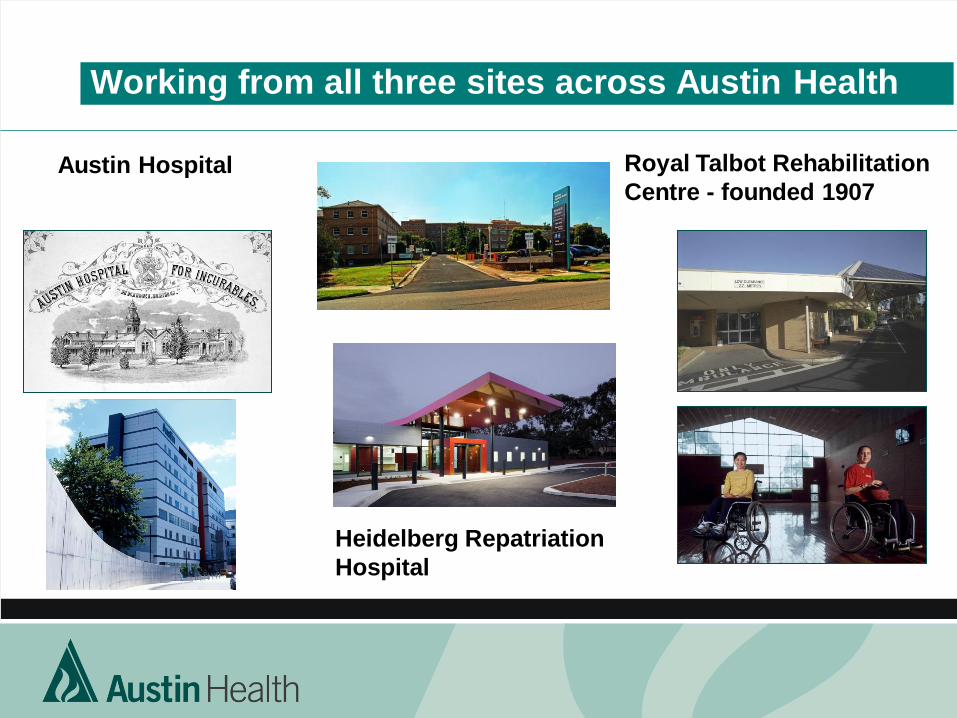
Working from all three sites across Austin Health
Austin Hospital
Heidelberg Repatriation
Hospital
Royal Talbot Rehabilitation
Centre - founded 1907
Drivers For Change Context of Healthcare
• Increasing demand
– Growing population
– Ageing population
– Increasing co-morbidities/chronic disease
– Increased expectations and less access to GPs
• Workforce
– Traditional models stretched but insufficient progress on new models
– Turnover and shortages
– Siloed
• Policy - Constrained funding
– Driving greater integration
– Increased focus toward a positive impact on acute demand
– Shrinking resources
– Department of Health – Health Independence Program Guidelines
What that means to Austin Health
• Increasing complexity of patients
• Increasing age of patients
• Pressure on acute to move patients downstream to
subacute or the community.
• Increasing number of patients that do not fit our traditional
service models.
• Challenges to discharge
Questions?
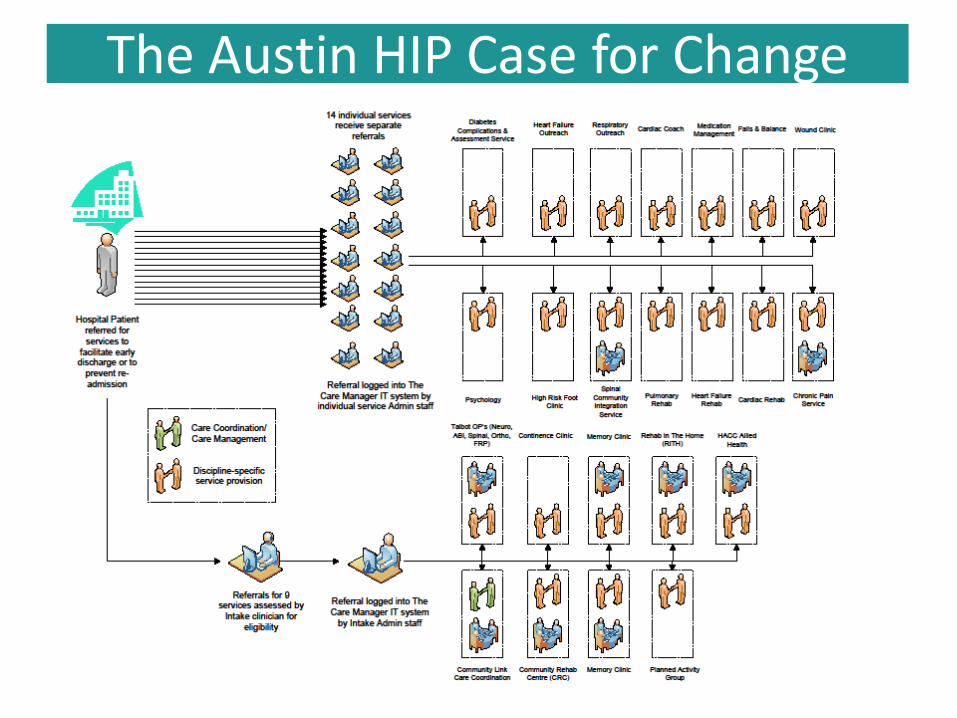
The Austin HIP Case for Change
WHY Health Independence Program
Integration – Client- Patient
•Deliver person centred care for all HIP clients
•Better Client outcomes - seamless pathway from entry to
hospital to discharge
•Improve the patient experience
•Improve equity of access for HIP eligible clients
•Provide care coordination of complex needs for all HIP
clients
WHY Health Independence Program
Integration – Staff
•Increased opportunity for:
• skilled and experienced staff to ensure a client-centred
continuity of care approach wherever possible
• professional disciplines with regard to practice
•Efficiencies in service delivery and profession supervision
for HIP Staff and Austin Health more broadly
WHY Health Independence Program
Integration – System
•Simplify the HIP service system
•Minimise duplication
•Reduce fragmentation of service delivery across funding
streams
•Increase flexibility in service delivery
•Improved Efficiencies
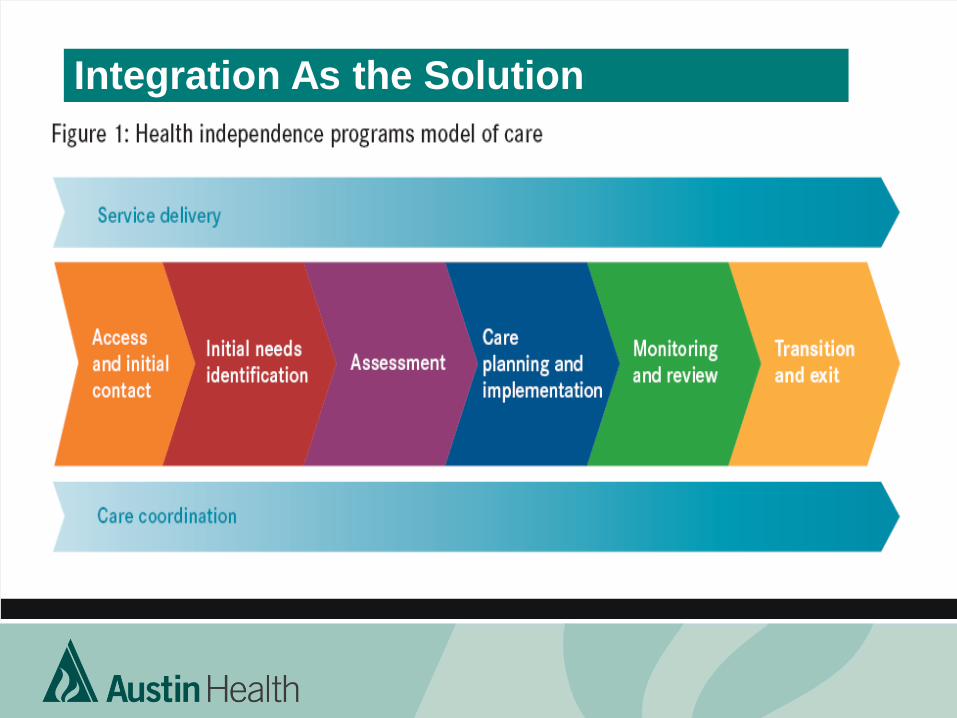
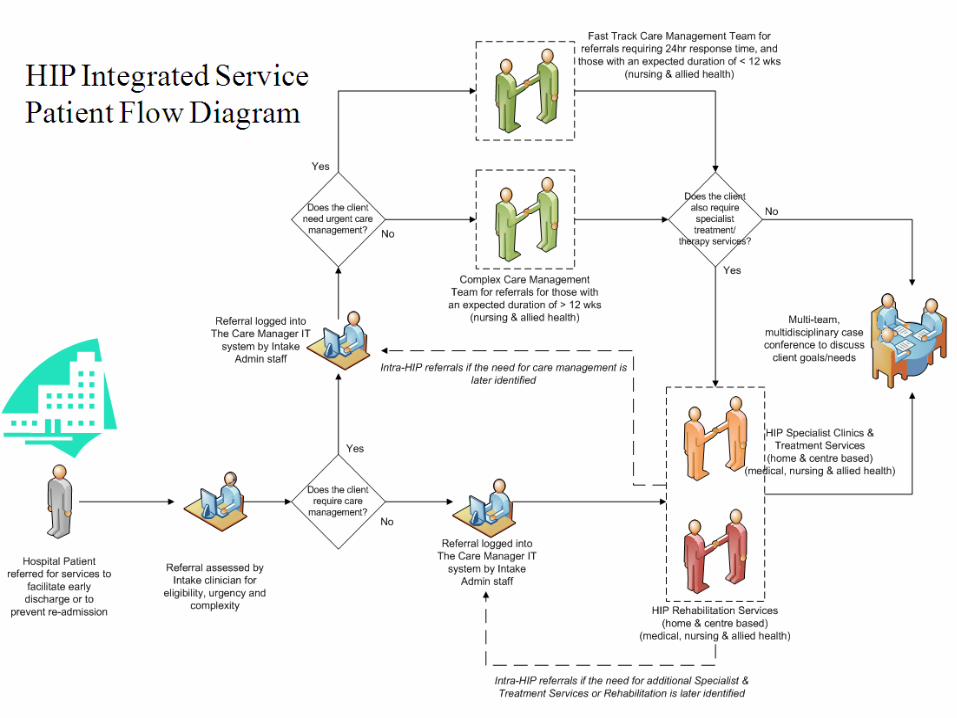
Integration As the Solution
Planning For Change
• Stakeholder Engagement – Workshop – Outcome: shared
Austin Vision
• Development of the HIP Integrated Service Model
• Establishment of Key Deliverables – Evaluation Framework
• Matching the workforce to the service model
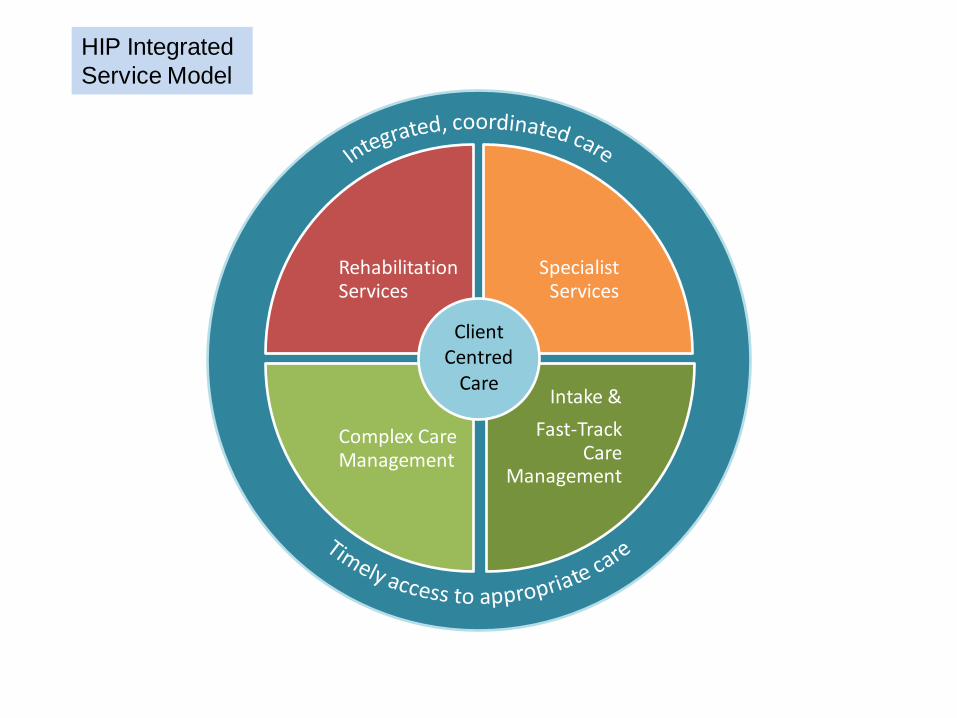
Rehabilitation Services
Specialist Services
Intake &
Fast-Track Care
Management
Complex Care Management
Client Centred
Care
HIP Integrated
Service Model
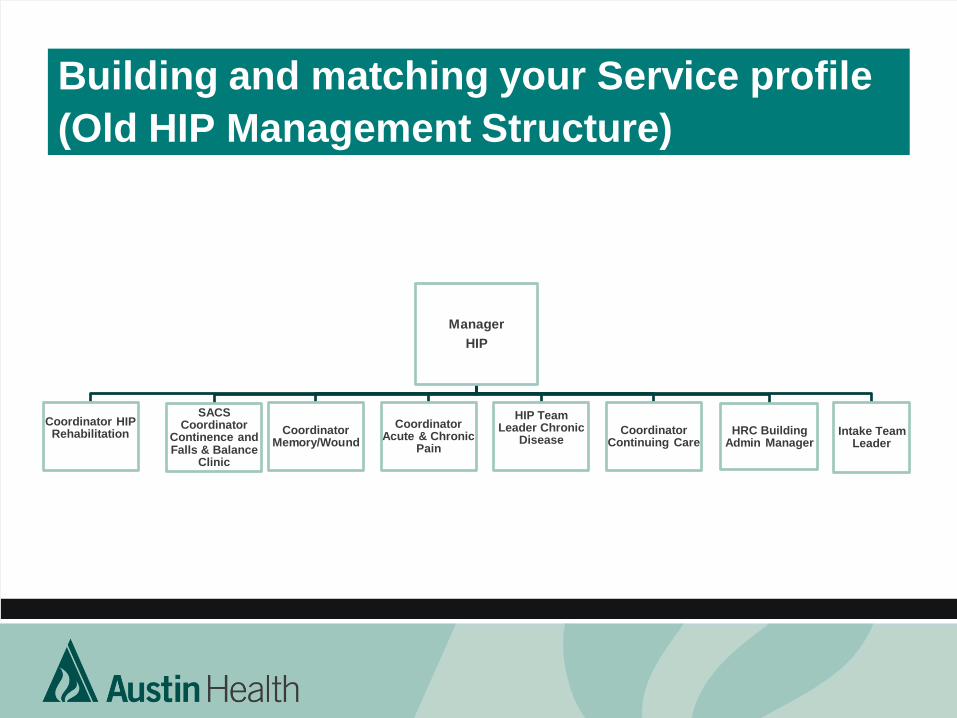
Building and matching your Service profile
(Old HIP Management Structure)
Manager
HIP
Coordinator HIP Rehabilitation
SACS Coordinator
Continence and Falls & Balance
Clinic
Coordinator Memory/Wound
Coordinator Acute & Chronic
Pain
HIP Team Leader Chronic
Disease
Coordinator Continuing Care
HRC Building Admin Manager
Intake Team Leader
Building and Matching your Service profile
(Old HIP Clinical Structure) Your Workforce
Matching staff to integrated clinical structure
• Align Leadership structure with vision and model of care
• Match like intervention with like
• Broaden senior clinician leadership participation \ Identify
training needs
• Develop a change management strategy
• Executive sign off and approval
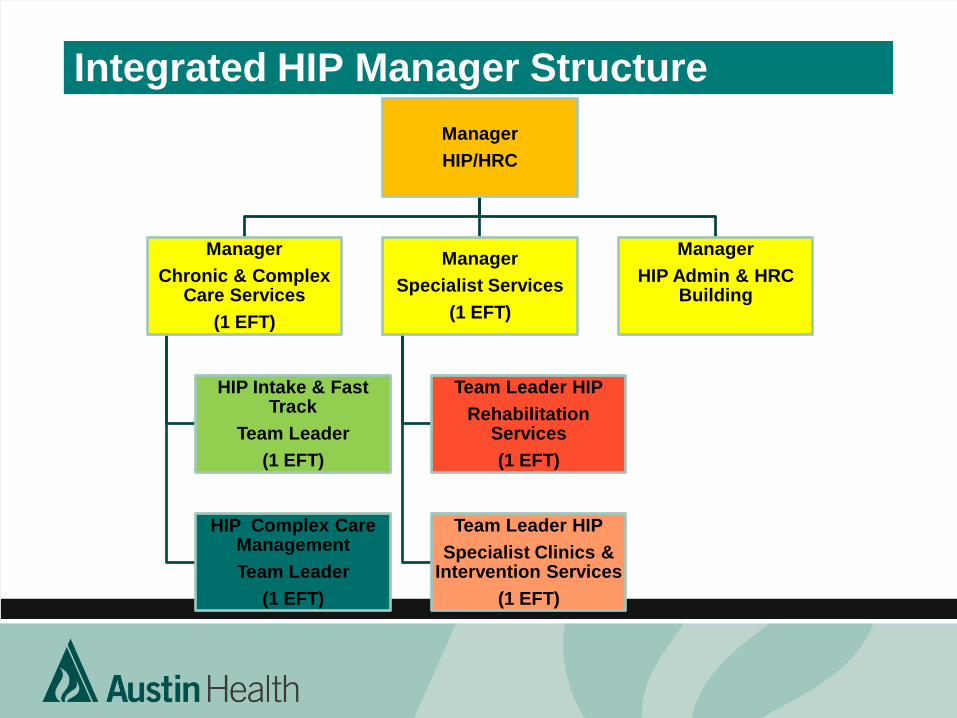
Integrated HIP Manager Structure
Manager
HIP/HRC
Manager
Chronic & Complex Care Services
(1 EFT)
HIP Intake & Fast Track
Team Leader
(1 EFT)
HIP Complex Care Management
Team Leader
(1 EFT)
Manager
Specialist Services
(1 EFT)
Team Leader HIP
Rehabilitation Services
(1 EFT)
Team Leader HIP
Specialist Clinics & Intervention Services
(1 EFT)
Manager
HIP Admin & HRC Building
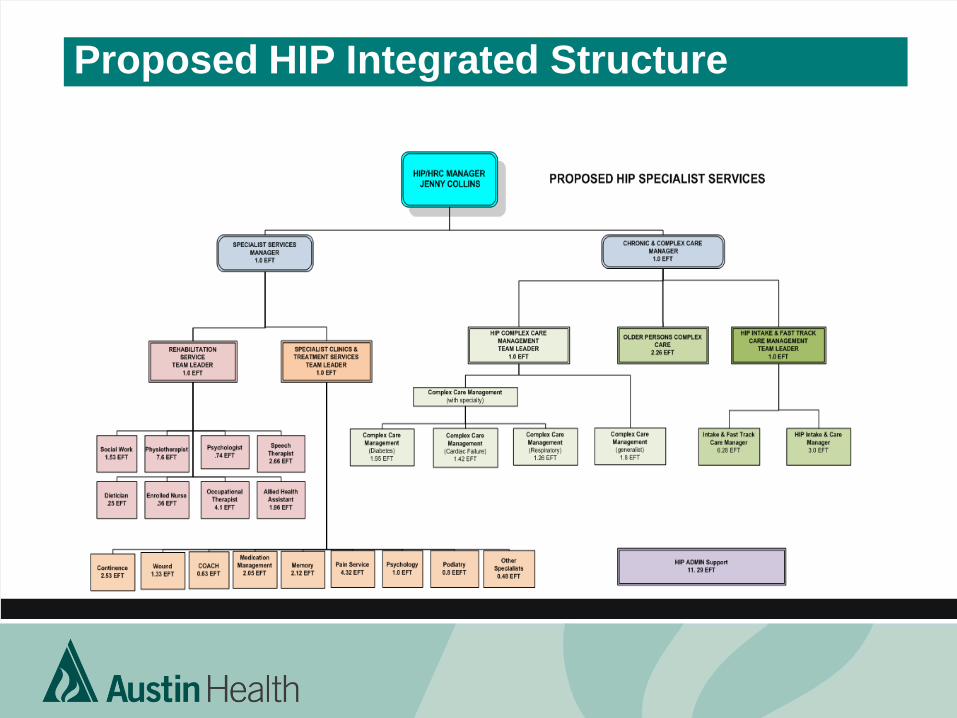
Proposed HIP Integrated Structure
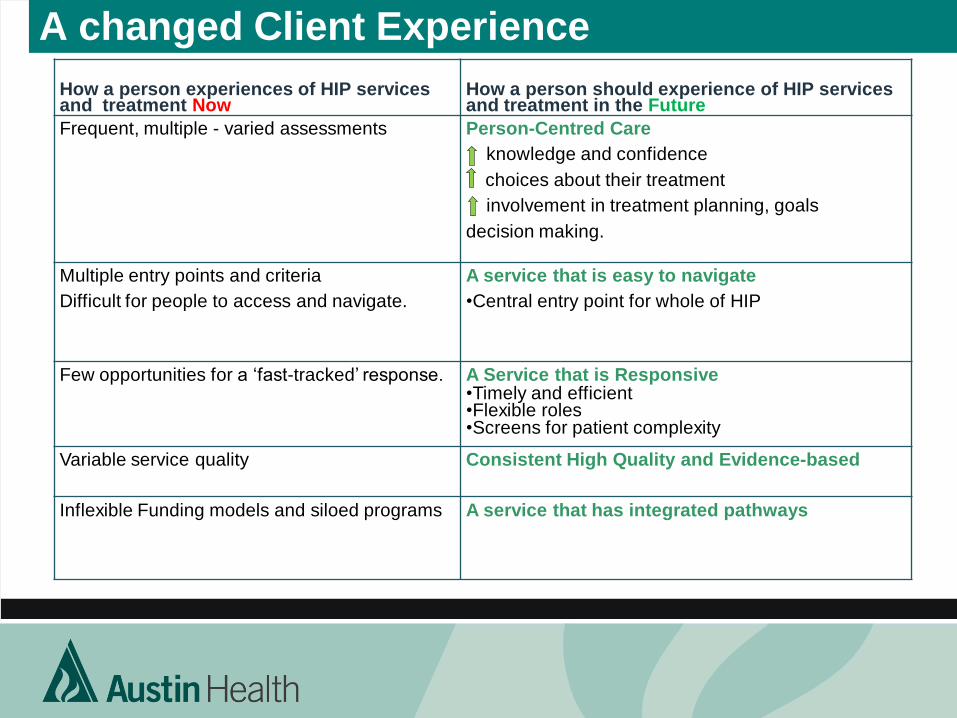
A changed Client Experience
How a person experiences of HIP services and treatment Now
How a person should experience of HIP services and treatment in the Future
Frequent, multiple - varied assessments Person-Centred Care
knowledge and confidence
choices about their treatment
involvement in treatment planning, goals
decision making.
Multiple entry points and criteria
Difficult for people to access and navigate.
A service that is easy to navigate
•Central entry point for whole of HIP
Few opportunities for a ‘fast-tracked’ response. A Service that is Responsive •Timely and efficient •Flexible roles •Screens for patient complexity
Variable service quality Consistent High Quality and Evidence-based
Inflexible Funding models and siloed programs
A service that has integrated pathways
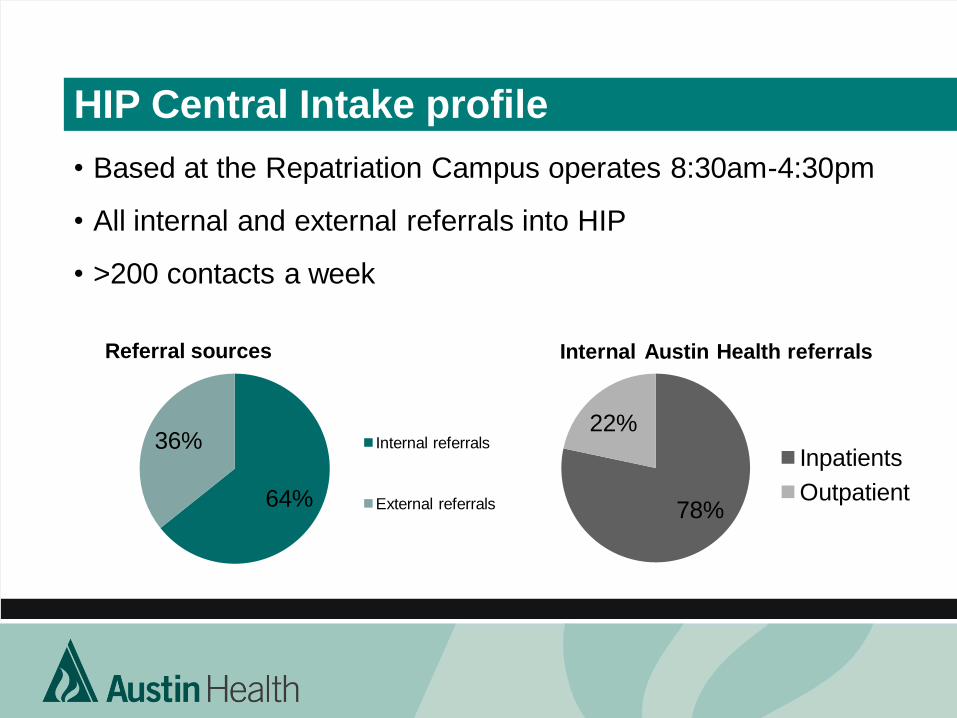
HIP Central Intake profile
• Based at the Repatriation Campus operates 8:30am-4:30pm
• All internal and external referrals into HIP
• >200 contacts a week
64%
36%
Referral sources
Internal referrals
External referrals 78%
22%
Internal Austin Health referrals
Inpatients
Outpatient
0
200
400
600
800
1000
1200
July August September October November December
Nu
mb
er o
f n
ew r
efe
rral
s
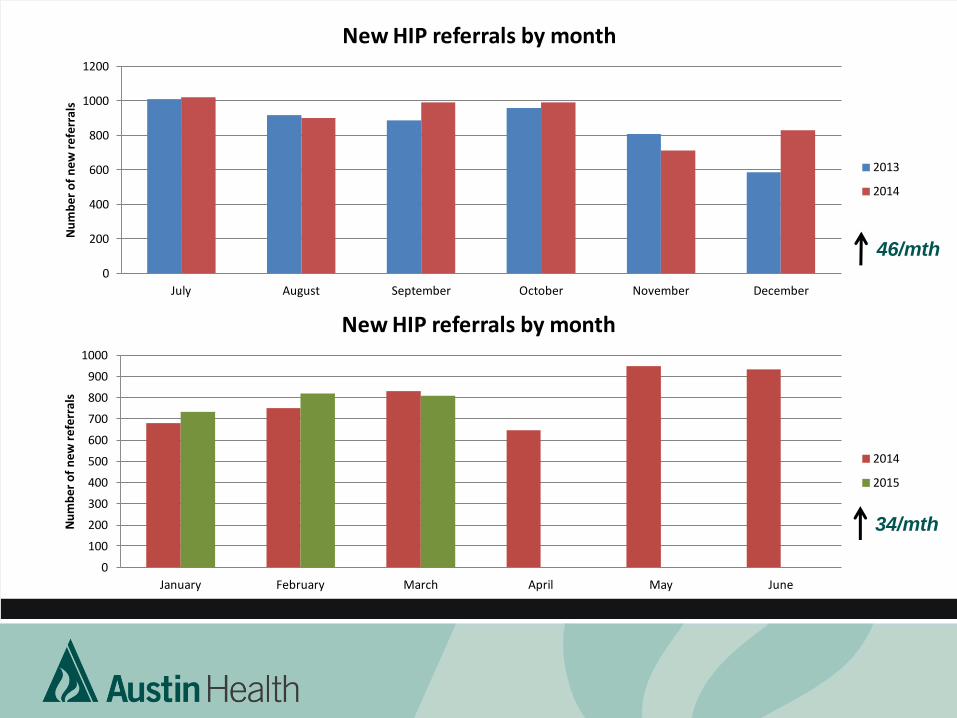
New HIP referrals by month
2013
2014
0
100
200
300
400
500
600
700
800
900
1000
January February March April May June
Nu
mb
er o
f n
ew r
efe
rral
s
New HIP referrals by month
2014
2015
46/mth
34/mth
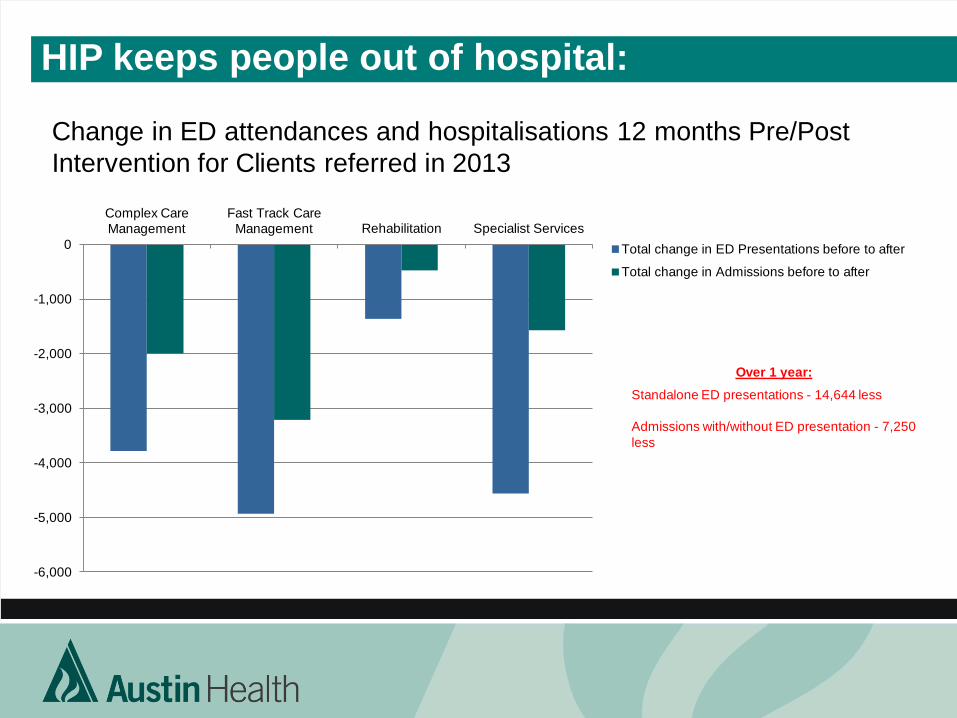
HIP keeps people out of hospital:
Change in ED attendances and hospitalisations 12 months Pre/Post
Intervention for Clients referred in 2013
-6,000
-5,000
-4,000
-3,000
-2,000
-1,000
0
Complex Care
Management
Fast Track Care
Management Rehabilitation Specialist Services
Total change in ED Presentations before to after
Total change in Admissions before to after
Over 1 year:
Standalone ED presentations - 14,644 less
Admissions with/without ED presentation - 7,250
less
Learnings to facilitate success
• Develop a clear vision!
• Clear rationale – Why are we doing this?
• Executive Leadership and support
• Culture Change as well as Service Change
This takes time and may be difficult!
• Stakeholder communication and management
Acknowledgements
• Alan McCubbin
• Evelyn Gould
• HIP Team
Questions?