Embed Size (px)
Citation preview
The Conundrum of Mitral Regurgitation
in Heart Failure
Multimodality ImagingMultimodality ImagingPhilippe Pibarot, DVM, PhD, Philippe Pibarot, DVM, PhD, FACC, FASE, FESCFACC, FASE, FESCCanada Canada Research Chair in Valvular Heart Research Chair in Valvular Heart DiseaseDisease
UniversitéUniversitéLAVALLAVAL
InstitutInstitut UniversitaireUniversitaire de Cardiologie de Cardiologie et de Pneumologie de Québec / et de Pneumologie de Québec / Québec Heart & Lung InstituteQuébec Heart & Lung Institute
Disclosure related to this Disclosure related to this presentation: presentation: NoneNone
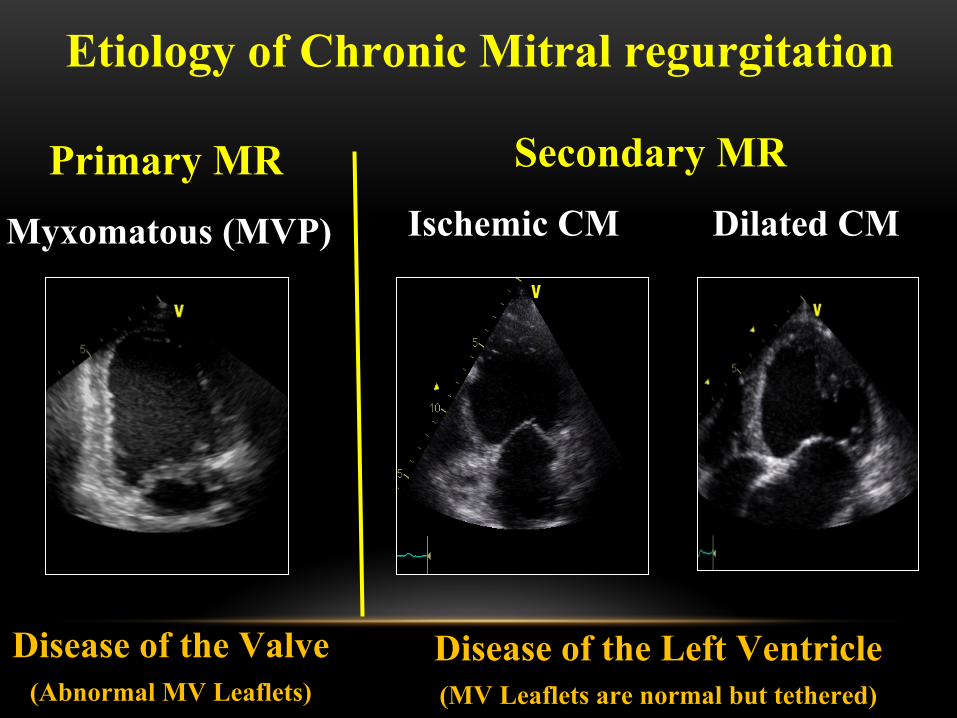
Etiology of Chronic Mitral regurgitation
Primary MRMyxomatous (MVP)
Secondary MRIschemic CM Dilated CM
Disease of the Valve(Abnormal MV Leaflets)
Disease of the Left Ventricle(MV Leaflets are normal but tethered)
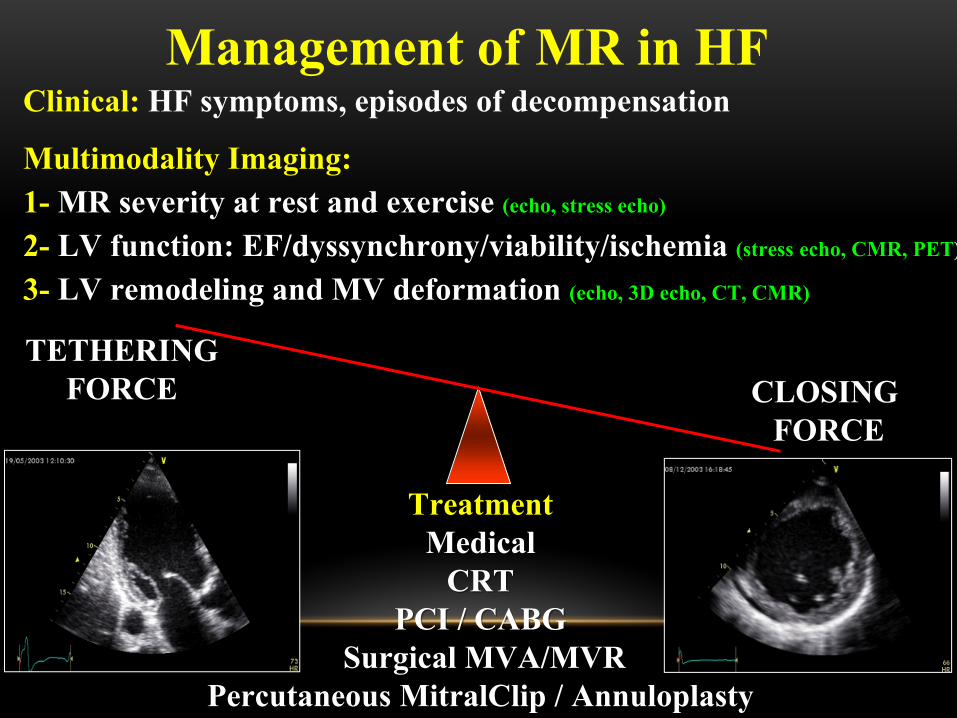
Management of MR in HF
TreatmentMedicalMedical
CRTCRTPCI / CABGPCI / CABG
SurgicalSurgical MVA/MVRMVA/MVRPercutaneousPercutaneous MitralClipMitralClip / Annuloplasty / Annuloplasty
TETHERING FORCE CLOSING
FORCE
Multimodality Imaging:1- MR severity at rest and exercise (echo, stress echo)
2- LV function: EF/dyssynchrony/viability/ischemia (stress echo, CMR, PET)
3- LV remodeling and MV deformation (echo, 3D echo, CT, CMR)
Clinical: HF symptoms, episodes of decompensation
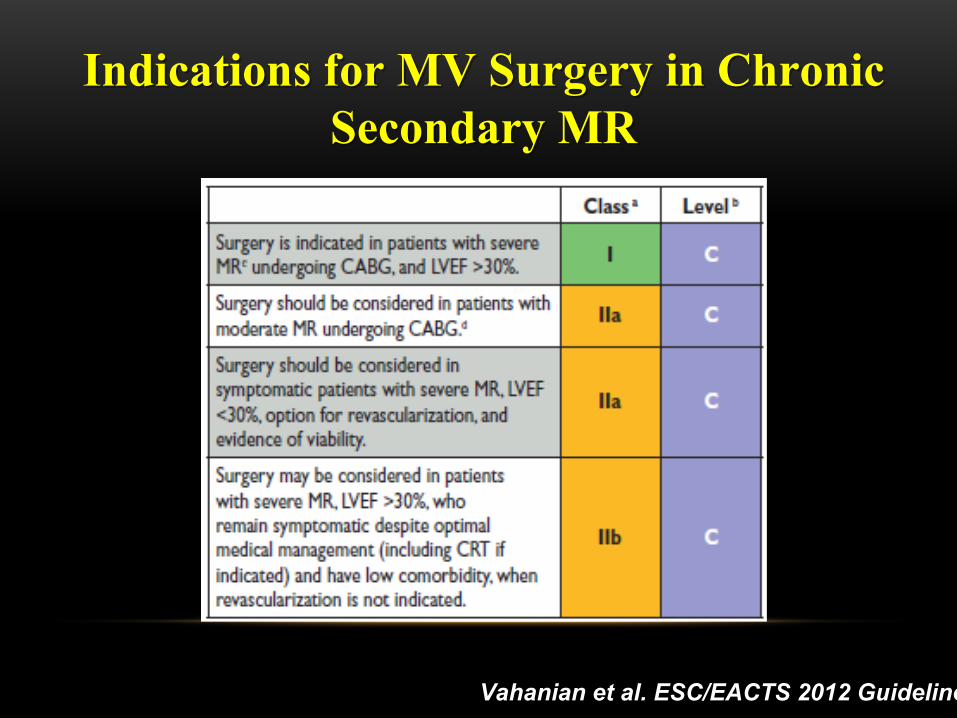
Indications for Indications for MV Surgery MV Surgery in in Chronic Chronic Secondary MRSecondary MR
Vahanian et al. ESC/EACTS 2012 Guidelines
Multimodality Imaging – Step 1
Assessing of MR Severity at rest and during exercise
- To stratify risk
- To determine indication for MV intervention
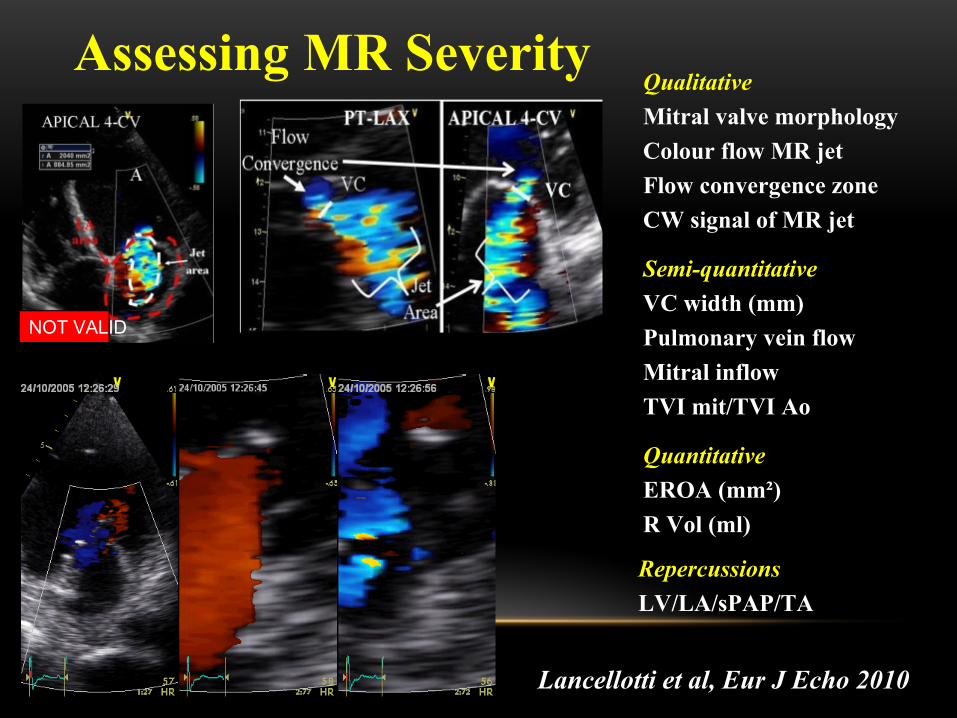
Assessing MR Severity
NOT VALID
Lancellotti et al, Eur J Echo 2010
QualitativeMitral valve morphologyColour flow MR jetFlow convergence zoneCW signal of MR jet
Semi-quantitativeVC width (mm)Pulmonary vein flowMitral inflowTVI mit/TVI Ao
QuantitativeEROA (mm²)R Vol (ml)
RepercussionsLV/LA/sPAP/TA
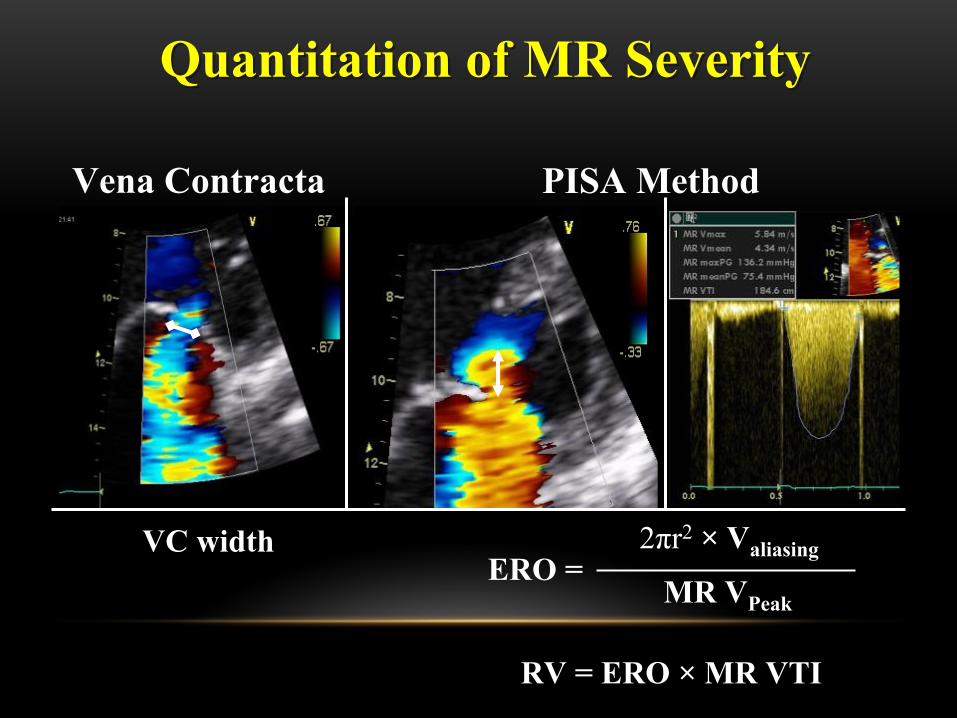
ERO =MR VPeak
RV = ERO × MR VTI
VC width
Quantitation of MR SeverityQuantitation of MR Severity
2πr2 × Valiasing
Vena Contracta PISA Method
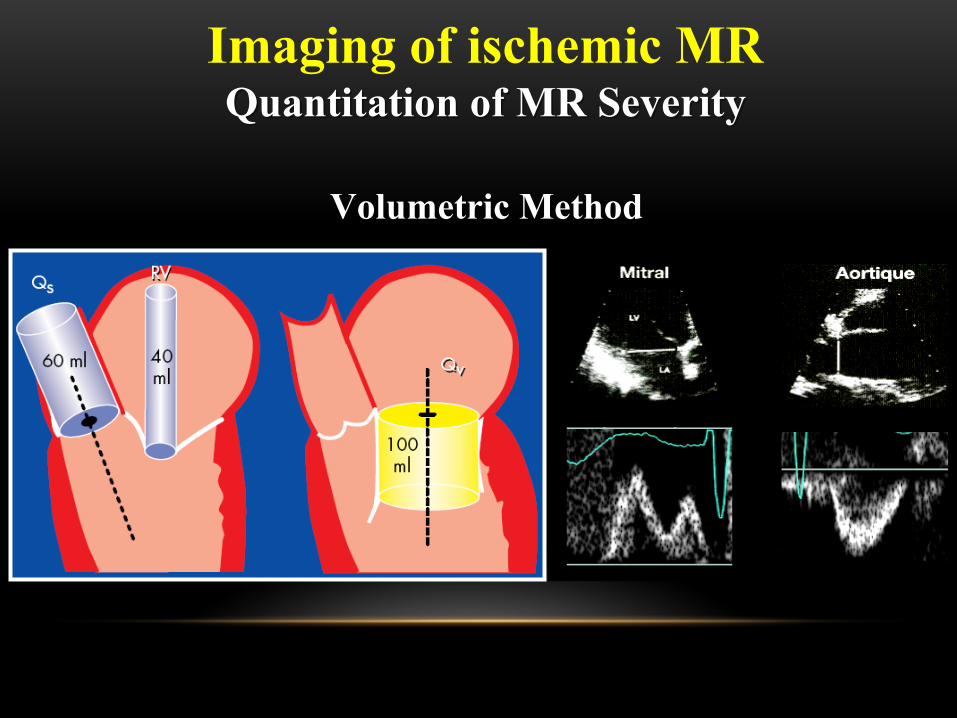
Imaging of ischemic MRQuantitation of MR SeverityQuantitation of MR Severity
Volumetric Method
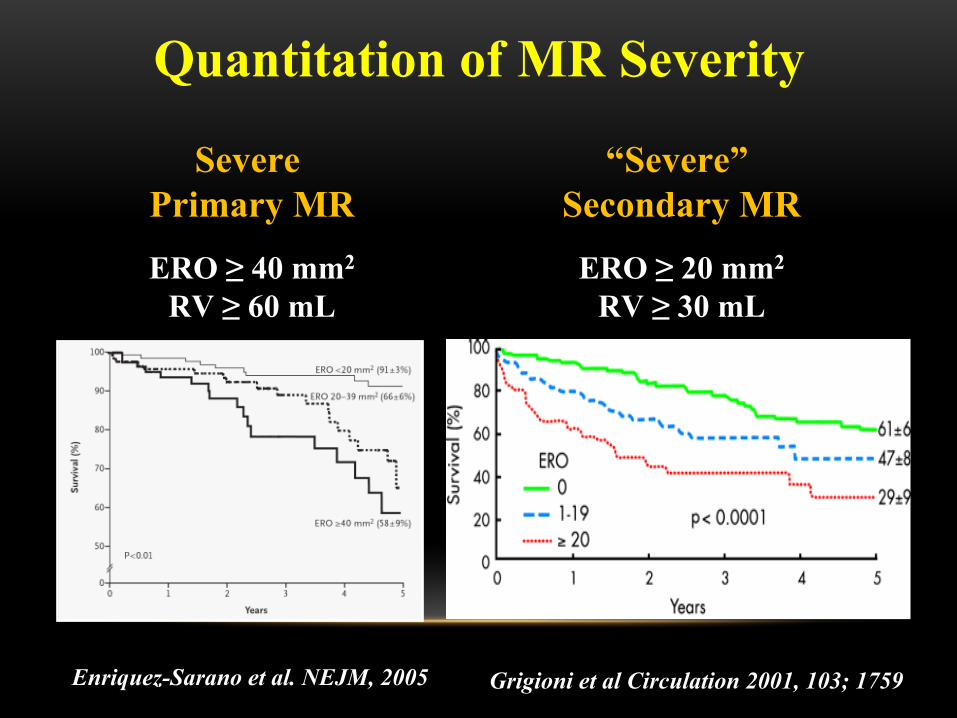
Quantitation of MR Severity
Severe Primary MR
ERO ≥ 40 mm2
RV ≥ 60 mL
“Severe” Secondary MR
ERO ≥ 20 mm2
RV ≥ 30 mL
Enriquez-Sarano et al. NEJM, 2005 Grigioni et al Circulation 2001, 103; 1759
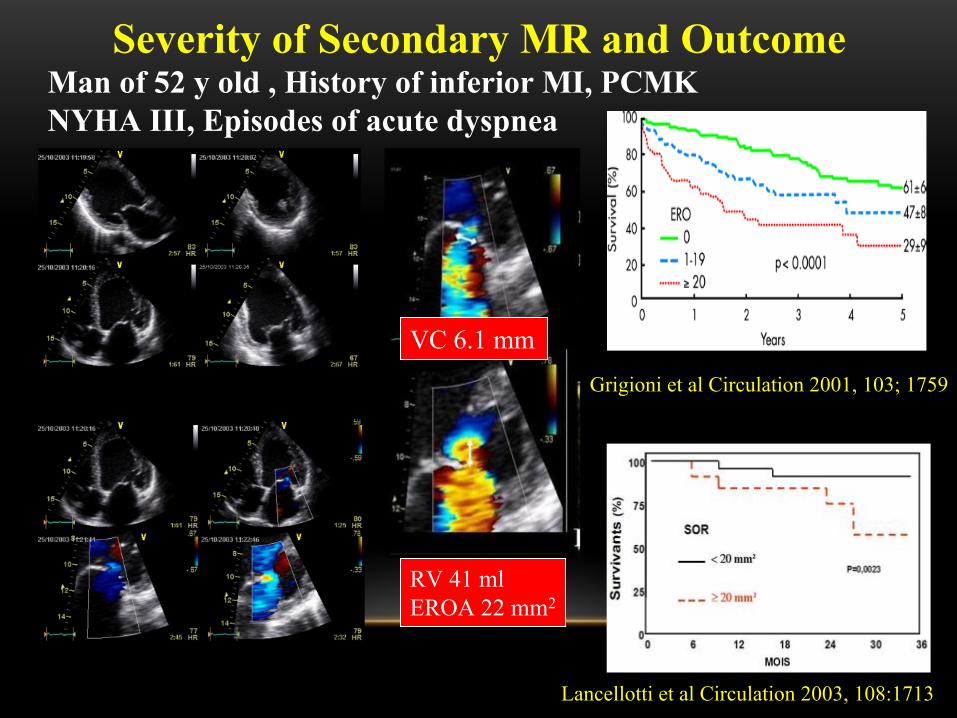
VC 6.1 mm
RV 41 mlEROA 22 mm2
Man of 52 y old , History of inferior MI, PCMK NYHA III, Episodes of acute dyspnea
Grigioni et al Circulation 2001, 103; 1759
Lancellotti et al Circulation 2003, 108:1713
Severity of Secondary MR and Outcome
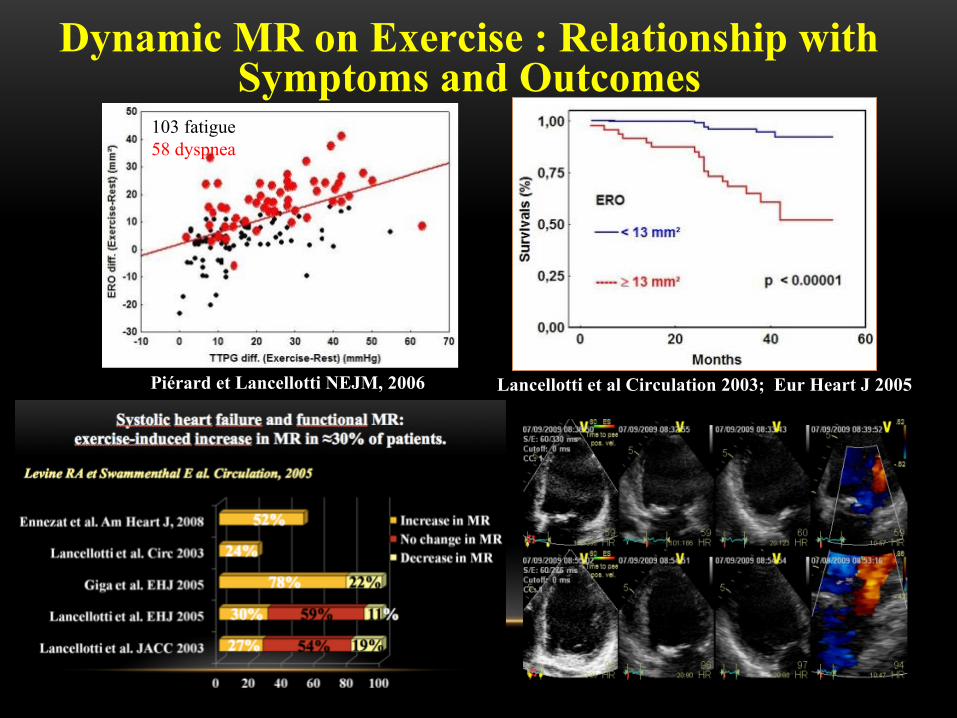
103 fatigue58 dyspnea
Dynamic MR on Exercise : Relationship with Symptoms and Outcomes
Lancellotti et al Circulation 2003; Eur Heart J 2005Piérard et Lancellotti NEJM, 2006
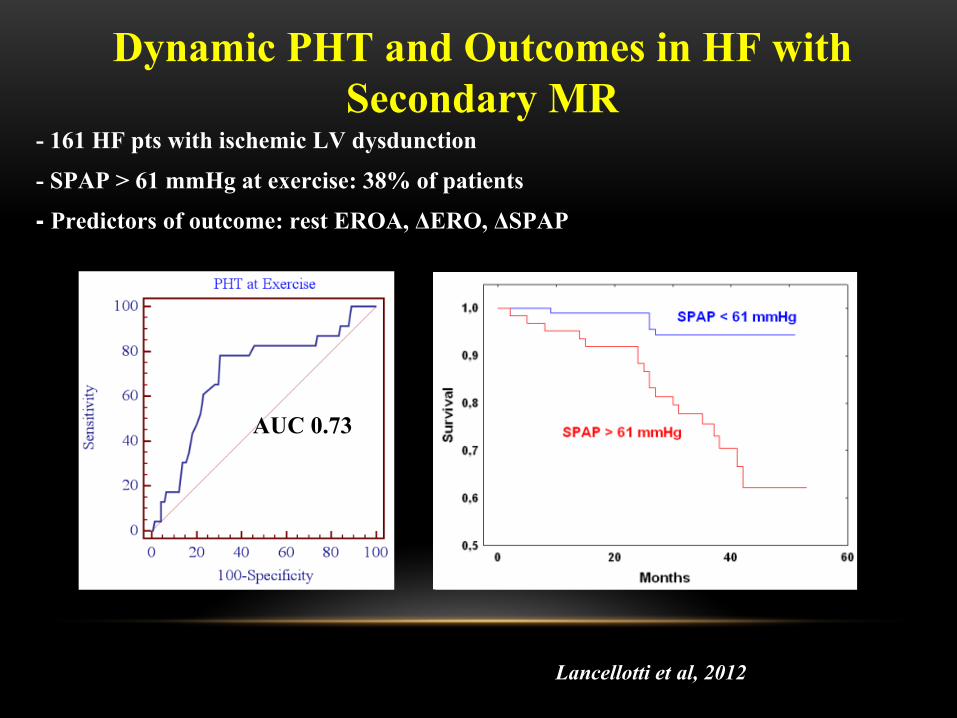
Lancellotti et al, 2012
Dynamic PHT and Outcomes in HF with Secondary MR
AUC: 0.7 for 61 mmHg
- 161 HF pts with ischemic LV dysdunction
- SPAP > 61 mmHg at exercise: 38% of patients
- Predictors of outcome: rest EROA, ΔERO, ΔSPAP
AUC 0.73
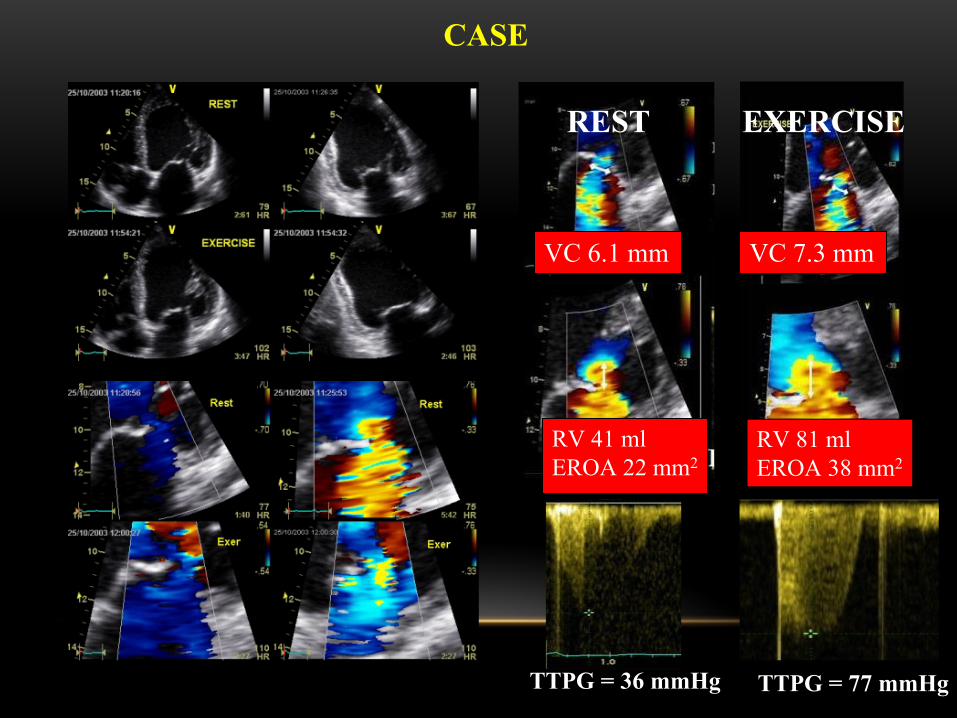
REST EXERCISE
VC 7.3 mmVC 6.1 mm
RV 41 mlEROA 22 mm2
CASE
RV 81 mlEROA 38 mm2
TTPG = 77 mmHgTTPG = 36 mmHg
Secondary MR is a disease of the left ventricle!
So look at MR Severity and …. at the left ventricle
Multimodality Imaging – Step 2
Assessing LV function/ synchrony / viability/ ischemia
- To stratify risk
- To determine indication for CRT
- To determine indication and options for revascularization
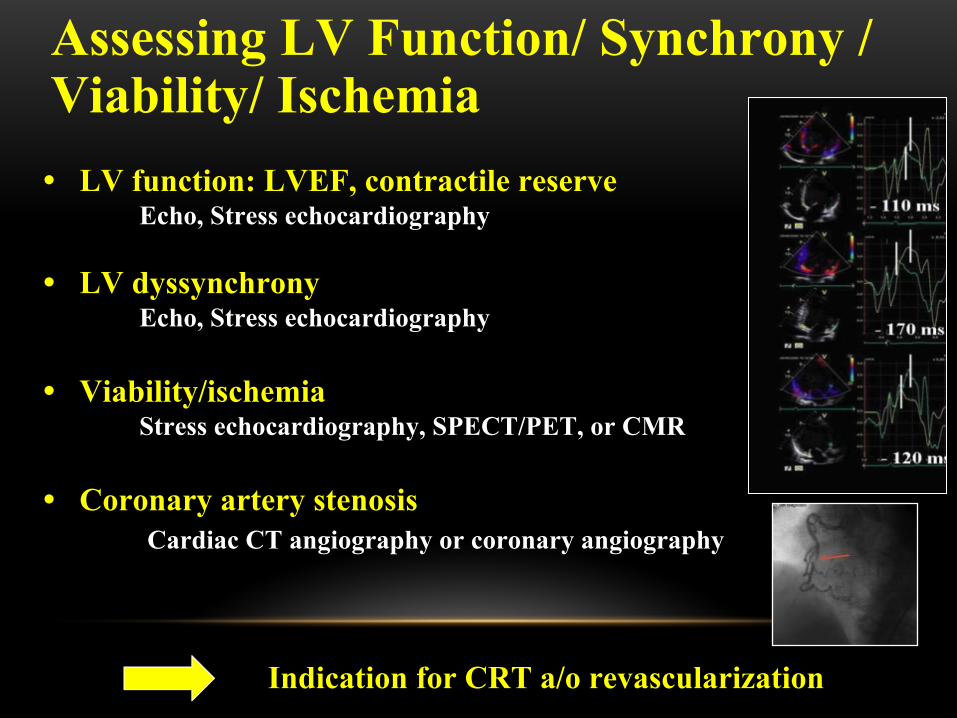
• LV function: LVEF, contractile reserveEcho, Stress echocardiography
• LV dyssynchronyEcho, Stress echocardiography
• Viability/ischemiaStress echocardiography, SPECT/PET, or CMR
• Coronary artery stenosis Cardiac CT angiography or coronary angiography
Assessing LV Function/ Synchrony / Viability/ Ischemia
Indication for CRT a/o revascularization
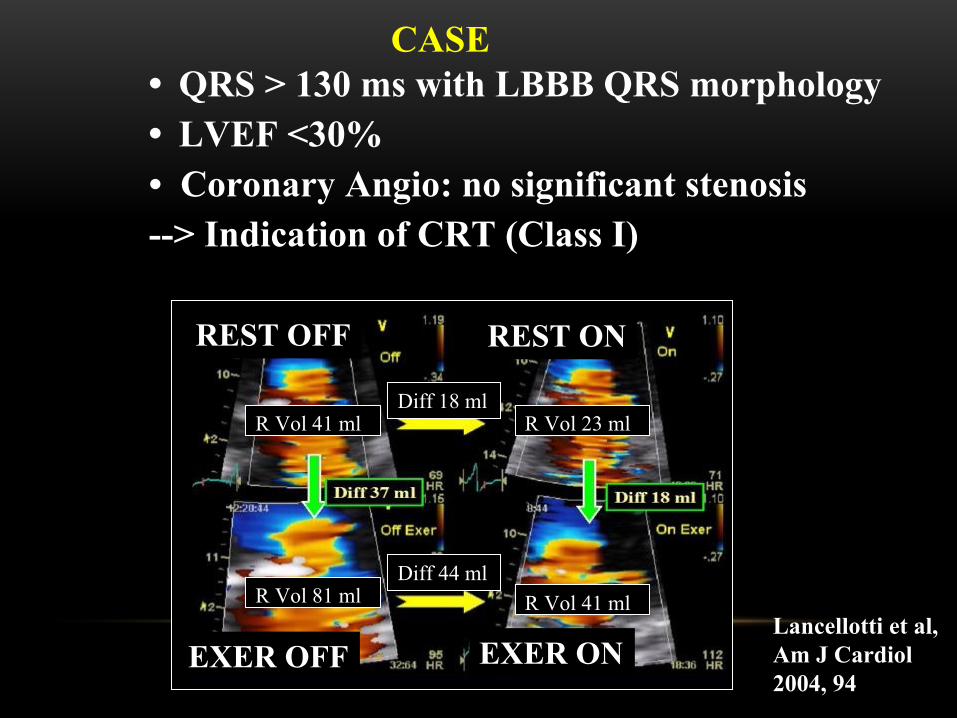
CASE • QRS > 130 ms with LBBB QRS morphology• LVEF <30%• Coronary Angio: no significant stenosis--> Indication of CRT (Class I)
Lancellotti et al, Am J Cardiol 2004, 94
R Vol 41 ml
R Vol 81 ml R Vol 41 ml
R Vol 23 mlDiff 18 ml
Diff 44 ml
REST OFF REST ON
EXER OFF EXER ON
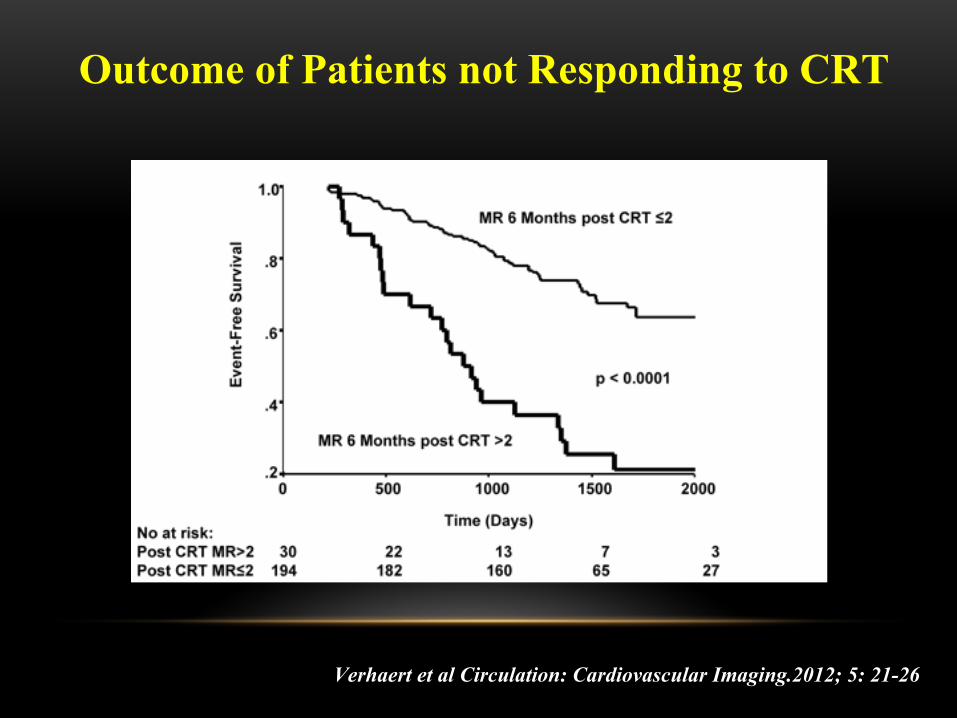
Verhaert et al Circulation: Cardiovascular Imaging.2012; 5: 21-26
Outcome of Patients not Responding to CRT
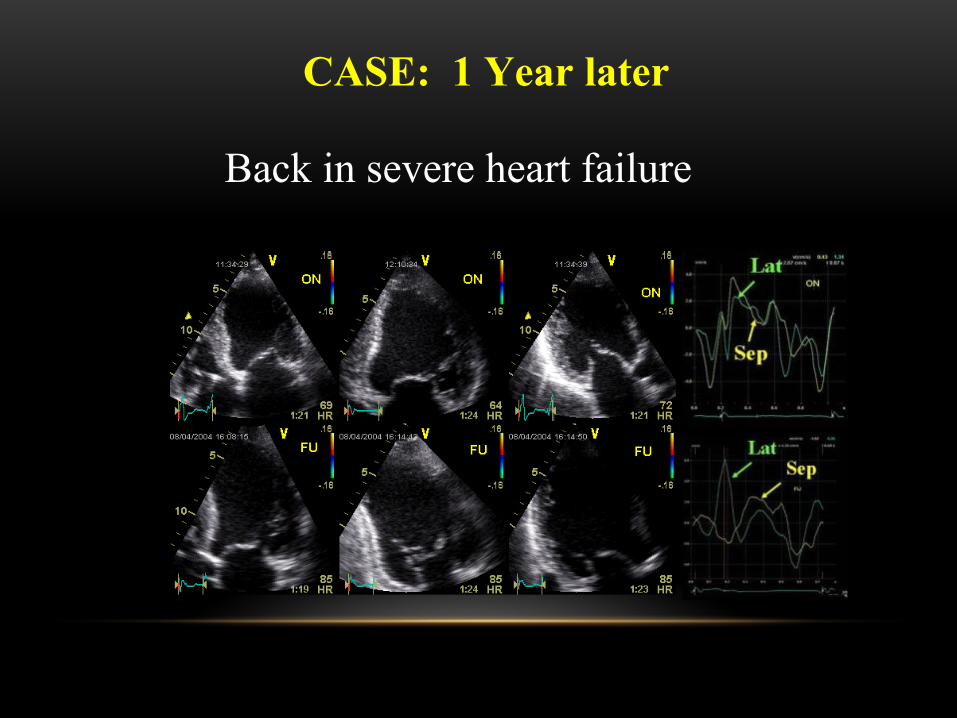
CASE: 1 Year later
Back in severe heart failure
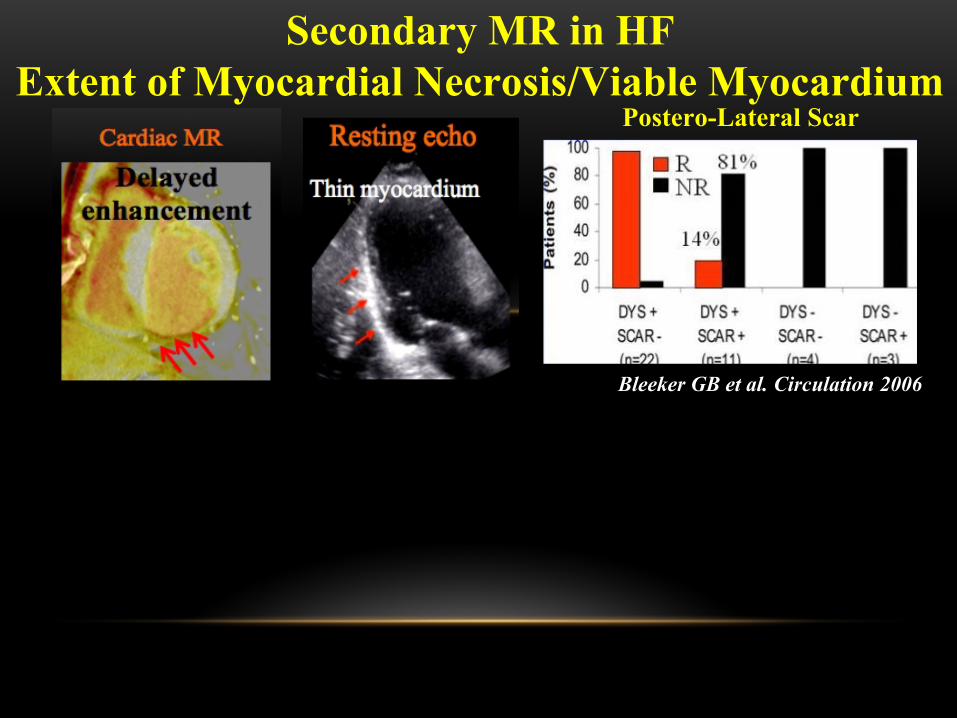
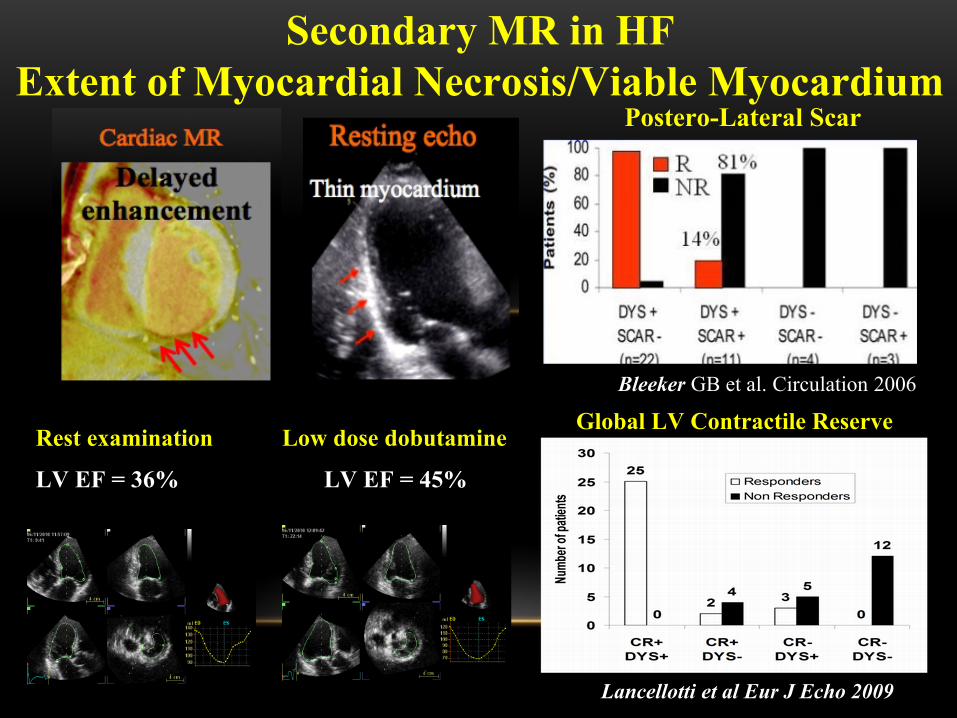
Secondary MR in HFExtent of Myocardial Necrosis/Viable Myocardium
Postero-Lateral Scar
Bleeker GB et al. Circulation 2006
Postero-Lateral Scar
Lancellotti et al Eur J Echo 2009
Bleeker GB et al. Circulation 2006
Global LV Contractile ReserveRest examination
LV EF = 36%
Low dose dobutamine
LV EF = 45%
Secondary MR in HFExtent of Myocardial Necrosis/Viable Myocardium
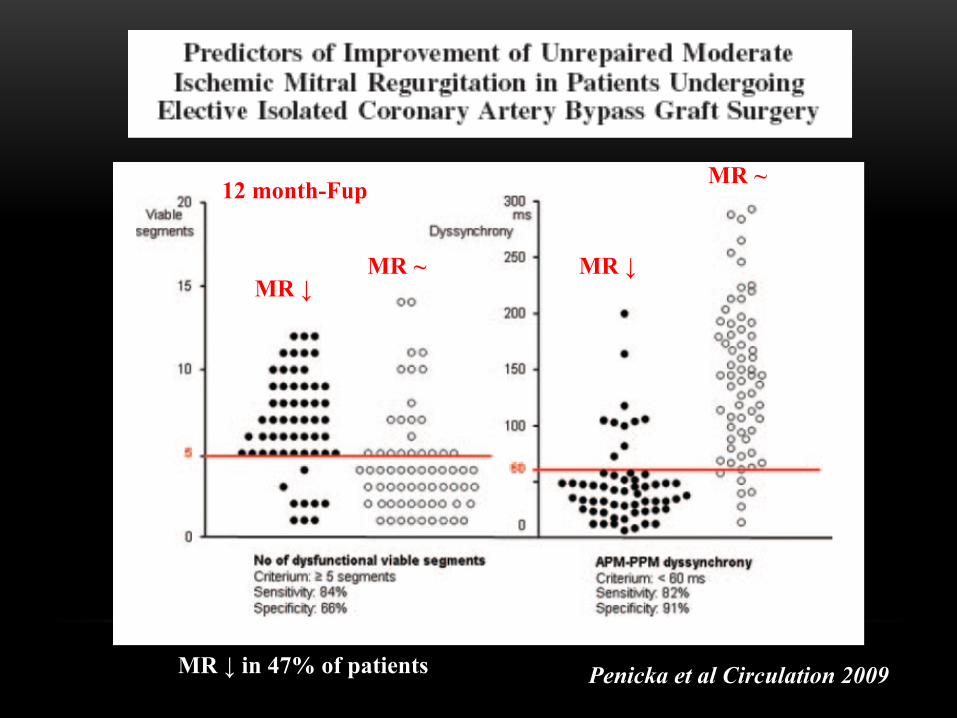
Penicka et al Circulation 2009MR ↓ in 47% of patients
MR ↓MR ↓MR ~
MR ~12 month-Fup
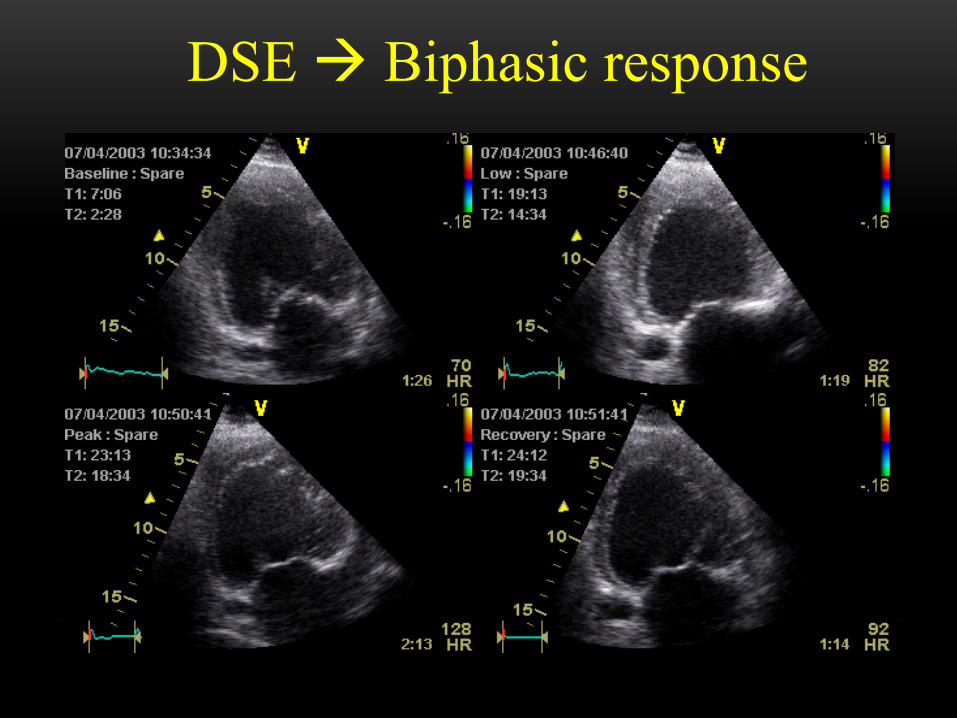
DSE Biphasic response
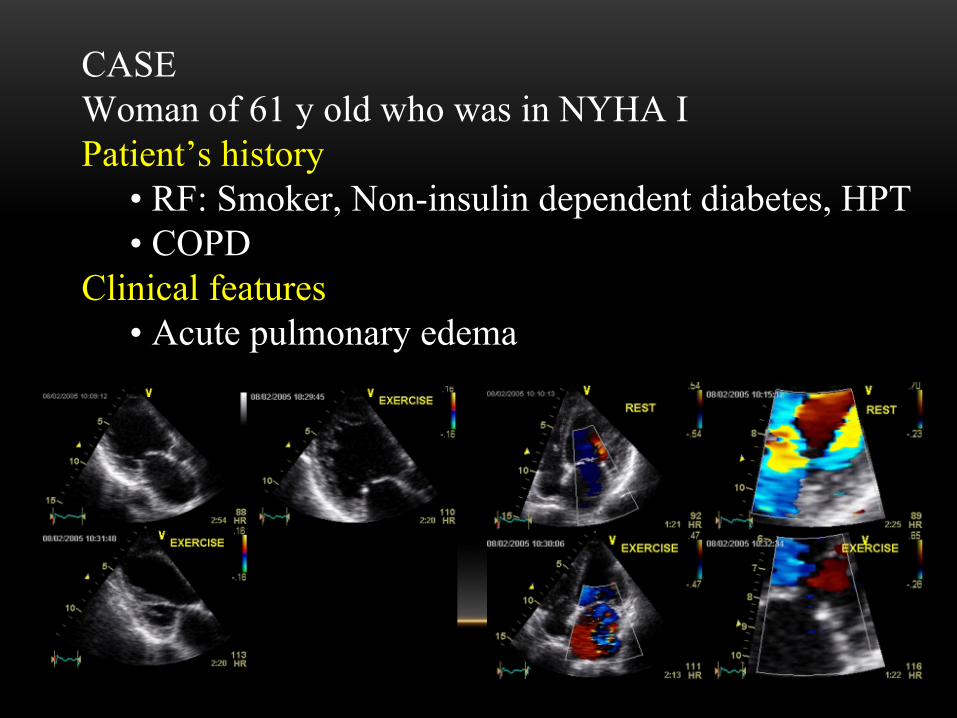
CASEWoman of 61 y old who was in NYHA I Patient’s history
• RF: Smoker, Non-insulin dependent diabetes, HPT• COPD
Clinical features• Acute pulmonary edema
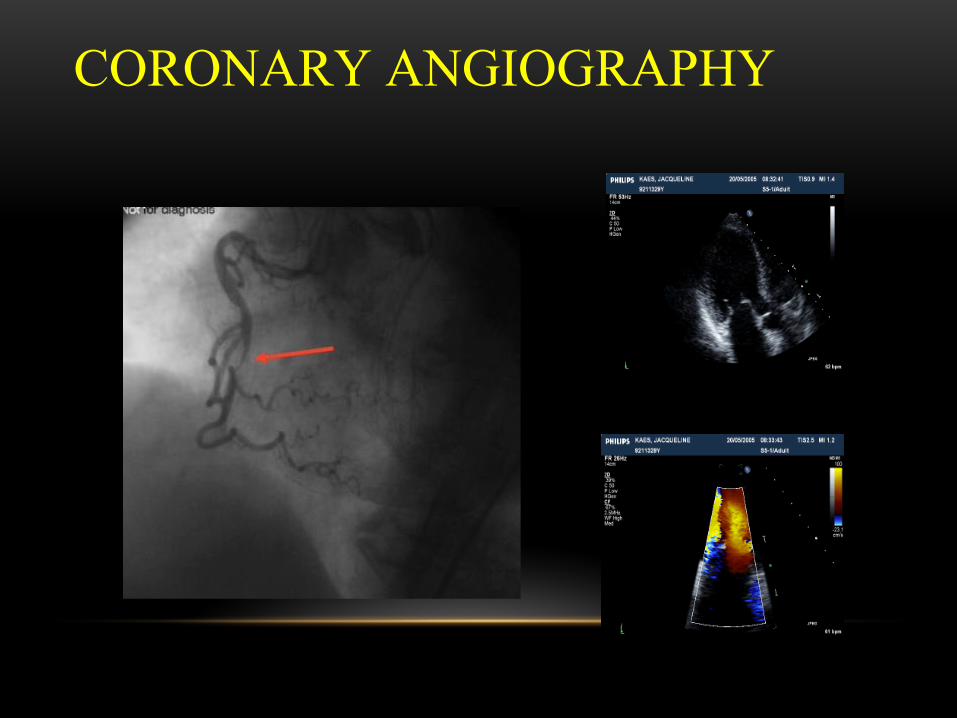
CORONARY ANGIOGRAPHY
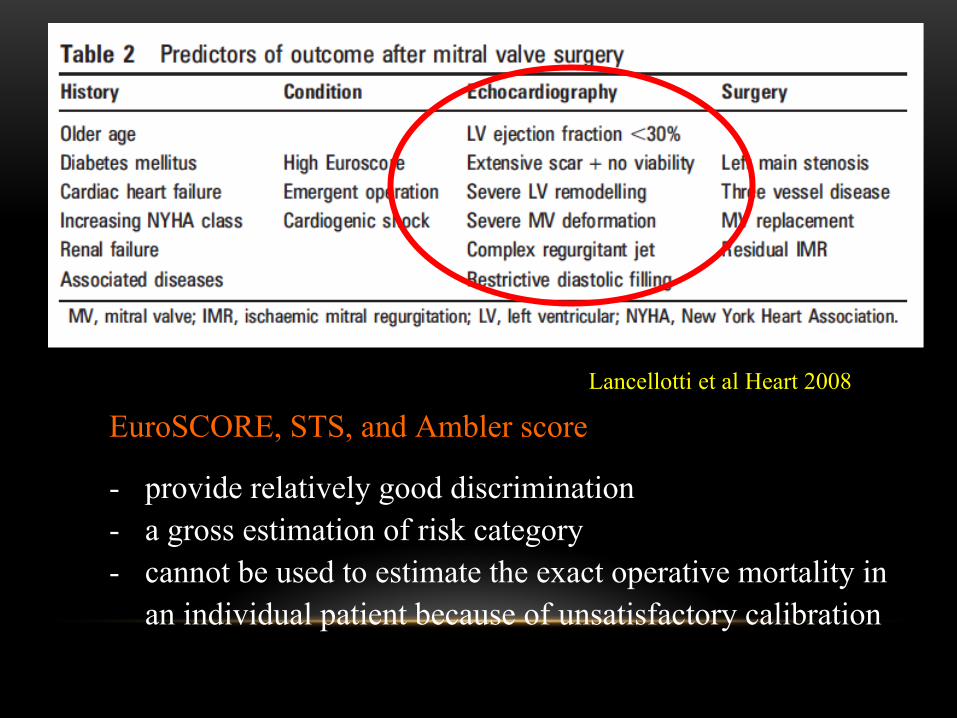
EuroSCORE, STS, and Ambler score
- provide relatively good discrimination- a gross estimation of risk category- cannot be used to estimate the exact operative mortality in
an individual patient because of unsatisfactory calibration
Lancellotti et al Heart 2008
Cas présentation NB: Non inidcation for revascOther case with option?RESTREST
EXERCISEEXERCISE
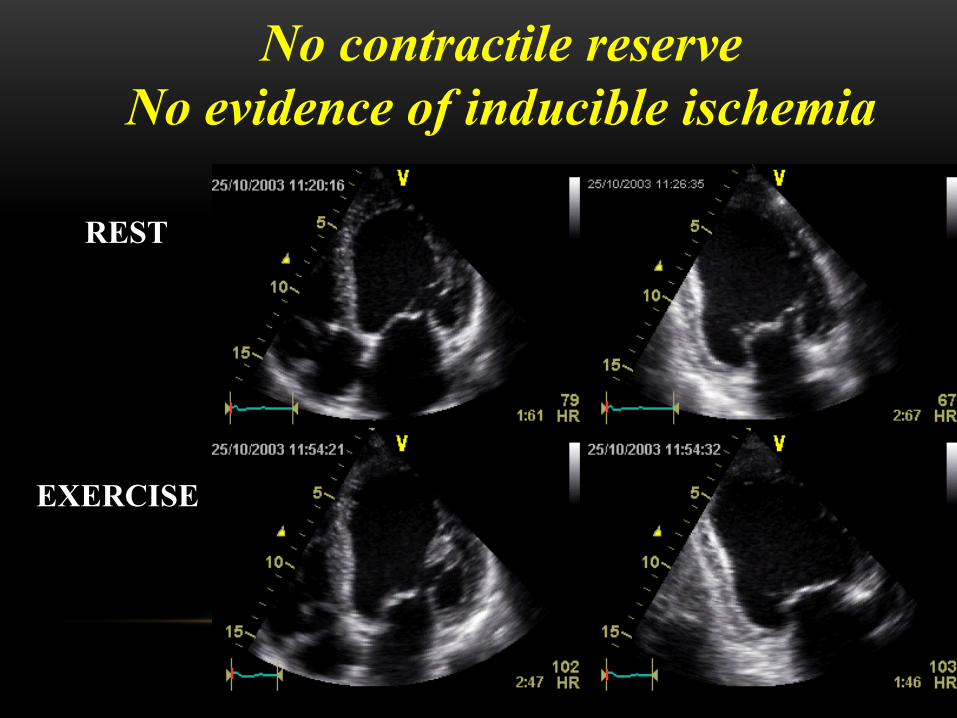
No contractile reserveNo evidence of inducible ischemia
Multimodality Imaging – Step 3
Assessing LV remodeling & MV deformation
- To predict risk of persistent / recurrent MR following MV annuloplasty
- To determine best option for MV intervention
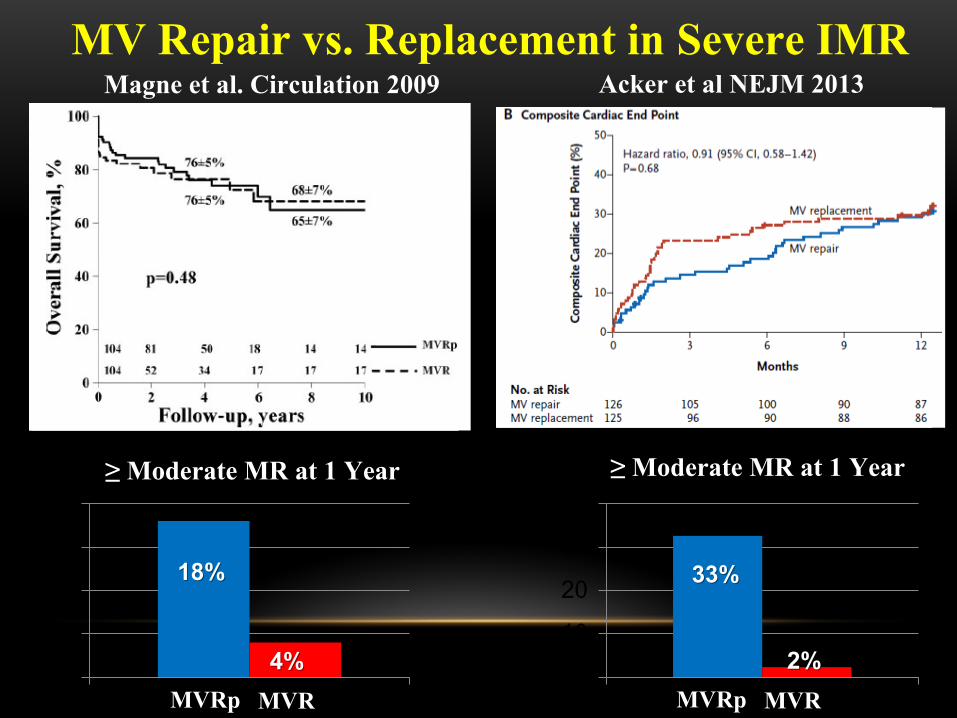
MV Repair vs. Replacement in Severe IMR
0
5
10
15
20≥ Moderate MR at 1 Year
18%18%
44%% 0
10
20
30
40≥ Moderate MR at 1 Year
33%33%
2%2%
Magne et al. Circulation 2009 Acker et al NEJM 2013
MVRp MVR MVRp MVR
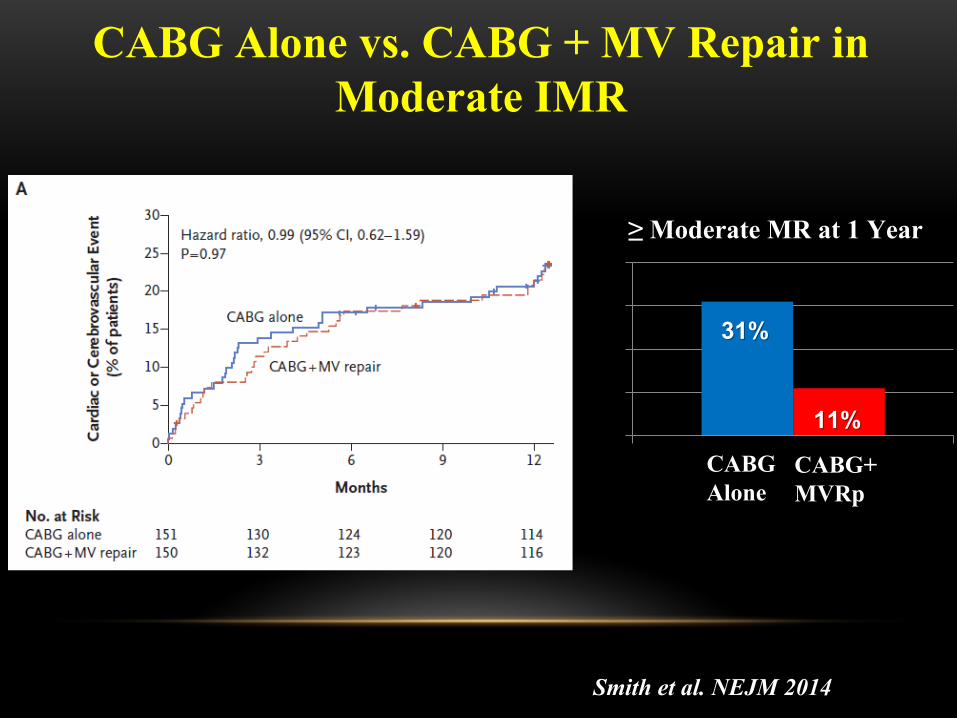
CABG Alone vs. CABG + MV Repair in Moderate IMR
0
10
20
30
40≥ Moderate MR at 1 Year
31%31%
11%11%
Smith et al. NEJM 2014
CABGAlone
CABG+MVRp
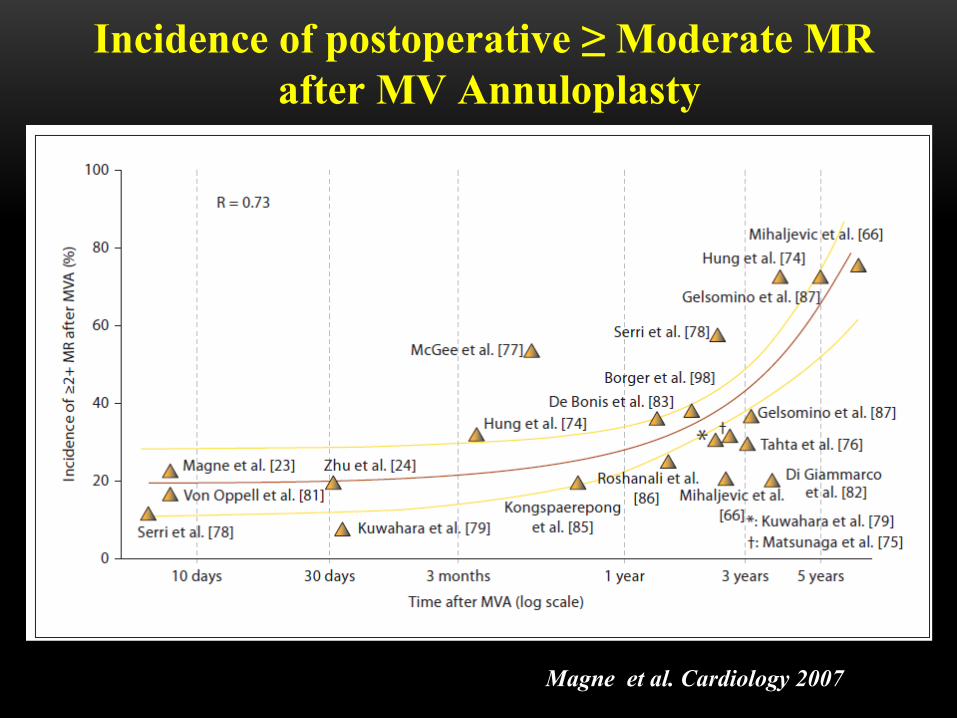
Incidence of postoperative ≥ Moderate MR after MV Annuloplasty
Magne et al. Cardiology 2007
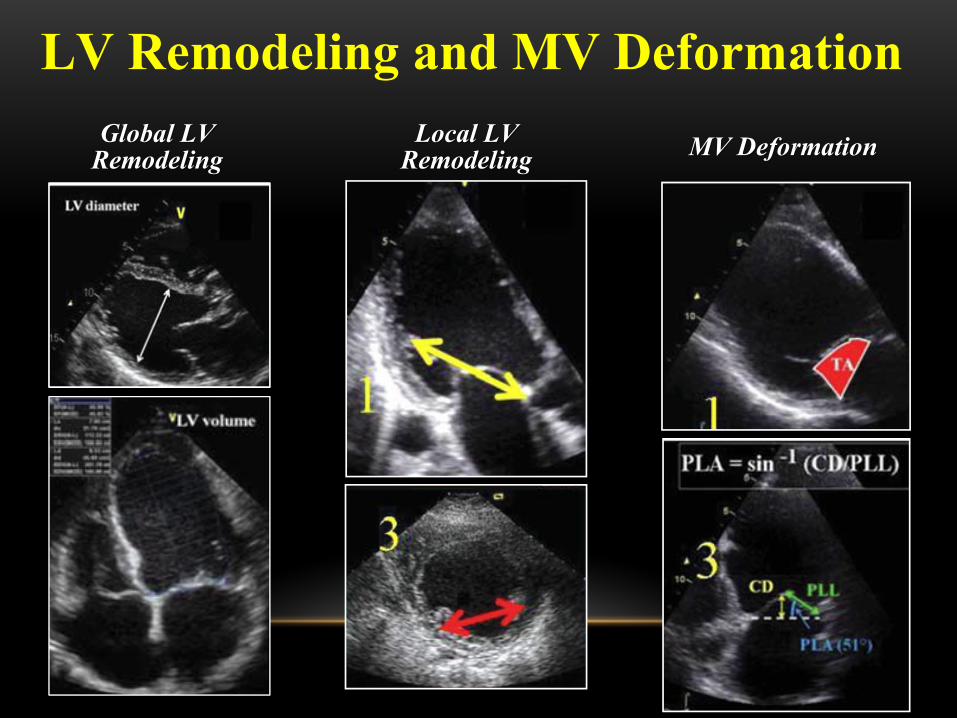
LV Remodeling and MV Deformation Global LV Global LV
RemodelingRemodelingLocal LV Local LV
RemodelingRemodeling MV DeformationMV Deformation
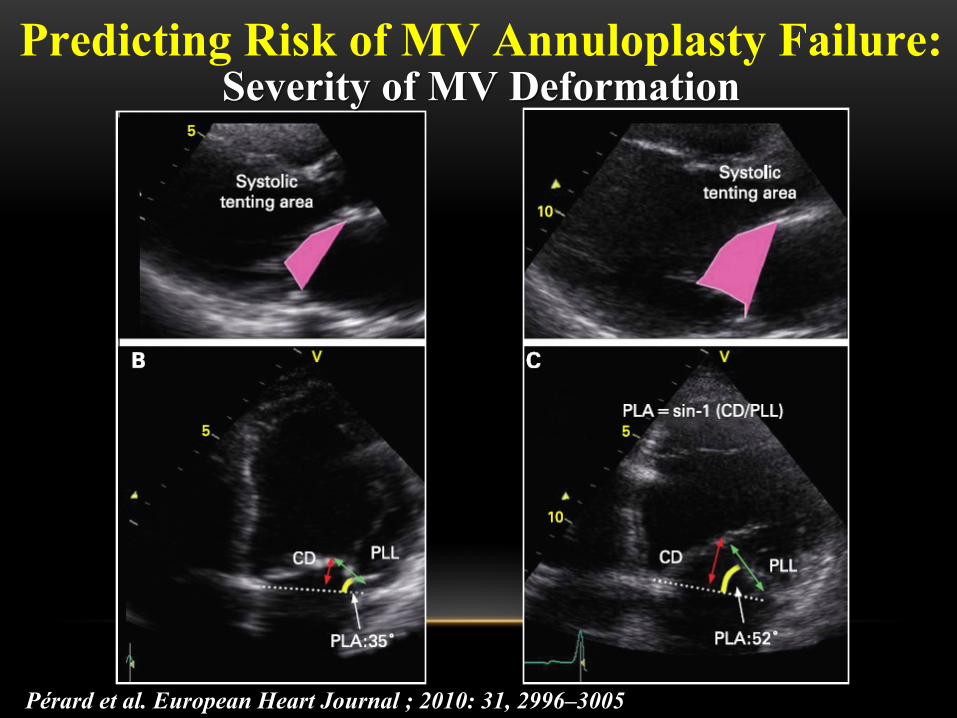
Predicting Risk of MV Annuloplasty Failure:Severity of MV DeformationSeverity of MV Deformation
Pérard et al. European Heart Journal ; 2010: 31, 2996–3005
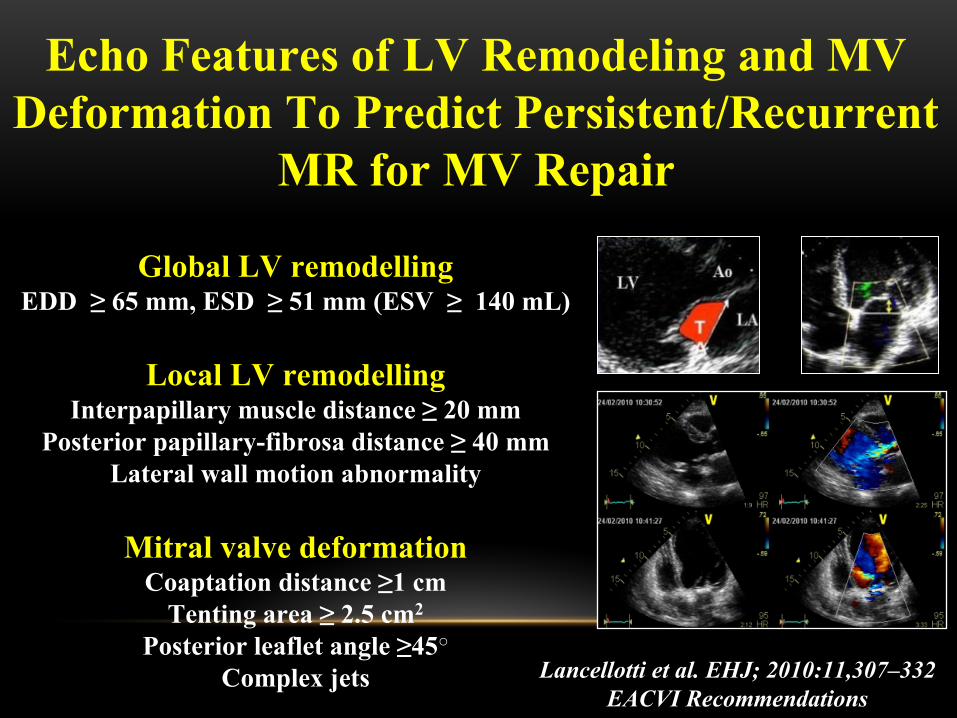
Global LV remodellingEDD ≥ 65 mm, ESD ≥ 51 mm (ESV ≥ 140 mL)
Local LV remodellingInterpapillary muscle distance ≥ 20 mm
Posterior papillary-fibrosa distance ≥ 40 mmLateral wall motion abnormality
Mitral valve deformationCoaptation distance ≥1 cm
Tenting area ≥ 2.5 cm2
Posterior leaflet angle ≥45○
Complex jets
Echo Features of LV Remodeling and MV Deformation To Predict Persistent/Recurrent
MR for MV Repair
Lancellotti et al. EHJ; 2010:11,307–332EACVI Recommendations
FUTURE PERSPECTIVES
Secondary MR is not ONLY a disease of the left ventricle!
It is ALSO a maladaptation of the MV leaflets
So look at the MV leaflet size
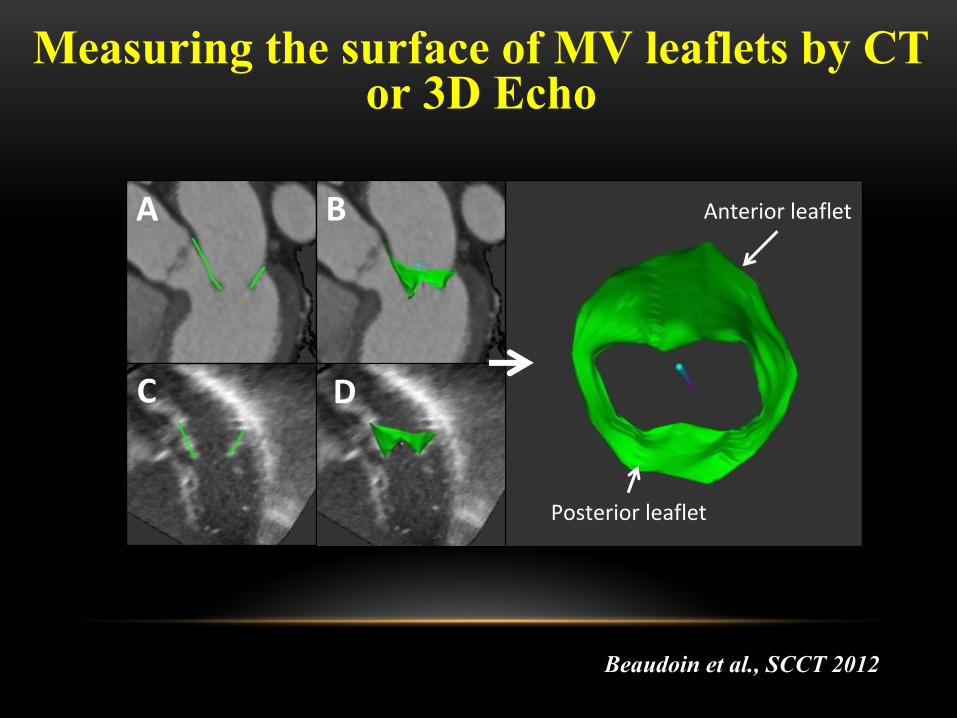
Beaudoin et al., SCCT 2012
Anterior leaflet
Posterior leaflet
F
A B
DC
Measuring the surface of MV leaflets by CT or 3D Echo
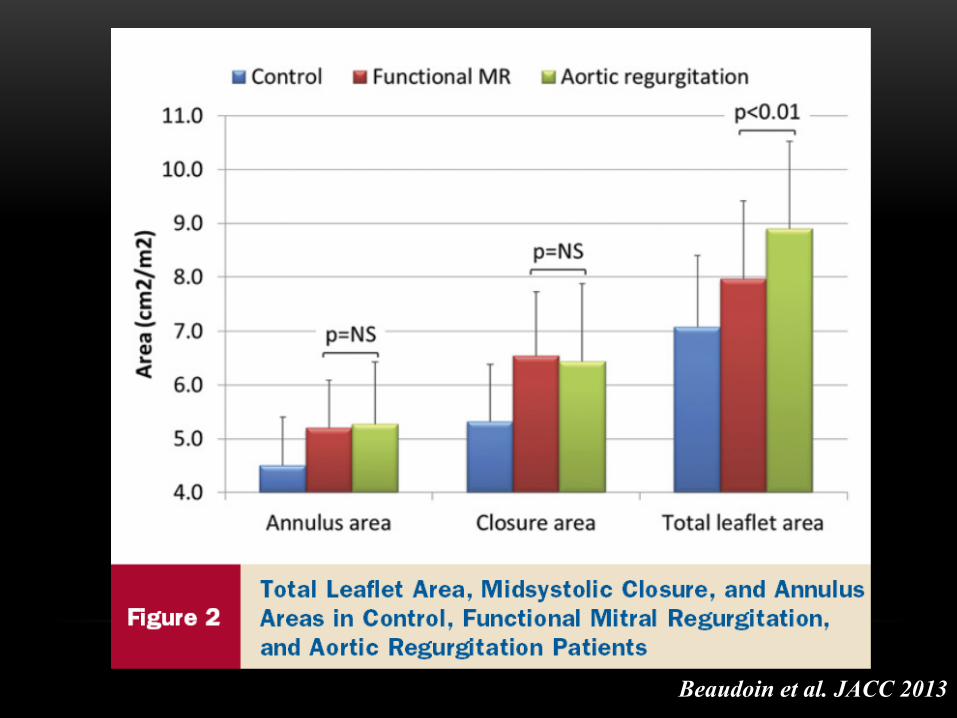
Beaudoin et al. JACC 2013
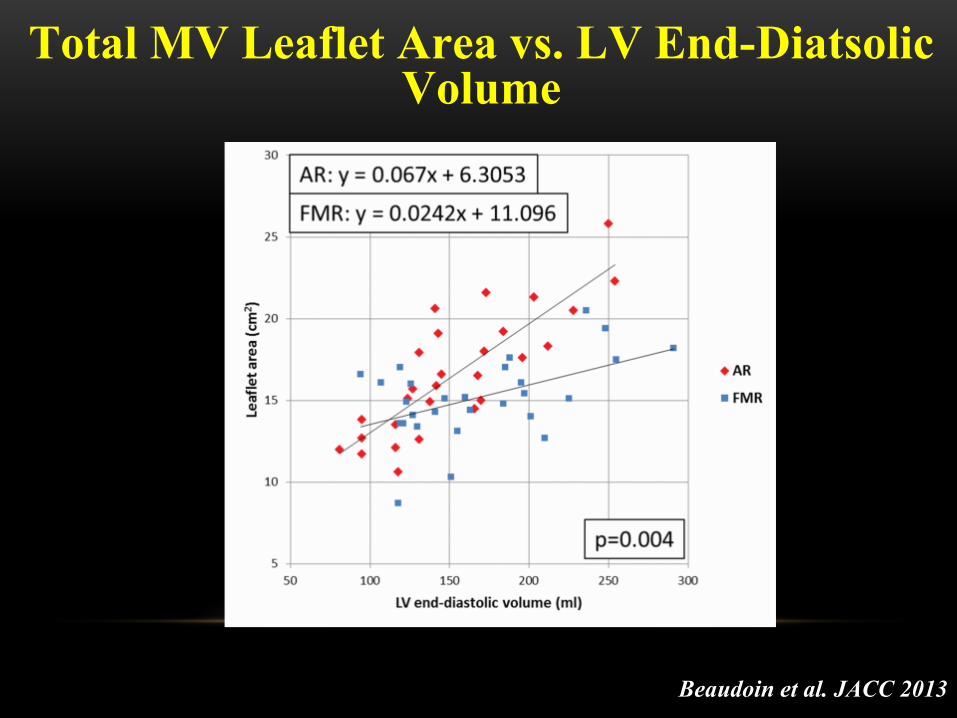
Beaudoin et al. JACC 2013
Total MV Leaflet Area vs. LV End-Diatsolic Volume
• Patients with secondary MR have inadequate leaflet compensation, as expressed by decreased ratios of leaflet area / annulus area
• Imaging will play a key role to understand why some patients have adequate vs inadequate valve adaptation
• Medications targeting the TGF-beta pathway may help to reduce the leaflet/annulus size mismatch and thus secondary MR in HF
Total MV Leaflet Area vs. LV End-Diatsolic Volume
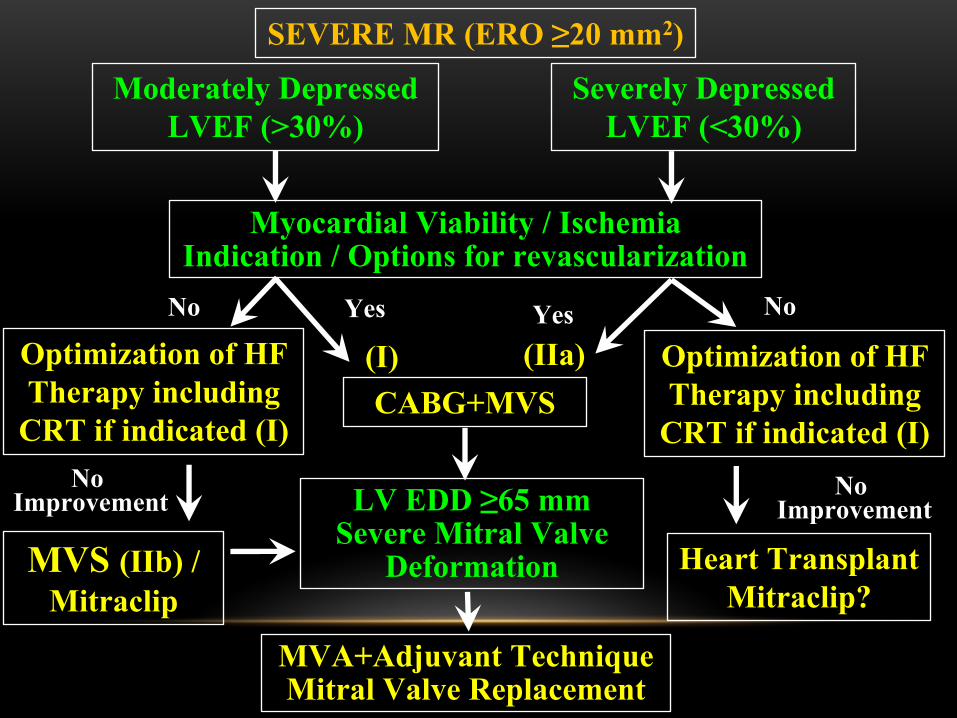
SEVERE MR (ERO ≥20 mm2)
LV EDD ≥65 mmSevere Mitral Valve
Deformation
CABG+MVS
MVA+Adjuvant TechniqueMitral Valve Replacement
Optimization of HF Therapy including
CRT if indicated (I)
Myocardial Viability / IschemiaIndication / Options for revascularization
Heart TransplantMitraclip?
MVS (IIb) /Mitraclip
Moderately Depressed LVEF (>30%)
Severely Depressed LVEF (<30%)
No Yes NoYes(IIa)(I) Optimization of HF
Therapy including CRT if indicated (I)
No Improvement
No Improvement
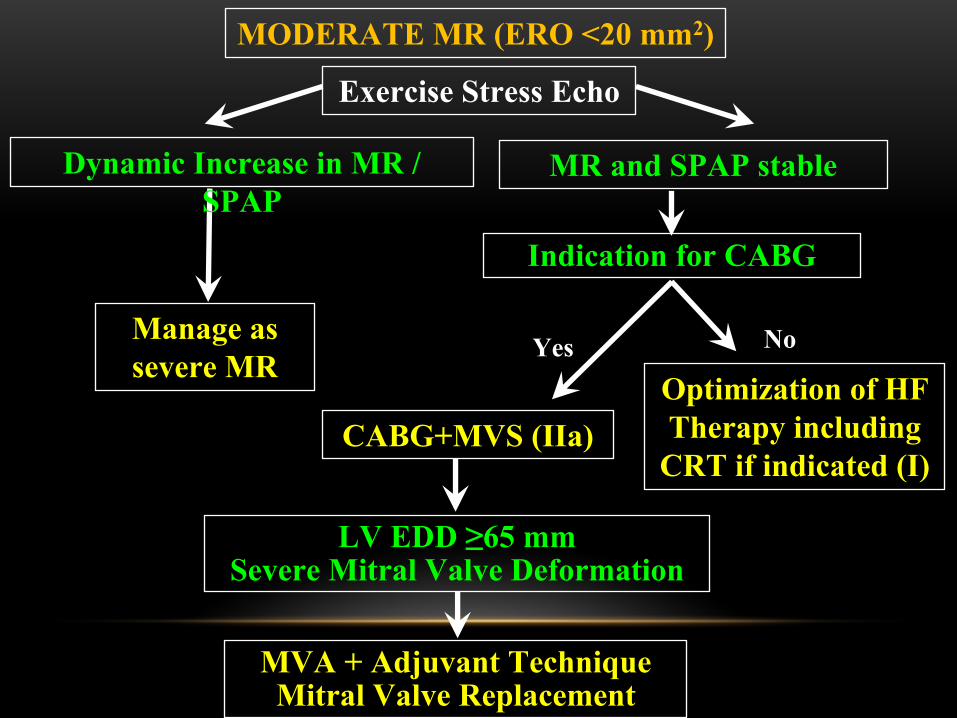
MODERATE MR (ERO <20 mm2)
LV EDD ≥65 mmSevere Mitral Valve Deformation
CABG+MVS (IIa)
MVA + Adjuvant TechniqueMitral Valve Replacement
Manage as severe MR
Indication for CABG
Dynamic Increase in MR / SPAP
NoYesOptimization of HF Therapy including
CRT if indicated (I)
MR and SPAP stable
Exercise Stress Echo