Embed Size (px)
DESCRIPTION
2014 POTA Conference Presentation Handout
Citation preview
Child Development, Reflex Retention
and the Impact on Learning
POTA ANNUAL CONFERENCE NOVEMBER 1, 2014
Presen ted by
Jenn i fe r Doy le , MA OTR/L & Karen Gua l t ie r i , MS OTR/L
Neurodevelopment
Learning Objectives
Develop a basic understanding of the progression of reflex activation and integration in typical development
Understand the role of movement and play on the developmental progression
Identify barriers that interfere with reflex integration
Identify the behavioral and sensory challenges of children with unintegrated reflex patterns across environments
Understand basic principles and techniques for identifying these children through direct testing and clinical observation
Learn simple, effective activities to implement into your practice
About Us
❖ Jennifer Doyle has been practicing occupational therapy
in pediatrics for 14 years. She is certified in Sensory Integration (SIPT) and Neurodevelopmental Treatment (NDT). She is also trained in The Listening Program, Therapeutic Listening, Rhythmic Movement Training Interactive Metronome, and has completed her Level 1 mentorship with Lucy Jane Miller.
❖ Karen Gualtieri has been practicing occupational therapy for 11 years with extensive training in sensory integration. Karen is DIR/Floortime trained. She also has certifications in The Listening Program, Advanced Therapeutic Listening, Rhythmic Movement Trainingand Handwriting Without Tears.
Developmental Milestones
➢Lifting head
➢Rolling
➢Crawling
➢Sitting unsupported
➢Pulling to stand
➢Cruising
➢Walking
Central Nervous System
• Consists of the brain and spinal
cord.
• In the first year, your baby’s brain
triples in weight.
• By the end of the second year, your
toddler’s brain weighs three
quarters that of an adult’s brain.
Central Nervous System
• Brain gets bigger=more activity.
• The metabolism of a baby’s brain,
(measured by how much blood
sugar it uses) increases steadily
until age 3.
• At age 3, a child’s brain is more
than twice as active as an adult’s
brain
Central Nervous System
• Most of the brain cells are developed in-utero.
• After birth, there is extensive branching through
axons and dendrites.
• Extensions allow for connection and
communication within the CNS
• Pruning of unused brain cells and connections is
equally important for specialization of brain areas
and efficiency of processing
• More connections=more able to process a variety
of sensory input
Central Nervous System
• Myelination begins before
birth and continues
throughout childhood.
• Myelin (fatty sheath) protects the growing
nerves and helps them communicate better by
increasing the rate at which impulses travel
within the system.
• The brain undertakes this task in stages and
may not be completed until age 10.
Environmental Changes Impacting Development
• Shift toward a more sedentary lifestyle
– Decreased recess and gym time due to budget cuts
– Decreased opportunity for outside play
• Electronic games and toys, television, video
games
– less movement during play
– instant gratification affecting coping skill development
• Back to sleep initiative leading to children
having less tummy time– Children are not spending enough time in antigravity positions to
properly elicit reflex patterns and/or integrate them
Environmental Changes Impacting Development
• Devices for propping baby or confining baby
(carseat carriers, bouncy saucers, jumpers, etc)
– Decreased opportunity for movement and
environmental exploration
– Decreased sensory information from the environment
Purpose of Primitive and Transitional
Reflexes
• The primitive reflexes develop at different
times provide movement patterns for baby’s
survival.
• As the baby’s central nervous system
becomes myelenated through antigravity
and core postural activation, these reflexes
become integrated and the child can move
within these patterns but also against these
patterns.
Purpose of Primitive and Transitional
Reflexes
• The reflexes allow a baby to move through
the birth canal (ATNR, STNR, Spinal
Galant, TLR), find food when the visual
system has not fully developed (rooting),
and begin to move his/her body against
gravity to roll, crawl and walk.
Reflexes and Early
Development
• Researchers have found differences in
reflexes and movement patterns in
children with autism as young as 3 months.
Infantile Reflexes Gone Astray in Autism, University of Florida, Departments of Psychiatry, Psychology and
Computer Science. Philip Teitelbaum (1), Osnat B. Teitelbaum (1), Joshua Fryman (2), and Ralph Maurer (3)
2004.
• They found a lack of head verticalization when the infant
was tilted to the left and right, with the head remaining in
midline instead of righting itself. This can persist into
grade school.
Reflexes and Early Development
• They also found atypical rolling in children
with a persistent ATNR later diagnosed with
Asperger’s Syndrome.
• When these children turned their head to
the left, their left arm extended (ATNR). The
rolled to the opposite side using extension
instead of flexion as is typical. They used
their extended arm as a leaver.
Biomarkers for Autism
Researchers from the Children’s National Health System have identified that head circumference and head tilting reflex are reliable biomarkers for autism between 9 and 12 months of age.
1000 subjects. 49 with abnormal results.
15 at risk for ASD, 34 at risk for developmental language delay.
14/15 children at risk for ASD eventually sustained the diagnosis.
C.A. Samango-Sprouse, E.J. Stapleton, F. Alibadi, R. Graw, R. Vickers, K. Haskell, T. Sadeghin, R.
Jameson, C.L. Parmele, A.L. Gropman. Idenitification of infants at risk for autism spectrum disorder and
developmental language delay prior to 12 months. Autism, 2014
Moro Reflex
• The “startle reflex”
• Elicited by posterior loss of
support
• Usually present until 4 or 5
months of age
• Has 2 distinct phases
– 1st phase: Abduction of
arms and extension of
neck
– 2nd phase: adduction of
arms and flexion of trunk
Moro Reflex
• If this reflex is unintegrated, the child can
have difficulty with self-soothing and may be
frequently anxious and on ‘high alert’
• Functions as an alarm, and overstimulates
“flight or flight”.
• When overstimulated, hypersensitivity can
develop in sensory systems especially in
the visual, auditory, and tactile systems
(specifically light touch and vibration).
Moro Reflex
• Integrated response: Person is able to clasp
hands quickly and without emotional
response.
• Retained reactions include: delay in
reaction, incomplete arm movement, breath
holding, skin changes, leg extension or
arms away from chest.
Tonic Labyrinthine Reflex
• A primitive reflex which is present at birth and
integrated by 6 months of age
• (prone) When the head is tipped back the body
goes into extension and (supine) when the bends
forward, the body goes into flexion
• This reflex helps the baby move through the birth
canal.
Tonic Labyrinthine Reflex• Provides opportunity for head alignment and eye
pairing for the foundation for bilateral
coordination and posture
• In typically developing children, eyes converge
when head tilts forward and eyes diverge when
neck is extended.
• Low muscle tone and slouched
posture may result when
unintegrated.
• Fear of heights is also common.
Tonic Labyrinthine Reflex
• Integrated response: Body remains relaxed
and does not move.
• Retained reactions include changes in
muscle tone in legs, loss of balance,
nausea, dizziness, changes in skin color or
changes in breathing.
Landau
• This reflex emerges at 3 months of age (transitional reflex)
and is integrated by 12 months
• Characterized by extension or arching of the back when
the infant is placed in the horizontal plane
• If this reflex does not develop, this can be an indication of
a motor development issue. If not integrated, movements
can be stiff, in lower body with challenges in hopping and
jumping.
Landau
• Retained reactions include involuntary
movement of the feet and legs off the floor,
extensor tone throughout body.
• When integrated, you should be able to move
in and out of this position without difficulty
and without affecting your ability to learn
move movements.
Asymmetrical Tonic Neck Reflex
• This reflex is present at birth and
is usually integrated by 6 months
of age
• When the infant turns her head,
the arm and leg on the side the
head is turned to extend and the
opposite side bends
• This reflex is also known as the
fencing reflex
• If this reflex is not integrated,
difficulties arise with crossing
midline and using hands together.
Effects of Retained ATNR
Problems with handwriting
Difficulties with reading
Mixed laterality
Difficulty or inability to cross midline
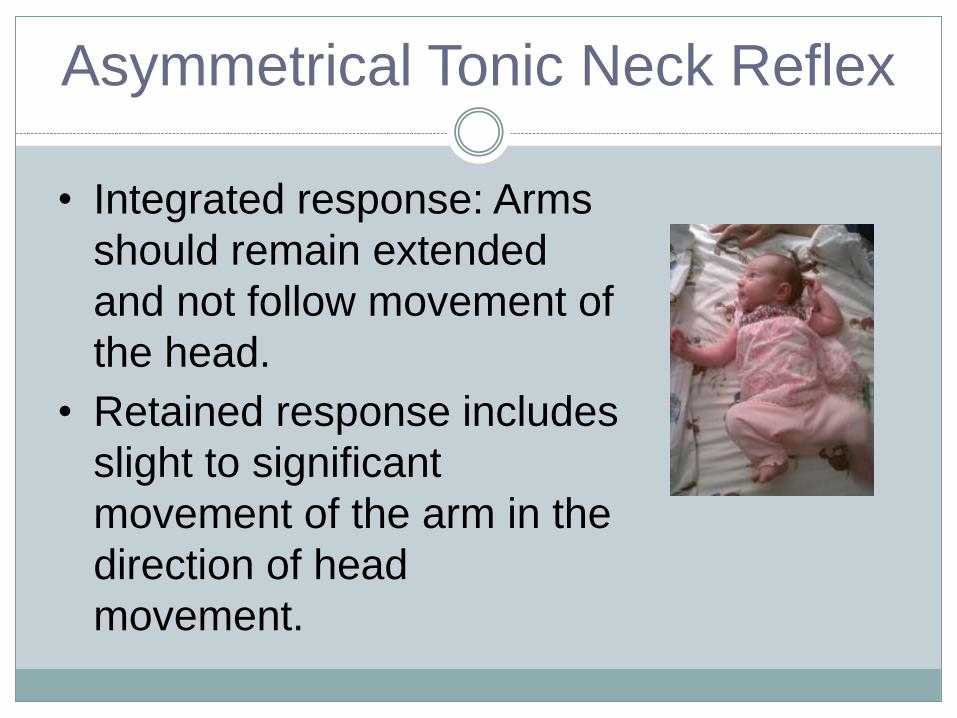
Asymmetrical Tonic Neck Reflex
• Integrated response: Arms
should remain extended
and not follow movement of
the head.
• Retained response includes
slight to significant
movement of the arm in the
direction of head
movement.
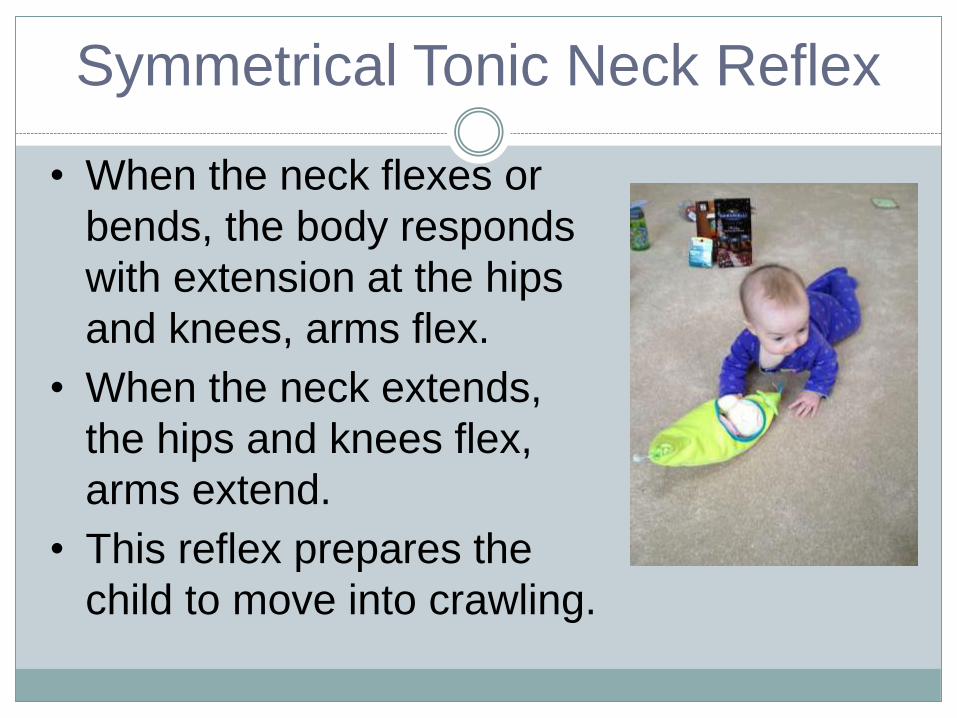
Symmetrical Tonic Neck Reflex
• When the neck flexes or
bends, the body responds
with extension at the hips
and knees, arms flex.
• When the neck extends,
the hips and knees flex,
arms extend.
• This reflex prepares the
child to move into crawling.
Symmetrical Tonic Neck Reflex
• When this reflex is not integrated, the child typically crawls late, does ‘bunny hop’ crawl, or does not crawl at all.
• Balance may challenging.
• This reflex is clearly observed in children
with significant neurological issues, such as
cerebral palsy.
Effects of retained STNR
Poor posture
Poor hand-eye coordination
Messy eating
Poor copying from blackboard
Child tends to be farsighted with poor visual accommodation
Symmetrical Tonic Neck Reflex
• Integrated response: Body should remain in
position as head moves.
• Retained response includes hip movement,
bending of arms, arching of back, moving
into cat sit position, difficulty moving head
and breathing/pallor changes.
Spinal Galant Reflex
• This reflex is elicited by touching sides of
the spine. It helps the baby move through
the birth canal and begin to move from
their tummy.
• It is present at birth and integrated
between 3 and 9 months.
• The body will respond by rotating the hip
and flexing toward and on the side of the
touch.
Spinal Galant Reflex
• Lack of integration can result in fatigue,
bedwetting, hyperactivity and attention
difficulties.
• It can make sitting still very difficult.
• Children may also develop sensitivity to
waist bands that presents as tactile
hypersensitivity.
Spinal Galant Reflex
• Integrated response: No movement of the
back with touch.
• Retained response includes movement of
the hip towards the stimulation.
Signs of Reflex Retention
• The person should be able to move with the reflexive
pattern but also move against the reflexive movement
pattern without significant effort
• Behavioral Signs
– Trouble staying seated in chair; falls out of chair
– Difficulty with fluidity between eye convergence and
divergence such as copying from the board
– Difficulty with attention, focus, and concentration
– Low tone, clumsiness
Case Study: Eli
Background information
∗Eli is an 11 year old boy with a diagnosis of
cerebral palsy. Increased tone on the right
compared to the left side.
∗He has difficulty with balance and
coordination and often falls. Wears AFOs all
of the time
∗Has difficulties with peer interaction at
school, participation in school activities and
completion of assignments (has a 1:1 aide all
day at school).
Case Study: Eli (cont.)
Strengths
∗Desires peer interaction
∗Enjoys coming to therapy and
wants to participate
∗Reports enjoying school
∗Loves his iPad and has an
interest in cell phones and
computers
Challenges
∗Poor communication skills
∗Poor balance/ clumsy -
needs close supervision or
contact guard assist to
navigate environment
∗Shallow breath which affects
arousal level and speech
quality
∗Poor bilateral coordination
due to spasticity
Previous Interventions Trialed
with Eli∗ Behavioral approaches
∗ Occupational Therapy in the school setting – focused on
remediation of fine motor deficits and classroom
accommodations
∗ Interactive Metronome – Eli’s mother originally sought out
our clinic for IM Home. Eli was unable to focus and
participate for a long enough duration for significant change
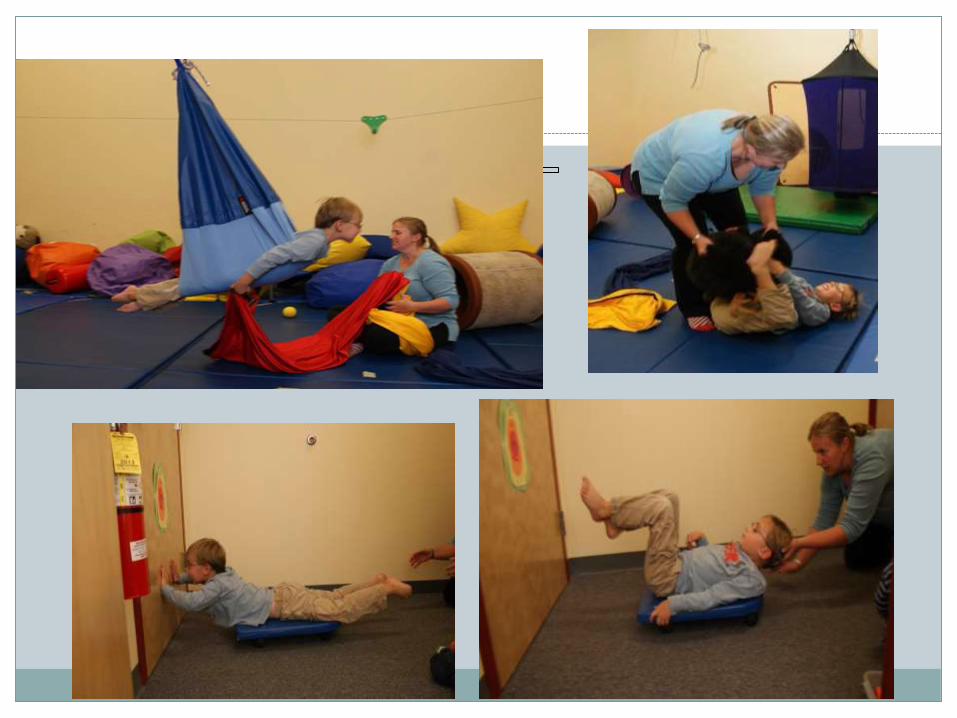
Eli’s Treatment Progression
Integration of Moro Reflex
∗Breath activities
∗ Bubbles/ bubbles with straw/ bubble bowls
∗ Whistles/ pinwheeels
∗Supine Flexion activities
∗ Pillow pull
∗ Egg rock
∗ Tear drop swing
∗Prone Extension activities – balance tone and work on
bilateral coordination/ symmetrical movement patterns
∗ Prone extension in hammock swing with upper extremity pull
∗ Scooterboard wall push offs
Eli’s Treatment Progression
(cont.)∗ Cross- lateral movement patterns (ATNR and STNR integration)
∗ Crawling through resistive tunnel
∗ Resistive crawling
∗ Interactive Metronome was revisited after 6 months of clinic based
sensory integrative treatment. Eli was able to participate in the
program. Eli continued with clinic based treatment for an additional 6
months with a frequency every other week and participated in the IM-
Home program.
∗ A home exercise/ activity program was established for home and was
completed on a daily basis
∗ Eli participated in Therapeutic Listening during treatment sessions at
the clinic
A Case Study…Sherri
Sherri is a 7 year old adopted girl who comes to our clinic for occupational therapy services.
She has a diagnosis of an immature bladder with a history of toileting accidents…this is a main concern for mom as she feels it affects Sherri’s function in all areas of Sherri’s life.
Areas of Weakness How does it Affect Function?
Low muscle tone in upper and lower extremities
Low-average strength in hands, arms and trunk
Postural reactions and postural control below average
Distracted by visual input in her environment
Trouble processing sensory information visually and auditorIly
Poor hand writing
Trouble using hands together
Falls out of chair
Trouble getting dressed
Falls and or trips with movement
Frequently is incontinent of urine
Physical Observations …
Treatment approaches trialed by Family Biofeedback at a Hospital in Philadelphia (Family
was told Sherri was not a good candidate due to limited attention)
Potty watch ( used at school and home; watch has a timer so Sherri has a reminder to empty her bladder)
Extracurricular activities for upper, lower body and core strengthening (Yoga, Gymnastics, Jazz & Soccer)
Reflexes Tested
Spinal Galant…Sherri tested positive when swiped on right and left sides of her spine
ATNR…Sherri unable to keep elbows straight when head was turned
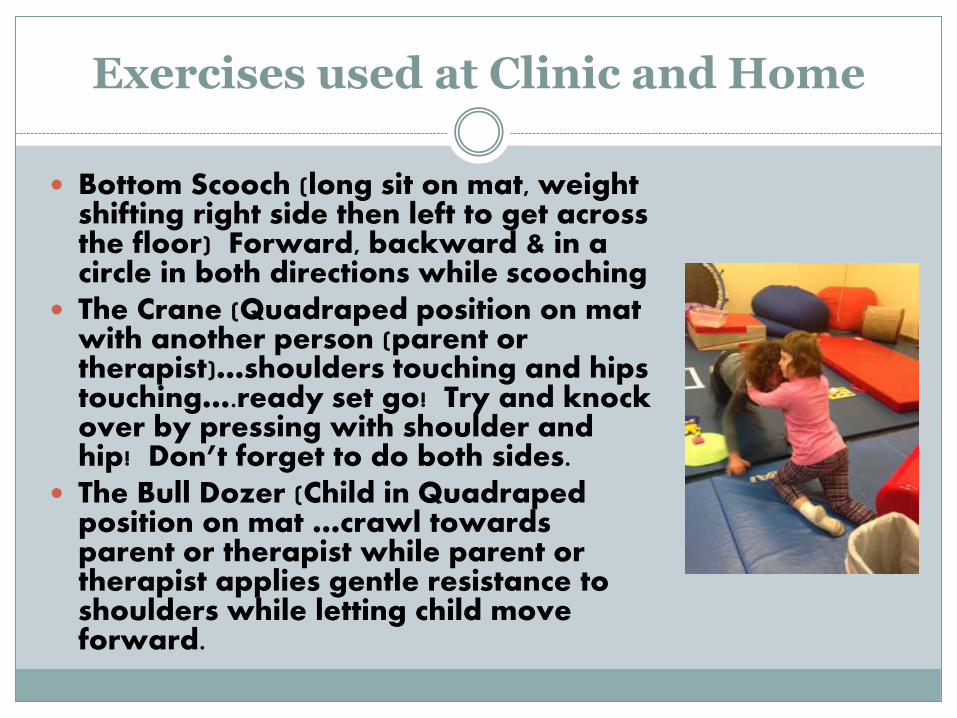
Exercises used at Clinic and Home
Bottom Scooch (long sit on mat, weight shifting right side then left to get across the floor) Forward, backward & in a circle in both directions while scooching
The Crane (Quadraped position on mat with another person (parent or therapist)…shoulders touching and hips touching….ready set go! Try and knock over by pressing with shoulder and hip! Don’t forget to do both sides.
The Bull Dozer (Child in Quadrapedposition on mat …crawl towards parent or therapist while parent or therapist applies gentle resistance to shoulders while letting child move forward.
Speed Bump….. Back on Track!
Sherri’s mom fell during the winter and hurt her wrist…
Mom stopped doing the exercises at home
AS A RESULT… Sherri had an increase in
incontinence at school and home
Sherri started using Potty watch again
Sherri’s mom resumed exercises
Sherri’s incontinence decreased
Potty watch…Sherri no longer wears it
Sherri is more functional in her everyday life!
Sherri’s Progress when Exercises done at home and in clinic

Intervention Strategies
Posture and Respiration
“If you can’t breath, you can’t function”
● Proper postural alignment allows for optimal diaphragmatic excursion
● Movement through developmental (antigravity) movement patterns allows for mature spinal curves to develop full excursion of the diaphragm
● Control over respiration allows for regulation of basal levels and affects arousal level
Rhythmic Movement
• The cerebellum is the brain structure
responsible for providing timing and grading
of movements for efficient and accurate
motor output.
Rhythm and Timing
• Underlying theory: Neural timing is important to efficient processing of sensory input. Rhythm and timing are important for development of motor planning, language, academic skills.
Rhythm and Timing
o Developing rhythm and timing with music and movement
o Using metronome app during treatment/in home programs and having the child tap to the beat, tap on a ball, use rhythm sticks, jump to the beat, bounce a ball to the beat.
o Using music with a strong beat or a metronome set at 60 (heartbeat) to help regulation. Can be used in home programs.
o Using rhythm as an important part of movement to help children develop regulation.
o Humming, singing and using kazoos to incorporate voice to the beat
Resistive Movement
• Grade difficulty of exercise• Increase proprioceptive input for increased body
awareness
• Obtain desired response especially when
trying to elicit flexion with rolling (instead of
extension)
• Provide sensory regulation by slowing
movement down
References and Additional Reading
Ayres, A. J., PhD. (2005). Sensory Processing and the Child: 25th Anniversary Edition. Los Angeles, CA.
• Bloomburg, H. & Dempsey, M., (2011) Movements that Heal: Rhythmic Movement Training and Primitive Reflex Integration.
Blyth, S. G. (2004). The Well Balanced Child: Movement and Early Learning. Stroud, Gloucestershire.
• “Building Blocks for Sensory Integration”, (2012). Continuing education course taught by Sheila Frick, OTR. Westfield, NJ.
Frick, S., OTR and Young, S., PhD (2012). Therapeutic Listening: Listening with the Whole Body. Vital Links. Madison, WI.
Goddard, S., (2002).Reflexes, Learning and Behavior: A Window into the Child’s Mind.Fern Ridge Press, Eugene, Oregon.
W E B S I T E :
W W W . B E T H L E H E M P E D I A T R I C . C O M
L I K E U S O N F A C E B O O K
E M A I L
J E N @ B E T H L E H E M P E D I A T R I C . C O M
K A R E N G @ B E T H L E H E M P E D I A T R I C . C O M
( 6 1 0 ) 6 2 5 - 4 4 0 4
3 0 1 2 E M R I C K B L V D .
B E T H L E H E M , P A 1 8 0 2 0
Questions?





























