Embed Size (px)
Citation preview
16-‐02-‐15
1
Computerised Decision Support for Chronic Disease Management
Niels Peek
Health e-Research Centre Farr Institute for Health Informatics Research
The University of Manchester
11th February 2015 Digital Health Assembly, Cardiff, UK
1. Computerised decision support: An ultrabrief history
2. What types of systems exist? Are they effective?
3. CDS for chronic disease management
4. Example: PANDIT
5. Challenges for the future
6. Conclusion
Menu
• The first RCT was published in 1948.
• Currently, ± 5000 biomedical research articles are published daily, including 75 randomised clinical trials
• The biomedical literature doubles every 19 years
• Doctors would have to read 20 scientific papers a day, on average, to maintain their knowledge 1
1 Shaneyfelt T. Building bridges to quality. JAMA 2001; 286: 2600–1.
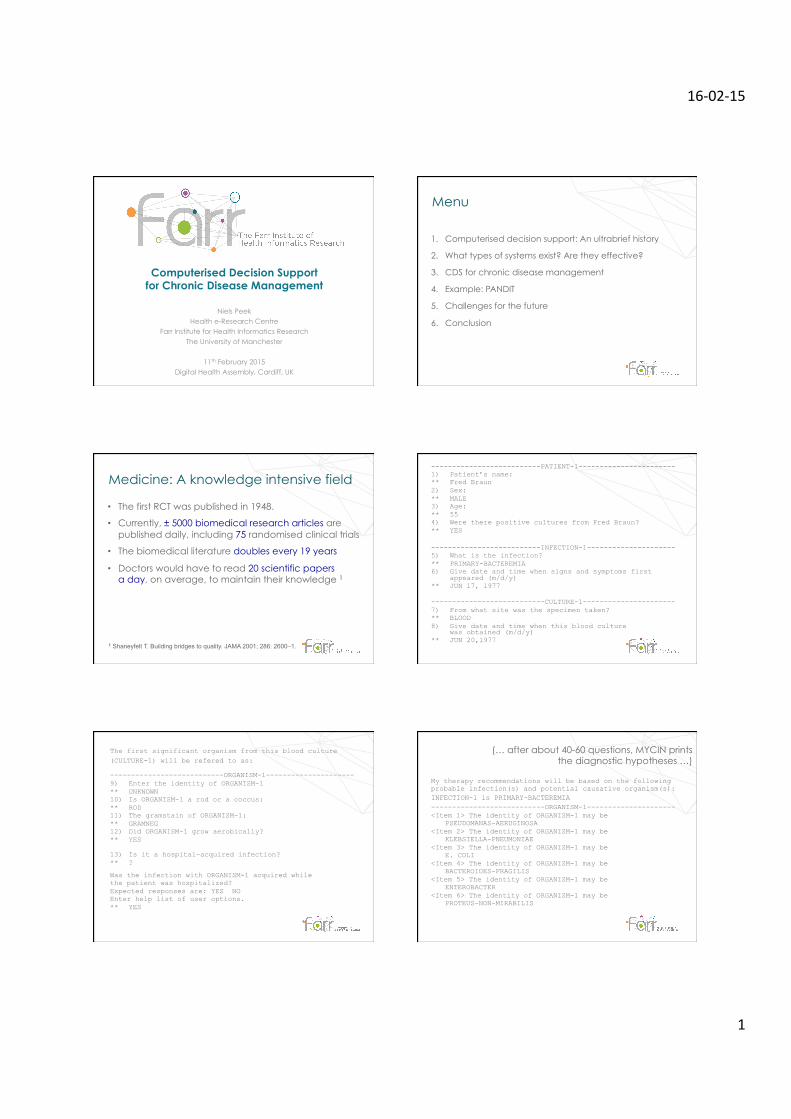
Medicine: A knowledge intensive field --------------------------PATIENT-1----------------------- 1) Patient’s name: ** Fred Braun 2) Sex: ** MALE 3) Age: ** 55 4) Were there positive cultures from Fred Braun? ** YES --------------------------INFECTION-1--------------------- 5) What is the infection? ** PRIMARY-BACTEREMIA 6) Give date and time when signs and symptoms first
appeared (m/d/y) ** JUN 17, 1977 ---------------------------CULTURE-1---------------------- 7) From what site was the specimen taken? ** BLOOD 8) Give date and time when this blood culture
was obtained (m/d/y) ** JUN 20,1977
The first significant organism from this blood culture (CULTURE-1) will be refered to as:
---------------------------ORGANISM-1--------------------- 9) Enter the identity of ORGANISM-1 ** UNKNOWN 10) Is ORGANISM-1 a rod or a coccus: ** ROD 11) The gramstain of ORGANISM-1: ** GRAMNEG 12) Did ORGANISM-1 grow aerobically? ** YES 13) Is it a hospital-acquired infection? ** ?
Was the infection with ORGANISM-1 acquired while the patient was hospitalized? Expected responses are: YES NO Enter help list of user options. ** YES
(… after about 40-60 questions, MYCIN prints the diagnostic hypotheses …)
My therapy recommendations will be based on the following probable infection(s) and potential causative organism(s): INFECTION-1 is PRIMARY-BACTEREMIA ---------------------------ORGANISM-1--------------------- <Item 1> The identity of ORGANISM-1 may be
PSEUDOMANAS-AERUGINOSA <Item 2> The identity of ORGANISM-1 may be
KLEBSIELLA-PNEUMONIAE <Item 3> The identity of ORGANISM-1 may be
E. COLI <Item 4> The identity of ORGANISM-1 may be
BACTEROIDES-FRAGILIS <Item 5> The identity of ORGANISM-1 may be
ENTEROBACTER <Item 6> The identity of ORGANISM-1 may be
PROTEUS-NON-MIRABILIS
16-‐02-‐15
2
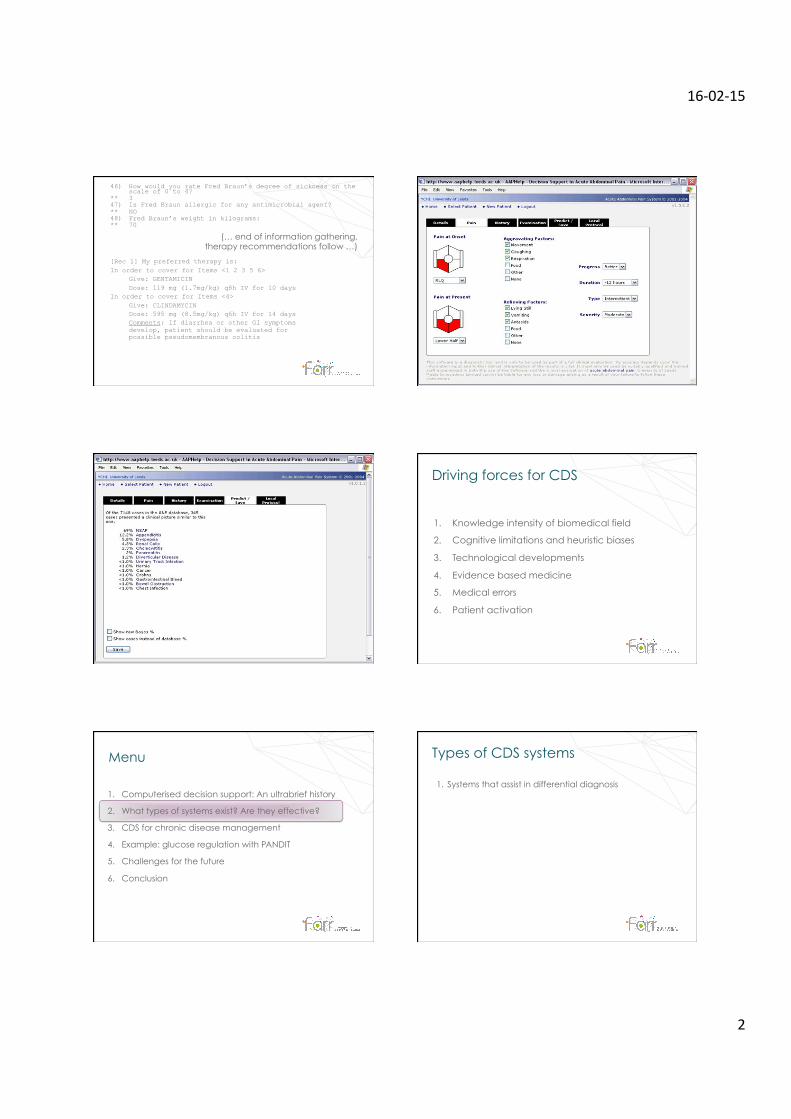
46) How would you rate Fred Braun’s degree of sickness on the scale of 0 to 4?
** 3 47) Is Fred Braun allergic for any antimicrobial agent? ** NO 48) Fred Braun’s weight in kilograms: ** 70
(… end of information gathering, therapy recommendations follow …)
[Rec 1] My preferred therapy is: In order to cover for Items <1 2 3 5 6>
Give: GENTAMICIN Dose: 119 mg (1.7mg/kg) q8h IV for 10 days
In order to cover for Items <4> Give: CLINDAMYCIN Dose: 595 mg (8.5mg/kg) q6h IV for 14 days Comments: If diarrhea or other GI symptoms develop, patient should be evaluated for possible pseudomembranous colitis
1. Knowledge intensity of biomedical field
2. Cognitive limitations and heuristic biases
3. Technological developments
4. Evidence based medicine
5. Medical errors
6. Patient activation
Driving forces for CDS
1. Computerised decision support: An ultrabrief history
2. What types of systems exist? Are they effective?
3. CDS for chronic disease management
4. Example: glucose regulation with PANDIT
5. Challenges for the future
6. Conclusion
Menu
1. Systems that assist in differential diagnosis
Types of CDS systems
16-‐02-‐15
3
1. Context-sensitive retrieval of knowledge sources (“infobuttons”)
2. Patient-specific recommendations for direct action (e.g. alerts, reminders)
3. Systems that group information: dashboards, order sets
4. Risk assessment tools
5. Patient decision aids
Types of CDS systems
1. Systems that assist in differential diagnosis
2. Patient-specific recommendations for direct action (e.g. alerts, reminders)
Types of CDS systems
401
12.3.5 Integrated Communication and Reporting Support
Increasingly, the delivery of patient care requires multiple health care professionals and may cross many organizations; thus, the effectiveness, effi -ciency, and timeliness of communication among such team members and organizations are increasingly important. Such communications usually focus on a single patient and may require a care provider to read content from his or her local EHR or from an external clinical system or to send information from his system to an exter-nal system. Therefore, communication tools should be an integrated part of the EHR system.
Ideally providers’ offi ces, the hospital, and the emergency room should all be linked
together—not a technical challenge with today’s Internet, but still an administrative challenge due to organizational barriers. Connectivity to the patient’s home will be increasingly impor-tant to patient- provider communication: for delivery of reminders directly to patients (Sherifali et al. 2011 ), and for home health mon-itoring, such as home blood pressure (Earle 2011 ; Green et al. 2008 ), and glucose monitor-ing. The patient’s personal health record (PHR) will also become an important destination for clinical messages and test results (see Chap. 17 ). Relevant information can be “pushed” to the user via e-mail or pager services (Major et al. 2002 ; Poon et al. 2002 ) or “pulled” by users on demand during their routine interactions with the computer.
a
b
Fig. 12.6 Drug-alert display screens from Partners out-patient medical record application (Longitudinal Medical Record, LMR). The screens show ( a ) a drug-allergy alert
for captopril, and ( b ) a drug-drug interaction between cip-rofl oxacin and warfarin (Source: Courtesy of Partners Health Care System, Chestnut Hill, MA)
12 Electronic Health Record Systems
1. Systems that assist in differential diagnosis
2. Patient-specific recommendations for direct action (e.g. alerts, reminders)
3. Systems that group information: dashboards, order sets
Types of CDS systems
1. Systems that assist in differential diagnosis
2. Patient-specific recommendations for direct action (e.g. alerts, reminders)
3. Systems that group information: dashboards, order sets
4. Risk assessment tools
Types of CDS systems
16-‐02-‐15
4
1. Systems that assist in differential diagnosis
2. Patient-specific recommendations for direct action (e.g. alerts, reminders)
3. Systems that group information: dashboards, order sets
4. Risk assessment tools
5. Patient decision aids
Types of CDS systems
16-‐02-‐15
5
• Roshanov et al. reviewed 162 randomised CDS trial
• Systems improved the process of medical care in 52-64% of studies
• Proof of positive impact on patient outcomes was rare
• Positive effects were found for systems that
- also provided advice to patients (OR 2.77) - required a reason for over-riding advice (OR 11.23) - were evaluated by their developers (OR 4.35)
• Systems that were integrated with EHR or CPOE systems were less likely to be effective (OR 0.37)
Roshanov et al., BMJ 2013;346:f657.
Are CDS systems effective?
1. Computerised decision support: An ultrabrief history
2. What types of systems exist? Are they effective?
3. CDS for chronic disease management
4. Example: glucose regulation with PANDIT
5. Challenges for the future
6. Conclusion
Menu Development of chronic diseases
disease process histological and func2onal changes
symptoms
Time
• Acute care - reactive - speed is important
- short-term outcomes - marginal role for patients
• Chronic care - focus on prevention - needs to be proactive
- long-term outcomes - important role for patients
Acute vs chronic care
1. Systems that assist in differential diagnosis
2. Patient-specific recommendations for direct action (e.g. alerts, reminders)
3. Systems that group information: dashboards, order sets
4. Risk assessment tools
5. Patient decision aids
Types of CDS systems
16-‐02-‐15
6
1. Systems that assist in differential diagnosis
2. Patient-specific recommendations for direct action (e.g. alerts, reminders)
3. Systems that group information: dashboards, order sets
4. Risk assessment tools
5. Patient decision aids
Types of CDS systems
Assist in prevention
E.g. 10-year cardiovascular risk screening
1. Systems that assist in differential diagnosis
2. Patient-specific recommendations for direct action (e.g. alerts, reminders)
3. Systems that group information: dashboards, order sets
4. Risk assessment tools
5. Patient decision aids
Types of CDS systems
Early detection of chronic
disease E.g. blood pressure out of
range
1. Systems that assist in differential diagnosis
2. Patient-specific recommendations for direct action (e.g. alerts, reminders)
3. Systems that group information: dashboards, order sets
4. Risk assessment tools
5. Patient decision aids
Types of CDS systems
Standardisation of care pathways
E.g. referral schemes
1. Systems that assist in differential diagnosis
2. Patient-specific recommendations for direct action (e.g. alerts, reminders)
3. Systems that group information: dashboards, order sets
4. Risk assessment tools
5. Patient decision aids
Types of CDS systems
Informed and shared decision
making
E.g. cardiovascular
medication
1. Systems that assist in differential diagnosis
2. Patient-specific recommendations for direct action (e.g. alerts, reminders)
3. Systems that group information: dashboards, order sets
4. Risk assessment tools
5. Patient decision aids
6. Self-regulation support
Types of CDS systems
Control theory
16-‐02-‐15
7
1. Computerised decision support: An ultrabrief history
2. What types of systems exist? Are they effective?
3. CDS for chronic disease management
4. Example: glucose regulation with PANDIT
5. Challenges for the future
6. Conclusion
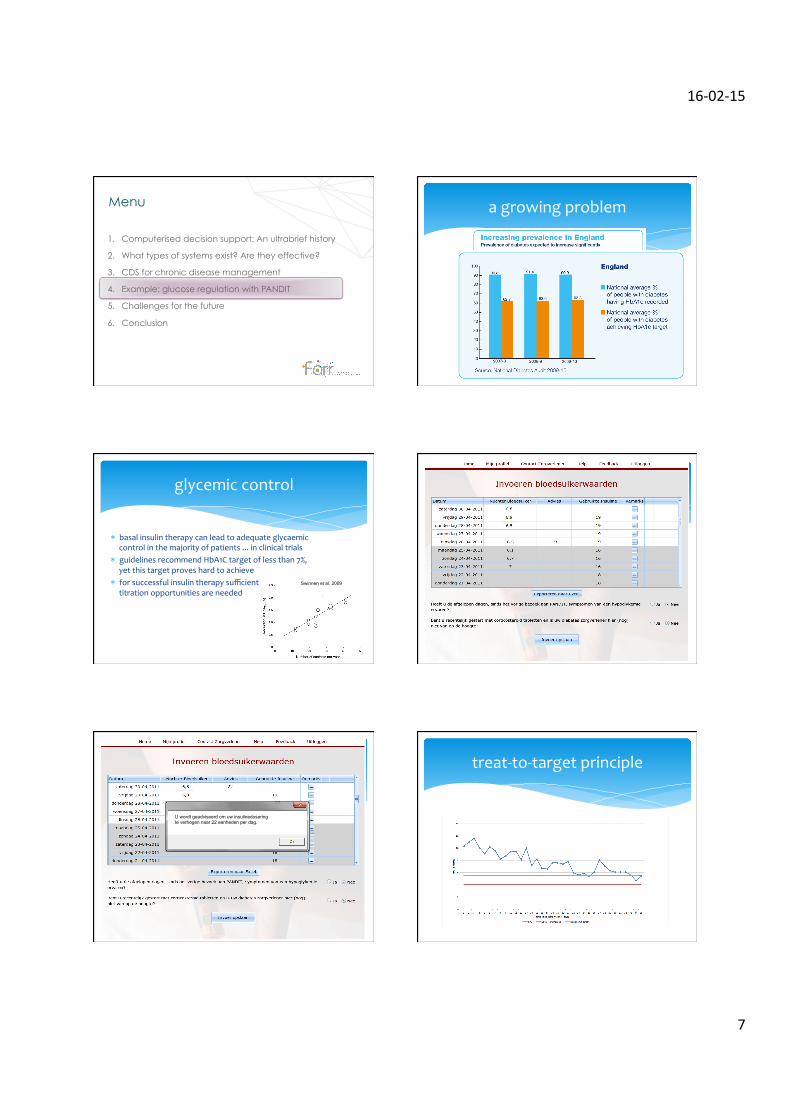
Menu a growing problem
* basal insulin therapy can lead to adequate glycaemic control in the majority of patients ... in clinical trials * guidelines recommend HbA1C target of less than 7%,
yet this target proves hard to achieve * for successful insulin therapy sufficient
titration opportunities are needed
glycemic control
Swinnen et al. 2009
U wordt geadviseerd om uw insulinedosering te verhogen naar 22 eenheden per dag.
treat-‐to-‐target principle
16-‐02-‐15
8
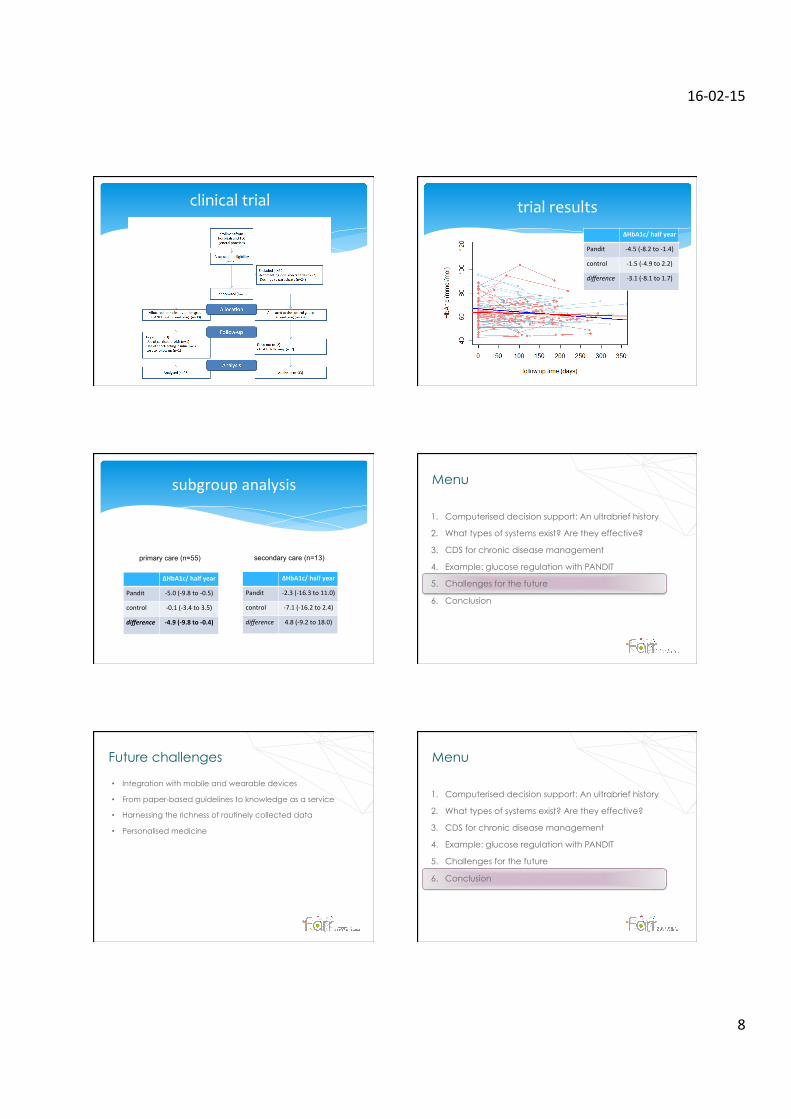
clinical trial trial results ΔHbA1c/ half year
Pandit -‐4.5 (-‐8.2 to -‐1.4)
control -‐1.5 (-‐4.9 to 2.2)
difference -‐3.1 (-‐8.1 to 1.7)
subgroup analysis
ΔHbA1c/ half year
Pandit -‐5.0 (-‐9.8 to -‐0.5)
control -‐0.1 (-‐3.4 to 3.5)
difference -‐4.9 (-‐9.8 to -‐0.4)
primary care (n=55)
ΔHbA1c/ half year
Pandit -‐2.3 (-‐16.3 to 11.0)
control -‐7.1 (-‐16.2 to 2.4)
difference 4.8 (-‐9.2 to 18.0)
secondary care (n=13)
1. Computerised decision support: An ultrabrief history
2. What types of systems exist? Are they effective?
3. CDS for chronic disease management
4. Example: glucose regulation with PANDIT
5. Challenges for the future
6. Conclusion
Menu
• Integration with mobile and wearable devices
• From paper-based guidelines to knowledge as a service
• Harnessing the richness of routinely collected data
• Personalised medicine
Future challenges
1. Computerised decision support: An ultrabrief history
2. What types of systems exist? Are they effective?
3. CDS for chronic disease management
4. Example: glucose regulation with PANDIT
5. Challenges for the future
6. Conclusion
Menu
16-‐02-‐15
9
• Computerised decision support is an umbrella term
• Variety of driving forces – shift over time
• Reasonably good effects on processes of care
• Chronic disease management – prevention
– early detection – care pathways
– shared decision making – self-regulation
Conclusions
• Airin Simon • Frits Holleman • Joost Hoekstra • Roderik Kraaijenhagen • Ameen Abu-Hanna
Niels Peek MRC Health eResearch Centre The University of Manchester
@NielsPeek
Thanks






![AMS Assembly Thursday, October 24th 2013 Kingston City ... · 10/24/2013 · 10th, 2013, as seen in Appendix C: Peek Freans [Motion 5] e. That AMS Assembly approve the amendment](https://img.pdfslide.net/doc/110x75/5faa67f94d927225a02edc61/ams-assembly-thursday-october-24th-2013-kingston-city-10242013-10th-2013.jpg)