Embed Size (px)
Citation preview

104/15/2304/15/23 11
National Rural Health Mission:National Rural Health Mission:A Ground RealityA Ground Reality
Presented by:Presented by:
Dr. Y.L. TekhreDr. Y.L. TekhreDirector (Research)Director (Research)
National Human Rights CommissionNational Human Rights Commission
Email: Email: [email protected] & [email protected][email protected] & [email protected]. [Resi.] Ph. [Resi.] 011-26161708011-26161708(Office) (Office) 011- 23386581 (Mobile) 9868182696011- 23386581 (Mobile) 9868182696
2
Some of the features• Allocation for human resources in health
from Rs. 62 crore in 2009-10 to Rs. 323 crore in 2010-11
• India is short by 6 lakh doctors, 10 lakh nurses and 2 lakh dental surgeons
• The overall allocation for the health ministry increased by 14% from Rs. 19,534 crore to Rs. 22,300 crore for 2010-11
3
• Cancer, diabetes, mental health and cardiovascular disease received a major push
• Cancer kills 50 people in India every hour while 7% of the country’s adult population is estimated to be suffering from mental health problems
• Annual health survey to prepare the health profile of all districts (626 districts) will be conducted in 2010-11 to benefit the NRHM
4
• Shift in National Health Policy - From Hospital based services to
• Community based services duly backed by Strong Referral Services
• Challenges to Health & Healthy Living– Rural India (Majority of population living in
villages)– High density of rural population– Varied Linguistic & Ethnic background– Illiteracy– Low per capita income
5
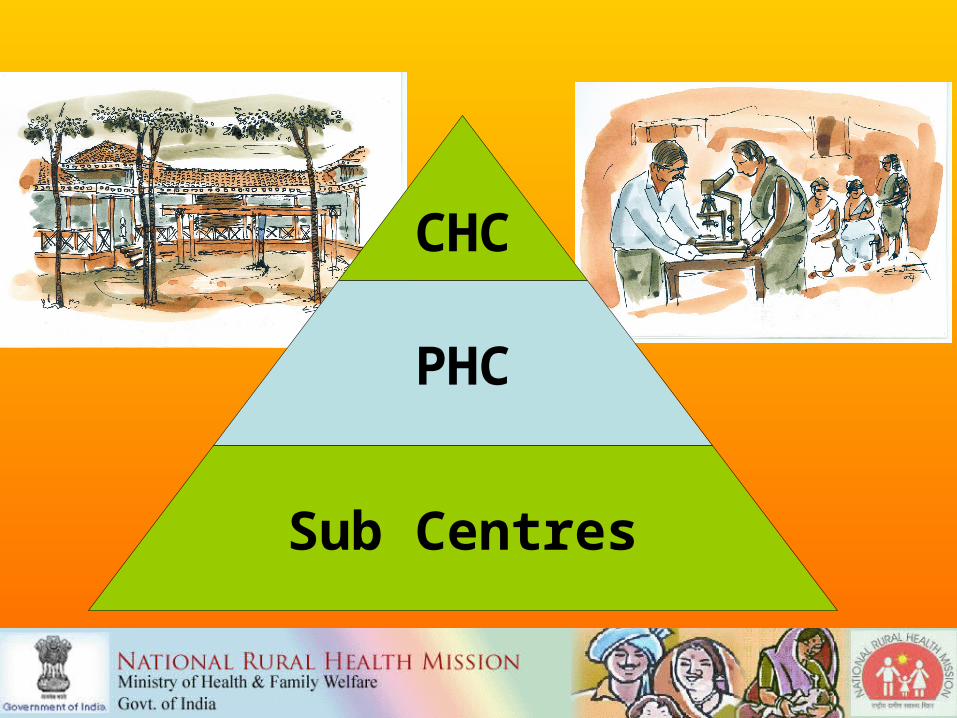
CHC
PHC
Sub Centres
6
The Structure of the Public Health System
• Health is a state subject. Family Welfare is a concurrent subject, Primary health care is a PRI devolved area – Mandated role of local governments
• Most institutions and manpower in state sector.
• Most programmes are in the central sector
National Programmes address only about 25% of all morbidities. States have to address the major part of this.
• National Programmes cannot succeed without basic health systems being functional
7
Rejuvenate the Health delivery System
Universal Health Care AccessAffordabilityEquity Quality
Reduce IMR, MMR,TFRImprove Disease control
National Rural Health Mission Launched in April,
2005
8
EXPECTED OUTCOMES 2005 - 2012
•Universal Health care, well functioning health delivery system.
•IMR reduced to 30/1000 live births by 2012
•MMR reduced to 100/100,000 live births by 2012
•TFR reduced to 2.1 by 2012
•Malaria Mortality Reduction Rate – 60% upto 2012
•Kala Azar eliminated by 2010, Filaria reduced by 80 % by 2010
•Dengue Mortality reduced by 50% by 2012
•TB DOTS series – maintain 85% cure rate
•Responsive Health System
9
Strategies
•Improve Infrastructure•Augment manpower•Improve management•Flexibility to states to deploy funds
•Decentralisation•Communitization
10
• An audit of maternal deaths will be conducted soon in all states, said the Health Minister Mr. Azad…
• "This year, we have taken another new initiative on a national level and that is the introduction of maternal death audits at the community as well as the facility level,"
11
The Paradigm Shift• Decentralised planning:
•2005 : normative funding•2006 : state PIPs•2007 : district Plans & state PIPs•2008 : block desegregation in IDHAP, state
PIPs.•2009 : villages should make village health
plans
• Need to •create capacity.•create quality and appraisal mechanisms•address uneven development
12
Planning at the user end
• Resource Mapping – service providers, communication facilities , drinking water sources, sanitation, nutritional status, levels of poverty.
• Understanding main health problems of women and children, providers used, perception of public health services and providers
• Main illnesses in the community, Health care related expenditure, problems faced in referral and transport, perceptions about family planning and gender, Role of PRI in health related areas ( water, sanitation)
• Understanding process of Pregnancy, labour and post natal care, beliefs and practices – Key informant interview with elderly women, TBA.
13
Planning at the user endUnderstanding Community Participation and Ownership
Meeting PRI members to understand perception of health needs
Additional information
– Any special health related studies in the district by any agency
– Any Health NGO active in the district
– Other Community Based Organizations in the district
14
• Outputs and Outcome based
• Not only •how many buildings were built•how many training were conducted
• but also•how it impacted on behavior change•service delivery•health status.
The Paradigm Shift
15
BASIC FEATURES of community monitoring
• PRIs, community based organizations and NGOs, along with health department functionaries should be involved in the preparation and mobilization phase
• The committees that are formed at various levels must have concomitant authority i.e. they must have the power to initiate action.
• Capacities of the members of a village level committee have to be built
• Involvement of the general public by means of regular ‘Public dialogue’ or Public hearing (Jan Samvad / Jan Sunwai)
16
TOOLS OF MONITORINGVillage Level
• Village Health Register - Records of ANM - Public dialogue (Jan Sa)
• Village Health Calendar- Infant and maternal death auditPHC level
• Charter of Citizens Rights – IPHS - PHC Health Plan
Block level• IPHS - Charter of Citizens Rights - Block Health Plan
District level• Report from the PHC / District Mission Health committees• Public Dialogue (Jan Samvad)
State level• Reports of the District Health committees• Periodic assessment reports by various taskforces / State level
committees about the progress made in formulating policies according to IPH Standards, NHRC recommendations and its implementation status etc.
17
• Community Participation • Bringing the public back into public
health
• At hamlet level : ASHA, VHSC, SHGs, Panchayats.
• At the facility level: RKS• At the management level : health societies
The Paradigm Shift
18
Likely capacity needs Developing and supporting more
than
• 6000 Block Mission Team and Block Resource Groups
• 600 District level Mission Teams and Resource Groups
• 35 State/UT level Mission Teams and Resource Centres
• 1.75 lakh ANMs, 26000 LHVs, 26000 Staff Nurses
• 26000 Medical Officers into Skilled Birth Attendants.
• 2 lakh ANMs, Nurses, etc. at induction level.

19
Likely capacity needs Developing and supporting more than
• 7 lakh Village Health and Sanitation Committees
• 1.75 lakh Sub Centre level Panchayat Committees
• 25000 PHC level PRI/HDC/RKS Committees
• 6500 CHC level PRI/ HDC/RKS Committees
• 1200 Taluka/ Sub Divisional level Hospital Committees.
• 600 District Hospital level Committees.
20
Reproductive Health
• Abortion• Infertility• Contraception• Sexually Transmitted Diseases
21
AdolescenceWHO defines adolescence both
in terms of age (spanning the ages between 10 and 19 years) and in terms of a phase of life marked by special attributes.
These attributes include:
22
1. Rapid physical growth and development
2. Physical, social and psychological maturity but not all at the same time
3. Sexual maturity and the sexual activity
4. Development of adult mental processes and adult identity
5. Transition from total socio-economic dependence to relative independence

23
Pregnancy Health
• Ensuring safe motherhood
• Complications of Pregnancy
24
Important aspects of NHRM
• Ensuring effective healthcare, especially to the poor and vulnerable sections
• Ayurveda, Yoga & Naturopathy, Unani, Siddha and Homoeopathy (AYUSH)
25
Contd.
• Under AYUSH, there is a network of 3,360 hospitals and 21,769 dispensaries across the country
• The NRHM covers all the villages through village-based "Accredited Social Health Activists" (ASHA) who would act as a link between the health centers and the villagers
26
• The ASHA would be trained to advise villagers about:
• Sanitation, Hygiene, Contraception, and Immunization to provide Primary Medical Care for Diarrhoea, Minor Injuries, and Fevers; and to escort patients to Medical Centers
• They would also deliver Directly Observed Treatment Short (DOTS) course for tuberculosis and oral rehydration; distribute folic acid tablets and chloroquine to patients and alert authorities to unusual outbreaks.
27
ASHAs would be honorary volunteers, there is a provision to provide them with performance-based compensation for undertaking specific health or other social sector programmes with measurable outputs, thus promoting employment for these volunteers
•‘One ASHA per 1000 population’. In tribal, hilly, desert areas the norm could be relaxed to one ASHA per habitation, dependant on workload etc.
28
Criteria for selection as ASHA
• ASHA must be primarily a woman resident of the village - ‘Married/Widow/Divorced’ and preferably in the age group of 25 to 45 yrs.
• ASHA should have effective communication skills, leadership qualities and be able to reach out to the community.
• She should be a literate woman with formal education up to Eighth Class. This may be relaxed only if no suitable person with this qualification is available.
29
Maternal Mortality
Maternal Mortality Ratio“ number of women who die in a year due to causes related to pregnancy and child birth for every 100, 000 live births ”
Wide Variations:India 301/100,000 live birthsTamil Nadu 134/100,000 live birthsU.P. 517/100,000 live birthsSweden/USA 8-12/100,000 live births Sri Lanka 24/100,000 live birthsMalaysia 20/100,000 live births
30
Population
Agriculture
Health
Education
Economy
Urbanisation
Environment

311
WHERE WE STAND
NPP 2000 and the present scenario:
1. 2010 Population replacement (put back now to 2021)
2. 2045Population Stabilization (put back now to 2060 (1.53 billion in 2060).
3. EAG states constitute 42% of the population (TFR between 3.4 and 4.3)
32
Low male participation Low age at marriage for girls Low age at bearing Children Low spacing between pregnancies Too many pregnancies Strong preference for son Low female literacy Low women’s empowerment
AREAS OF CONCERN IN FP ( Socio cultural factors)
33
3457
Areas of concern in FP (Programmatic factors)
Large unmet needs for contraception
Poor quality of family planning services
Inadequate attention to spacing methods
Low proportion of safe deliveries
35
India’s Challenge
26 million births every year
1.1 million die before 4 weeks of age
1.7 million die before completing 1 year
2.2 million die before completing 5 years
77,000 mothers die in this process
36
What to do?• Increasing public expenditure on health• Reducing regional imbalance in health
infrastructure• Pooling resources• Integration of organizational structures• Optimization of health manpower• Decentralization and district
management of health programmes
37
• Community participation and ownership of assets
• Induction of management and financial personnel into district health system
• Operationalizing community health centers into functional hospitals meeting Indian Public Health Standards in each Block of the Country
38
• India needs over 6,800 more hospitals in rural areas to provide basic health facilities to people
"There is still a shortage of 4,477 primary healthcare centres and 2,337 community healthcare centres as per the 2001 population norms," the survey said. (Annual Survey)
39
• Almost 29% of the existing health infrastructure is in rented buildings. Poor upkeep and maintenance, and high absenteeism of manpower in the rural areas are the main problems in the health delivery system."
• The latest audit report of the Controller and Auditor General (CAG) on National Rural Health Mission (NRHM) has found that hundreds of crores are lying unspent
4055
41

42
THANK
YOU
THANK
YOU






























