Embed Size (px)
Citation preview
ColorectalCancerTaskForceMonthlyMee2ngSeptember8,2016
Presenter:RyanKerr
COLORECTAL CANCER SCREENING OPTIONS FROM THE NEW USPSTF RECOMMENDATION
STATEMENT: A BRIEF OVERVIEW
CRC Screening Tests
• Flexible Sigmoidoscopy
• Colonoscopy • CT Colonography
• gFOBT (guaiac)
• FIT • FIT-DNA Test
(Cologuard)
Stool-Based
• SEPT9 DNA Test (Epi proColon)
Direct Visualization
Serology (Blood)
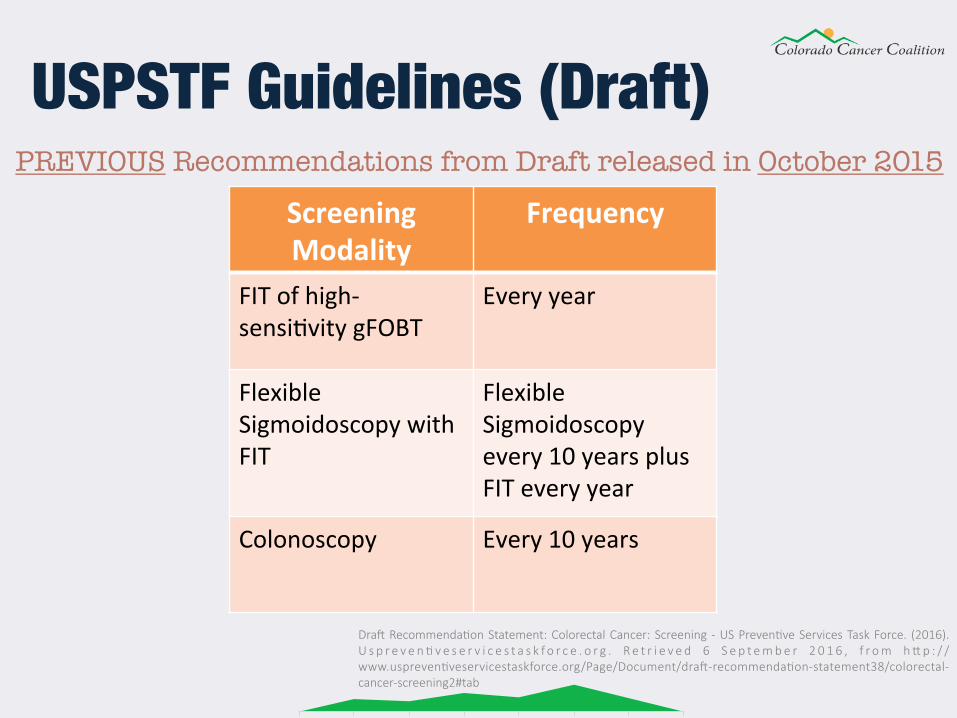
PREVIOUS Recommendations from Draft released in October 2015
USPSTF Guidelines (Draft) ScreeningModality
Frequency
FITofhigh-sensi2vitygFOBT
Everyyear
FlexibleSigmoidoscopywithFIT
FlexibleSigmoidoscopyevery10yearsplusFITeveryyear
Colonoscopy Every10years
Dra$ Recommenda-on Statement: Colorectal Cancer: Screening - US Preven-ve Services Task Force. (2016). U s p r e v e n - v e s e r v i c e s t a s k f o r c e . o r g . R e t r i e v e d 6 S e p t e m b e r 2 0 1 6 , f r o m h I p : / /www.uspreven-veservicestaskforce.org/Page/Document/dra$-recommenda-on-statement38/colorectal-cancer-screening2#tab
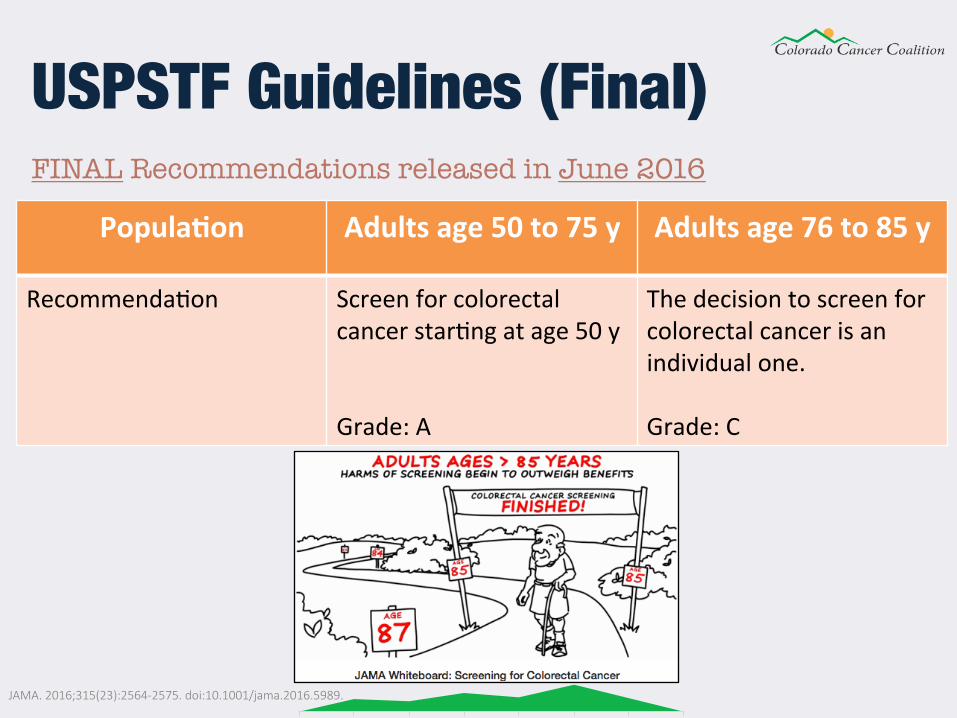
USPSTF Guidelines (Final) FINAL Recommendations released in June 2016 Popula5on Adultsage50to75y Adultsage76to85y
Recommenda2on Screenforcolorectalcancerstar2ngatage50yGrade:A
Thedecisiontoscreenforcolorectalcancerisanindividualone.Grade:C
JAMA. 2016;315(23):2564-2575. doi:10.1001/jama.2016.5989.
USPSTF Guidelines (Final)
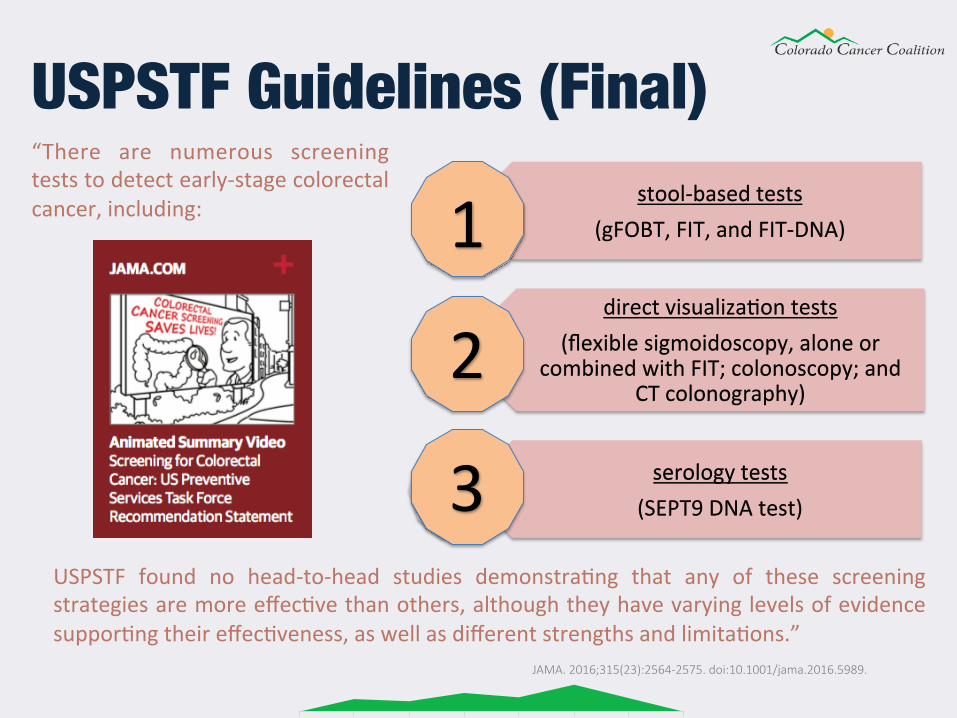
JAMA. 2016;315(23):2564-2575. doi:10.1001/jama.2016.5989.
stool-basedtests(gFOBT,FIT,andFIT-DNA)
directvisualiza2ontests(flexiblesigmoidoscopy,aloneor
combinedwithFIT;colonoscopy;andCTcolonography)
serologytests(SEPT9DNAtest)
“There are numerous screeningteststodetectearly-stagecolorectalcancer,including:
USPSTF found no head-to-head studies demonstra2ng that any of these screeningstrategiesaremoreeffec2vethanothers,althoughtheyhavevaryinglevelsofevidencesuppor2ngtheireffec2veness,aswellasdifferentstrengthsandlimita2ons.”
1
2
3
USPSTF Guidelines (Final)
JAMA. 2016;315(23):2564-2575. doi:10.1001/jama.2016.5989.
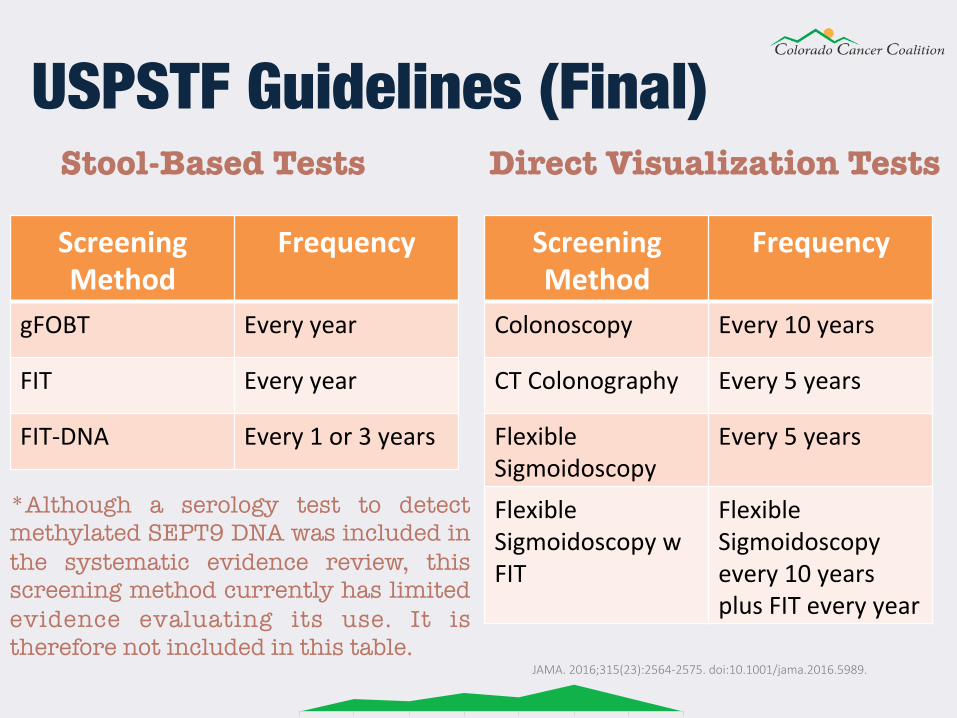
USPSTF Guidelines (Final)
ScreeningMethod
Frequency
Colonoscopy Every10years
CTColonography Every5years
FlexibleSigmoidoscopy
Every5years
FlexibleSigmoidoscopywFIT
FlexibleSigmoidoscopyevery10yearsplusFITeveryyear
Stool-Based Tests Direct Visualization Tests
ScreeningMethod
Frequency
gFOBT Everyyear
FIT Everyyear
FIT-DNA Every1or3years
*Although a serology test to detect methylated SEPT9 DNA was included in the systematic evidence review, this screening method currently has limited evidence evaluating its use. It is therefore not included in this table.
JAMA. 2016;315(23):2564-2575. doi:10.1001/jama.2016.5989.
gFOBT (guaiac) Guaiac-based fecal occult blood test
• Detects heme in stool on guaiac paper • Guaiac is a substance from a plant that is used to coat the FOBT test
cards • Prior to taking the test, you must avoid red meat, certain veggies
and fruits, certain medications and supplements • You collect a stool sample from 3 different bowel movements. • For each bowel movement, you smear a small amount of the stool on
a card provided in the kit • You mail the card to a laboratory for testing • A positive test result must be followed up with a colonoscopy • Not as accurate as newer FIT technology (less sensitive and specific)
gFOBT (guaiac)
Stool guaiac test: MedlinePlus Medical Encyclopedia. (2016). Medlineplus.gov. Retrieved 6 September 2016, from hIps://medlineplus.gov/ency/ar-cle/003393.htm
JAMA. 2016;315(23):2564-2575. doi:10.1001/jama.2016.5989.
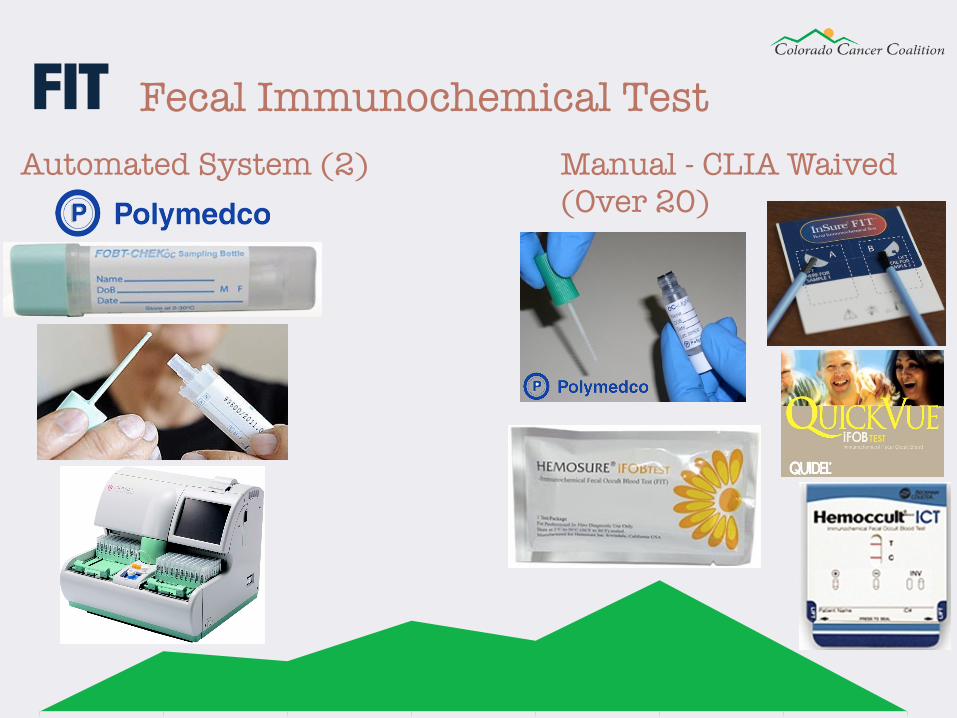
FIT Fecal Immunochemical Test Manual - CLIA Waived (Over 20)
Automated System (2)
• Detects invisible human hemoglobin in stool • Higher sensitivity and specificity than gFOBT • Polyps or tumors in the colon have blood vessels on their surface
that can release a small amount of blood into the stool • No advanced prep or dietary restrictions and no medication
modification • Test is completed at home and resulted in a clinical laboratory • Low cost and easy to complete (high compliance) • Annual test (unless abnormal result) • A positive result usually means a colonoscopy is required
FIT
JAMA. 2016;315(23):2564-2575. doi:10.1001/jama.2016.5989. Colorectal Cancer (CRC) 104: Ge]ng Tested. (2016). Gastro.org. Retrieved 6 September 2016, from hIp://www.gastro.org/info_for_pa-ents/colorectal-cancer-crc-104-ge]ng-tested
• Many FITs on the market • Some FITs are indicated for the patient to provide more than 1
sample from separate bowel movements • Two types of FITs (results read manually or by automated analyzer) • “Among the FITs that are cleared by the US Food and Drug
Administration (FDA) and available for use in the United States, the OC FIT-CHEK family of FITs (Polymedco)—which include the OC-Light and the OC-Auto—have the best test performance characteristics (i.e., highest sensitivity and specificity).”
• Auto FITs allow for accurate screening at a population level • Lower sensitivity and higher specificity than Cologuard (single test
comparison)
FIT
JAMA. 2016;315(23):2564-2575. doi:10.1001/jama.2016.5989.

FIT-DNA (Cologuard)
• “Cologuard is designed to analyze patients’ stool for the presence of hemoglobin and DNA methylation and mutation markers, which may indicate the presence of colorectal cancer or precancerous lesions.”
• “Every day the colon sheds cells that line the inside of the colon. Cologuard utilizes 11 distinct molecular biomarkers (including FIT) to detect the DNA and hemoglobin (red blood cells) released from abnormal cells, if present.”
• No advanced prep or dietary restrictions and no medication modification • A positive Cologuard result still requires a diagnostic colonoscopy • In a one time screening comparison, Cologuard is more sensitive but less
specific than FIT (which means it has a higher number of false-positive results and higher likelihood of follow-up colonoscopy and experiencing an associated adverse event per screening test)
• Limited evidence for frequency of use, so for now CMS determined a 3 year interval
• It has a very involved collection process and a completed test must be returned to Madison Wisconsin within 72 hours
FIT-DNA (Cologuard)
JAMA. 2016;315(23):2564-2575. doi:10.1001/jama.2016.5989. Cologuard’s FDA Approved Pa-ent Brochure
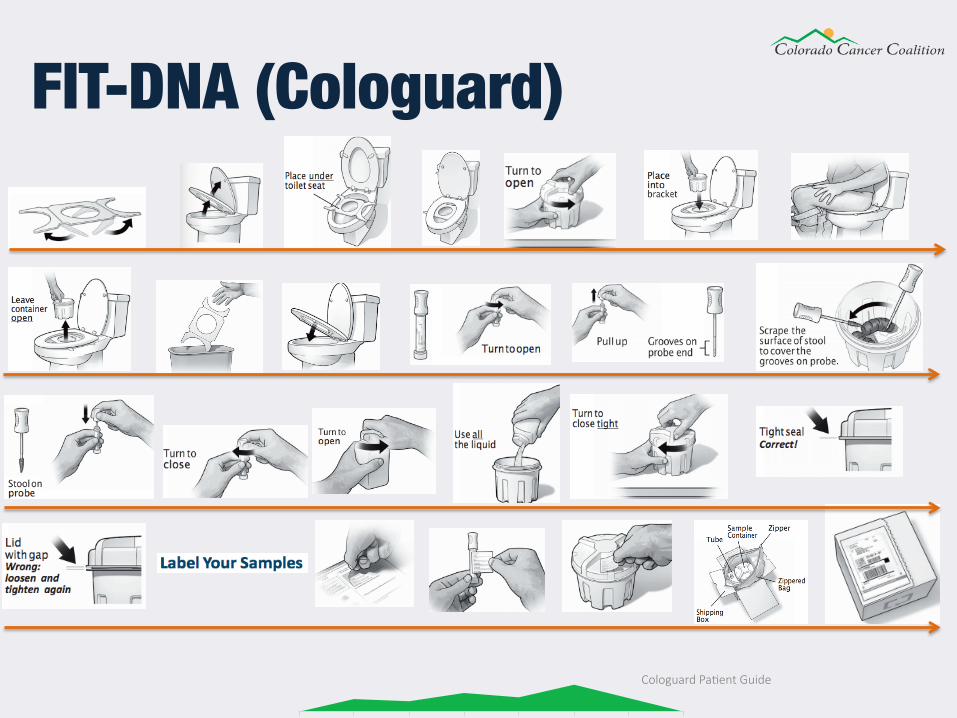
FIT-DNA (Cologuard)
Cologuard Pa-ent Guide
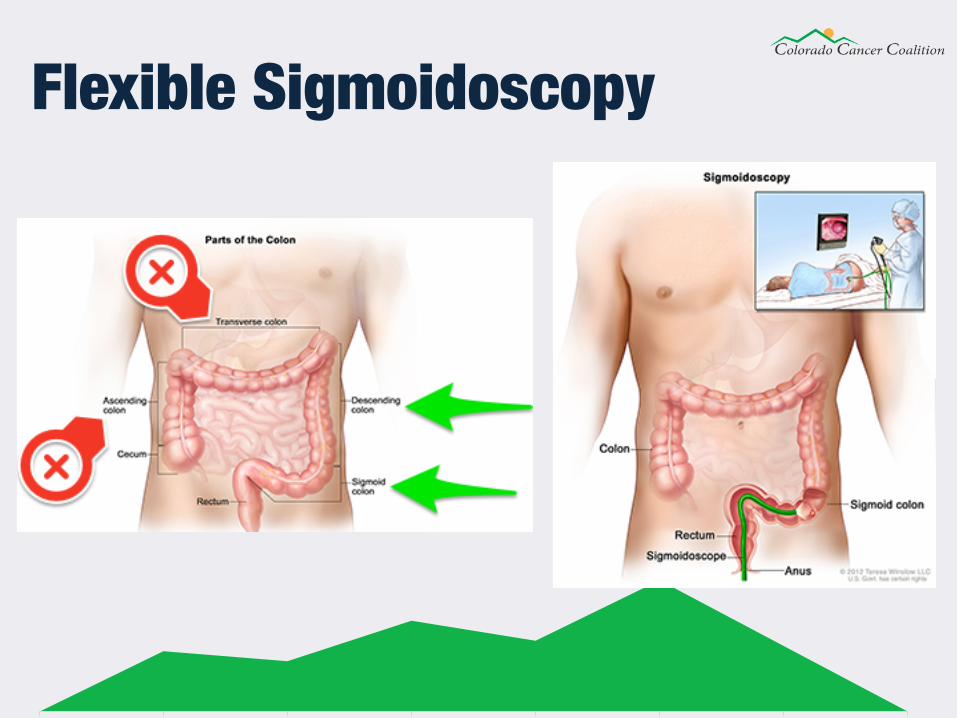
Flexible Sigmoidoscopy
• For this test, the doctor puts a short, thin, flexible, lighted tube into your rectum
• Using a tiny video camera at the tip of the tube, the doctor checks for polyps or cancer inside the rectum and lower third of the colon.
• If necessary, tissue samples (biopsies) can be taken through the scope during a flexible sigmoidoscopy exam, however a follow up colonoscopy may still be required
• Similar bowel prep to that for a colonoscopy • Can be performed during an office visit or at an outpatient center • It typically does not require sedatives or anesthesia • The procedure generally takes 20 minutes • Only 1.3% screening eligible population underwent a flexible
sigmoidoscopy in 2010
Flexible Sigmoidoscopy
Flexible Sigmoidoscopy. (2016). Niddk.nih.gov. Retrieved 6 September 2016, from hIps://www.niddk.nih.gov/health-informa-on/health-topics/diagnos-c-tests/flexible-sigmoidoscopy/Pages/diagnos-c-test.aspx 'Vanished' in US, Sigmoidoscopy Saves Lives in Norway. (2016). Medscape. Retrieved 6 September 2016, from hIp://www.medscape.com/viewar-cle/829806#vp_2
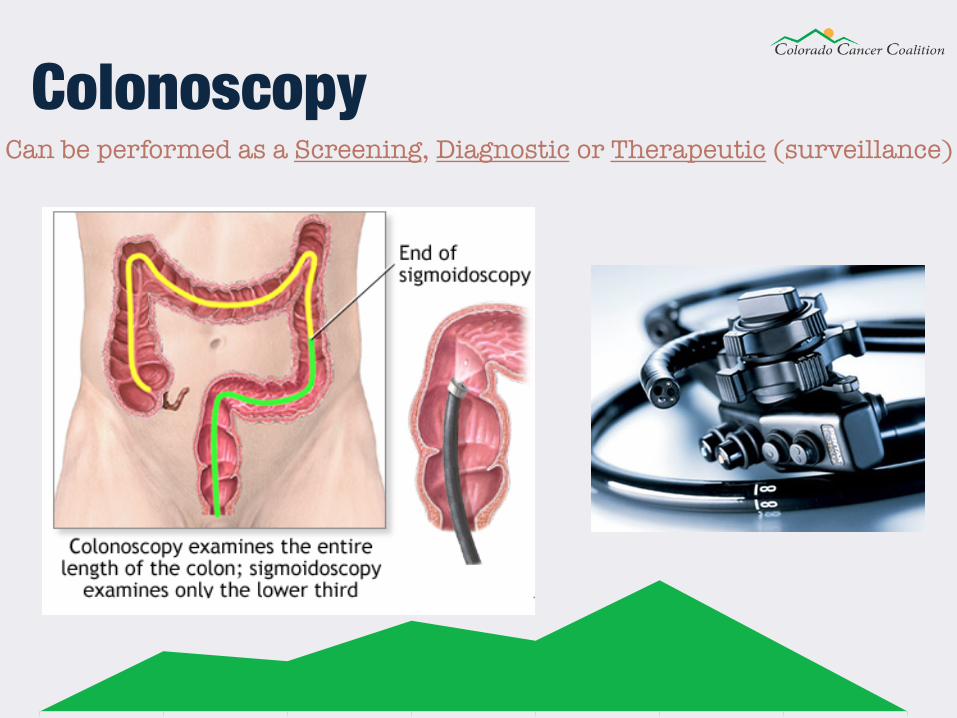
Colonoscopy Can be performed as a Screening, Diagnostic or Therapeutic (surveillance)
Colonoscopy • This is similar to flexible sigmoidoscopy, except the doctor uses a
longer, thin, flexible, lighted tube with a camera on the end, called a colonoscope or scope, to check for polyps or cancer inside the rectum and the entire colon
• During the test, the doctor can find and remove most polyps and some cancers
• Colonoscopy also is used as a follow-up test if anything unusual is found during one of the other screening tests
• Fasting and bowel cleanse required • Sedatives or anesthesia are usually required (You must prearrange a
ride home from procedure ) • The procedure takes about 30 minutes • While the risk of side effects are low, perforations and major bleeding
are possible • Expensive Colonoscopy. (2016). Niddk.nih.gov. Retrieved 6 September 2016, from hIps://www.niddk.nih.gov/health-
informa-on/health-topics/diagnos-c-tests/colonoscopy/Pages/diagnos-c-test.aspx
CT Colonography Computed Tomography Colonography
• Virtual colonoscopy, also called computerized tomography (CT) colonography, is a procedure that uses a combination of x rays and computer technology to create 3D images of the rectum and entire colon
• Uses low dose radiation CT scanning to obtain an interior view of the colon that is otherwise only seen with a scope
• The night before a CTC, the patient must cleanse the bowel as well as drink a special dye, called contrast medium
• Examination takes about 10 minutes and does not require sedatives • If abnormalities are found, colonoscopy is required (12%-25% of the
time) • CTC is completed by radiologist
CT Colonography
hIps://www.niddk.nih.gov/health-informa-on/health-topics/diagnos-c-tests/virtual-colonoscopy/Pages/diagnos-c-test.aspx#best
During the procedure: • The patient is placed in a supine position on the examination table • The patient may be given a dosage of Butylscopolamine
intravenously to minimize muscle activity in the area • A thin tube is inserted into the rectum, so that air can be pumped
through the tube in order to inflate the colon for better viewing. • The table moves through the scanner • The patient is asked to hold his/her breath during the scan to avoid
distortion on the images • The scan is then repeated with the patient lying in a prone position
CT Colonography
hIps://www.niddk.nih.gov/health-informa-on/health-topics/diagnos-c-tests/virtual-colonoscopy/Pages/diagnos-c-test.aspx#best
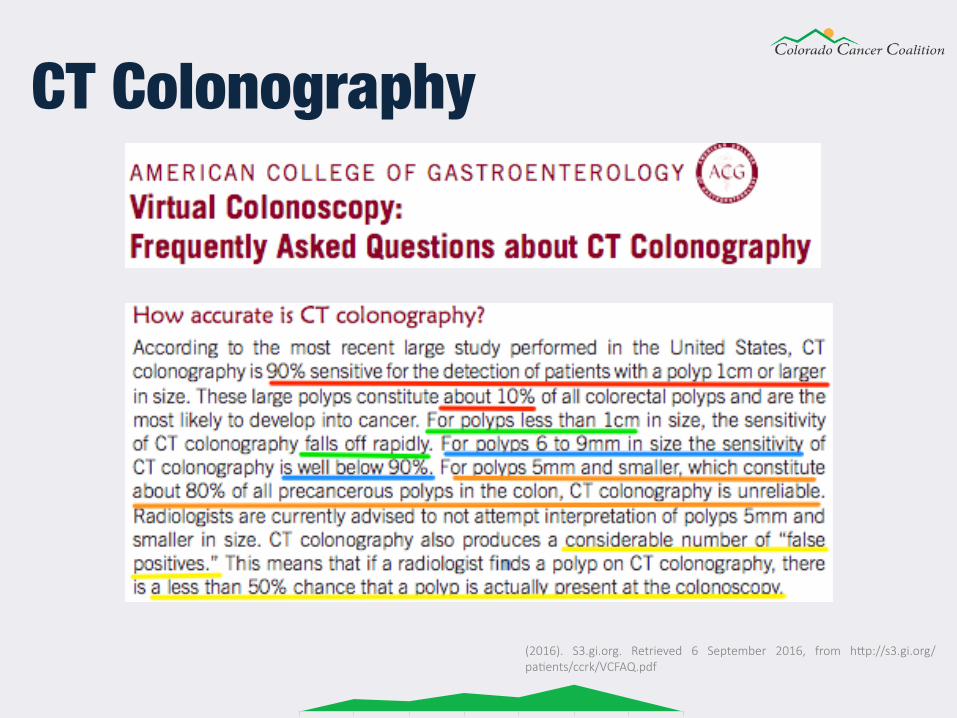
CT Colonography
(2016). S3.gi.org. Retrieved 6 September 2016, from hIp://s3.gi.org/pa-ents/ccrk/VCFAQ.pdf
SEPT9 DNA (Epi proColon)
• It detects a specific type of DNA called Septin 9. • Septin 9 DNA is altered in colorectal cancer tumor cells more often
than in normal cells • The tumor cells release altered Septin 9 DNA into the bloodstream • The altered DNA can be detected in a blood sample • Epi proColon is highly accurate for the detection of methylated
Septin 9 DNA in blood • Altered Septin 9 DNA is often found in blood samples from people
with colorectal cancer • In April 2016, Epi proColon (third generation) became the first FDA
approved blood-based test for CRC screening
SEPT9 DNA (Epi proColon)
Clinical Chemistry, September 2014 vol. 60 no. 9 1183-1191 doi: 10.1373/clinchem.2013.221044
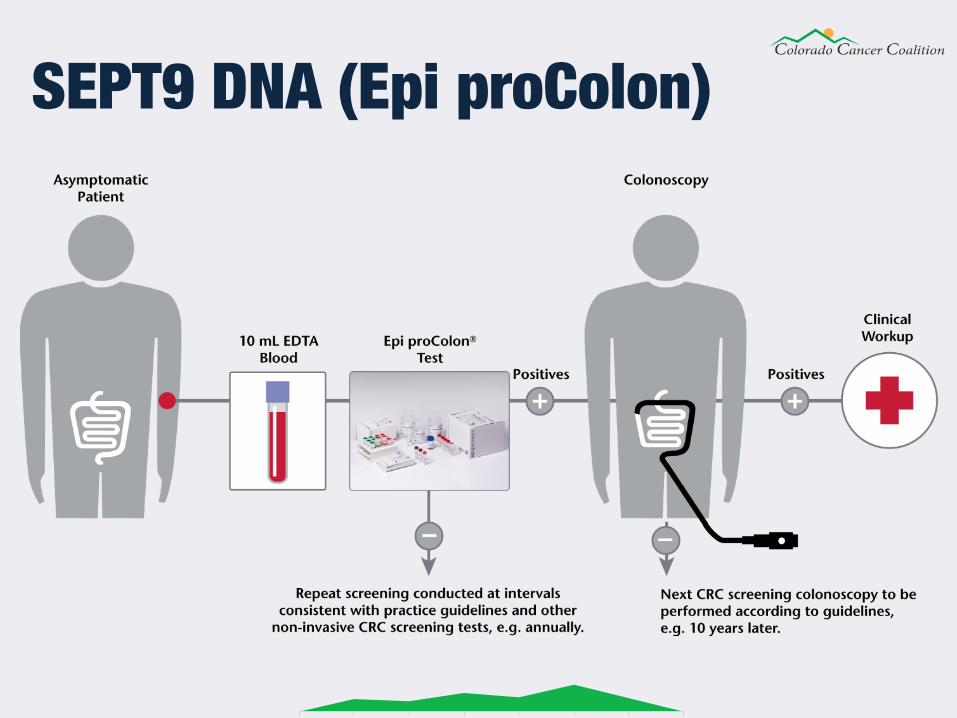
• It is currently recommended for annual screening to eligible individuals who are unable or unwilling to have a colonoscopy or a FIT
• Simple blood draw with no preparation necessary • High patient compliance • No advanced prep or dietary restrictions and no medication
modification • Approximately 70% sensitivity, 80% specificity, 99.7% NPV
(negative predictive value) • Positive test result requires a follow up colonoscopy. • It has been assigned a CPT billing code for 2017 • Jury is still out on Epi proColon
SEPT9 DNA (Epi proColon)
Clinical Chemistry, September 2014 vol. 60 no. 9 1183-1191 doi: 10.1373/clinchem.2013.221044 PLoS One 2014, 9(6):1-8. e98238 DOI: 10.1371/journal.pone.0098238
SEPT9 DNA (Epi proColon)
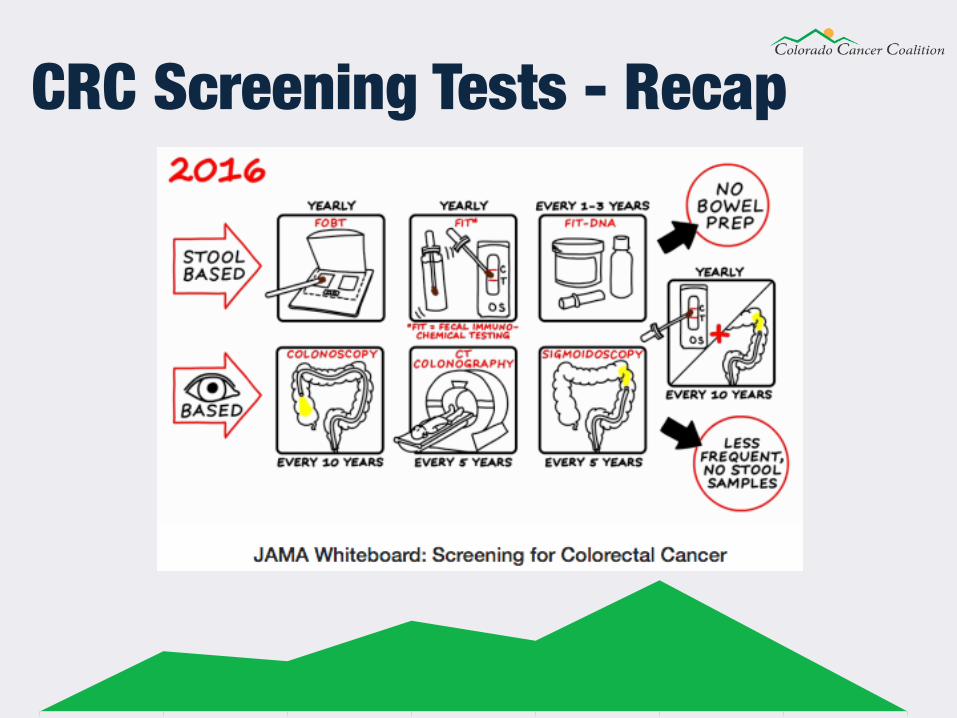
CRC Screening Tests - Recap

Questions?
Appendix • Which Test is Best?
• Considerations for an Individual
• Considerations for a Population
• Benefits, Harms and Burdens - Models
• Pros and Cons of Each Screening Strategy
There is no single “best test” for any person. Each test has advantages and disadvantages. Talk to your doctor about the pros and cons of each test, and how often to be tested. Which test to use depends on:
• Your preferences. • Your medical condition. • The likelihood that you will get the test. • The resources available for testing and follow-up.
Which Test is Best?
CDC - Colorectal Cancer Screening Tests. (2016). Cdc.gov. Retrieved 6 September 2016, from hIp://www.cdc.gov/cancer/colorectal/basic_info/screening/tests.htm
Considerations for CRC screening at a population level:
• Accuracy
• Compliance
• Colonoscopy Capacity
• Potential Harms/Cost Burden
Which Test is Best?
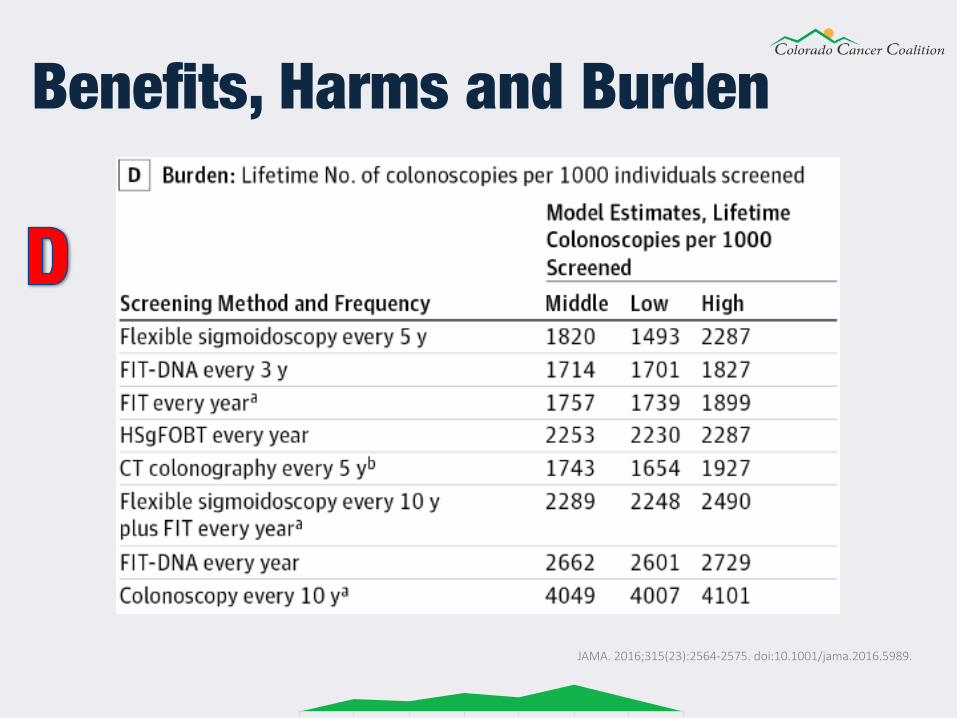
“Outcomes are from Cancer Intervention and Surveillance Modeling Network (CISNET) models, which include the Simulation Model of Colorectal Cancer (SimCRC), the Microsimulation Screening Analysis (MISCAN) for Colorectal Cancer, and the Colorectal Cancer Simulated Population model for Incidence and Natural History (CRC-SPIN).2 Screening occurs between the ages of 50 and 75 years, with follow-up continuing throughout an individual’s remaining life span.”
Benefits, Harms and Burden
JAMA. 2016;315(23):2564-2575. doi:10.1001/jama.2016.5989.
Benefits, Harms and Burden
JAMA. 2016;315(23):2564-2575. doi:10.1001/jama.2016.5989.
Benefits, Harms and Burden
JAMA. 2016;315(23):2564-2575. doi:10.1001/jama.2016.5989.
Benefits, Harms and Burden
JAMA. 2016;315(23):2564-2575. doi:10.1001/jama.2016.5989.
Benefits, Harms and Burden
JAMA. 2016;315(23):2564-2575. doi:10.1001/jama.2016.5989.
Pros and Cons of Each Screening Strategy
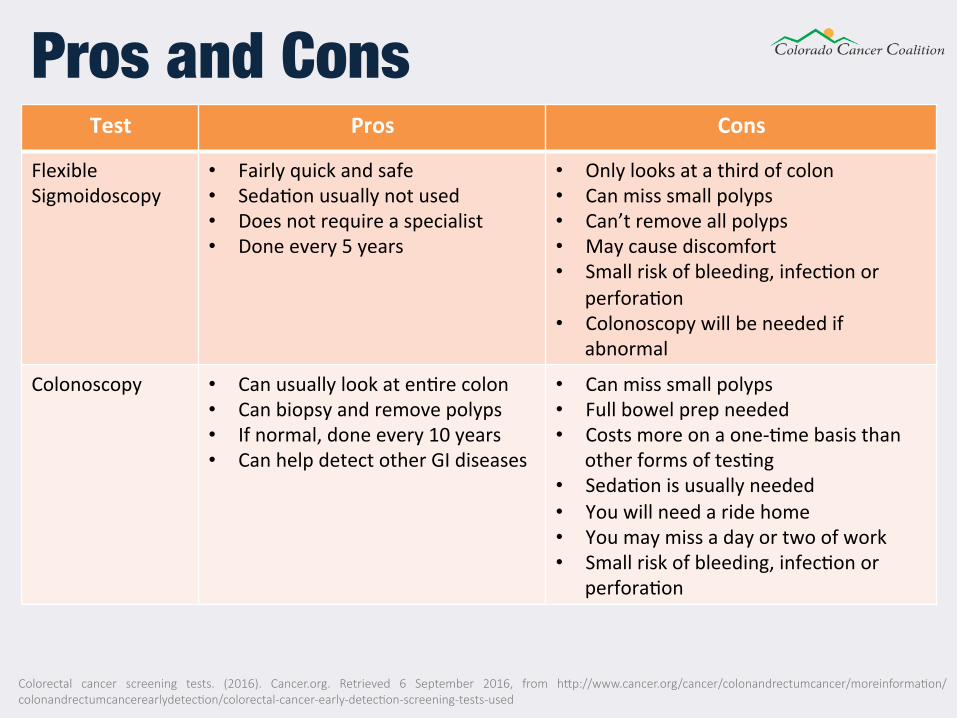
Test Pros Cons
FlexibleSigmoidoscopy
• Fairlyquickandsafe• Seda2onusuallynotused• Doesnotrequireaspecialist• Doneevery5years
• Onlylooksatathirdofcolon• Canmisssmallpolyps• Can’tremoveallpolyps• Maycausediscomfort• Smallriskofbleeding,infec2onor
perfora2on• Colonoscopywillbeneededif
abnormal
Colonoscopy • Canusuallylookaten2recolon• Canbiopsyandremovepolyps• Ifnormal,doneevery10years• CanhelpdetectotherGIdiseases
• Canmisssmallpolyps• Fullbowelprepneeded• Costsmoreonaone-2mebasisthan
otherformsoftes2ng• Seda2onisusuallyneeded• Youwillneedaridehome• Youmaymissadayortwoofwork• Smallriskofbleeding,infec2onor
perfora2on
Pros and Cons
Colorectal cancer screening tests. (2016). Cancer.org. Retrieved 6 September 2016, from hIp://www.cancer.org/cancer/colonandrectumcancer/moreinforma-on/colonandrectumcancerearlydetec-on/colorectal-cancer-early-detec-on-screening-tests-used
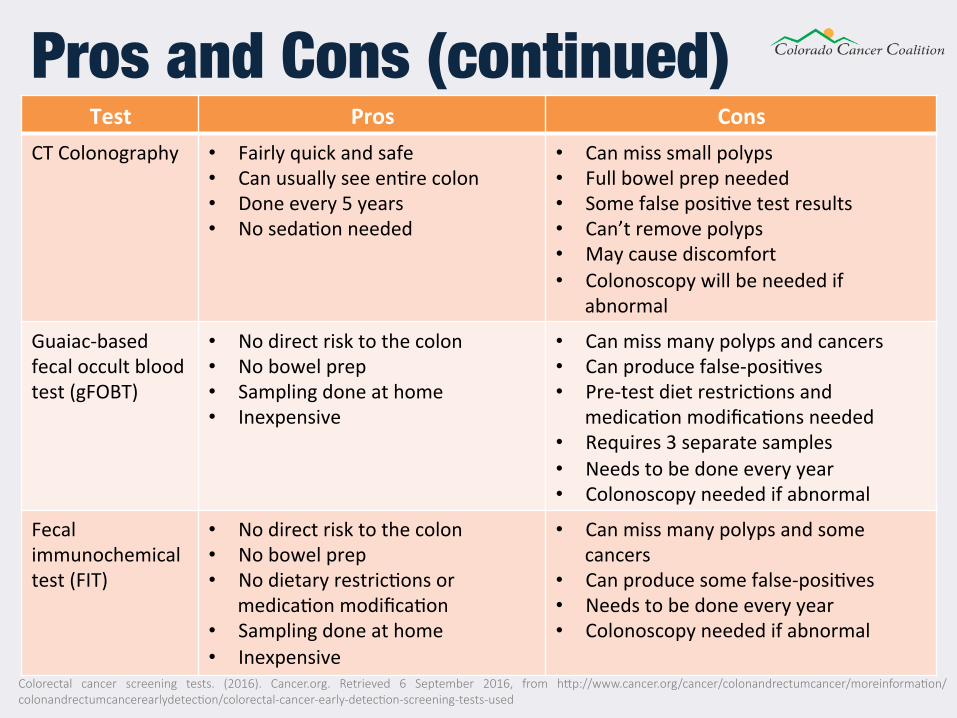
Test Pros ConsCTColonography • Fairlyquickandsafe
• Canusuallyseeen2recolon• Doneevery5years• Noseda2onneeded
• Canmisssmallpolyps• Fullbowelprepneeded• Somefalseposi2vetestresults• Can’tremovepolyps• Maycausediscomfort• Colonoscopywillbeneededif
abnormal
Guaiac-basedfecaloccultbloodtest(gFOBT)
• Nodirectrisktothecolon• Nobowelprep• Samplingdoneathome• Inexpensive
• Canmissmanypolypsandcancers• Canproducefalse-posi2ves• Pre-testdietrestric2onsand
medica2onmodifica2onsneeded• Requires3separatesamples• Needstobedoneeveryyear• Colonoscopyneededifabnormal
Fecalimmunochemicaltest(FIT)
• Nodirectrisktothecolon• Nobowelprep• Nodietaryrestric2onsor
medica2onmodifica2on• Samplingdoneathome• Inexpensive
• Canmissmanypolypsandsomecancers
• Canproducesomefalse-posi2ves• Needstobedoneeveryyear• Colonoscopyneededifabnormal
Pros and Cons (continued)
Colorectal cancer screening tests. (2016). Cancer.org. Retrieved 6 September 2016, from hIp://www.cancer.org/cancer/colonandrectumcancer/moreinforma-on/colonandrectumcancerearlydetec-on/colorectal-cancer-early-detec-on-screening-tests-used
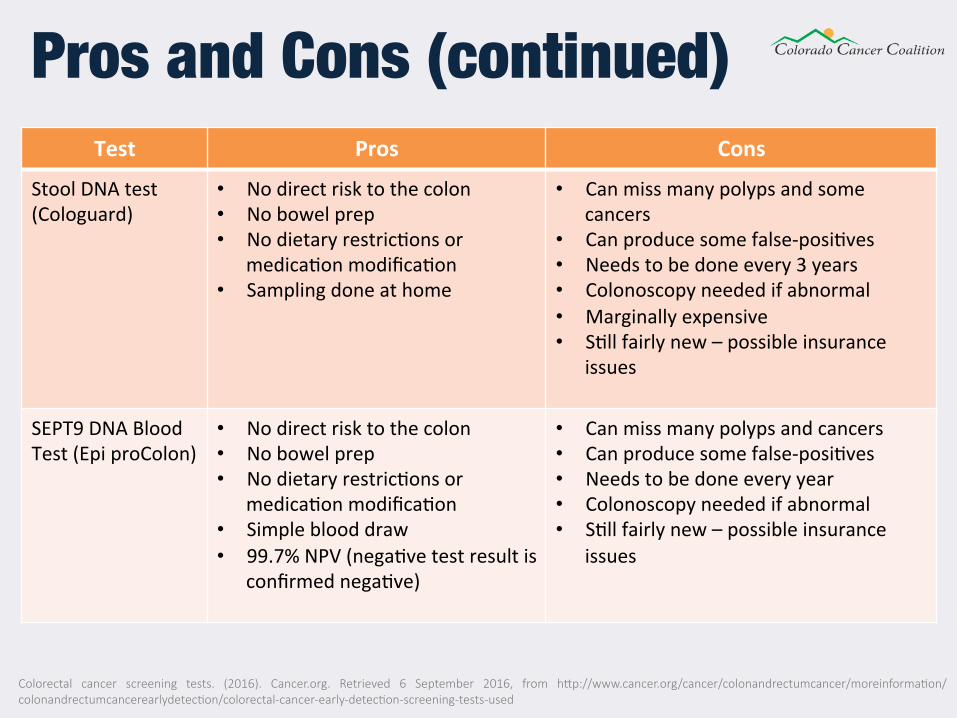
Test Pros Cons
StoolDNAtest(Cologuard)
• Nodirectrisktothecolon• Nobowelprep• Nodietaryrestric2onsor
medica2onmodifica2on• Samplingdoneathome
• Canmissmanypolypsandsomecancers
• Canproducesomefalse-posi2ves• Needstobedoneevery3years• Colonoscopyneededifabnormal• Marginallyexpensive• S2llfairlynew–possibleinsurance
issues
SEPT9DNABloodTest(EpiproColon)
• Nodirectrisktothecolon• Nobowelprep• Nodietaryrestric2onsor
medica2onmodifica2on• Simpleblooddraw• 99.7%NPV(nega2vetestresultis
confirmednega2ve)
• Canmissmanypolypsandcancers• Canproducesomefalse-posi2ves• Needstobedoneeveryyear• Colonoscopyneededifabnormal• S2llfairlynew–possibleinsurance
issues
Pros and Cons (continued)
Colorectal cancer screening tests. (2016). Cancer.org. Retrieved 6 September 2016, from hIp://www.cancer.org/cancer/colonandrectumcancer/moreinforma-on/colonandrectumcancerearlydetec-on/colorectal-cancer-early-detec-on-screening-tests-used