Embed Size (px)
DESCRIPTION
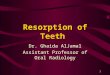
Odontoclasts are multinucleated cells that destroy part or all of the affected tooth’s hard tissue. Odontoclastic resorption starts in the cementum (i.e., a bone-like tissue that covers the tooth root) and spreads into the dentin via dentinal tubules. The destroyed root surface is replaced by cementum. Enamel becomes involved secondary to the “caving in” of underlying dentin, creating a resorption lesion. Feline odontoclastic resorption is a common syndrome affecting cat teeth. Feline odontoclastic resorption lesions (FORLs) have been referred to as cavities, neck lesions, cervical line or neck erosions, oral or odontoclastic resorption lesions (ORLs), and external odontoclastic resorption lesions (EORLs).
Citation preview

WHAT ARE ODONTOCLASTICRESORPTION LESIONS?
Odontoclasts are multinucleatedcells that destroy part or all of theaffected tooth’s hard tissue.Odontoclastic resorption starts in thecementum (i.e., a bone-like tissue thatcovers the tooth root) and spreads intothe dentin via dentinal tubules. Thedestroyed root surface is replaced bycementum. Enamel becomes involvedsecondary to the “caving in” ofunderlying dentin, creating a resorptionlesion. Feline odontoclastic resorptionis a common syndrome affecting catteeth. Feline odontoclastic resorptionlesions (FORLs) have been referred toas cavities, neck lesions, cervical line orneck erosions, oral or odontoclasticresorption lesions (ORLs), and externalodontoclastic resorption lesions(EORLs).
Surface resorption of root cementum
ALSO IN THIS ISSUE:
Ask the Vet ................................ 5
Intraoral Imaging Techniques..... 6
� Stage 1—Lesions extend only intothe cementum covering the root. Thisstage occurs subgingivally where thetooth surface is exposed to cells thatcan become odontoclasts. Becausethere is no enamel involvement, Stage1 lesions are difficult to detect; theyare not radiographically apparent.
� Stage 2—Lesions progress throughthe cementum into the dentin of theroot or crown but do not expose thepulp. Stage 2 lesions are painfulbecause dentin tubules are exposed.Hyperplastic gingiva may cover thesedefects. Enamel may be affected from
N O V E M B E R 2 0 0 6 V O L U M E 4 , N U M B E R 4
leads to reparative formation of bone orcementum-like tissue. The initialcementum resorption extends into thedentin, forming resorption channels thatoften extend into the dentin of thecrown. The loss of crown dentin increasesthe fragility of the tooth and theunsupported enamel. Alternatively, theenamel is also resorbed. Eithermechanism results in the classic clinicalpresentation, a cavity filled withconnective tissue.
CLASSIFICATION OFODONTOCLASTICRESORPTION LESIONS
There are several systems in use toclassify resorption lesions. One method isto characterize the lesions into threestages: acute, chronic, and remodeling.
Another system is based on clinicaland radiographic examination of theFORL:
Feline Odontoclastic Resorption LesionsJan Bellows, DVM, DAVDC, DABVPHometown Animal Hospital and All Pets Dental ClinicWeston, Florida
A NEWSLETTER OF PRACTICAL MEDICINE FOR VETERINARY PROFESSIONALSA NEWSLETTER OF PRACTICAL MEDICINE FOR VETERINARY PROFESSIONALS

2 HARTZ® COMPANION ANIMALSM • NOVEMBER 2006 • VOL. 4, NO. 4
Consulting Editors
Bruce TrumanSenior DirectorAnimal Health and NutritionThe Hartz Mountain Corporation
Jill A. Richardson, DVMDirectorConsumer RelationsThe Hartz Mountain Corporation
Associate Editor
David LevyAssistant ManagerAnimal Health and NutritionThe Hartz Mountain Corporation
HARTZ® COMPANION ANIMALSM
is produced for The Hartz Mountain Corporation by Veterinary Learning Systems, 780 Township Line Rd.,Yardley, PA 19067.
Copyright © 2006 The Hartz Mountain Corporation. All rights reserved.
Hartz® and other marks are owned byThe Hartz Mountain Corporation.
Printed in U.S.A. No part of thispublication may be reproduced in anyform without the express writtenpermission of the publisher.
For more information on The HartzMountain Corporation, visitwww.hartz.com.
N O V E M B E R 2 0 0 6 V O L U M E 4 , N U M B E R 4
A NEWSLETTER OF PRACTICAL MEDICINE FOR VETERINARY PROFESSIONALS
odontoclasts of the periodontium orsubjacent dentin (Figure 1).
� Stage 3—Lesions progress into thepulp of the root canal or pulpchamber and are painful. Bleeding onprobing and spontaneous fracture ofthe crown (enamel and dentin) can beseen (Figure 2).
� Stage 4—Lesions destroy a significantamount of the crown (Figure 3).
� Stage 5—Lesions have significantroot replacement resorption withhealing of the gingiva. There will notbe any clinically apparent tooth tissue.
Some also classify FORLs based onthe radiographic appearance of theperiodontal ligament space:
� Type 1—Lesions are caused byinflammation (periodontitis,endodontic disease). The root appearsnormal, and periodontal ligamentspace is still observable. Themandibular molar is most commonlyaffected (Figure 4).
� Type 2—The affected tooth isankylosed to the alveolus. Type 2lesions are not associated withperiodontitis; instead, noninflammatoryreplacement resorption results inankylosis (surface and/or replacementresorption in which the bone andtooth substance become fused).Type 2 lesions most commonly affect the mandibular third premolars(Figure 5).
WHAT CAUSES FELINEODONTOCLASTICRESORPTION LESIONS?
The cause of odontoclastic resorptionis not known. Histologically, there is nodecalcification in the dentin, suggestingthat the resorption lesions are not similarto human dental caries most often causedby Streptococcus mutans. Theories includeincreased calcium in feline diets andabnormal pressure on the affected teeth as well as feline leukemia andimmunodeficiency disease. The etiologyis unknown but is likely multifactorial.
A recent investigation of factorscontrolling calcium homeostasis in catswith and without FORLs has shown thatserum hydroxy vitamin D concentrationis elevated in cats with FORLs and thatcats with FORLs may have been fed dietswith excessive vitamin D content. Afactor that creates abnormal formation ormineralization of cementum couldprecipitate the development of cementalresorptions. Experimental studies of the
Figure 1. (A) Stage 2 FORL. (B) Radiograph of Stage 2 FORL.
A B

dental effects of vitamin D toxicosis inother species show effects similar to thoseseen in cats with FORLs.
HOW ARE FELINEODONTOCLASTICRESORPTION LESIONSDIAGNOSED?
Most affected cats do not showclinical signs. Some cats may experiencehypersalivation, oral bleeding, or difficultychewing. Affected cats may pick up anddrop food (especially hard food) wheneating; others hiss while chewing.
Behavior changes, such as becomingreclusive or aggressive, have been noted insome cats with FORLs.
A cotton-tipped applicator applied tothe suspected FORL (Stages 2 through4) usually causes pain evidenced by jawspasms.
FORLs can occur above or below the free gingival margin. Most occur at the labial or buccal surface near thecementoenamel junction where the freegingiva meets the tooth surface; calculusand hyperplastic gingival tissue mayobscure the lesion.
FORLs can be found on any tooth;the mandibular third premolar and molarare most commonly affected, followed bythe maxillary third and fourth premolars.
With the cat under general anesthesia,lesions can be examined with an explorer;a fine Shepherd’s hook type is preferred.The explorer helps identify subgingivallesions coronal to the alveolar bone; thefurcation area is a frequent site, and theexaminer must distinguish a resorptionlesion from disease limited to alveolarbone loss.
The lesions can be detected through acombination of visual inspection, tactileexamination with a dental explorer, andradiography.
Radiography will identify lesions that are localized to the root surfaceswithin the alveolar bone, which may not be detected by clinical methods.Consequently, radiography is required todiagnose FORLs. Complete surveyintraoral radiographs are recommended
for cats presented for an oral assessment,treatment, and prevention visit.
Radiographic appearance varies fromminute radiolucent defects of the toothprimarily at the cementoenamel junctionto internal resorption and ankylosis of theapex to the supporting bone.
Intraoral films should include:
� Maxillary incisors (one film) � Maxillary canines (two films—one for
each side)
Figure 2. Stage 3 FORL.
HARTZ® COMPANION ANIMALSM • NOVEMBER 2006 • VOL. 4, NO. 4 3
Figure 3. Stage 4 FORL.
Figure 4. (A) Type 1 FORL of themandibular molar. (B) Radiograph ofType 1 lesion with visible periodontalligament space.
A
B
� Maxillary premolars and molars (twofilms—one for each side)
� Mandibular incisors (one film) � Mandibular canines (two films—one
for each side) � Mandibular premolars and molars
(two films—one for each side)
ARE ALL CATS EQUALLYAFFECTED?
Reported studies reveal that 20% to72% of cats are affected with FORLs.The reported variance is related todiagnostic methods: Some studies entailvisual confirmation only compared withothers that include visual, tactile, andradiologic examination. Most of thesestudies have shown an increasedincidence with increasing age.
The mandibular third premolars arethe most commonly affected teeth(Figure 6). Often, both sides are affected.
TREATMENTThe first step in treatment of an
odontoclastic resorption–affected tooth is proper diagnosis. Under general
Figure 5. Type 2 FORL.

anesthesia, suspected lesions should beexamined with a fine Shepherd’s hooktype of explorer. The furcation area(where tooth roots meet) is a frequentsite of lesions, and the examiner mustdistinguish between a resorption lesionand disease limited to alveolar bone losssecondary to periodontal disease. This isespecially true for the mandibular molar,where the furcation is distally located
compared with othermultirooted teeth.After clinical andtactile examination,intraoral radiographsare taken to evaluateroot structure andinvolvement of thepulp chamber.
FORLs areconsidered to beprogressive and can bepainful to the patient.
For Type 1 lesions in which theperiodontal ligament is observable onradiographs, the recommended treatmentis flap exposure followed by full crownand root extraction. Type 2 lesions invarious stages of ankylosis are treatedeither by conservative management untilthe lesion penetrates into the oral cavityor, preferably, by crown amputation viaflap exposure and flap closure, leaving
ankylosed root(s) to continue fusing withthe alveolar bone.
PREVENTIONTo date, there is no known proven
method to prevent FORLs. Once adefinitive etiology is determined,methods of prevention will hopefully bedeveloped.
SUGGESTED READINGLyon KF: Odontoclastic resorptive lesions, in August JR
(ed): Consultations in Feline Internal Medicine, ed 5.St. Louis, Elsevier Science, 2006.
Lyon KF: Subgingival odontoclastic resorptive lesions.Classification, treatment, and results in 58 cats. VetClin North Am Small Anim Pract 22(6):1417–1432,1992.
Reiter AM, Lewis JR, Okuda A: Update on the etiologyof tooth resorption in domestic cats. Vet Clin NorthAm Small Anim Pract 35(4):913–942, 2005.
Reiter AM, Mendoza KA: Feline odontoclasticresorptive lesions—An unsolved enigma in veterinarydentistry. Vet Clin North Am Small Anim Pract32(4):791–837, 2002.
Figure 6. Multiple FORLs on the mandibular third premolar.

ASK THE VETQ
A
Additional newsletters may be obtained by contacting us at [email protected] or by phone at 800-275-1414.
Jill A. Richardson, DVM, is Director of Consumer Relations atThe Hartz Mountain Corporation.
I have two dogs that I have been giving rawhidefor many years. I recently spoke with anotherveterinarian who informed me that rawhide isvery dangerous and is made with arsenic andformaldehyde. Now I am worried! Can you pleasehelp clear this up?
Rawhide was first introduced as a pet treat in the 1950s asa way of satisfying a dog’s natural need to chew. Rawhidecan provide the chewing satisfaction that dogs crave and,when used daily, can also effectively remove plaque andtartar. You may find the following information aboutrawhide useful.
What is rawhide?Rawhide is simply the inner layer of cattle hide. Duringprocessing, cattle skin is split into an inner and an outer layer.The outer layer is tougher and is used in the leather industry forsuch items as shoes and clothing. The inner layer is softer and isformed into various shapes for dog rawhide chews. Since it ismade from cattle hide, rawhide is not recommended for animalswith beef allergies.
How is Hartz® rawhide manufactured?The inner layer of the hide comes in raw and is cleaned with a food-grade prewash. It is later treated with food-gradewhitening and antibacterial agents. Afterward, it is rinsedthoroughly and rolled through a ringer. It is then formed intoshapes and oven dried. To ensure the highest quality andsanitation, samples of the product are tested before, during, andafter the process by members of the Hartz Quality ControlTeam.
Arsenic, formaldehyde, or other dangerous chemicals are notused in processing Hartz rawhide.
How safe is rawhide? The Hartz Mountain Corporation prides itself on providing thehighest quality rawhide. As previously stated, testing of rawhidetakes place before, during, and after the production process. Qualitycontrol continues through product monitoring and inspection.
Rawhide is considered highly digestible. In a study on the
efficacy of rawhide published in the Journal of the AmericanVeterinary Medical Association, dogs were fed three rawhidestrips per day for 3 weeks, and no adverse effects from chewingand/or consuming rawhide were noted.1 Also, undigested piecesof rawhide were not found in the feces of any of the studydogs.
What are the nutritional values for rawhide?Rawhide is approximately 80% to 85% protein, 10% to 12%fiber and moisture, and 1% to 2% fat. Rawhide is notconsidered a food item, but for those counting calories, rawhidehas about 130 calories per ounce.
How does rawhide help keep teeth clean?Dogs have a natural instinct for chewing. Giving a dog rawhidetreats to chew helps keep their teeth and gums healthy. Theabrasive action of rawhide chewing helps reduce plaque andcalculus. Rawhide also provides the necessary chewing exerciseto strengthen gums and is a great way to relieve boredom,frustration, or anxiety.
How effective is rawhide at cleaning a dog’s teeth?Rawhide has been shown to be an effective way of decreasingplaque and calculus formation. In fact, according to a study,rawhide effectively decreased plaque by 25% when given dailyas a treat.1
Rawhide coated with HMP (hexametaphosphate) is evenmore effective at reducing tartar formation on dogs’ teeth thanregular rawhide. HMP is classified as a food additive and worksby interfering with the mineralization of plaque, therebypreventing accumulation and tartar formation. It can also helpsoften and remove existing tartar. According to a study byHartz, when dogs chewed rawhide coated with HMP, plaquewas decreased up to 83%.2
What is the difference between basted and infusedrawhide?Basted rawhide has flavor coating on the outside of the rawhide.Infused rawhide has flavor infused throughout. Infused rawhide isproduced using a patented process in which chicken stock isinfused throughout the entire hide to increase the flavor and enticedogs to chew longer. According to a Hartz study, dogs preferinfused rawhide 20 to 1 over unflavored rawhide.
HARTZ® COMPANION ANIMALSM • NOVEMBER 2006 • VOL. 4, NO. 4 5
(continues on back cover)

Figure 3. Projectionfor maxillary premolarsand molar. (A) Thetubehead should be centeredover the side of the cat’s facejust below the lateralcanthus. The mesial edge ofthe cone is near the medialcanthus, and the distal edgeof the cone is at the base ofthe ear. The arrow depictsthe direction of the primaryx-ray beam. Size 2 or 4intraoral film can be used toview the entire upper lateraldentition. (B) The cat’s head should be placed in ventral recumbency and a small roll inserted under the neck to keep the hard palate parallel to the tabletop. Size 2 or 4 intraoral film can then be placed under the hard palate. The x-ray cone should be directed downward at an approximate angle of 30˚ to thehorizontal plane of the table top or hard palate to minimize superimposition of the zygomatic arch. The primary x-ray beam should not be perpendicular tothe bisecting plane.
Figure 2. Lateraloblique projection formaxillary canine teeth. (A)The tubehead should becentered over the uppercanine tooth and adjacentpremolars. The arrow depictsthe direction of the primaryx-ray beam. Size 2 intraoralfilm is recommended forcats. (B) The cat’s headshould be placed in ventralrecumbency and a rollpositioned under the jaw tokeep the hard palate parallelto the table top. Size 2intraoral film can then beplaced under the canine tooth and premolars. The x-ray cone should be horizontally directed at an angle of 45˚ as shown and tipped downward at an angleof 45˚ to 60˚ to the horizontal plane of the hard palate. The primary x-ray beam will be almost perpendicular to the bisecting plane.
Figure 1. Projectionfor maxillary incisors. (A)The tubehead should becentered over the upperincisors. The arrow depictsthe angle of the primary x-ray beam. Size 2 film isrecommended for viewingall of the upper dentition tothe level of the firstpremolar. Size 4 film canalso fit in a cat’s mouth ifpreferred. (B) The cat’s headshould be placed in ventralrecumbency with a small rollinserted under the chin tokeep the hard palateparallel to the table top. Size 2 or 4 intraoral film can then be placed below the incisors and canine teeth. The x-ray cone should be directed downward atan angle of 60˚ to the horizontal plane or the hard palate. The primary x-ray beam will be almost perpendicular to the bisecting plane.
6 HARTZ® COMPANION ANIMALSM • NOVEMBER 2006 • VOL. 4, NO. 4
Intraoral Imaging Techniques*
B
B
B
IMAGE FIELD AND FILM PLACEMENT PATIENT POSITIONING
Film
Film
*From: Intraoral imaging techniques, in Mulligan TW, Aller SA, Williams CA: Atlas of Canine & Feline Radiography. Yardley, PA, VeterinaryLearning Systems, 1998, pp 27–44. The book can be purchased online at www.vlsstore.com or by calling 800-426-9119.
Film
A
A
A

HARTZ® COMPANION ANIMALSM • NOVEMBER 2006 • VOL. 4, NO. 4 7
Figure 6. Lateralprojection for mandibularpremolars and molar(parallel technique). (A) The tubehead should be centered over themandibular premolars andmolar. Size 2 intraoral film isrecommended. (B) The cat’shead should be placed inlateral recumbency and aspacer inserted under thejaw to keep the hard palateperpendicular to the planeof the table top. Size 2intraoral film can then beplaced in the vestibulebetween the tongue and mandible, making sure that the film does not traumatize the symphyseal area during insertion and removal. The x-ray cone shouldbe positioned perpendicular to the film and teeth at an angle of about 60˚ to the horizontal plane or table top. The primary x-ray beam will be almostperpendicular to the film and teeth.
Figure 5. Lateraloblique projection formandibular canine teeth.(A) The tubehead should becentered over the mandibularcanine tooth. The arrowdepicts the direction of the x-ray beam. Unlike obliqueprojection in dogs, thepremolars and canine teethdo not usually becomesuperimposed for radiographsof cats. The view shows theinterdental (interproximal)bone of the canine tooth andthird premolar. Size 2intraoral film isrecommended. (B) The cat’s head should be placed in dorsal recumbency and a roll positioned under the neck to keep the hard palate parallel to the table top.Size 2 intraoral film can then be placed under the canine tooth and third premolar. The x-ray cone should be directed toward the interproximal space of thelateral incisor and canine tooth as shown and tipped downward at an angle of 45˚ to 60˚ to the hard palate. The primary x-ray beam will be almost perpendicularto the bisecting plane. Gauze sponges can be used to stabilize the film in the back of the mouth. All sponges and the film should be removed at the same time.
Figure 4. Projectionfor mandibular incisorsand canine teeth. (A) Thetubehead should be centeredover the lower incisors. Thearrow depicts the directionof the primary x-ray beam.Size 2 intraoral film isrecommended forradiographs of the entirelower dentition to the canineteeth; however, size 4 filmcan be used if preferred. (B)The cat’s head should bepositioned in dorsalrecumbency and a small rollinserted under the neck tokeep the hard palate parallel to the table top. Intraoral film can then be placed below the incisors and canine teeth. The x-ray cone should be directed at anapproximate angle of 60˚ to the horizontal plane of the hard palate or table top. The primary x-ray beam will be almost perpendicular to the bisecting angle.
B
B
B
IMAGE FIELD AND FILM PLACEMENT PATIENT POSITIONING
Film
Film
A
Film
A
A

ASK THE VET (continued from page 5)
Veterinary Learning Systems780 Township Line RoadYardley, PA 19067
PRST STDU.S. POSTAGE
PAIDYORK, PA
PERMIT #200
402348
Which Hartz products have the Veterinary Oral HealthCouncil acceptance seal?The Veterinary Oral Health Council (VOHC) exists to recognizeproducts that meet standards of plaque and calculus retardation in dogsand cats. Products are awarded the VOHC Seal of Acceptance followingreview of data from trials conducted according to VOHC protocols. TheVeterinary Oral Health Council has given its seal of acceptance to theHartz® Chew-Dent™ Infused Rawhide product for dogs.
How do you choose the appropriate rawhide for a dog?There are many shapes and flavors of rawhide available on themarket. Choosing rawhide with HMP will help provide better dentalbenefits. Also, dogs with tendencies for food aggression should begiven any treat, including rawhide, cautiously and never in thepresence of other animals.
The following quick guide can help you choose the correct treat foryour pet:
• Pencil-shaped rawhides—Smaller dogs like to chew on oneend while holding the other end with their paws. The pencil tiphelps clean teeth when the dog chews on it.
• Bone-shaped rawhides—Last longer than sticks or chips.Thicker bones can keep a dog chewing longer.
• Chips—Quick chewy treats that can be given as rewards. The chipsare usually eaten more quickly than the bone-shaped rawhides.
• Braided rawhides—Longer lasting and have the stick shape thatdogs love.
• Twists with two different flavors—Provide twice the flavorand are longer lasting than plain strips.
• Munchy rawhide treats—Quick crunchy treats that are greatfor senior pets because they are easier to chew.
• Long rawhide rolls—Dogs enjoy “fetching” these like theywould a stick.
• Pressed rawhides—Made from layers of rawhide skin pressedtogether by a machine; these are great for very aggressivechewers, as the rawhide is compressed and keeps the dogchewing longer.
How can I learn more about rawhide and dental care for dogs?If you would like to receive copies of the Hartz® Dental Brochuresand free samples of Hartz® Dental rawhide products, you can call800-275-1414 (9 AM to 5 PM EST) or email [email protected].
REFERENCES1. Effect of chewing rawhide and cereal biscuit on removal of dental calculus
in dogs. JAVMA 197(2):213–219, 1990.2. Effect of sodium hexametaphosphate on dental calculus formation in
dogs. Am J Vet Res 56(7):913–918, 1995.