Embed Size (px)
Citation preview


PhysiologyAcid-Base
Birgland Joseph, MD

pH of Body Fluids• normal range of arterial pH is 7.37 to 7.42• Acidemia: arterial pH is less than 7.37• Alkalemia: Arterial pH is greater than 7.42• Conc. of H⁺ is responsible for acid-base status• In arterial blood
– the H+ concentration is 40 × 10-9 equivalents per liter (or 40 nEq/L),
• Mechanisms of maintaining normal pH – buffering of H+ in both ECF &ICF – respiratory compensation– renal compensation

Relationship between [H+] and pH

Acid Production in the Body
• Types of Acids– Volatile acid
• CO₂• Produced from aerobic metabolism• CO₂ combines with H₂O to form the weak acid H₂CO₃⁻, which
dissociates into H⁺ and HCO₃⁻
• Carbonic anhydrase catalyzes the reversible reaction b/t CO₂ and H₂O
– Non-volatile acid• aka fixed acids• Sulfuric acid, phosphoric acid• ~ 40 -60 mmoles/day is produced• Ketoacids, lactic acid, β-hydroxybutyric acid, glycolic acid, oxalic
acid & salicylic acid: over produced in disease or ingested

Buffers
• Prevents change in pH when H⁺ ions are added to or removed from a sol.
• Most effective within 1.0 pH unit of the pK (–ve logarithm of the [H⁺] at which ½ of the acid molecules are dissociated
and are undissociated)of the buffer – i.e; in the linear portion of the titration curve
• Types– Extracellular– Intracellular

• Extracellular buffers– Mostly HCO3-, which is produced from CO2 and H2O
• pK of CO2/HCO3- buffer pair is 6.1
– Phoshate • Minor buffer• pK of H2PO4-/HPO4- is 6.8• Most important as a urinary buffer
– Excretion of H+ is called titratable acid
• Intracellular buffers– Organic phosphates
• AMP, ADP, ATP, DPG
– Proteins– Hemoglobin: major buffer
• Deoxyhemoglobin is better buffer than oxyhemoglobin

Henderson-Hasselbalch Equation
• Used to calculate pH
– where • pH = -log10 [H+] (pH units) • pK = –ve logarithm of the [H⁺] at which ½ of the acid
molecules are dissociated and are undissociated• [A-] = Concentration of base form of buffer (mEq/L); is the
H acceptor• [HA] = Concentration of acid form of buffer (mEq/L); is the
H donor• When the conc. of A- and Ha are equal, the pH of
the sol. = the pH of the buffer

Ex of cal• SAMPLE PROBLEM
– The pK of the HPO4-2/H2PO4
- buffer pair is 6.8. Answer two questions about this buffer: (1) At a blood pH of 7.4, what are the relative concentrations of the acid form and the base form of this buffer pair? (2) At what pH would the concentrations of the acid and base forms be equal?
• SOLUTION– The acid form of this buffer is H2PO4
-, and the base form is HPO4
-2.The relative concentrations of the acid and base forms are set by the pH of the solution and the characteristic pK.

• Answering the first question: The relative concentrations of acid and base forms at pH 7.4 are calculated with the Henderson-Hasselbalch equation. (Hint: In the last step of the solution, take the antilog of both sides of the equation!)
•
•Therefore, at pH 7.4, the concentration of the base form (HPO4
-2) is approximately fourfold that of the acid form (H2PO4
-).

• Answering the second question: The pH at which there would be equal concentrations of the acid and base forms can also be calculated from the Henderson-Hasselbalch equation. When the acid and base forms are in equal concentrations, HPO4
-2/H2PO4- =
1.0.
•
•The calculated pH equals the pK of the buffer. This important calculation demonstrates that when the pH of a solution equals the pK, the concentrations of the acid and base forms of the buffer are equal. As discussed later in the chapter, a buffer functions best when the pH of the solution is equal (or nearly equal) to the pK, precisely because the concentrations of the acid and base forms are equal, or nearly equal.

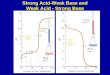
Titration Curves• Describes how the pH of a buffered sol. changes as H ions are
added to it or removed from it• As H⁺ ions are added to the sol., the HA form is produced• As H⁺ ions are removed, the A⁻ form is produced• A buffer is most effective in the linear proportion of the
titration curve, where the addition of removal of H causes little change to pH– Most effective physiologic buffer will have a pK with 1.0 pH unit of 7.4
(7.4 ±1.0)– Outside of the effective range addition of removal of H⁺ changes sol.
drastically• Based on Henderson-Hasselbalch Equation, when the pH of
the sol. = pK, the conc. of HA and A are equal

Figure 7-2 Titration curve of a weak acid (HA) and its conjugate base (A-). When pH equals pK, there are equal concentrations of HA and A-.

ECF & ICF buffers
• ECF buffers– Bicoarbonate– phosphate
• ICF– Organic phosphate– proteins

Figure 7-3 Comparison of titration curves for H2PO4-/HPO4
-2 and CO2/HCO3
-. ECF, Extracellular fluid

Figure 7-4 Acid-base map. The relationships shown are between arterial blood PCO2, [HCO3
-], and pH.

Renal Acid-Base
• Reabsorption of HCO₃⁻• Figure 7-5 Mechanism for reabsorption of filtered HCO3
- in a cell of the proximal tubule. ATP, Adenosine triphosphate.

Regulation of filtered HCO₃⁻• Filtered load
– Increases in the filtered load leads to increased HCO₃⁻ reabsorption. – If plasma [HCO3} becomes high (metabolic alkalosis), then filtration
will exceed reabsorption and excretion will occur• PCO₂
– ↑ PCO₂ → ↑ HCO₃⁻ reabsorption; d/t ↑ICF [H⁺] for secretion– ↓ PCO₂ → ↓ HCO₃⁻ reabsorption; d/t ↓ICF [H⁺] for secretion
• ECF volume– Expansion → ↓ HCO₃⁻ reabsorption– Contraction → ↑ HCO₃⁻ reabsorption (contraction alkalosis)
• Angiotensin II– Stimulates Na⁺-H⁺ exchange and thus increases HCO₃⁻ reabsorption– Contributes to contraction alkalosis secondary to ECF vol. expansion

Excretion of Fixed H⁺
• Excretion of H⁺ as titratable acid (H₂PO₄⁻)• Figure 7-6 Mechanism for excretion of H+ as titratable acid.
ATP, Adenosine triphosphate

• Excretion of H⁺ as NH4 (ammonium)• Figure 7-8 Mechanism of excretion of H+ as NH4
+. In the proximal tubule, NH3 is produced from glutamine in the renal cells, and NH4
+ is secreted by the Na+-H+ exchanger. In the collecting ducts, NH3 diffuses from the medullary interstitium into the lumen, combines with secreted H+ in the lumen, and is excreted as NH4
+. ATP, Adenosine triphosphate.

Acid-Base Disorders– Metabolic Acidosis– Metabolic alkalosis– Respiratory acidosis– Respiratory Alkalosis
– Anion gap

Figure 7-10 Values for simple acid-base disorders superimposed on acid-base map.

• Metabolic Acidosis – Over-production or injestion of fixed acid or loss
of base (↓HCO₃⁻) produces and increase in arterial [H⁺] (acidemia)
– Primary disturbance = ↓[ HCO₃⁻]– HCO₃⁻ is used to buffer the extra acid– Compensation
• Respiratory compensation = hyperventilation (kussmaul breathing – deep rapid respiration, common in type 1 diabetics d/t keto acids)
• Renal compensation = – ↑ excretion of H⁺ as titratable acid & NH₄– ↑”new” HCO₃⁻ reabsorption
• Chronic metabolic acidosis = adaptive ↑ in NH₃ synthesis

Table 7-4. Causes of Metabolic Acidosis
Cause Examples Comments
Excessive production or ingestion of fixed H+ Diabetic ketoacidosis Accumulation of β-OH butyric acid and acetoacetic acid
↑ Anion gap
Lactic acidosis Accumulation of lactic acid during hypoxia
↑ Anion gap
Salicylate poisoning Also causes respiratory alkalosis
↑ Anion gap
Methanol/formaldehyde poisoning Converted to formic acid
↑ Anion gap
↑ Osmolar gap
Ethylene glycol poisoning Converted to glycolic and oxalic acids
↑ Anion gap
↑ Osmolar gap
Loss of HCO3- Diarrhea Gastrointestinal loss of HCO3
-
Normal anion gap
Hyperchloremia
Type 2 renal tubular acidosis (type 2 RTA) Renal loss of HCO3- (failure to reabsorb filtered HCO3
-)
Normal anion gap
Hyperchloremia
Inability to excrete fixed H+ Chronic renal failure ↓ Excretion of H+ as NH4+
↑ Anion gap
Type 1 renal tubular acidosis (type 1 RTA) ↓ Excretion of H+ as titratable acid and NH4+
↓ Ability to acidify urine
Normal anion gap
Type 4 renal tubular acidosis (type 4 RTA) Hypoaldosteronism
↓ Excretion of NH4+
Hyperkalemia inhibits NH3 synthesis
Normal anion gap

• Serum anion gap– Represents unmeasured anions in serum
• Phosphate, Citrate, Sulfate, protein– Anion gap = [Na⁺] – ([Cl⁻] + [HCO₃⁻])– Normal = 8 - 16 mEq/L– In Metabolic acidosis, as HCO₃⁻ decreases, an
anion such as Cl⁻ must be increased for electro-neutrality.
– ↑s by an ↑ in conc. of unmeasured anions (eg. phoxphate, lactate) to replace HCO₃⁻
– Hyperchloremic metabolic acidosis: Cl⁻ (unmeasured anion) is increased to replace HCO₃⁻ with a normal anion gap

• Metabolic Alkalosis– Loss of fixed H⁺ or gain of base → ↓ arterial [H⁺]
(alkalemia)– Primary disturbance = ↑ [HCO₃⁻]
• Eg vomiting: lost of H⁺ in gastric acid, leaving behind HCO₃⁻ in blood
– Compensation• Respiratory Comp.: hypoventilation• Renal comp: ↑ HCO₃⁻ excretion
– Filtered load exceeding reabsorption rate
– If ECF vol. contraction occurs, HCO₃⁻ reabsorption will ↑, worsening the metabolic alkalosis

Table 7-5. Causes of Metabolic Alkalosis
Cause Examples Comments
Loss of H+ Vomiting Loss of gastric H+
HCO3- remains in the blood
Maintained by volume contraction
Hypokalemia
Hyperaldosteronism Increased H+ secretion by intercalated cells
Hypokalemia
Gain of HCO3- Ingestion of NaHCO3
-
Milk-alkali syndrome (chronic disorder of the kidney; induced by large amounts of alkali and calcim in the Rx of peptic ucler, can progress to renal failure)
Ingestion of large amounts of
HCO3- in conjunction with renal
failure
Volume contraction alkalosis Loop or thiazide diuretics ↑ HCO3- reabsorption due to ↑
angiotensin II and aldosterone

Figure 7-11 Generation and maintenance of metabolic alkalosis with vomiting. ECF, Extracellular fluid

• Respiratory Acidosis– D/t ↓ respiratory rate and retention of CO₂– Pimary disturbance = ↑ arterial CO₂ → ↑[H⁺]– Compensation
• No resp. compensation• Renal comp
– ↑ excretion of H⁺ as titratable H⁺ and NH₄– ↑reabsorption of “new” HCO₃⁻
– Acute resp. acidosis: renal comp. has not yet occurred
– Chronic resp. acidosis: renal comp.

Table 7-6. Causes of Respiratory Acidosis
Cause Examples Comments
Inhibition of the medullary respiratory center Opiates, barbiturates, anestheticsLesions of the central nervous system
Central sleep apnea
Oxygen therapy Inhibition of peripheral chemoreceptors
Disorders of respiratory muscles Guillain-Barré syndrome, polio, amyotrophic lateral sclerosis (ALS), multiple sclerosis
Airway obstruction Aspiration
Obstructive sleep apnea
Laryngospasm
Disorders of gas exchange Acute respiratory distress syndrome (ARDS) ↓ Exchange of CO2 between pulmonary
capillary blood and alveolar gas
Chronic obstructive pulmonary disease (COPD)
Pneumonia
Pulmonary edema

• Respiratory Alkalosis– d/t ↑ respiratory rate (hyperventilation)– Primary disturbance = ↓ PCO₂– Compensation
• No resp. comp.• Renal comp.
– ↓H⁺ excretion– ↑HCO₃⁻ excretion
– Acute resp. alkalosis: renal compensation has not yet occurred
– Chronic resp. alkalosis: renal comp.

Table 7-7. Causes of Respiratory Alkalosis
Cause Examples Comments
Stimulation of the medullary respiratory center
Hysterical hyperventilationGram-negative septicemia
Salicylate poisoning Also causes metabolic acidosis
Neurologic disorders (tumor; stroke)
Hypoxemia High altitudePneumonia; pulmonary embolism
Hypoxemia stimulates peripheral chemoreceptors
Severe anemia
Mechanical ventilation

Table 7-2. Summary of Acid-Base Disorders
Disorder CO2 + H2O →← H+ + HCO3-
Respiratory Compensation
Renal Compensation or Correction
Metabolic Acidosis
↓ ↑ ↓ Hyperventilation
↑ HCO3-
reabsorption (correction)
Metabolic Alkalosis
↑ ↓ ↑ Hypoventilation
↑ HCO3-
excretion (correction)
Respiratory Acidosis
↑ ↑ ↑ None ↑ HCO3-
reabsorption (compensation)
Respiratory Alkalosis
↓ ↓ ↓ None ↓ HCO3-
reabsorption (compensation)
Bold arrows indicate initial disturbance.