Embed Size (px)
DESCRIPTION
we are in a financially unsustainable position - some of these slides are most sobering
Citation preview

HFMA – Western Pennsylvania Chapter
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved. 0
Kaufman Hall Point of View Discussion
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved.
Pittsburgh, Pennsylvania / July 19, 2011

HFMA – Western Pennsylvania Chapter
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved. 1
Discussion Outline
• Background – What Is Driving Our “Point of View”
• Kaufman Hall’s Point of View
• Best Practices for Positioning Your Organization for Success

HFMA – Western Pennsylvania Chapter
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved. 2
Background – What Is Driving Our “Point of View”

HFMA – Western Pennsylvania Chapter
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved. 3
The Word of the Moment in Healthcare Is “Unsustainable”
As in:
þ The size of the federal budget deficit is unsustainable
þ The annual increase in the Medicare budget is unsustainable
þ The percentage of healthcare spending to GDP is unsustainable

HFMA – Western Pennsylvania Chapter
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved. 4
Federal Government Outlays and Revenues (% of GDP) CBO Scenario Based on Expected Law
2010 through 2040

HFMA – Western Pennsylvania Chapter
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved. 5
Projected National Health Expenditures under ACA*Expenditures projected to increase 85 percent from 2009 to 2019
Source: Andrea M. Sisko, Christopher J. Truffer, Sean P. Keehan, John A. Poisal, M. Kent Clemens, and Andrew J. Madison. “National Health Spending Projections: The Estimated Impact of Reform Through 2019,” Health Affairs, no. 10 (2010):1933-1941. * Used September 2010 projections from CMS: Office of the Actuary.
$ billions

HFMA – Western Pennsylvania Chapter
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved. 6
Family of Four – Total PPO Cost Versus Median Family Income
% of Income 15% 18% 26% 45% 42% 38%
Sources: PPO cost 2002-2011, Milliman; median family income 2002-2011, Census Bureau.Notes: 2011 family income is an estimate for Federal FY12; total PPO cost = employer contribution, employee payroll deduction, and employee out-of-pocket co-pays/deductibles. Numbers rounded to nearest hundred.

HFMA – Western Pennsylvania Chapter
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved. 7
Costs by Age CategoriesHeathcare Costs by Age
$-
$5,000
$10,000
$15,000
$20,000
$25,000
$30,000
$35,000
$40,000
$45,000
0 10 20 30 40 50 60 70 80 90
Age
Ann
ual p
er c
apita
hea
lthca
re c
osts
UKGermanySwedenUSSpain
U.S. is spending much more for older ages
Source: Fischbeck, Paul. “US-Eruope Comparisons of Health Risk for Specific Gender-Age Groups” Carnegie Mellon University; September, 2009.

HFMA – Western Pennsylvania Chapter
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved. 8
Healthcare Reform Is Back on the Table – Driven by Concerns Over the Federal Deficit and State Budget Challenges
• Recent Gallup poll put “Federal spending and the budget deficit” as the #2 concern of Americans, surpassed only by “the economy”
• Standard & Poor’s issues a negative outlook on U.S. “AAA” credit rating for the first time in history
• Both democrats and republicans agree on the need for significant deficit reductions, but have strong differences of opinion on how to get there
• You don’t have to be a political scientist to recognize that healthcare reform legislation will be altered, and is a moving target
• You don’t have to be a math wizard to understand that Medicare and Medicaid funding are prime targets and that providers will likely absorb the brunt of the reductions
Sources: Gallup Poll, March 21, 2011. www.gallup.com/poll/146708/Americans-Worries-Economy-Budget-Top-Issues.aspx; Standard & Poor’s: AAA Rating on USA Affirmed; Outlook Revised to Negative, Apr. 18, 2011.

HFMA – Western Pennsylvania Chapter
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved. 9
The Model for Healthcare Reform (Massachusetts) Is Ahead of the Curve…Lessons to Be Learned
• Massachusetts enacted “Romneycare” in 2006
• According to the Attorney Generals Office of Massachusetts as of June 2011: “We continue to face significant challenges in addressing historic market dysfunction and in shifting how we purchase health care to align payments with “value”… We have only just begun...”
• The United States enacted “Obamacare” in 2010…
Source: Massachusetts Attorney General “Examination of Health Care Cost Trends and Cost Drivers…Report for Annual Public Hearing” June 22, 2011.

HFMA – Western Pennsylvania Chapter
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved. 10
• The challenges of Addressing Market Dysfunction and Promoting Value-Based Purchasing
– There is wide variation in the payments made by health insurers to providers that is not adequately explained by differences in quality of care
– Globally paid providers do not have consistently lower total medical expenses
– Total medical spending is on average higher for the care of health plan members with higher incomes
– Tiered and limited network products have increased consumer engagement in value-based purchasing decisions
– PPO health plans create significant impediments for providers to coordinate care effectively…
– Health care provider organizations designed around primary care can coordinate care effectively…
Source: Massachusetts Attorney General “Examination of Health Care Cost Trends and Cost Drivers…Report for Annual Public Hearing” June 22, 2011.
The Model for Healthcare Reform (Massachusetts) Is Ahead of the Curve…Lessons to Be Learned (continued)

HFMA – Western Pennsylvania Chapter
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved. 11
• “We believe that policymakers should focus on…the twin goals of improving market function and encouraging care coordination” by:
– Promote tiered and limited network products– Reduce health care price distortions through temporary statutory
restrictions until tiered and limited network products and commercial market transparency can improve market function
– Encourage consumers to select a PCP who can assist in coordinating care
– Promote coordination of patient care through primary care providers including the infrastructure necessary to coordinate care and by giving providers timely access to relevant patient data regardless of their size or payment methodology
– Develop reports for providers and the public to guide development of patient care
– Develop appropriate regulations, solvency standards, and oversight for providers who contract to manage the risk of insured and self-insured populations
The Model for Healthcare Reform (Massachusetts) Is Ahead of the Curve…Lessons to Be Learned (continued)
Source: Massachusetts Attorney General “Examination of Health Care Cost Trends and Cost Drivers…Report for Annual Public Hearing” June 22, 2011.

HFMA – Western Pennsylvania Chapter
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved. 12
Kaufman Hall’s Point of View

HFMA – Western Pennsylvania Chapter
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved. 13
What Is Likely to Occur with Healthcare Reform as a Result of the Changing Climate
• Near term – moderate to severe reductions in provider reimbursement− Across the board hits – ready, fire, aim given the need for
rapid action?
− Targeted cuts with consideration to key political constituents?
• State government will play a larger role in defining how reform policy advances are executed
• Near/ intermediate/ long term – the evolution of the reimbursement model will continue to advance from an activity-based to a value-based system – driven by both private and public initiatives

HFMA – Western Pennsylvania Chapter
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved. 14
Implications for Providers – What Do We Know• Near-term success will be dependent on the ability to change cost
structure this means more than the usual re-engineering and will also require reduction in utilization (Brown University/ University of Miami SCM research)
• Longer-term success will be dependent on the ability to deliver value(measurable and demonstrated quality/ cost)…creating this value will require unrelenting innovation in service organization and delivery models
• A new set of core competencies will be required to achieve the above • In essence, we are faced with a manufacturing problem• Provider industry aggregation seems inevitable given this set of
core competencies and this manufacturing problem• Over the long term, healthcare organizations will likely fall into three
broad categories – population health managers, major participants/ components, contracted providers
• Standing still is not a viable option

HFMA – Western Pennsylvania Chapter
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved. 15
An Urgent Need: Rethinking Care Delivery
“In my 30 years with Sutter Health, I’ve never experienced a more urgent situation… I’ve also never been more confident that, together, we will rethink the way we deliver healthcare –by becoming even more efficient and more innovative. Our path is clear; deliver high-quality medical services as cost effectively as possible.”
Pat Fry, Sutter Health President and CEO
Source: Sutter Health, a publication for employees, physicians and volunteersFebruary 2011, Volume 6, Issue 1.

HFMA – Western Pennsylvania Chapter
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved.
Integration Attributes Key Characteristics of the Best Prepared
Physician/ Hospital IntegrationA highly aligned medical staff characterized by shared goals, outcomes-based contractual arrangements, significant planning input, and adequately represented in organizational governance
Care Coordination/ Management Capability
Use of care coordination tools and processes by an empowered and integrated workforce to meet performance goals that are regularly measured and reported
Information Systems Sophistication
An IT platform that supports clinical decision making, information management, facile communications, and access by all stakeholders (physicians, patients, administration) to proper treatment and strategic decision making
Service Distribution System Effectiveness
A rational service distribution system that has accessible primary care and easy access (both physically and through referrals) across the care continuum, delivered in contemporary facilities with contemporary equipment
Cost ManagementA right-sized organization-wide cost structure, highlighted by appropriate levels of staffing, capital spending, overhead support, and supply chain costs; constantly reviewed based on comparative peer group studies and benchmarks
Scale and Market Essentiality Sufficient scale to attract competitive clinical and administrative talent, realize economies, drive marketplace innovation, and be an essential provider to health plans and patients
Brand Identification Well recognized and respected, associated with high-quality and service excellence.
Payor Relationships/ Contracts Maintaining strong relationships with payors and the ability to negotiate support for “new era” business practices
Financial Strength/ Capital Capacity
Strong appeal to capital markets through sustained operations, revenue growth, and balance sheet strength
New Core Competencies Will Be Required of Hospitals and Health Systems for Success in the Future
16

HFMA – Western Pennsylvania Chapter
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved. 17
How Have Other Industries Solved a Manufacturing Problem?
• Product standardization
• Process automation and standardization (to reduce product variation)
• Application of labor saving technologies
• Matching labor input requirements to the task
• Amassing highly talented product and process design teams
• Leveraging scale economies in purchasing, supply chain management, and corporate overhead

HFMA – Western Pennsylvania Chapter
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved.
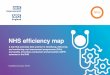
The Hospital/ Health Provider Industry Is Highly Fragmented
18
11.5%
21.7%
32.1%
54.9%
68.0%
94.1%
70.6%
92.5%
0%
25%
50%
75%
100%
Top 5 Top 15 Top 5 Top 15 Top 5 Top 15 Top 5 Top 15
Industry Leaders’ Market Share
Hospitals Microchip Manufacturing
Airlines Retail Pharmacy
11.5%
21.7%
32.1%
54.9%
68.0%
94.1%
70.6%
92.5%
0%
25%
50%
75%
100%
Top 5 Top 15 Top 5 Top 15 Top 5 Top 15 Top 5 Top 15
Industry Leaders’ Market Share
Hospitals Microchip Manufacturing
Airlines Retail Pharmacy

HFMA – Western Pennsylvania Chapter
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved. 19
Takeaways from Past Industry Consolidation
• Access to capital is a key competitive advantage cited in the majority of cases
• Consolidation is common in mature markets at end of growth curve
• Consolidation is common in industries in which there is a shift in the revenue model
• Consolidation provides industries with overcapacity a passive way to phase out underutilized or inefficient resources
• Sophisticated information systems are expensive, but highly leverageable and improve the ability of organizations to realize efficiencies in both contiguous and non-contiguous markets
• Regulatory policy influence can be a key enabler or deterrent to industry consolidation

HFMA – Western Pennsylvania Chapter
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved.
Focus on Retail Pharmacy• The incorporation of a pharmacy benefit in
health insurance plans shifts payment responsibility from the consumer to the insurer
• Insurers utilize their leverage and negotiate lower drug prices with retail pharmacies for their enrollment base
• Broad geographic coverage (scale) and brand recognition become essential attributes for retail pharmacy success in order to negotiate sustainable rates
• Sophisticated IT becomes imperative for interface with commercial and governmental programs and now consumers
• Scale becomes imperative to drive operating costs to their lowest possible level
• The independent retail pharmacy all but disappears
20
Source: “Pharmaceutical Marketplace Dynamics: Expenditures, Distribution, Coverage, Pricing.” National Association of Chain Drug Stores. May 2000. “History of the Digest.” National Community Pharmacists Association. 2001. “Consolidation of US Retail Pharmacy Industry. TATA Consultancy Services. August 2009.

HFMA – Western Pennsylvania Chapter
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved. 21
Other Implications for Providers
• There is, and there likely will continue to be, a lot of uncertainty in the environment regarding:
− The predominant forms/ mechanisms that will prevail related to value-based reimbursement (i.e., rewards/ penalties for quality or absence of quality; bonuses for cost effectiveness; bundled payments; capitation)
− Who will lead the reorganization of the healthcare market –hospitals and health systems, IPAs, insurers
• Planning in an uncertain world requires organizations to establish a Point of View

HFMA – Western Pennsylvania Chapter
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved. 22
Best Practices for Positioning Your Organization for Success

HFMA – Western Pennsylvania Chapter
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved. 23
Evaluating the Situation
• Establish a point of view
− Based on a combination of art and science, establish an opinion of where the industry is headed
− Understand the challenges and opportunities
• Develop a sound financial plan and perform scenario/ option analysis as a basis for developing the organization’s future direction

HFMA – Western Pennsylvania Chapter
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved. 24
The Strategic Financial Plan Development Process
Initial Phase Core Analytics Plan
Understand Your Current Position
Develop Sound Baseline Financial Projections
Scenario Planning/ Sensitivity/ Risk
Analysis
Quantify Strategic Initiatives/ Define
Portfolio
• Historical credit profile
• Access to capital• Capital needs
Inventory• Capital Position
Analysis to quantify capital shortfall
• Financial performance comparisons
• Integrate market plans
• Incorporate capital inventory
• Apply “known” future variables.
• Project “business as usual”
• Assess capital capacity and constraints
• Quantify strategic initiatives
• Incorporate “probable” scenarios (e.g., healthcare reform)
• Include committed capital investment plans
• Perform sensitivity analysis
• Assess plan viability• Re-iterate analytic
process
• Evaluate strategic “options” as to future value creation
• Define optimal portfolio of strategies
• Identify and refine implementation plan
• Begin implementation
Key
Proc
esse
sKe
y Obj
ectiv
es

HFMA – Western Pennsylvania Chapter
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved. 25
Be Decisive
Understand your options and take action:• What steps can your organization take to streamline its
cost structure to be as efficient as possible in the new environment?
• Have you planned effectively for POTENTIAL changes in the reimbursement structure/ methodology, and what if they do not occur as “planned?”
• Can the organization stand on its own or do you need a partner?
• What have you not thought about/ factored into your decision making?

HFMA – Western Pennsylvania Chapter
Copyright 2011 Kaufman, Hall & Associates, Inc. All rights reserved. 26
Continually Re-evaluate
Most importantly – The process of strategic financial planning is not a “one-time” exercise:
• Continue to evaluate and modify the direction of the organization as the changes in the industry are coming fast and furious
• Your plans from last year are obsolete
• Your plans today will change in six months, maybe sooner, as more clarity around reform and its ultimate impact become more well defined