Embed Size (px)
DESCRIPTION
Trials with patient reported endpoints are reporting increased efficiencies when using electronic patient reported outcomes (ePRO), compared to paper diary data collection methods. To date, approximately 20% of all trials with patient reported endpoints are using ePRO solutions to collect efficacy data. As the adoption of electronic patient reported outcomes continues to increase, sponsors are finding new ways to justify this technology’s ROI, and identify the types of trials that are best suited to ePRO (versus paper). This article will describe how several market-leading sponsors have quantified the benefits of better data quality, with case examples from recent trials implemented by PHT Corporation (PHT). These analyses are provided with the intention to inform the clinical research community, and provide the frameworks for further ROI determinations.
Citation preview

1. Perfect Patients
complete every fi eld clearly, and
in the proper format. Even in this
rare best case scenario, the only
way to know it was completed at
8:00 pm is because the subject
said so.
2. Forgetful Patients
are a data manager’s dream, but
a clinical researcher’s nightmare.
The worst part is, you have no way
of knowing that you’re losing data
until it’s too late.
3. Selective Patients
force you to make assumptions -
did the subject mean December
or February? Was the medication
taken? Doing anything other
than throwing this away could be
dangerous.
4. Enthusiastic Patients have
tremendous energy and want
to provide as much information
as they can. But it is illogical,
illegible and likely contains AEs.
This is an ideal patient for an
eDiary!
Paper diary examples courtesy of Dr. Stuart Donovan
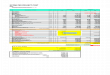
What Does Paper Cost?Most organizations haven’t assigned a cost to paper PROs, unless they’re outsourcing the entire function of data collection and management to CROs. Here are the numbers:
• A typical study includes 250–300 patients who are in trial for 3 months, required to complete 1 diary daily. This translates into 90 diaries per patient.
• Processing each diary involves form creation, printing, translation, binding and shipping to sites; followed by data entry, transfer, reconciliation, queries and changes; and fi nally return shipment. The estimated cost is $20/page.
Per Patient Cost Paper PRO $1800 Per Patient Average Cost PHT ePRO $1300
Electronic capture savings per patient $500
• Average savings on a typical study using ePRO vs. paper is $125,000 – $150,000.
Does ePRO Data Quality Differ from Paper?Improvements in data quality provided by electronic patient-reported outcome systems are widely reported and accepted throughout the clinical research community. Patient diary data collected electronically is time-stamped, legible and logical with real-time validation provided to patients while entering diary information. ePRO supports multi-site international trials with remote data monitoring via the web with real-time status reporting overall and per site, participant status tracking and on-demand subject randomization.
Contrary to paper diaries, ePRO data collection can ensure complete patient responses. With trustworthy data, trial sponsors no longer run the risk of having a promising compound rejected due to unreliable paper PRO data.
How to Quantify ePRO ROI:
Improving Trial Effi ciencies: Making the Business Case for ePRO
PHT Insights — First Quarter 2009
The Four Types of Paper Patients

Enhanced data integrity further enables1. Attributable, legible, contemporaneous, original and accurate (ALCOA) patient data that is complete and time-stamped through the use of alarms, branching logic and edit checks;
2. Reduced data variance for improved quality of study results and reduced number of patients to show effi cacy;
3. Real time access to diary data between visits for enhanced safety and compliance monitoring;
4. Adaptive trial designs with pre-programmed adaptations and reduced standard deviation for more conclusive planned interim analyses; and
5. Libraries of experience and metrics with data including compliance and data variance/standard deviations for specifi c indications.
How Does ePRO Enable Faster Trials?Cycle times and therefore trial times can be reduced with electronic patient-reported outcomes. Electronic data capture eliminates manual data entry times and other data point changes. Final data analysis sets can be provided within days after a trial’s conclusion.
By reducing data variance, fewer patients are required especially in Phase II trials. Scientifi c outcomes are more conclusive, and greater power of study is achieved by reduced standard deviation.
ePRO does not eliminate the need for accurate data review and monitoring, but it does enable trial sponsors to improve power of study with smaller samples, and to reach no-go decisions much faster than they could otherwise.
What is the FDA position on ePRO?The FDA has reviewed ePRO vs. PRO, and cites unsupervised data entry as a major drawback to paper reported outcomes. PRO instruments [paper] that require patients to rely on memory, especially if they must recall over a period of time, or to average their response over a period of time, may threaten the accuracy of the PRO data.
According to the FDA, “If a patient diary or some other form of unsupervised data entry is used, the FDA plans to review the protocol to determine what measures are taken to ensure that patients make entries according to the study design and not, for example, just before a clinic visit when their reports will be collected.”1
The European Medicines Agency (EMEA) has also commented on ePRO vs. PRO, providing this Guidance on endpoints in asthma: “If home recording equipment is used, reproducibility is particularly important and an electronic diary record should be considered to validate the timing of measurements.”2 ; and on effi cacy for steroid contraceptive, “The separate calculation of the Pearl Index for method failure requires reliable methods for recording of compliance (e.g. electronic patient diaries) not to include non-compliers in the denominator.”3
Which Trials are Best Suited for ePRO? Trials with patient-reported endpoints– whether in home or in medical offi ces–report rapid gains in effi ciencies and data integrity with ePRO. Trials within these therapeutic areas (TAs) have been early adopters of ePRO:
• Neurology/CNS• Respiratory• Behavior Modifi cation• Gastrointestinal • Genitourinary• Immunology
PHT has also demonstrated ePRO effi ciencies within
• Oncology• Endocrine and metabolic disorders• Dermatology• Ears, nose, throat, eye and teeth• Musculo-skeletal
Trials across TAs where patient-reported data is sensitive in nature, where it’s critical to track adverse symptoms between visits such as worsening symptoms, rescue medications, specifi c events such as suicide ideation also received increased ROI when utilizing ePRO.
SummarySponsors, trial managers and health outcome directors continue to obtain greater degrees of data quality, program effi ciency and patient safety with ePRO. For more information, contact PHT at 1.877.360.2901.
1) Lines 334-337, ‘Guidance for Industry. Patient-Reported Outcome Measures: Use in Medical Product Development to Support Labeling Claims. DRAFT GUIDANCE.’ U.S. Department of Health and Human Services, Food and Drug Administration, Center for Drug Evaluation and Research (CDER), Center for Biologics Evaluation and Research (CBER), Center for Devices and Radiological Health (CDRH). February 2006 2) Section 8.1, ‘Note for Guidance on the Clinical Investigation of Medicinal Products in the Treatment of Asthma’, The European Agency for the Evaluation of Medicinal Products, Evaluation of Medicines for Human Use, November 2002. 3) Section 3.1, ‘Note for Guidance on Clinical Investigation of Steroid Contraceptives in Women, The European Agency for the Evaluation of Medicinal Products, Evaluation of Medicines for Human Use, February 2000.
2
The FDA approved a Novartis drug for chronic constipation for use with women, but indicated more data would be needed for men. Therefore, Novartis planned another study and estimated a sample size of 1,026 male subjects would be required to prove effi cacy based on traditional paper variance statistics. Subsequently, the pharmaceutical company elected to use PHT’s LogPad® System instead of paper.
Once the study was already underway, the FDA surprised Novartis by deciding to approve the drug for men without further data. Novartis stopped the trial, but allowed the 322 enrolled subjects to complete treatment. To the amazement of the clinical team, study power was reached with 69% fewer subjects - representing less than one-third the planned sample size!
Case Study: Novartis
Study power was
reached with less
than one-third the planned-
sample size!

Case Study: Merck Research Laboratories
Data AnalysisData captured from both arms revealed statistically equivalent means (118 minutes from paper, 109 minutes from the LogPad), but the ranges were different. As shown in Figure 2, the distribution of responses on paper varied widely from -20 to 380. This means one subject claimed to have average 20 minutes less sleep per night, while another reported an additional 6 hours. Further, the distribution tends to cluster around 30-, 60- and 90-minute intervals. This suggests evidence of recall bias, as responses are more general and less precise when made after-the-fact.
Conversely, the LogPad distribution in Figure 3 is much tighter around the mean and more Gaussian, with fewer and less extreme outliers. Meanwhile, continuous responses indicate more accurate data reporting. A visual inspection of Figure 4 shows the comparison of variance.
ResultsAnalysis performed by Merck showed a 35% lower standard deviation for LogPad data as compared to paper. Merck calculated that this reduced variance would have enabled them to reach study power with 56% fewer patients–saving an estimated $340,000 (assuming $6,000 per patient).
In addition, Merck had to process three times more data changes and notifi cation forms to clarify paper data, and incurred 58 hours of data entry compared to zero for the LogPad arm. Compliance was high in both arms (96% for paper, 92% for LogPad), but as discussed earlier only ePRO compliance can be verifi ed as opposed to purported by subjects.
These fi ndings were presented by Jay Pearson, Senior Director at Merck.
3
Figure 2: Paper Distribution Figure 3: LogPad Distribution Figure 4: Distribution Overlay
MORNING QUESTIONAIRE (Continued)8. How would you describe the quality of your sleep last night? (check only one box.)
1= Excellent ❑ 2= Good ❑ 3= Fair ❑ 4= Poor ❑
Figure 1: A study question on the LogPad and paper diary
Merck initiated the fi rst randomized trial to evaluate the relative
capacities of paper diaries and electronic patient diaries
(Figure 1) to prove effi cacy. 101 patients were randomized to two
arms based on data capture method (paper or LogPad) and treated
with an approved drug for insomnia. The study examined primary
endpoint data of change in minutes of sleep time and compared
results from the arms in many categories.

LogPad
SitePad®
StudyWorks®
eSense™ Sensors
ePRO Designer
Study Archive
PROVision™ Scientifi c Services
Trial Success Program™ (TSP)
PHT Support Center
Scientifi c Review and Validation
Site Telecom Assessments
Technology Transfer
PHT LogPad – The mobile Hand Held for home eDiaries
PHT Electronic Patient-Reported Outcome (ePRO) System Components
Read About: Banning Paper DiariesWhy Paper Diaries Should Be Banned in Clinical Trials
Pharmaceutical Executive Europe, March, 2009
PHT author Valdo Arnera, MD, outlines specifi c reasons why pharmaceutical and biotechnology companies should replace paper diaries with ePRO.
Read it online at: www.phtcorp.com.
For more information:US Account Executives: 1.877.360.2910European Account Executives: 41.22.879.91.00
PHT Corporation
500 Rutherford Avenue
Boston, MA 02129 USA
Toll-Free: 877.360.2901
PHT Corporation Sàrl
2, chemin Louis-Hubert
1213 Petit-Lancy, Geneva, Switzerland
Phone: 41.22.879.91.00
Insights Q1 2009
www.phtcorp.com
Copyright © 2010 PHT Corporation
v8.2010
Electronic Patient-Reported Outcome (ePRO) Solutions
“ I believe the SitePad Tablet
is something that can
help our entire industry,
and patients, as well,” says Joachim Löwin,
Clinical Information Science Leader, AstraZeneca.
About PHT CorporationPHT is the global innovator in ePRO (electronic patient-reported
outcome) systems that simplify clinical data management and
streamline eClinical trials. Since 1994, patient experiences
captured by PHT’s ePRO System have been used successfully
in over 440 global trials by more than 100 biopharmaceutical
companies, resulting in at least 14 regulatory submissions
and 11 approvals. By capturing high-quality and time-stamped
assessments, trial sponsors are able to run smaller, safer and
more conclusive clinical research programs resulting in signifi cant
R&D cost savings. For more information, review the educational
content and interactive PHT ePRO System demonstrations at
PHT’s award-winning site www.phtcorp.com.












![I'M A MARKETER, HOW CAN I JUSTIFY MARKETING ROI [INBOUND 2014]](https://img.pdfslide.net/doc/110x75/558a2999d8b42a46028b462a/im-a-marketer-how-can-i-justify-marketing-roi-inbound-2014.jpg)