Embed Size (px)
Citation preview

HYPOXIC CELL SENSITIZERS
Dr Bharti Devnani
Moderator:-Dr Ritu Bhutani

What is the Hypoxic cell sensitizer? What are the characteristics of an ideal Radio sensitizer? Enumerate all Radio sensitizers.

GOAL OF RADIATION THERAPY

CONCEPTS
Two concepts fundamental to understanding the
rationale for modification of radiation response
1. Therapeutic ratio – defined as NTT/TLD
Both of these parameters have sigmoid dose response curves
As the separation between these curves increases, the
likelihood increases that treatment will be effective & not
cause an unacceptable level of morbidity
2. Efficacy & toxicity profile of the modifier – directly affect
TR
A radiosensitizing agent that exacerbates toxicity to same
extent that it improves efficacy – TR unchanged or worsened


RADIOSENSITISERS
Physical and Chemical (pharmacological) agents that increase
the lethal effects of radiation when administered in
conjunction to radiotherapy.

TYPES OF SENSITISERS
Non hypoxic cell sensitisers(Halogenated pyrimidines )
Differential effect is based on the premise that tumor cells cycle faster and therefore incorporate more of the drug than the surrounding normal tissues.
Hypoxic-cell sensitizers
Increase the radiosensitivity of cells deficient in molecular oxygen(tumors) but have no effect on normally aerated cells.

Oxygen fixes the damage by free radical to DNA. (O2 fixation hypothesis)
Why o2 is required?

CHARACTERISTICS OF AN IDEAL HYPOXIC CELL SENSITIZER
1. Selectively sensitize hypoxic cells at concentration that would
result in acceptable normal tissue toxicity (differential effect)
2. Chemically stable & not subject to rapid metabolic break down
3. Highly soluble in water or lipids & must be capable of diffusing
a considerable distance through a nonvascularized cell mass
to reach the hypoxic cell
4. It should be effective at relatively low daily dose /# used in
conventional fractionated radiotherapy

METHODS TO SENSITIZE HYPOXIC CELLS
Physical Chemical

METHODS TO SENSITIZE OR ELIMINATE HYPOXIC CELLS
1. Physical
Overcoming hypoxia by eliminating it with treatment that increases
delivery of oxygen to tumor i.e. increases the oxygen carrying
capacity of blood and increasing the tumor blood flow
a) Hyperbaric oxygen
b) Carbogen with or without nicotinamide
c) ARCON
d) Hyperthermia

METHODS TO SENSITIZE OR ELIMINATE HYPOXIC CELLS2. Chemical
a) Modifiers of Hb
b) Hypoxic cell sensitizers
c) Hypoxic cytotoxins or bioreductive dugs - Pharmacological
targeting of hypoxic cells – cytotoxic to hypoxic tumor cells
d) Biologic modifiers
e) Chemotherapeutic drugs

Physical radiosensitizers

HYPERBARIC OXYGEN
An increase in barometric pressure of the gas breathed by the patient during radiotherapy is termed ‘hyperbaric oxygen (HBO) therapy’.
Pioneered by Churchill-Davidson in 1968 at St. Thomas' Hospital in London.
Patients were sealed in chambers filled with pure oxygen raised to a pressure of 3 atm.

HYPERBARIC OXYGEN

Problems
Feeling of claustrophobia
Unconventional hypofractionated schemes
Increase in late normal tissue damage(damage
to laryngeal cartilage in studies)
Risk of fire
Cumbersome Side effects - damage to the ears, sinuses and
lungs from the effects of pressure, temporary worsening of myopia, acute central nervous system oxygen toxicity (seizures)Discarded due to introduction of better chemical radiosensitisers that would achieve same end by simpler
means

Clinical trial of HBO
largest of the multicentre clinical trials of HBO is performed by the British Medical Research Council.
Results:-Benefit observed in (both LRC & OS) Advanced head and neck cancer Uterine cervix cancer
Benefit was not observed in bladder cancer;Improvement in LRC
(6.6%) & survival


CARBOGEN
Pure oxygen if breathed – vasoconstriction - closing
down of some blood vessels – defeats the object
Carbogen – 95% O2 +5% CO2
Rationale – addition of CO2 to gas breathing mixture -
shift the oxyHb association curve to right – facilitate
unloading of oxygen into most hypoxic tissues
Simple attempt to overcome chronic hypoxia
Can be given under normobaric condition. Failed to show significant therapeutic gain (Horsman et al., 2007).

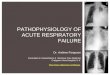
Diffusion limited chronic hypoxiaHypoxia Perfusion limited acute hypoxia

NICOTINAMIDE(B3)
Prevents the transient fluctuations in tumour blood flow that lead to the development of acute hypoxia (Horsman et al.,1990).
Benefit has been seen when combined with Hyperthermia, Perfluorochemical emulsions, Pentoxifylline and High oxygen-content gas breathing (Horsman,1995).

ARCON
Accelerated – to overcome proliferation
Hyperfractionated – to spare late responding normal
tissues
Carbogen breathing – to overcome chronic hypoxia
Nicotinamide – to overcome acute hypoxia



PHASE III TRIAL
Laryngeal carcinoma(Netherland)
Increase in regional control rate 93% v/s 86%(p=.04) With equal toxicity

Chemical sensitizers

Modifiers of hemoglobin

BLOOD TRANSFUSION
Anemia – powerful adverse prognostic factor in pts of Ca
Cervix, H& N cancers & lung cancer
Investigated in no. of studies
1st clinical investigation – in advanced cervical cancer
Transfusion to pts with low Hb levels - ↑ed oxygen tension
within tumor
Transfusion to Hb level of 11g/dl or higher – improved survival
Not been supported by data from controlled randomized trials
H & N Cancer pts – 2 phase II trials from DAHANCA study
group – failed to demonstrate any benefit

ERYTHROPOETIN
Low Hb concentration ↓es radiation response of tumors
Two studies conducted in H & N cancers failed to show any benefit
In one of the studies – pts who received erythropoetin showed
significantly poor outcome than those who did not
? Erythropoietin may stimulate tumor growth
Schedules –
Thrice weekly – 150 U/kg s.c
Weekly - 40000 U s.c.

PERFLUOROCARBONS
Artificial blood substances
Small particles capable of carrying more oxygen or
manipulating the oxygen unloading capacity of blood
Potential usefulness uncertain

HYPOXIC CELL SENSITISERS
Nine different drugs have reached clinical evaluation
Misonidazole, Metronidazole, Benznidazole, Desmethyl-misonidazole Etanidazole, Pimonidazole Nimorazole, Ornidazole Rsu1069

Hypoxic Cell Radiosensitizers
The first candidate to satisfy these criteriawas Misonidazole

Hypoxic Cell Radiosensitizers

METRONIDAZOLE
1st generation 5-nitroimidazole
Sensitizer Enhancement ratio - 1.2
Formulations - 500 mg tablets or 500mg /100 ml solution
Half life – 9.8 hrs
Total cumulative dose not to exceed 54 gm/m2
Multiple doses 6gm/m2 3 times/wk for 3- 4week
Optimal time for administration - 4 hour before
radiation
Dose limiting toxicity –
Gastrointestinal
Sensory peripheral neuropathy

MISONIDAZOLE
2nd generation 2- nitroimidazole
Higher electron affinity
Sensitizer Enhancement ratio – 1.4 with multiple dose of 2 gm/m2 1.15 with 0.5mg/m2
Formulations 500 and 100 mg tablets and capsules
once or twice/wk for 5-6 wks
Total cumulative dose not to exceed 12 gm/m2
Optimal time for administration -- 4 hour before radiation
Dose limiting toxicity- gastrointestinal Sensory peripheral neuropathy that progress to
central nervous system toxicity

DAHANCA 2
DAHANCA 2, showed a highly significant improvement in thestratification subgroup of pharynx tumors, but not inthe prognostically better glottic carcinomas

ETANIDAZOLE (SR2508)
3rd generation, analog of Misonidazole
SER- 2.5-3 with dose of 12 g/m2
Arthralgia seen more often with 48 hr continuous infusion
1000mg/19.4 ml saline solution
Total dose - 40.8 g/m2 at 1.7-2g/m2 3 times/wk for 6 wks
30 min before radiationLesser neurotoxic due to
Shorter half life
Lower lipid solubility(less rapidly taken by the neural
tissue)No significant benefit was observed in two large head and neck cancer trials, one in the USAand the other in Europe.

ETANIDAZOLE
RTOG phase III study with Etanidazole in head and neck tumors
n- 521 patients
Conventionally fractionated RT RT
with Etanidazole 2mg/m2 with out Etanidazole
three times wk
No grade III or IV central nervous system or peripheral neuropathy was observed.
The 2-year actuarial local tumor control was 40% in each arm, and the survival was 41% and 43%, respectively, in the irradiation alone and the irradiation plus etanidazole arms
No overall benefit when Etanidazole
added to conventional radiotherapy

PIMONIDAZOLE
4- nitroimidazole
More potent than Misonidazole Uncharged at acid pH, thus promoting its accumulation in
ischaemic regions of tumours.
Several – fold ↑ in tumor concentration
Maximum tolerated dose – 750 mg/m2
Dose limiting toxicity – CNS manifesting as disorientation & malaise A pimonidazole trial was started in uterine cervix, but was stopped
when it became evident that those patients who received pimonidazole showed a poorer response.

NIMORAZOLE
A 5-nitroimidazole of same structural class as metronidazole
Administered in form of gelatin-coated capsules containing 500
mg active drug
Given orally 90 min prior to irradiation.
Daily dose 1200 mg/m2 body surface
Total dose should not exceed 40g/m2 or 75 g in total.
Less effective radio sensitizer then Misonidazole or Etanidazole
Less toxic, no cumulative neuropathy
Large dose can be given
dose-limiting toxicity is nausea and vomiting

NIMORAZOLE

NIMORAZOLE – DAHANCA 5
Significant improvement in terms of LRC & OS
Nimorazole significantly improves the effect of radiotherapeutic management of supraglottic and pharynx tumors and can be given without major
side-effects

As a consequence, nimorazole has now become part of the standard treatment schedule for head and neck tumours in Denmark.

DEVELOPMENT OF NITROIMIDAZOLES
Metronidazole
Misonidazole more active, toxic, benefit in subgroup
Etanidazole less toxic, not active
Nimorazole less active, much less toxic, benefit in H& N cancer

Summary of nitroimidazoles trials

NEWER NITROIMIDAZOLES
Doranidazole promising preliminary results were obtained
in a phase III study with intraoperative radiotherapy in advanced pancreatic cancer
Sanazol which in an International Atomic Energy
Agency multicentre randomized trial (Dobrowsky et al., 2007) in cervical cancer was found to significantly increase local control and survival following radical radiotherapy

OVERGAARD META-ANALYSIS 10,779 patients 83 RCT Hyperbaric oxygen (HBO) (28 trials), Hypoxic radiosensitizers (52 trials), Oxygen or carbogen breathing (3 trials), Blood transfusion (1 trial).
The tumor sites were Bladder (16 trials), Uterine cervix (15 trials), Central nervous system (13 trials), Head and neck (24 trials), Lung" (11 trials), Esophagus (2 trials), Mixed (2trials).

RESULTS OF META-ANALYSIS
Statistically significant benefit in LRC(4.7%) & OS (2.7%)

Locoregional tumor control was stastically significant in H&N (p=0.0002)

Hypoxic cytotoxins

HYPOXIC CYTOTOXINS BIOREDUCTIVE DRUGS
Elimination of radioresistant hypoxic cells by selectively killing them.
These compounds undergo intracellular reduction to form active cytotoxic species, primarily under low oxygen tensions.
Maximum cytotoxicity to cells at maximum distance from
tumor blood vessels
Overcome major cause of resistance of solid tumors –
inadequate oxygenation & drug delivery to tumor cells distant
to blood vessel

HYPOXIC CYTOTOXINS
Quinone antibiotics
• MMC• EO9• porfirom
ycin
Nitroaromatic compounds
• Misonidazole
• (Rb-6145)
• Nlcq-1, Cb1954, Sn23862
• Pr-104

QUINONE ANTIBIOTIC - MITOMYCIN C
Prototype bioreductive drug
Used as chemotherapy agent for many years
Cytotoxic to relative radio resistant hypoxic cells
But the differential cytotoxicity between hypoxic and
oxygenated cells , however is small
Acts as an alkylating agent after intracellular activation &
inhibits DNA – DNA cross linking, DNA depolymerization
Dose limiting toxicity – cumulative myelosuppression
Mitomycin C plays an important role in conjunction with
radiotherapy and 5FU, the definitive, chemoradiation
squamous cell carcinoma of the anus

PORFIROMYCIN
A mitomycin C derivative
Provides greater differential cytotoxicity between hypoxic and
oxygenated cells in vitro
Phase III study
Compared patients treated with conventionally fractionated
radiation plus mitomycin C versus radiation plus porfiromycin
The median follow-up - >6 years. Hematologic and non-
hematologic toxicity was equivalent in the two treatment arms
Mitomycin C was superior to porfiromycin with respect to 5-
year local relapse-free survival (91.6% vs. 72.7%; p = 0.01)

Local-regional relapse-free survival (82% vs. 65.3%; p =
0.05)
Disease-free survival (72.8% vs. 52.9%; p = 0.03)
There were no significant differences between the two
arms with respect to overall survival (49% vs. 54%) or
distant metastasis-free rate (80% vs. 76%)
Their data supported the continuing use of mitomycin C as
an adjunct to radiation therapy in advanced head and neck
cancer and will become the control arm for future studies
PORFIROMYCIN…

TIRAPAZEMINE (SR 4233) Highly selective toxicity against hypoxic cells both in vivo and
vitro
MOA- Drug is reduced by intracellular reductases to form highly
reactive radical - produces both double & single strand breaks in
DNA
Analysis of DNA and chromosomal breaks after hypoxic exposure
to Tirapazemine suggests that DNA double-strand breaks are the
primary lesion causing cell death
Efficacy depends on no. of effective doses that can be
administered during course of RT & presence of hypoxic tumor
cells
S/E – nausea & muscle cramping

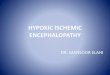
TIRAPAZEMINE
Hypoxic/cytotoxicity ratio –
ratio of drug concentration under
aerated and hypoxic condition
required to produce same cell
survival
Unlike the oxygen-mimetic
sensitizers, tirapazamine-
mediated therapeutic
enhancement occurs both when
the drug is given before or after
irradiation.
Tirapazamine can also
enhance the cytotoxicity of
cisplatin

N= 121 STAGE III/IV SCC OF THE HEAD AND NECK RANDOMIZED TO RECEIVE DEFINITIVE RADIOTHERAPY (70 GY IN 7 WEEKS)
Tirapazamine On day 2 of weeks 1, 4, and 7,290 mg/m2 was administered for 2 hours, followed 1 hour later by cisplatin 75 mg/m2 for 1 hr
followed immediately by radiotherapy
In addition, tirapazamine 160 mg/m2 was given before radiation three times/week in weeks 2 and 3
Cisplatin 50 mg/m2 was given before radiotherapy on day 1 of weeks 6 and 7 of radiotherapy
and
Fluorouracil 360 mg/m2/d was given by continuous infusion from day 1 - 5 (120-hour infusion) of weeks 6 and 7 of radiotherapy
Arm 2. n-58Arm 1,n-62


Three-year failure-free survival rates were 55% with TPZ/CIS
and 44% with chemo RT( p .16)
Three-year locoregional failure-free rates were 84% in
the TPZ/CIS arm and 66% in the chemo RT arm (p .069)
Toxicity
More febrile neutropenia and grade 3 or 4 late mucous
membrane toxicity were observed with TPZ/CIS
Compliance with protocol treatment was satisfactory on both
arms

Markers of hypoxic cells

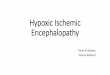
MARKERS OF HYPOXIC CELLS
Radioactive labeled nitroimidazoles
Bioreduction Deposition
of radionuclide
Quickly excretedWithout
breaking down
Hypoxia Aerobic tissue

RADIOACTIVE LABELED NITROIMIDAZOLES
Nitroimidazole can be labeled with I 123
Hypoxic region of tumour can be visualized with single
photon emission computed tomography
Now, tumor Hypoxia can be detected by [18F]-Misonidazole
Positron Emission( FMISO-PET) in Patients With Advanced
Head and Neck Cancer imaging
Noninvasive procedure that can be used as predictive assay
in individual patients
The availability of methods to detect significant areas of
hypoxia can allow selection of patients who may benefit from
method of overcoming hypoxia

CONCLUSION 1896 -First radiotherapy treatment. 1909 -First clinical observation by Gollwald Schwarz
showing Reduced blood flow caused radioresistance. 1953- First experimental observation of potential
importance of hypoxia in radiotherapy. 1955 -First observation of hypoxia in human tumors. 1955 -First hyperbaric treatment. 1968- Results from first randomized trial. 1976 -First randomized study with hypoxie
radiosensitizer. 19,95- More than 10000 patients in 83 randomized
trials. Metaanalysis shows highly significant survival and local control benefit.
2013- Still no impact on general dinical practice.

NOVEL DRUGS
5 promising redox modulators are in development.
Tirapazamine AQ4N RSR13 facilitates delivery of oxygen to
tumor cells, thereby rendering them more sensitive to radiation.
Motexafin gadolinium, with a porphyrin-like structure, selectively accumulates in tumor cells and thereby enhances radiation-induced DNA damage.
HIF-1 inhibitors target a transcription factor that regulates hypoxia related events and cell survival.

HIF-1 TARGETING AGENTS
Soluble guanylyl cycle activators (e.g., YC-1) (84, 85),
HSP90 inhibitors (e.g., geldanamycin radicicola) (80, 81, 86),
PI3K inhibitors (e.g., wortmannin, LY294002) mTOR inhibitors(e.g., Rapamycin, CCI-779) Microtubule modifiers (e.g., 2-
methyloxyestradiol, vincristine,Taxol) topoisomerase I inhibitors