Embed Size (px)
Citation preview

1
Reproductive HealthReproductive HealthAdvisory CommitteeAdvisory Committee
September 30, 2003September 30, 2003
Pamela Williamson Joyce, RACPamela Williamson Joyce, RACVice President, Regulatory AffairsVice President, Regulatory Affairs
& Quality Assurance – US& Quality Assurance – USSerono, Inc.Serono, Inc.
NDA NDA ##21-32221-322

2
Proposed Indication – LuverisProposed Indication – Luveris®®
Luveris® (lutropin alfa for injection) administered with follitropin alfa for injection,
is indicated for stimulation of follicular development in infertile hypogonadotropic
hypogonadal women with profound LH deficiency (LH < 1.2 IU/L)*
** The indication presented in the NDA was amended on August 21, 2003 to be consistent with The indication presented in the NDA was amended on August 21, 2003 to be consistent with the indication as currently approved for Luveristhe indication as currently approved for Luveris®® in the European Union and other countries in the European Union and other countries outside of the United Statesoutside of the United States

3
AgendaAgenda
Introduction and Introduction and Regulatory HistoryRegulatory History
Pamela Williamson Joyce, RACPamela Williamson Joyce, RACVice President, Regulatory Affairs & Quality Vice President, Regulatory Affairs & Quality
Assurance Assurance – US– USSerono, Inc.Serono, Inc.
Need for and Role of LH: Need for and Role of LH: HH Women with Profound HH Women with Profound Gonadotropin DeficiencyGonadotropin Deficiency
Jerome Strauss, M.D., Ph.D.Jerome Strauss, M.D., Ph.D.Luigi Mastroianni Jr. ProfessorLuigi Mastroianni Jr. Professor
Director, Center for Research on Director, Center for Research on Reproduction and Women’s HealthReproduction and Women’s Health
University of PennsylvaniaUniversity of Pennsylvania
LuverisLuveris®® Clinical Development Clinical Development ProgramProgram
Paul Lammers, M.D.Paul Lammers, M.D.Chief Medical OfficerChief Medical OfficerSerono, Inc.Serono, Inc.
Clinical Perspective and Clinical Perspective and Risk/Benefit AssessmentRisk/Benefit Assessment
Nanette F. Santoro, M.D.Nanette F. Santoro, M.D.Professor and Director, Division of Professor and Director, Division of
Reproductive EndocrinologyReproductive EndocrinologyDepartment of Obstetrics and Gynecology Department of Obstetrics and Gynecology
and Women’s Healthand Women’s HealthAlbert Einstein College of MedicineAlbert Einstein College of Medicine
Summary and ConclusionsSummary and Conclusions Pamela Williamson Joyce, RACPamela Williamson Joyce, RACSerono, Inc.Serono, Inc.

4
LuverisLuveris®® (lutropin alfa for injection) (lutropin alfa for injection)
• Luteinizing hormone produced by recombinant Luteinizing hormone produced by recombinant DNA technologyDNA technology
• Common namesCommon names– Recombinant human luteinizing hormoneRecombinant human luteinizing hormone– r-hLHr-hLH
• Lyophilized powder in 75 IU vialsLyophilized powder in 75 IU vials
• Self-administered by subcutaneous injectionSelf-administered by subcutaneous injection

5
Currently Approved in 46 Countries Currently Approved in 46 Countries
ArgentinaArgentina GreeceGreece PeruPeru
AustraliaAustralia GuatemalaGuatemala PolandPoland
AustriaAustria HollandHolland PortugalPortugal
BelgiumBelgium Hong KongHong Kong RomaniaRomania
BrazilBrazil HungaryHungary SingaporeSingapore
BulgariaBulgaria IcelandIceland Slovak RepublicSlovak Republic
ChileChile IrelandIreland SloveniaSlovenia
ColombiaColombia IsraelIsrael SpainSpain
Costa RicaCosta Rica ItalyItaly Sri LankaSri Lanka
Czech RepublicCzech Republic LatviaLatvia SwedenSweden
DenmarkDenmark LithuaniaLithuania SwitzerlandSwitzerland
Dominican RepublicDominican Republic LuxemburgLuxemburg Trinidad & TobaggoTrinidad & Tobaggo
EstoniaEstonia MauritiusMauritius United KingdomUnited Kingdom
FinlandFinland MexicoMexico UruguayUruguay
FranceFrance NorwayNorway VenezuelaVenezuela
GermanyGermany

6
Orphan Drug Designation for LuverisOrphan Drug Designation for Luveris®®
““For use in association with recombinant human For use in association with recombinant human follicle stimulating hormone for the treatment follicle stimulating hormone for the treatment
of women with chronic anovulation due to of women with chronic anovulation due to hypogonadotropic hypogonadism”hypogonadotropic hypogonadism”
Orphan Drug Orphan Drug RegulationRegulation
Provides incentive for the development Provides incentive for the development of drugs to treat rare diseases and of drugs to treat rare diseases and conditionsconditions
Rare Disease Rare Disease or Conditionor Condition
Prevalence < 200,000 patients with the Prevalence < 200,000 patients with the disease in the USdisease in the US
PrevalencePrevalence Hypogonadotropic Hypogonadal WomenHypogonadotropic Hypogonadal Women2,800-5,600 (1/50,000-1/25,000)*2,800-5,600 (1/50,000-1/25,000)*
* OOPD * OOPD ##94-80294-802

7
Regulatory History – LuverisRegulatory History – Luveris®®
Clinical Development ProgramClinical Development Program
May 1992May 1992 Pre-IND Meeting - clinical program of r-Pre-IND Meeting - clinical program of r-hLH for follicular developmenthLH for follicular development
2 Phase II/III Studies (6253, 6905)2 Phase II/III Studies (6253, 6905)
March 1999March 1999 Studies completed – 2 different Studies completed – 2 different populations – insufficient for NDA filingpopulations – insufficient for NDA filing
Confirmatory Phase III trial (Study Confirmatory Phase III trial (Study 21008) required for approval21008) required for approval
December December 20002000
Pre-NDA meeting with FDA Division of Pre-NDA meeting with FDA Division of Reproductive and Urologic Drug Reproductive and Urologic Drug ProductsProducts
April 2001April 2001 NDA submitted to FDANDA submitted to FDA

8
Regulatory History – LuverisRegulatory History – Luveris® ® (cont’d)(cont’d)Clinical Development ProgramClinical Development Program
March 2002March 2002 Not Approvable LetterNot Approvable Letter
• Insufficient evidence to support Insufficient evidence to support efficacy of the 75 IU/day doseefficacy of the 75 IU/day dose
• Conduct another Phase III studyConduct another Phase III study– Efficacy vs. PlaceboEfficacy vs. Placebo
– Ovulation inductionOvulation induction
– Dose rangingDose ranging
– Placebo, 75 IU and lower dose (50 or 25 IU)Placebo, 75 IU and lower dose (50 or 25 IU)
April 2002April 2002 Type A meeting – cycle cancellation due Type A meeting – cycle cancellation due to to RiskRisk of OHSS of OHSS
January 2003January 2003 FDA will bring LuverisFDA will bring Luveris®® before before Advisory CommitteeAdvisory Committee

9
Regulatory History – LuverisRegulatory History – Luveris® ® (cont’d)(cont’d)Clinical Development ProgramClinical Development Program
April 2003April 2003 NDA amended to include results from NDA amended to include results from extension study (21415) for confirmatory extension study (21415) for confirmatory
phase III trialphase III trial
August 2003August 2003 NDA amended to revise indicationNDA amended to revise indication

10
Topics for DiscussionTopics for Discussion
• Is there a need for recombinant luteinizing Is there a need for recombinant luteinizing hormone?hormone?
• Has the appropriate patient population been Has the appropriate patient population been defined?defined?
• Has a safe and effective dose been identified?Has a safe and effective dose been identified?– 75 IU/day75 IU/day
• Is the composite primary endpoint of follicular Is the composite primary endpoint of follicular development an appropriate endpoint to assess development an appropriate endpoint to assess efficacy in this patient population?efficacy in this patient population?

11
Topics for Discussion Topics for Discussion (cont’d)(cont’d)
• Is the definition of treatment success appropriate?Is the definition of treatment success appropriate?– Primary efficacy endpointPrimary efficacy endpoint
• Follicular developmentFollicular development– Cancellation for the Cancellation for the RiskRisk of OHSS of OHSS– PregnancyPregnancy
• Serum Serum -hCG pregnancy test and/or ultrasound-hCG pregnancy test and/or ultrasound
• Do the data support the safety and efficacy of Do the data support the safety and efficacy of LuverisLuveris®® in the proposed indication? in the proposed indication?
• Should another phase III double-blind Should another phase III double-blind placebo-controlled clinical trial be required for placebo-controlled clinical trial be required for approval of Luverisapproval of Luveris®® in patients with this rare in patients with this rare condition?condition?

12
External Consultant ExpertsExternal Consultant Experts
Sarah L. Berga, MDSarah L. Berga, MD• James Robert McCord Professor and ChairJames Robert McCord Professor and Chair
Department of Gynecology and ObstetricsDepartment of Gynecology and ObstetricsEmory University School of MedicineEmory University School of Medicine
Michael Diamond, MDMichael Diamond, MD• Kamram S. Moghissi Professor and Associate Chair Kamram S. Moghissi Professor and Associate Chair
of Obstetrics and Gynecology,of Obstetrics and Gynecology,Director, Division of Reproductive Endocrinology & InfertilityDirector, Division of Reproductive Endocrinology & InfertilityWayne State University (Detroit, MI)Wayne State University (Detroit, MI)
Gary Koch, PhDGary Koch, PhD• Statistical ConsultantStatistical Consultant
Chapel Hill, NCChapel Hill, NC

13
External Consultant Experts External Consultant Experts (cont’d)(cont’d)
Bert Spilker, MD, PhDBert Spilker, MD, PhD• Co-founder and former PresidentCo-founder and former President
Orphan MedicalOrphan MedicalAdjunct Professor of Medicine; Clinical Professor of PharmacyAdjunct Professor of Medicine; Clinical Professor of PharmacyUniversity of North Carolina (Chapel Hill, NC)University of North Carolina (Chapel Hill, NC)
Nanette F. Santoro, MDNanette F. Santoro, MD• Professor andProfessor and Director, Division of Reproductive EndocrinologyDirector, Division of Reproductive Endocrinology
Department of Obstetrics and Gynecology and Women’s HealthDepartment of Obstetrics and Gynecology and Women’s HealthAlbert Einstein College of Medicine (NY)Albert Einstein College of Medicine (NY)
Jerome Strauss, MD, PhDJerome Strauss, MD, PhD• Luigi Mastroianni Jr ProfessorLuigi Mastroianni Jr Professor
Director, Center for Research on Reproduction and Women’s HealthDirector, Center for Research on Reproduction and Women’s HealthUniversity of PennsylvaniaUniversity of PennsylvaniaAssociate Chairman, Department of Obstetrics and GynecologyAssociate Chairman, Department of Obstetrics and Gynecology

14
Need for and Role of LH in Need for and Role of LH in HH Women with Profound HH Women with Profound Gonadotropin DeficiencyGonadotropin Deficiency
Jerome F. Strauss III, MD, PhDJerome F. Strauss III, MD, PhDLuigi Mastroianni Jr ProfessorLuigi Mastroianni Jr Professor
Director, Center for Research on Director, Center for Research on Reproduction & Women’s HealthReproduction & Women’s Health
University of PennsylvaniaUniversity of Pennsylvania
Associate Chairman, Department of Associate Chairman, Department of Obstetrics and GynecologyObstetrics and Gynecology

15
OutlineOutline
• Heterogeneity of pathophysiology and phenotype Heterogeneity of pathophysiology and phenotype in Hypogonadotropic Hypogonadism (HH)in Hypogonadotropic Hypogonadism (HH)
• Consequences of profound LH deficiencyConsequences of profound LH deficiency
• Current therapeutic options for HHCurrent therapeutic options for HH
• Unmet medical needUnmet medical need

16
CNS InfluenceCNS Influence
Steroidal andSteroidal andNonsteroidalNonsteroidalFeedbackFeedback
GnRHGnRH
LH FSHLH FSH
HH Can Be Caused by Hypothalamic HH Can Be Caused by Hypothalamic Disorders, Pituitary Disease or BothDisorders, Pituitary Disease or Both
HypothalamusHypothalamus
PituitaryPituitary
OvaryOvary

17
HH: A Rare, Heterogeneous ConditionHH: A Rare, Heterogeneous Condition
PathophysiologyPathophysiology
• CongenitalCongenital
• AcquiredAcquired
• Variable deficiencyVariable deficiency– Pan-hypopituitarismPan-hypopituitarism– Isolated gonadotropin deficiencyIsolated gonadotropin deficiency– Moderate impairmentModerate impairment

18
Diagnosis of Profound LH Deficiency in HHDiagnosis of Profound LH Deficiency in HH
• Serum LH levels < 1.2 IU/LSerum LH levels < 1.2 IU/L– Shoham Z et al. Shoham Z et al. Fertil SterilFertil Steril 1991; 56:1048-1053 1991; 56:1048-1053
• Endocrine or functional evidence of estradiol Endocrine or functional evidence of estradiol deficiencydeficiency– Estradiol level <30 pg/mlEstradiol level <30 pg/ml– Failed progestin challenge testFailed progestin challenge test

19
OutlineOutline
• Heterogeneity of pathophysiology and phenotype Heterogeneity of pathophysiology and phenotype in Hypogonadotropic Hypogonadism (HH)in Hypogonadotropic Hypogonadism (HH)
• Consequences of profound LH deficiencyConsequences of profound LH deficiency
• Current therapeutic options for HHCurrent therapeutic options for HH
• Unmet medical needUnmet medical need

20
Role of LH in Ovarian FunctionRole of LH in Ovarian Function
• Follicular steroidogenesisFollicular steroidogenesis– Stimulation of androgen synthesis by theca cellsStimulation of androgen synthesis by theca cells
• Follicular maturationFollicular maturation– Can support terminal stages of follicular maturationCan support terminal stages of follicular maturation
• OvulationOvulation– Resumption of meiosisResumption of meiosis– OvulationOvulation– LuteinizationLuteinization
• Maintenance of luteal functionMaintenance of luteal function

21
LH and FSH Action on the FollicleLH and FSH Action on the Follicle
Theca externa cellsTheca externa cells
Theca interna cellsTheca interna cells
Capillary networkCapillary network Basement membraneBasement membrane
CumulusOophoruscells
OocyteZona pellucida
Granulosacells Follicular
antrum
LH receptorsLH receptorson theca cellson theca cells
FSH receptors FSH receptors on granulosa on granulosa cellscells
EE22
FSHFSH
LHLHAA

22
Ovarian Defects in LH Receptor KO MiceOvarian Defects in LH Receptor KO Mice
Zhang et al. Zhang et al. Mol EndocrinolMol Endocrinol. 15:172-183, 2001.. 15:172-183, 2001.

23
HH Treated with r-hFSH AloneHH Treated with r-hFSH Alone
Shoham Z et al. Shoham Z et al. Fertil SterilFertil Steril 1993; 59:738 1993; 59:738
00
55
1010
1515
00 55 1010 1515 2020DaysDays
Serum FSHSerum FSH
5050
100100
FollicleFollicle
EstradiolEstradiol
r-hFSHr-hFSH
EstradiolEstradiol(pg/ml)(pg/ml)
Follicle SizeFollicle Size(mm)(mm)
and FSHand FSH(IU/L)(IU/L)
00
99EndometrialEndometrialThicknessThickness
(mm)(mm)

24
HH Treated with r-hFSH and r-hLHHH Treated with r-hFSH and r-hLH
EstradiolEstradiol(pg/ml)(pg/ml)
Serono data Study 6253Serono data Study 6253
Follicle SizeFollicle Size(mm)(mm)
and FSHand FSH(IU/L)(IU/L)
r-hFSHr-hFSH
r-hLHr-hLH
00
55
1010
1515
00 55 1010 1515 2020DaysDays
5050
100100
2020
Serum FSHSerum FSH
FollicleFollicle
EstradiolEstradiol
150150
200200
250250
300300
350350
400400
00
00
99EndometrialEndometrialThicknessThickness
(mm)(mm)

25
The LH Therapeutic Window ConceptThe LH Therapeutic Window Concept
• Follicular growth impairedFollicular growth impaired
• Inadequate androgen (and estrogen) synthesisInadequate androgen (and estrogen) synthesis
• No full oocyte maturationNo full oocyte maturation
LH thresholdLH threshold
Normal follicular growth and developmentNormal follicular growth and development
Normal androgen and estrogen biosynthesisNormal androgen and estrogen biosynthesis
Normal oocyte maturationNormal oocyte maturation
Balasch J, FBalasch J, Fábreques F. ábreques F. Curr Opin Obstet GynecolCurr Opin Obstet Gynecol 2002, 14:265-274 2002, 14:265-274
• Suppression of granulosa cell proliferationSuppression of granulosa cell proliferation
• Follicular atresia (nondominant follicles)Follicular atresia (nondominant follicles)
• Premature luteinization (preovulatory follicle)Premature luteinization (preovulatory follicle)
• Oocyte development compromisedOocyte development compromisedLH ceilingLH ceiling

26
OutlineOutline
• Heterogeneity of pathophysiology and phenotype Heterogeneity of pathophysiology and phenotype in Hypogonadotropic Hypogonadism (HH)in Hypogonadotropic Hypogonadism (HH)
• Consequences of profound LH deficiencyConsequences of profound LH deficiency
• Current therapeutic options for HHCurrent therapeutic options for HH
• Unmet medical needUnmet medical need

27
Current Therapeutic Options for HHCurrent Therapeutic Options for HH
Gonadotropin Releasing Hormone (GnRH)Gonadotropin Releasing Hormone (GnRH)
• ProPro– Effective in women with hypothalamic disease Effective in women with hypothalamic disease
and intact pituitaryand intact pituitary– Monofollicular ovulation Monofollicular ovulation
• ConCon– Approved but discontinuedApproved but discontinued– Requires long-term pulsatile infusionRequires long-term pulsatile infusion

28
Current Therapeutic Options for HHCurrent Therapeutic Options for HH
Human Menopausal Gonadotropins (hMG)Human Menopausal Gonadotropins (hMG)
• ProPro– Reported to be effective in mostly small, Reported to be effective in mostly small,
uncontrolled seriesuncontrolled series– Can be used in women with hypothalamic and/or Can be used in women with hypothalamic and/or
pituitary diseasepituitary disease
• ConCon– Fixed ratio of FSH and LHFixed ratio of FSH and LH– Ovarian Hyperstimulation Syndrome (OHSS)Ovarian Hyperstimulation Syndrome (OHSS)– Multiple gestationMultiple gestation

29
OutlineOutline
• Heterogeneity of pathophysiology and phenotype Heterogeneity of pathophysiology and phenotype in Hypogonadotropic Hypogonadism (HH)in Hypogonadotropic Hypogonadism (HH)
• Consequences of profound LH deficiencyConsequences of profound LH deficiency
• Current therapeutic options for HHCurrent therapeutic options for HH
• Unmet medical needUnmet medical need

30
Unmet Medical NeedUnmet Medical Need
• No FDA approved LH-only treatment for No FDA approved LH-only treatment for profoundly LH deficient patientsprofoundly LH deficient patients
• Individualization/titrationIndividualization/titration– No options available for individualization of treatmentNo options available for individualization of treatment
• Recombinant ProductRecombinant Product– PurityPurity
– ConsistencyConsistency
– S.C. administrationS.C. administration

31
ConclusionsConclusions
• LH is required for follicular competencyLH is required for follicular competency
• HH is a very rare, heterogeneous disorderHH is a very rare, heterogeneous disorder
• HH women profoundly deficient in LH require HH women profoundly deficient in LH require exogenous LH for normal follicular functionexogenous LH for normal follicular function
• Optimal therapy of HH is based on individualized Optimal therapy of HH is based on individualized treatmenttreatment

32
LuverisLuveris®® Clinical Development ProgramClinical Development Program
Paul Lammers, MDPaul Lammers, MDChief Medical OfficerChief Medical Officer
Serono, Inc.Serono, Inc.

33
Presentation OutlinePresentation Outline
• LuverisLuveris®® (r-hLH) Clinical Development Program (r-hLH) Clinical Development Program– Study Design Considerations Study Design Considerations – Study Endpoints & Definition of Treatment EffectStudy Endpoints & Definition of Treatment Effect
• Dose Finding Studies Dose Finding Studies
• Efficacy OverviewEfficacy Overview– Confirmatory Phase III Study 21008Confirmatory Phase III Study 21008– Extension Study 21415Extension Study 21415– Pregnancies & Pregnancy OutcomesPregnancies & Pregnancy Outcomes
• Safety OverviewSafety Overview
• Overall ConclusionsOverall Conclusions

34
Clinical Development Program of LuverisClinical Development Program of Luveris®®
* Fixed Dose of 150 IU r-hFSH* Fixed Dose of 150 IU r-hFSH
StudyStudy DescriptionDescription PopulationPopulationNo. of No. of
PatientsPatientsr-hLH Doses r-hLH Doses
(IU)(IU)
6253*6253* Dose FindingDose Finding Profoundly LH / Profoundly LH / FSH deficientFSH deficient
3838 0, 25, 75, 2250, 25, 75, 225
7798*7798* Dose Response, Dose Response, UncontrolledUncontrolled
Profoundly LH / Profoundly LH / FSH deficientFSH deficient
1515 75, 150, 22575, 150, 225
21008*21008* Confirmatory, Confirmatory, Double-BlindDouble-Blind
Profoundly LH / Profoundly LH / FSH deficientFSH deficient
3939 Placebo, 75Placebo, 75
2141521415 Extension Extension to 21008to 21008
Profoundly LH / Profoundly LH / FSH deficientFSH deficient
3131 75 75
6905*6905* Dose FindingDose Finding Hypo / hypoHypo / hypo 4040 0, 25, 75, 2250, 25, 75, 225
8297*8297* Sequential Dosing, Sequential Dosing, UncontrolledUncontrolled
Hypo / hypoHypo / hypo 3838 75, 150, 22575, 150, 225

35
Design ConsiderationsDesign ConsiderationsDose Finding Studies and Confirmatory Study 21008Dose Finding Studies and Confirmatory Study 21008
• Study design considerationsStudy design considerations– Identify a clear dose response Identify a clear dose response – Focus on effect of LH treatment onlyFocus on effect of LH treatment only– Avoid potential confounder: change in FSH doseAvoid potential confounder: change in FSH dose– Fix the dose of LH and FSH in each cycleFix the dose of LH and FSH in each cycle
• Clinical considerationsClinical considerations– Absence of pre-existing data in this population Absence of pre-existing data in this population – Provide adequate starting dose of FSH (150 IU)Provide adequate starting dose of FSH (150 IU)– Conservative criteria for discontinuing treatment for Conservative criteria for discontinuing treatment for
ovarian over-response (ovarian over-response (RiskRisk of OHSS) of OHSS)

36
Primary Composite Efficacy Endpoint: Primary Composite Efficacy Endpoint: Capture Various Actions of LH Capture Various Actions of LH
• Synergistic Action of LH with FSH on Synergistic Action of LH with FSH on Follicular GrowthFollicular Growth– Follicle size Follicle size 17 mm 17 mm
• Normal pre-ovulatory sizeNormal pre-ovulatory size
• Necessary Role of LH in Enabling Necessary Role of LH in Enabling Follicular FunctionFollicular Function– Serum ESerum E22 109 pg/ml (400 pmol/L) 109 pg/ml (400 pmol/L)
• Lower limit of normal, and adequate for endometrial Lower limit of normal, and adequate for endometrial responseresponse
• Contribution of LH to Corpus Luteum Competence, after Contribution of LH to Corpus Luteum Competence, after hCG AdministrationhCG Administration– Mid-luteal PMid-luteal P44 7.9 ng/ml (25 nmol/L) 7.9 ng/ml (25 nmol/L)
• Above threshold for normal ovulating womenAbove threshold for normal ovulating women(( 6.0 ng/mL) 6.0 ng/mL)

37
Definition of Treatment SuccessDefinition of Treatment Success
Composite Endpoint – Follicular DevelopmentComposite Endpoint – Follicular Development
1.1. At least one follicle At least one follicle 17 mm in diameter 17 mm in diameter
2.2. Pre-ovulatory Serum Estradiol Pre-ovulatory Serum Estradiol 109 pg/ml (400 pmol/L) 109 pg/ml (400 pmol/L)
3.3. Mid-luteal Phase Serum P Mid-luteal Phase Serum P44 7.9 ng/ml (25 nmol/L) 7.9 ng/ml (25 nmol/L)
OROR
PregnancyPregnancyPositive Positive -hCG-hCG (>10 mIU/mL) or confirmatory (>10 mIU/mL) or confirmatory UltrasoundUltrasound
OROR
Cycle Cancellation for Cycle Cancellation for RiskRisk of OHSS of OHSSOvarian Response:Ovarian Response: 3 follicles 3 follicles 15 mm and/or E 15 mm and/or E22 level >1100 pg/ml level >1100 pg/ml

38
Key Secondary Efficacy EndpointsKey Secondary Efficacy Endpoints
• Estradiol (EEstradiol (E22) level) level
• Endometrial thickness (mm)Endometrial thickness (mm)– Receptive uterine ‘milieu’Receptive uterine ‘milieu’
• Pregnancy RatePregnancy Rate

39
Dose Finding StudiesDose Finding Studies
Study 6253 and Study 6905 Study 6253 and Study 6905

40
Study 6253Study 6253
Study DesignStudy Design
• Controlled, parallel-designed, open-label, randomized, Controlled, parallel-designed, open-label, randomized,
3 cycle, dose-finding3 cycle, dose-finding– Multinational study: September 1993 - April 1995Multinational study: September 1993 - April 1995– 38 subjects enrolled in 10 centers in 4 countries38 subjects enrolled in 10 centers in 4 countries
• Standard dose-finding approachStandard dose-finding approach– r-hFSH: 150 IU per dayr-hFSH: 150 IU per day– r-hLH: 0, 25, 75, and 225 IU per day (1:1:1:1 in Cycle 1)r-hLH: 0, 25, 75, and 225 IU per day (1:1:1:1 in Cycle 1)– Protocol pre-specified an Armitage trend test to detect Protocol pre-specified an Armitage trend test to detect
relationship between the LH dose and follicular relationship between the LH dose and follicular development in Cycle 1development in Cycle 1
• Adequately powered at 85%Adequately powered at 85%

41
Study 6253Study 6253
Study Design Study Design (cont’d)(cont’d)
• Clinical Entry Criteria Clinical Entry Criteria – AmenorrheaAmenorrhea– Low gonadotropin levelsLow gonadotropin levels
• LH < 1.2 IU/L and FSH < 5 IU/L LH < 1.2 IU/L and FSH < 5 IU/L (Profoundly LH-deficient)(Profoundly LH-deficient)
– Negative progestin challenge test as indicator of chronic low Negative progestin challenge test as indicator of chronic low estrogen statusestrogen status
• Treatment duration up to 14 daysTreatment duration up to 14 days– If follicular response was ongoing (EIf follicular response was ongoing (E22 rise and follicle rise and follicle
> 10 mm), treatment could continue beyond 14 days> 10 mm), treatment could continue beyond 14 days
• Primary and secondary endpoints to be analyzed Primary and secondary endpoints to be analyzed in cycle 1in cycle 1
• Pregnancy rates to be evaluated across all 3 cyclesPregnancy rates to be evaluated across all 3 cycles

42
DiagnosisDiagnosisNo. of No. of
PatientsPatients
Primary AmenorrheaPrimary Amenorrhea
• Kallmann SyndromeKallmann Syndrome
• Idiopathic, isolated HHIdiopathic, isolated HH
• Trauma- or tumor-related isolated gonadotropin deficiencyTrauma- or tumor-related isolated gonadotropin deficiency
• Multiple pituitary deficienciesMultiple pituitary deficiencies
77
1414
11
66
Secondary AmenorrheaSecondary Amenorrhea
• Functional or idiopathic isolated gonadotropin deficiencyFunctional or idiopathic isolated gonadotropin deficiency
• Trauma- or tumor-related multiple pituitary deficienciesTrauma- or tumor-related multiple pituitary deficiencies
88
22
TotalTotal 3838
Study 6253Study 6253
Study PopulationStudy Population

43
Study 6253Study 6253
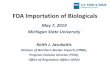
Percentage of Patients with Follicular Percentage of Patients with Follicular Development – Cycle 1Development – Cycle 1
63.6%70.0%
25.0%
11.1%
0 IU LH 25 IU LH 75 IU LH 225 IU LH
63.6%70.0%
25.0%
11.1%
0 IU LH 25 IU LH 75 IU LH 225 IU LH
1/9 2/8 7/11 7/10
p = 0.467p = 0.467 p = 0.020p = 0.020 p = 0.012p = 0.012p-values vs 0 IU LHp-values vs 0 IU LH
Trend Test*Trend Test*p = 0.004p = 0.004
* Statistically significant and robust * Statistically significant and robust

44
Study 6253Study 6253
Results for Patients Randomized to 225 IU Results for Patients Randomized to 225 IU in Cycle 1in Cycle 1
AdequateFollicular
Development;Received
hCG
InsufficientFollicular
Development
Ovarian Over-ResponseCycles Cancelled
Risk of OHSS
5/105/10
Cycle 1Cycle 1225 IU225 IU
Cycle 3Cycle 375 IU75 IU
3/33/3
Cycle 2Cycle 225 IU25 IU
1/51/5
7
6
5
4
3
2
1
10
9
8
5
4
37
6
5
4
3

45
Study 6253Study 6253
Secondary Efficacy Parameters – Cycle 1Secondary Efficacy Parameters – Cycle 1
Dose (IU LH)Dose (IU LH)
16.3 22.9
332.3
453.6
0
100
200
300
400
500
0 25 IU 75 IU 225 IU
16.3 22.9
332.3
453.6
0
100
200
300
400
500
0 25 IU 75 IU 225 IU
Median Pre-Ovulatory EMedian Pre-Ovulatory E22 Levels Levels(pg/ml)(pg/ml)
n=9 n=8 n=11 n=10
4.03.5
8.07.5
0
1
2
3
4
5
6
7
8
9
10
0 25 IU 75 IU 225 IU
4.03.5
8.07.5
0
1
2
3
4
5
6
7
8
9
10
0 25 IU 75 IU 225 IU
Median Endometrial ThicknessMedian Endometrial Thickness(mm)(mm)
n=9 n=8 n=11 n=10

46
Study 6905Study 6905
Study DesignStudy Design
• Controlled, parallel-designed, open-label, Controlled, parallel-designed, open-label, randomized, 3 cycle, dose-finding study in USrandomized, 3 cycle, dose-finding study in US– July 1994 - July 1997July 1994 - July 1997– 14 centers treated 40 subjects14 centers treated 40 subjects
• Dose Groups: 0, 25, 75, and 225 IU LH Dose Groups: 0, 25, 75, and 225 IU LH co-administered with 150 IU FSH dailyco-administered with 150 IU FSH daily– Randomization Ratio - 1:1:1:1 in cycle 1Randomization Ratio - 1:1:1:1 in cycle 1
• Fixed dose of LH and FSH within cyclesFixed dose of LH and FSH within cycles

47
Study 6905Study 6905
Study Design Study Design (cont’d)(cont’d)
• Major Differences to Study 6253Major Differences to Study 6253– LH < 13 IU/L and FSH < 11 IU/L*LH < 13 IU/L and FSH < 11 IU/L*
• Broader HH populationBroader HH population
– No progestin challenge test; ENo progestin challenge test; E22 < 60 pg/mL < 60 pg/mL– Treatment duration up to 21 daysTreatment duration up to 21 days
• If follicular maturation was imminent, treatment If follicular maturation was imminent, treatment could continue beyond 21 dayscould continue beyond 21 days
* <50* <50thth percentile normal percentile normal

48
Study 6905Study 6905
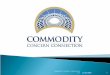
Percentage of Patients withPercentage of Patients with Follicular Follicular DevelopmentDevelopment
100.0%
72.7%66.7%63.6%
0 IU LH 25 IU LH 75 IU LH 225 IU LH
100.0%
72.7%66.7%63.6%
0 IU LH 25 IU LH 75 IU LH 225 IU LH
7/11 9/9 8/11 6/9
Trend TestTrend Testp = 0.774p = 0.774
Conclusion: the benefit of LH treatment was not Conclusion: the benefit of LH treatment was not demonstrated in the broader HH patient populationdemonstrated in the broader HH patient population

49
LuverisLuveris®® Clinical Development Program Clinical Development Program in Support of US Registrationin Support of US Registration
2 Phase II / III 2 Phase II / III Dose Response StudiesDose Response Studies
6253LH < 1.2 IU/LLH < 1.2 IU/LBenefit of LHBenefit of LH
6905Broader HH populationBroader HH population
LH > 1.2 IU/LLH > 1.2 IU/LNo Additional Benefit of LHNo Additional Benefit of LH
1992 2002
ConfirmatoryConfirmatory Phase III Study Phase III Study
requestedrequested(LH < 1.2 IU/L;(LH < 1.2 IU/L;
placebo vs 75 IU)placebo vs 75 IU)
21008

50
Lowest Effective DoseLowest Effective Dose
• Reasonable and sufficient range of doses studiedReasonable and sufficient range of doses studied(0, 25, 75, and 225 IU)(0, 25, 75, and 225 IU)
• 25 IU dose25 IU dose– Not clinically/statistically different from 0 IUNot clinically/statistically different from 0 IU– 75% non-response75% non-response
• 75 IU dose75 IU dose– Clinically/statistically different from 0 IU in primary endpoint Clinically/statistically different from 0 IU in primary endpoint
(more than a five-fold increase in patient response)(more than a five-fold increase in patient response)– Clinically different from 0 IU in secondary endpoints Clinically different from 0 IU in secondary endpoints
(E(E22 levels, and endometrial response) levels, and endometrial response)
• 225 IU dose225 IU dose– No additional benefit in efficacy compared to 75 IUNo additional benefit in efficacy compared to 75 IU
75 IU is the minimum effective dose 75 IU is the minimum effective dose providing maximum therapeutic benefitproviding maximum therapeutic benefit

51
LuverisLuveris®® Clinical Development Program Clinical Development Program in Support of US Registrationin Support of US Registration
1992 2002
2 Phase II / III 2 Phase II / III Dose Response StudiesDose Response Studies
6253LH < 1.2 IU/LLH < 1.2 IU/LBenefit of LHBenefit of LH
6905Broader HH populationBroader HH population
LH > 1.2 IU/LLH > 1.2 IU/LNo Additional Benefit of LHNo Additional Benefit of LH
Rollover ExtensionRollover ExtensionSupportive EfficacySupportive Efficacyand Safety Dataand Safety Data(LH <1.2 IU/L)(LH <1.2 IU/L)
21415
ConfirmatoryConfirmatory Phase III Study Phase III Study
requestedrequested(LH < 1.2 IU/L;(LH < 1.2 IU/L;
placebo vs 75 IU)placebo vs 75 IU)
21008

52
Efficacy OverviewEfficacy Overview
Confirmatory Phase III Trial Confirmatory Phase III Trial
Study 21008Study 21008

53
Study 21008Study 21008
Study DesignStudy Design
• Double-blind, randomized, placebo-controlled, Double-blind, randomized, placebo-controlled, multinational study in patients seeking multinational study in patients seeking pregnancypregnancy– 37 centers initiated; 25 centers enrolled 39 patients37 centers initiated; 25 centers enrolled 39 patients
• Dose Groups: Placebo and 75 IU LH Dose Groups: Placebo and 75 IU LH co-administered with 150 IU FSH dailyco-administered with 150 IU FSH daily– Randomization Ratio - 1:2Randomization Ratio - 1:2
• Fixed dose of LH and FSHFixed dose of LH and FSH

54
Study 21008Study 21008
Study Design Study Design (cont’d)(cont’d)
• Clinical Entry Criteria Clinical Entry Criteria – AmenorrheaAmenorrhea– Low gonadotropin levelsLow gonadotropin levels
• LH < 1.2 IU/L and FSH < 5 IU/L LH < 1.2 IU/L and FSH < 5 IU/L (Profoundly LH-deficient)(Profoundly LH-deficient)
– Negative progestin challenge test as indicator of chronic Negative progestin challenge test as indicator of chronic low estrogen statuslow estrogen status
• Treatment duration up to 14 daysTreatment duration up to 14 days– If follicular maturation was imminent, treatment could If follicular maturation was imminent, treatment could
continue beyond 14 dayscontinue beyond 14 days
• Single cycle of treatment (roll-over possibility to Single cycle of treatment (roll-over possibility to extension Study 21415)extension Study 21415)

55
Study 21008Study 21008
Study PopulationStudy Population
DiagnosisDiagnosisNo. of No. of
PatientsPatients
Primary AmenorrheaPrimary Amenorrhea• Kallmann SyndromeKallmann Syndrome
• Pan-hypopituitarismPan-hypopituitarism
• Other endocrine defectsOther endocrine defects
• UnspecifiedUnspecified
77
11
22
1010
Secondary AmenorrheaSecondary Amenorrhea• Other endocrine defectsOther endocrine defects
• Multiple endocrine defectsMultiple endocrine defects
• Pituitary tumor/surgeryPituitary tumor/surgery
• UnspecifiedUnspecified
22
11
11
1515
TotalTotal 3939

56
Study 21008Study 21008
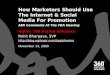
Percentage of Patients with Follicular Percentage of Patients with Follicular DevelopmentDevelopment
15.4%15.4%
65.4%65.4%
0%0%
10%10%
20%20%
30%30%
40%40%
50%50%
60%60%
70%70%
PlaceboPlacebo 75 IU LH75 IU LH
2/13 17/26
p = 0.006p = 0.006

57
Study 21008Study 21008
Percentage of Patients with Follicular Percentage of Patients with Follicular DevelopmentDevelopment
0%0%
10%10%
20%20%
30%30%
40%40%
50%50%
60%60%
70%70%
PlaceboPlacebo 75 IU LH75 IU LH
2/13 17/26
7.7%7.7%
42.3%42.3%
1/13 11/26
p = 0.006p = 0.006
p = 0.034p = 0.034
RiskRisk of OHSS of OHSS as a Failureas a Failure
15.4%15.4%
65.4%65.4%
ITTITT

58
Study 21008Study 21008
Comparison of Analyses – Comparison of Analyses – Follicular DevelopmentFollicular Development
Fisher’s Exact Fisher’s Exact p = 0.063p = 0.063Fisher’s Exact Fisher’s Exact p = 0.034p = 0.034
10/26 (38.5%)10/26 (38.5%)1/13 (7.7%)1/13 (7.7%)11/26 (42.3%)11/26 (42.3%)1/13 (7.7%)1/13 (7.7%)
75 IU75 IUPlaceboPlacebo75 IU75 IUPlaceboPlacebo
FDA’s AnalysisFDA’s AnalysisFDA Background Package, Section 2.2, Table 4FDA Background Package, Section 2.2, Table 4
Serono’s AnalysisSerono’s AnalysisSerono Background Package, Table 6.1.1-2Serono Background Package, Table 6.1.1-2
Risk of OHSS as FailureRisk of OHSS as Failure
16/26 (61.5%)16/26 (61.5%)2/13 (15.4%)2/13 (15.4%)17/26 (65.4%)17/26 (65.4%)2/13 (15.4%)2/13 (15.4%)
Fisher’s Exact Fisher’s Exact p = 0.008p = 0.008Fisher’s Exact Fisher’s Exact p = 0.006p = 0.006
75 IU75 IUPlaceboPlacebo75 IU75 IUPlaceboPlacebo
FDA’s AnalysisFDA’s AnalysisFDA Background Package, Section 2.2, Table 4FDA Background Package, Section 2.2, Table 4
Serono’s AnalysisSerono’s AnalysisSerono Background Package, Table 6.1.1-1Serono Background Package, Table 6.1.1-1
Primary AnalysisPrimary Analysis

59
Studies 21008 and 21415 Studies 21008 and 21415
Protocol Definition of SuccessProtocol Definition of Success
““The primary efficacy endpoint will be follicular The primary efficacy endpoint will be follicular development as defined by the following three development as defined by the following three parameters, all of which must be true:parameters, all of which must be true:– At least one follicle with a mean diameter At least one follicle with a mean diameter 17 mm and 17 mm and– Preovulatory EPreovulatory E22 serum level serum level 109 pg/mL (400 pmol/L) and 109 pg/mL (400 pmol/L) and– Mid-luteal phase PMid-luteal phase P44 level level 7.9 ng/mL (25 nmol/L) 7.9 ng/mL (25 nmol/L)
Should any patient be cancelled for Should any patient be cancelled for RiskRisk of OHSS, of OHSS, that patient will be counted as achieving follicular that patient will be counted as achieving follicular development. development. Should any patient achieve pregnancy, Should any patient achieve pregnancy, that patient will be counted as having achieved that patient will be counted as having achieved follicular development.”follicular development.”

60
Study 21008Study 21008
Patient 251-0001Patient 251-0001
Lead FollicleLead Follicle 20 mm20 mm (( 17 mm) 17 mm)
EE22106 pg/mL106 pg/mL (( 109 109
pg/mL)pg/mL)
PP4413.2 ng/mL13.2 ng/mL (( 7.9 ng/mL) 7.9 ng/mL)
March 7, 2000March 7, 2000 Day of hCGDay of hCG
April 4, 2000April 4, 2000 Serum hCG 102 mIU/mLSerum hCG 102 mIU/mL (( 10 10 mIU/mL)mIU/mL)
April 6, 2000April 6, 2000 Serum hCG 51 mIU/mLSerum hCG 51 mIU/mL

61
Efficacy OverviewEfficacy Overview
Extension Study 21415Extension Study 21415

62
Study Eligibility for 21415Study Eligibility for 21415
ConfirmatoryStudy 21008
Treatment ExtensionStudy 21415
1.1. Open Label Treatment:Open Label Treatment:75 IU LH and individualized 75 IU LH and individualized dose of FSH (75-225 IU) dose of FSH (75-225 IU) based on patient’s previous based on patient’s previous responseresponse
2.2. Consistent Primary EndpointConsistent Primary Endpoint
If no SAE or OHSS If no SAE or OHSS and not pregnant and not pregnant
1 Cycle Treatment1 Cycle Treatment
Up to 3 Additional CyclesUp to 3 Additional Cyclesof Treatmentof Treatment

63
Cycle 3n=8
Cycle 3n=8
n=31n=31
Cycle 1n=31
Cycle 1n=31
Cycle 2n=15
Cycle 2n=15
Study 21415Study 21415
Patient DispositionPatient Disposition
31 of 39 patients in Study 21008 enrolled 31 of 39 patients in Study 21008 enrolled and treated with 75 IU r-hLH in Study 21415and treated with 75 IU r-hLH in Study 21415• 11 Treated in 21008 with Placebo11 Treated in 21008 with Placebo
• 20 Treated in 21008 with 75 IU r-hLH20 Treated in 21008 with 75 IU r-hLH

64
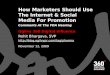
Study 21415Study 21415
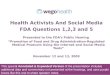
Cumulative Follicular Development with 75 IUCumulative Follicular Development with 75 IU
67.7%
83.9% 87.1%
0%
20%
40%
60%
80%
100%
Cycle 1 Cycle 2 Cycle 3
67.7%
83.9% 87.1%
0%
20%
40%
60%
80%
100%
Cycle 1 Cycle 2 Cycle 3
Cycle Cancellation for Cycle Cancellation for RiskRisk of OHSS of OHSS is mitigated with individualization of FSH doseis mitigated with individualization of FSH dose
21/31 26/31 27/31
With With RiskRisk of OHSS counted of OHSS countedas as SuccessSuccess
51.6%
83.9% 87.1%
Cycle 1 Cycle 2 Cycle 3
51.6%
83.9% 87.1%
Cycle 1 Cycle 2 Cycle 3
With With RiskRisk of OHSS counted of OHSS countedas as FailureFailure
16/31 26/31 27/31

65
Studies 21008 and 21415Studies 21008 and 21415
Impact of Cycle Cancellation for Impact of Cycle Cancellation for RiskRisk of of OHSS on Response in Subsequent CyclesOHSS on Response in Subsequent Cycles
• Cycle cancellation due to the Cycle cancellation due to the RiskRisk of OHSS is a of OHSS is a normal precaution in clinical practicenormal precaution in clinical practice
• Ovarian over-response is a treatment effect and Ovarian over-response is a treatment effect and provides guidance for next cycle of treatmentprovides guidance for next cycle of treatment
• 4 of the 11 patients whose cycles were cancelled 4 of the 11 patients whose cycles were cancelled due to due to RiskRisk of OHSS in 1 of OHSS in 1stst cycle of Study 21008 or cycle of Study 21008 or 21415 achieved pregnancy in Study 21415 with 21415 achieved pregnancy in Study 21415 with adjustment of FSH dose in subsequent cycleadjustment of FSH dose in subsequent cycle

66
9.1%
63.6%
36.4%
0.0%
Follicular Development Pregnancy
Placebo/FSH in Study 21008
75 IU LH/FSH in Study 21415
9.1%
63.6%
36.4%
0.0%
Follicular Development Pregnancy
Placebo/FSH in Study 21008
75 IU LH/FSH in Study 21415
Study 21415Study 21415
Sub Group: LH Naïve Patients (n=11)Sub Group: LH Naïve Patients (n=11)Follicular Development and PregnancyFollicular Development and Pregnancy
1/11 7/11 4/110/110/11

67
Study 21415Study 21415
PregnanciesPregnancies
Cycle 3n=8
Cycle 3n=8
n=31Received hCG = 27
n=31Received hCG = 27
Cycle 1n=31
Cycle 1n=31
Cycle 2n=15
Cycle 2n=15
Cumulative Total Pregnancy Rate in Patients Cumulative Total Pregnancy Rate in Patients Receiving hCG = 20/27 (74.1%)Receiving hCG = 20/27 (74.1%)
11Pregnancies
11Pregnancies
9Pregnancies
9Pregnancies
0Pregnancies
0Pregnancies

68
Study 21415Study 21415
ClinicalClinical PregnanciesPregnancies
Cycle 3n=8
Cycle 3n=8
n=31Received hCG = 27
n=31Received hCG = 27
Cycle 1n=31
Cycle 1n=31
Cycle 2n=15
Cycle 2n=15
Cumulative Clinical Pregnancy Rate in Patients Cumulative Clinical Pregnancy Rate in Patients Receiving hCG = 16/27 (59.3%)Receiving hCG = 16/27 (59.3%)
11Pregnancies
11Pregnancies
5Pregnancies
5Pregnancies
0Pregnancies
0Pregnancies

69
Summary of Pregnancy Results Summary of Pregnancy Results and Pregnancy Outcomesand Pregnancy Outcomes

70
Studies 6253, 21008 and 21415 Studies 6253, 21008 and 21415
Pregnancy Rates in Profoundly LH Deficient Pregnancy Rates in Profoundly LH Deficient Women (LH < 1.2 IU/L)Women (LH < 1.2 IU/L)
Treatment GroupTreatment Group Placebo/0 IUPlacebo/0 IU 25 IU LH25 IU LH 75 IU LH75 IU LH 225 IU LH225 IU LH
Patients Seeking Patients Seeking PregnancyPregnancy 2222 99 4848 88
Cycles of Treatment in Cycles of Treatment in Patients Seeking Patients Seeking PregnancyPregnancy
2222 99 9191 88
Total PregnanciesTotal Pregnancies
n (% patients)n (% patients)
[% cycles][% cycles]
2 (9.1%)2 (9.1%) 00 24 (50%)24 (50%)
[26.4%][26.4%]
1 (12.5%)1 (12.5%)
Clinical PregnanciesClinical Pregnancies
n (% patients)n (% patients)
[% cycles][% cycles]
1 (4.5%)1 (4.5%) 00 19 (39.6%)19 (39.6%)
[20.9%] [20.9%]
1 (12.5%)1 (12.5%)

71
All StudiesAll Studies
Pregnancy Outcome for Patients Pregnancy Outcome for Patients Seeking PregnancySeeking Pregnancy
Treatment GroupTreatment Group Placebo/0 IUPlacebo/0 IU 25 IU LH25 IU LH 75 IU LH75 IU LH 150 IU LH150 IU LH 225 IU LH225 IU LH
Patients Seeking Patients Seeking PregnancyPregnancy 4141 1919 111111 1313 3030
Cycles of TreatmentCycles of Treatment 4141 1919 196196 1414 3030
Total Pregnancies Total Pregnancies 77 22 5151 22 66
Clinical Pregnancies Clinical Pregnancies 55 11 4444 11 44
Clinical Pregnancies Clinical Pregnancies Leading to Live BirthsLeading to Live Births 44 11 3535 11 33
SingleSingle
TwinsTwins
TripletsTriplets
22
22
00
00
11
00
2222
1212
11
00
11
00
22
11
00
MiscarriageMiscarriage 22 00 66 00 11
Lost to follow-upLost to follow-up 00 00 33 00 00
OtherOther 11 00 22 00 00
StillbirthStillbirth 00 00 11 00 00

72
Efficacy ConclusionsEfficacy Conclusions

73
Efficacy Conclusions Efficacy Conclusions
• Study 6253 provides rationale for selection Study 6253 provides rationale for selection of 75 IU r-hLH as the of 75 IU r-hLH as the appropriate doseappropriate dose for HH for HH patients with profound LH deficiency patients with profound LH deficiency (LH < 1.2 IU/L)(LH < 1.2 IU/L)– No benefit of 25 IU dose of r-hLHNo benefit of 25 IU dose of r-hLH
– No additional benefit of 225 IU dose of r-hLHNo additional benefit of 225 IU dose of r-hLH
• Study 21008, the randomized, double-blind, Study 21008, the randomized, double-blind, placebo-controlled study, confirmed the efficacy placebo-controlled study, confirmed the efficacy of 75 IU r-hLH dose in the profoundly LH deficient of 75 IU r-hLH dose in the profoundly LH deficient (LH < 1.2 IU/L) patient population(LH < 1.2 IU/L) patient population

74
Efficacy Conclusions Efficacy Conclusions (cont’d)(cont’d)
• Study 21415 supports the efficacy of 75 IU as Study 21415 supports the efficacy of 75 IU as used in standard clinical practice with used in standard clinical practice with individualized dosingindividualized dosing– Cumulative follicular development rate 87.1%Cumulative follicular development rate 87.1%– Cumulative pregnancy rate 74.1%Cumulative pregnancy rate 74.1%
• Overall, a 50% (24/48) pregnancy rate in Overall, a 50% (24/48) pregnancy rate in profoundly LH-deficient women* (LH < 1.2 IU/L) profoundly LH-deficient women* (LH < 1.2 IU/L) on 75 IU doseon 75 IU dose
* Studies 6253, 21008, and 21415* Studies 6253, 21008, and 21415

75
Overview of Safety Overview of Safety

76
Safety ConclusionsSafety Conclusions
• Largest safety database in Female HH Patients Largest safety database in Female HH Patients (170 patients, 152 received r-hLH in 283 cycles)(170 patients, 152 received r-hLH in 283 cycles)
• No increase in adverse events when r-hLH is No increase in adverse events when r-hLH is co-administered with r-hFSH, compared to co-administered with r-hFSH, compared to r-hFSH aloner-hFSH alone
• Similar rates of OHSS across all dose groups, Similar rates of OHSS across all dose groups, including r-hFSH aloneincluding r-hFSH alone
• Safety profile of r-hLH comparable to currently Safety profile of r-hLH comparable to currently marketed gonadotropinsmarketed gonadotropins

77
Overall ConclusionsOverall ConclusionsLuverisLuveris®® Clinical Development Program Clinical Development Program
• Among women with HH, a cut-off value of 1.2 IU/L Among women with HH, a cut-off value of 1.2 IU/L differentiates between LH-dependence and differentiates between LH-dependence and LH-independence LH-independence
• Follicular development is an appropriate endpoint in Follicular development is an appropriate endpoint in this population and correlates with pregnancythis population and correlates with pregnancy
• Canceling a cycle is prudent clinical practice in an Canceling a cycle is prudent clinical practice in an over-responding patient with follicular developmentover-responding patient with follicular development
• Women with profound LH-deficiency clearly benefit Women with profound LH-deficiency clearly benefit from treatment with Luverisfrom treatment with Luveris®® 75 IU 75 IU
• The safety profile of LuverisThe safety profile of Luveris®® is similar to other is similar to other gonadotropins and is not different from treatment with gonadotropins and is not different from treatment with FSH aloneFSH alone

78
Clinical PerspectiveClinical Perspectiveandand
Risk/Benefit AssessmentRisk/Benefit Assessment
Nanette F. Santoro, MDNanette F. Santoro, MDProfessor and Director,Professor and Director,
Division of Reproductive EndocrinologyDivision of Reproductive Endocrinology
Department of Obstetrics and Gynecology Department of Obstetrics and Gynecology and Women’s Healthand Women’s Health
Albert Einstein College of MedicineAlbert Einstein College of Medicine

79
Hypogonadotropic Hypogonadism (HH) Hypogonadotropic Hypogonadism (HH) Women and InfertilityWomen and Infertility
• Absence of pubertal developmentAbsence of pubertal development
• Single endocrine factorSingle endocrine factor
• Potential to be highly fertile when ovarian Potential to be highly fertile when ovarian responsiveness is restoredresponsiveness is restored
• LH (in addition to FSH) is needed for optimal LH (in addition to FSH) is needed for optimal follicle growthfollicle growth
• Induction of follicular development as a prelude Induction of follicular development as a prelude to fertility is the therapeutic goalto fertility is the therapeutic goal

80
Follicular MaturationFollicular Maturation
FSHFSH
• Induces early growthInduces early growth
• Controls follicle numberControls follicle number
LHLH
• Provides estrogen precursorsProvides estrogen precursors
• Needed for latter stages of growthNeeded for latter stages of growth

r-hFSH in Woman with HH: Follicle Growth r-hFSH in Woman with HH: Follicle Growth Without EstradiolWithout Estradiol
Follicular sizeFollicular size(mm)(mm)
r-hFSHr-hFSH(IU/day)(IU/day)
7575
150150
00
hCGhCG(10,000 IU)(10,000 IU)
2020
1515
55
1010
00
88
66
22
44
00
FSH (IU/L)FSH (IU/L)LH (IU/L)LH (IU/L)
Estradiol (pmol/L)Estradiol (pmol/L)
81

82
RiskRisk of OHSS vs OHSS of OHSS vs OHSS
3 Developing Follicles3 Developing Follicles
OHSS: Massive Ovarian OHSS: Massive Ovarian Enlargement and Enlargement and
Multiple CystsMultiple Cysts

83
Follicular Development in HHFollicular Development in HH
• Give back what’s missingGive back what’s missing
–GnRH highly effective if intact pituitary function, GnRH highly effective if intact pituitary function,
but not availablebut not available
–Alternative strategy: exogenous gonadotropins Alternative strategy: exogenous gonadotropins (u-hMG), but combined fixed ratio and (u-hMG), but combined fixed ratio and IM administration is a limitation to treatmentIM administration is a limitation to treatment
–Optimal strategy: stand-alone recombinant Optimal strategy: stand-alone recombinant human LH and FSH allows titration and human LH and FSH allows titration and individualizationindividualization

84
Recombinant LHRecombinant LH
• Permissive and obligatory for follicle growthPermissive and obligatory for follicle growth
• FSH tailoring is needed in gonadotropin FSH tailoring is needed in gonadotropin cycles, therefore: rLH dose should be cycles, therefore: rLH dose should be ‘guaranteed’ to be sufficient! ‘guaranteed’ to be sufficient!
• 75 IU dose is adequate75 IU dose is adequate
• Maximizes return on investment (cycle) Maximizes return on investment (cycle) for patient and clinicianfor patient and clinician

85
Risks vs. BenefitsRisks vs. Benefits
RisksRisks
• Known complications of gonadotropins in Known complications of gonadotropins in infertility treatmentinfertility treatment– Ovarian Hyperstimulation Syndrome (OHSS)Ovarian Hyperstimulation Syndrome (OHSS)– Multiple birthsMultiple births
• Other minimal/transient treatment-related Other minimal/transient treatment-related adverse events (minor)adverse events (minor)
• Risks mitigated with proper diagnosis, Risks mitigated with proper diagnosis, dosing and observationdosing and observation

86
Risks vs. BenefitsRisks vs. Benefits
BenefitsBenefits
• Optimal folliculogenesis and endocrine profile Optimal folliculogenesis and endocrine profile based on individualized treatmentbased on individualized treatment
• Convenience (subcutaneous, self-administered)Convenience (subcutaneous, self-administered)
• Safety profile comparable to currently marketed Safety profile comparable to currently marketed gonadotropinsgonadotropins
• High pregnancy rate in this profoundly High pregnancy rate in this profoundly LH-deficient patient populationLH-deficient patient population

87
SummarySummary
• HH is a rare patient group for whom LH is HH is a rare patient group for whom LH is criticalcritical during folliculogenesis during folliculogenesis
• Provision of rLH to rFSH allows maximum Provision of rLH to rFSH allows maximum flexibility in treatment of these patientsflexibility in treatment of these patients
• Benefit/risk profile in favor of approval and Benefit/risk profile in favor of approval and making product available to patients and making product available to patients and physiciansphysicians

88
Summary and ConclusionsSummary and Conclusions
Pamela Williamson Joyce, RACPamela Williamson Joyce, RACVice President, Regulatory AffairsVice President, Regulatory Affairs
& Quality Assurance – U.S.& Quality Assurance – U.S.Serono, Inc.Serono, Inc.

89
ConclusionsConclusions
• Clear need for LH in treatment of patients with Clear need for LH in treatment of patients with this rare conditionthis rare condition
• Appropriate patient population – HH women, Appropriate patient population – HH women, profoundly LH deficientprofoundly LH deficient
• Optimal dose of 75 IU safe and effectiveOptimal dose of 75 IU safe and effective
• Follicular development, as prospectively defined, Follicular development, as prospectively defined, most appropriate to determine action of LHmost appropriate to determine action of LH
• Most extensive database in r-hLH in Most extensive database in r-hLH in hypogonadotropic hypogonadal women (n=170)hypogonadotropic hypogonadal women (n=170)

90
ConclusionsConclusions
• Largest double-blind placebo-controlled clinical Largest double-blind placebo-controlled clinical trial (21008) in patients with this rare conditiontrial (21008) in patients with this rare condition
• Pivotal trial positive whether cycle cancellation Pivotal trial positive whether cycle cancellation due to due to RiskRisk of OHSS analyzed as efficacy of OHSS analyzed as efficacy success or failuresuccess or failure
• Additional supportive efficacy, safety and Additional supportive efficacy, safety and pregnancy data (21415)pregnancy data (21415)

91
ConclusionsConclusions
• No increase in adverse events compared No increase in adverse events compared to placebo; safety similar to that of other to placebo; safety similar to that of other gonadotropin productsgonadotropin products
• LuverisLuveris®® is effective for treatment of infertile is effective for treatment of infertile women with profound LH deficiency women with profound LH deficiency (LH < 1.2 IU/L)(LH < 1.2 IU/L)
• Positive Benefit/Risk profilePositive Benefit/Risk profile