Embed Size (px)
Citation preview
ملزمة العملي لصف الرابع –مادة التولید
The Obstetric history and examination
زینب عبد األمیر جعفر .د
HISTORY TAKING
Greeting patients in appropriate way. Introduces yourself to the patient (I am a -medical student/doctor/etc- May I ask you some questions?) Puts the patient at ease. Enables the patient to elaborate presenting problem fully. Listens attentively. Use clear language and avoid medical jargon. Seeks clarification of words used by the patient as appropriate Phrases questions simply and clearly Identifies the patient's ideas, concerns and expectations Check of the patient’s cognitive state.)
* triple patient's name *triple husband's name * Age *age * Occupation * Occupation * Residence * Residence * Religion * Blood group&Rh * Marital status consanguinity * Blood group&Rh
Date of admission:-
:operationDate of delivery or -
No. of pregnancies regardless of how they endedG:
parity is the number of live births at any gestation or stillbirths P:after 24 weeks
A: (expulsion of conceptus before 24 weeks gestation)
o If the patient had ectopic or H.mole considered G1 & 1 ectopic or H.mole
o A twin pregnancy counts as a single pregnancy for gravidity but gives a parity of two considered as G1 P2
-LMP = First day of the last menstrual period.
1. the patients certainty of dates 2. the regularity of the cycle 3. the use of contraception
day of Gregorian calendar: stExpected date of delivery (1 EDD:-Naegles rule
What was the first day of her last menstrual period (LMP)? What was the length of her menstrual cycle and was it regular?
EDD=LMP-3mths+7days (for 28 day cycle) EDD=LMP+9mths+7days (for 28 day cycle) For a cycle longer than 28 days: will be later and needs to
be adjusted: the number of days by which the cycle is longer than 28 is added to the date calculated using Nägle’s rule
EDD=LMP+9mths/-3mths+7days+ (cycle length−28days) The reverse applies if the cycle is shorter than 28 days If a woman has recently stopped the combined oral
contraceptive, her cycles can be anovulatory and LMP is less useful
In the UK, ultrasound between 11 and 13 + 6 weeks is routine, and considered more accurate even than ‘certain’ dates.
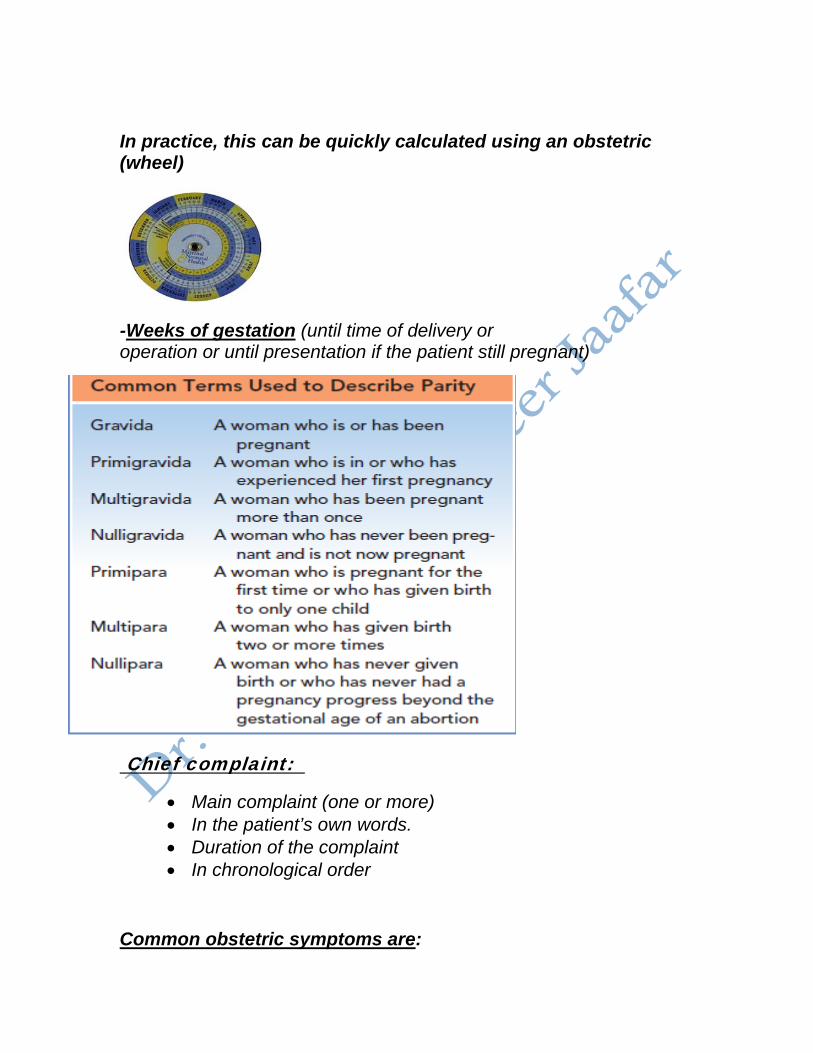
In practice, this can be quickly calculated using an obstetric (wheel)
(until time of delivery or Weeks of gestation-operation or until presentation if the patient still pregnant)
Chief complaint:
• Main complaint (one or more) • In the patient’s own words. • Duration of the complaint • In chronological order
Common obstetric symptoms are:
Bleeding per vagina, abdominal pain, urinary symptoms, headaches, reduced fetal movements, Emesis gravidarum, Urinary disturbances, Fetal kicks & quickening, Late Bleeding, PROM, Contractions
History of presenting complaint:
This section should focus on the presenting complaint
Each of the problems of the patient describes must be obtained in detail by questioning regarding:
1. what exactly the problem is 2. When exactly the problem is occurring, the date and time of
onset(Onset, severity, duration) 3. whether the symptoms are getting worse(course) 4. the duration of the symptoms when they do occur 5. how these symptoms are related to or influence other events
in her life. 6. What increases/decreases the symptom 7. Associated Other symptoms 8. Investigations done (date, place & results) 9. Treatment received (details & response) 10. Any complications 11. Admission history: course of illness, medication given and
investigations done, postoperative course until presentation
Certain important points should always be enquired about
1- Abdominal pain :‘SOCRATES’ is frequently used for taking an HPC of a pain:
Site: where is the pain?local or diffuse Onset: sudden or gradual? Speed of onset and any associated
circumstances Character: ‘Can you describe the pain?’ (e.g. sharp/dull,
burning/tingling,boring/stabbing, crushing/tugging, preferably using the patient’s own description rather than offering suggestions
Radiation: does the pain move elsewhere? Associated symptoms: shortness of breath, nausea, vomiting,
fever, sweating etc. Timing: (duration, course, pattern), - Since onset - Episodic or continuous
If episodic, duration and frequency of attacks If continuous, any changes in severity
Exacerbants/relievers: does anything make it better or worse? Severity: ‘Can you rate your pain out of ten, where one is barely
there, and ten is the worst pain imaginable? Does it prevent you from doing anything?’
2- Vaginal bleeding: • When bleeding started • Onset
Spontaneous following trauma Following PV examination or intercourse
• Course Continuous/intermittent Single attack/ recurrent
• Amount of blood loss Spotting Excessive 7presence of clots- N° of pads- need for
blood transfusion Passage of clots Associated with fainting attacks.
• Other symptoms
Pain(full description of pain) PE See warning symptoms of pregnancy Quality of fetal movements after the attack
• Speculum examination in the hospital 1. Vaginal discharge- amount, color, itching, odour, presence of blood. 2. if the patient in the third trimester, ask about fetal movement 3. if the patient is hypertensive or diabetic, ask about time of
diagnosis and the treatment she receive 4. If the patient has similar or related complaints previously mention
this and its timing
3- Discharge 1- Characters of the discharge ( colour , amount ,odour , consistency ) 2- Associated symptoms as : - Itching ( pruritis vulva ) - Menstrual irregularities 3- Factors that increase or decrease the discharge
4- A case of swelling
May be abdominal or at the vulva ( prolapse )
A. Site ,and size:The patient may describing it as lemon or orange size
B. Factors that increase or decrease the complaint . C. For prolapse
• Effect of straining on it ( present all over the time or only on straining )
• Associated urinary or G.I.T symptoms .
5- Case of pre-eclamptic toxaemia ( P.E.T ) A. Onset ,course and duration of the symptoms B. Ask about the signs and symptoms of the problem ( headache ,
blurring of vision , swelling lower limb ,……..,…… ) C. Attack of similar condition on previous pregnancy D. If she is still feel the foetal movement . E. Symptoms of imminent eclampsia, Aggravation of P.E.T symptoms
● loss of vision Sever epigastric pain 6- A case of diabetes with pregnancy .
A. The age of the onset and duration of the diabetes B. Dose of insulin or hypoglycaemic tablets taken. C. Associated symptoms:Polyuria , polydepsia , numbness in the
limbs , decrease in the weight . D. If she is still feel with the foetal movement . E. Symptoms of associated P.E.T .
7- Pregnancy of a cardiac patient .
1- About the cardiac disease
• Onset ( congenital , before pregnancy , during pregnancy ) • Course ( progressive , stationary , retrogressive ) • Duration ( since …………..) • Nature ( rheumatic , congenital , artificial valve , ……. )
2- About the association
Dyspnea ( at the rest , on exertion , orthpnea ,…….. ) Cough ( dry or productive , characters of sputum ) Haemoptysis , chest pain Pain in the right hypochondrium ( liver congestion )
3- If she is still feel with the foetal movement .
4- Therapeutic history especially if she take Lanoxine
Review of other systems:
o Appetite, weight loss or gain. o GIT, Urinary symptoms o Cardiovascular, respiratory and other systems.
Review of other systems:
GIT
• Appetite (increased or decreased ) • Vomiting(time,frequency,related to meal,projectile or not,relation
to pain,content food particles,colour odor,with blood or not,amount)
• Abdominalpain:(site,radiation,character,duration,severity,character,aggrivation factor,relieving factor)
• Diarrhoea:(frequancy,time in the day,character-watery –frothy,colour ,drug history)
• Constipation:(recurrent,long standing,any cholicky pain) • Flatulance: (related to the meal,directed up ward or down
ward,relieve pain or not)
• Dysphagia-difficulty in swelling(site,type of food,associated with pain or not)
• Water brush(excessive saliva screation) • Fever :either(high grade-sweating,rigor,chill)-or (low grade)
CVS
1. Chest pain • Site • Radiation • Severity • Character • Duration • Aggrevating factor • Relieving factor
2. Dyspnea • When dose it occur • At rest or only in exertion • At night only • Can sleep lying down
3. fatiguability 4. claudication 5. palpitation
• what bring it • duration • is the puls feeled regular or not
6. bleding tendency eg.epistaxis
History of present pregnancy:
:13 weeks) –First trimester (0 *
1. How pregnancy is diagnosed (conceived spontaneously or on treatment):
2. ANC (regular or irregular): 3. pain (abdominal or back pain): 4. bleeding (amount and duration): 5. Severe nausea and vomiting (hyper emesis gravidarum), weight
loss, hospital admission: 6. Urinary and bowel symptoms: 7. Any febrile illness or hospitalization: 8. Drugs and radiation exposure: 9. If the patient is hypertensive or diabetic, ask about early ANC visits
& treatment received.
:28 weeks) –Second trimester (14 *
1. Quickening: the first fetal movement (as the patient told in which month of pregnancy) This is the first perception of the foetal movement by the mother (16- 18 w in multigravida , 18-20 w in primigravida )
2. Abdominal pain: 3. Vaginal bleeding or discharge: 4. Urinary and bowel symptoms: 5. Weight gain and edema: 6. ANC (blood pressure and routine investigations):
delivery): –Third trimester (29 weeks *
1. Fetal movements (normally at least 4 movements in 1 hour or 10 in 12 hours)
2. Abdominal pain: 3. Vaginal bleeding or discharge: 4. Urinary and bowel symptoms: 5. Weight gain and edema: 6. ANC (blood pressure and routine investigations):
Past Obstetric history:
1. Date of marriage 2. when she conceived (any period of infertility) 3. For each pregnancy ask about:
duration(term, preterm or post term)
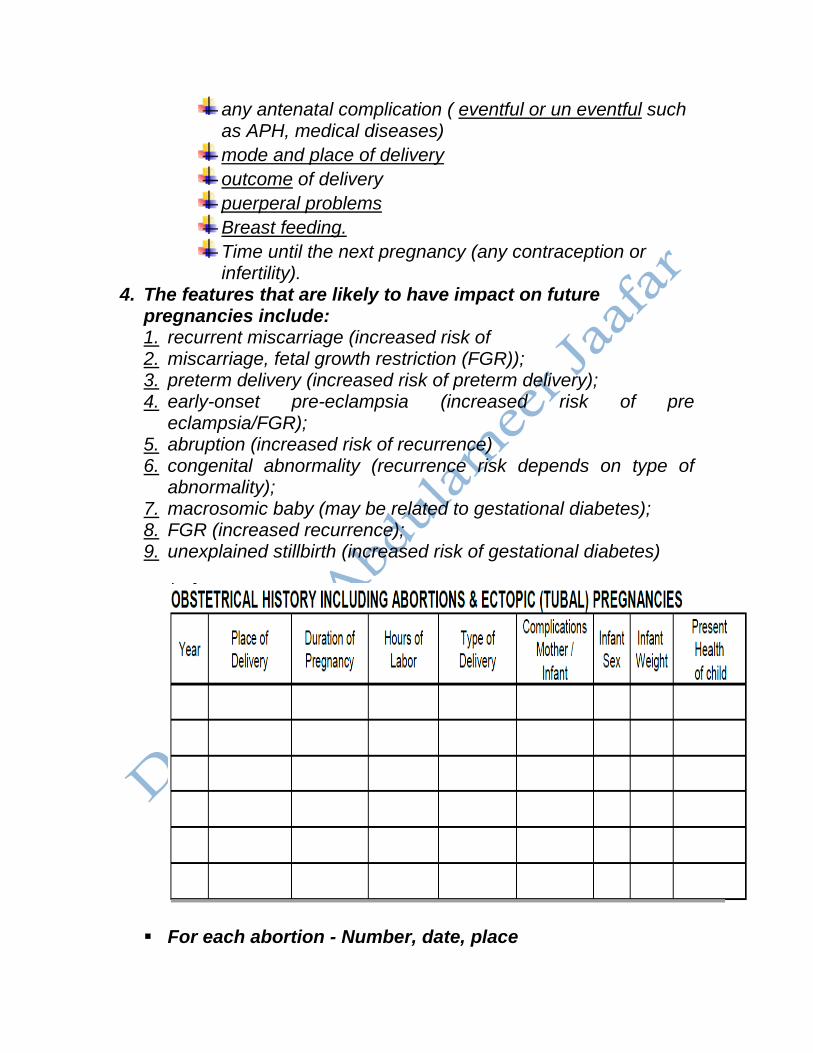
any antenatal complication ( eventful or un eventful such as APH, medical diseases) mode and place of delivery outcome of delivery puerperal problems Breast feeding. Time until the next pregnancy (any contraception or infertility).
4. The features that are likely to have impact on future pregnancies include: 1. recurrent miscarriage (increased risk of 2. miscarriage, fetal growth restriction (FGR)); 3. preterm delivery (increased risk of preterm delivery); 4. early-onset pre-eclampsia (increased risk of pre
eclampsia/FGR); 5. abruption (increased risk of recurrence) 6. congenital abnormality (recurrence risk depends on type of
abnormality); 7. macrosomic baby (may be related to gestational diabetes); 8. FGR (increased recurrence); 9. unexplained stillbirth (increased risk of gestational diabetes)
For each abortion - Number, date, place
1) Spontaneous (bleeding, pain, ROM) - Followed by evacuation or not? - Any post-abortive complications? e.g. bleeding, sepsis, perforation 2) Induced (e.g. blighted ovum)
Each CS 1) Order of pregnancy 2) Time 3) Place 4) Indication 5) Intraoperative complication (Injury :intestine, bladder) 6) Type of anesthesia 7) Need for blood transfusion 8) Postoperative 9) Wound infection 10) PPH 11) Puerperal sepsis:fever, diffuse bilateral lower abdominal pain,
offensive vaginal discharge and admission to hospital,DVT and pulmonary embolism
Past gynecological history:
1. Menstrual history:
Age of menarche. Usual duration of each period? Length of cycle. Painful cycles (treatment received) Does bleeding or spotting occur between periods or after
intercourse?
2. Previous gynecological surgery or treatment.
The date of last cervical smear. History of discomfort, pain, or bleeding during intercourse.
3. The use of contraception and type of contraception used.
4. History of infertility
Past medical history: Any serious illness or medical diseases, chronic disease e.g.
1. Diabetes mellitus:. 2. Hypertension: pre-eclampsia. 3. Renal disease 4. Epilepsy 5. Venous thromboembolic disease 6. Human immunodefi ciency virus (HIV) infection 7. Connective tissue diseases 8. Myasthenia gravis/myotonic dystrophy
Past surgical history:
• Anesthetic complications (as scoline apnea) • Previous operations (postoperative complications). • Blood transfusion.
Drug history:
Allergy to any drug. Chronic drug use such antihypertensive and antiepileptic drugs. For each medication, record:
1. Drug. 2. Dose and route. 3. Indication. 4. Date started.
Family history:
1. Any chronic medical diseases such as hypertension, DM, ,thromboembolic disease(increased risk of thrombophilia,thrombosis)
2. Consanguineous marriage 3. History of pre-eclampsia (increased risk of pre-eclampsia) 4. History of psychiatric disorder (increased risk of puerperal
psychosis.
5. History of twin pregnancy, congenital malformations or cerebral palsy or any potential genetic problems such as haemoglobinopathies or fetal inborn errors of metabolism
6. History of malignancies in the family. 7. History of tuberculosis ,allergies
Social history
1. Marital status, relative or not. 2. Family problems 3. living environment 4. Occupation 5. Income 6. Level of education 7. Housing conditions 8. Smoking and alcohol use. 9. Drug abuse
FINAL DIAGNOSIS
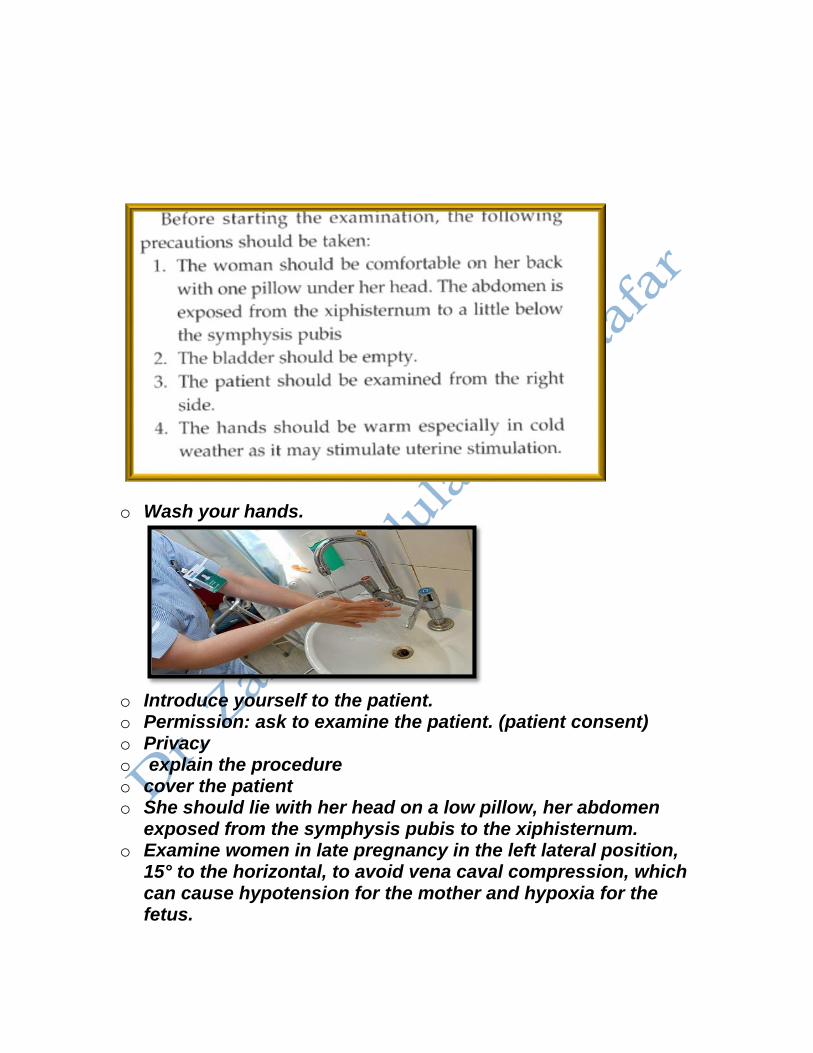
o Wash your hands.
o Introduce yourself to the patient. o Permission: ask to examine the patient. (patient consent) o Privacy o explain the procedure o cover the patient o She should lie with her head on a low pillow, her abdomen
exposed from the symphysis pubis to the xiphisternum. o Examine women in late pregnancy in the left lateral position,
15° to the horizontal, to avoid vena caval compression, which can cause hypotension for the mother and hypoxia for the fetus.
Vital signs:
1. B.P.: The patient lies comfortably with her back semi-prone at 45° using a correctly sized BP cuff should be placed at the level of the heart. Diastolic blood pressure is recorded as Korotkoff 5 (when the sound disappears) 90-140/60-90 normally
2. Pulse rate ,volume and rhythm (for 30 sec. if abnormal then count for 1 min.) tachycardia >100 bpm . ( 60-100/ min ).Slight increase of 10-15 / min may occur in obstetric ( physiological changes of pregnancy )
3. Respiratory rate: about 16-20 / min , pregnancy usually associated with hyperventilation (progesteron action ).
4. Temperature: The ‘normal’ oral or ear temperature is range between 36.6°C to 37.2°C (98°F to 99°F)), Rectal temperature is about 0.5°C higher than oral. The axilla is an unreliable site for measuring temperature. Use a digital thermometer under the tongue, or in the rectum or the external auditory meatus
5. • Weight • Height • BMI
Examination:
General examination:
1. General appearance:level of consciousness, ill, well, body built( obese or thin), dyspnea.Sick or well? Alert or drowsy?Cachectic or obese? Comfortable at rest?
2. Colour: • Jaundice (sclera, nail beds). • Pallor (lower palpebral conjunctiva, palms of the hand, nail
beds, tongue, lips) • Skin changes: There may be increased skin pigmentation
due to increased production of melanotropin. This may manifest as the following:
Face: Melasma, a frequently encountered skin change during pregnancy
Breasts: Darkening of areolas Abdomen: Linea nigra.
3. Neck and neck veins-for: • obvious thyroid swelling • raised JVP • Enlarged lymph nodes (neck, axillae and inguinal areas)
4. If the patient has cannula examine for site and signs of
thrombophlebitis
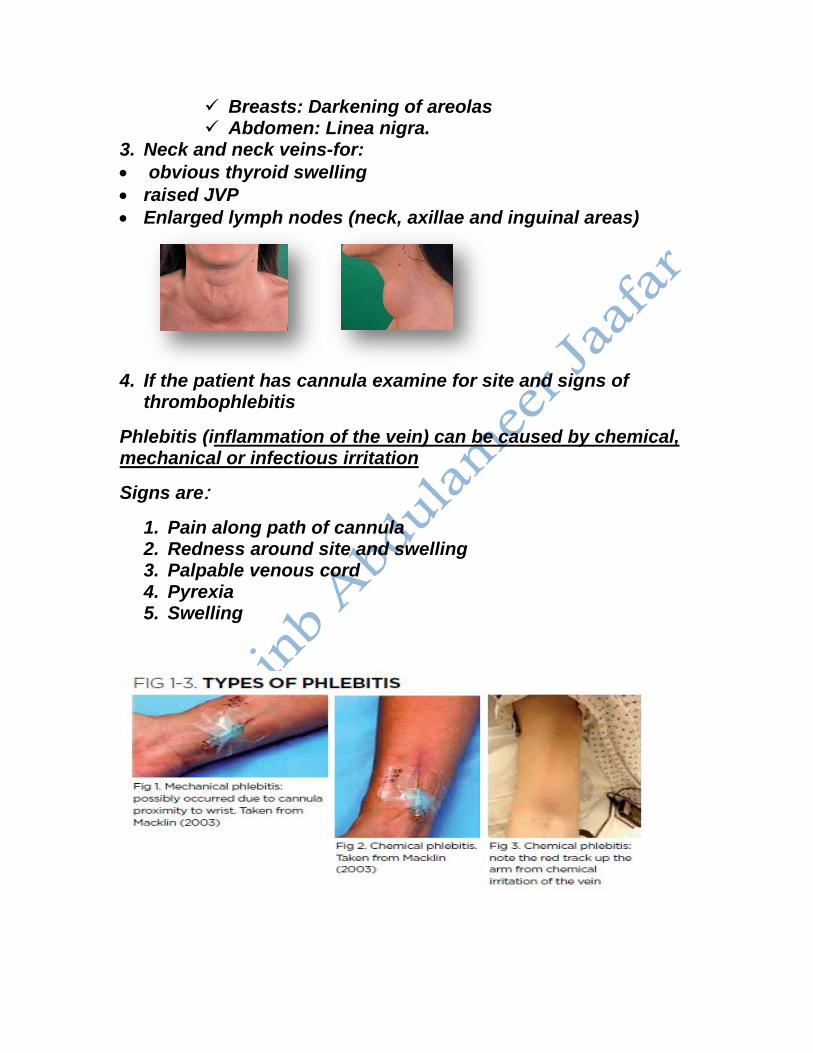
Phlebitis (inflammation of the vein) can be caused by chemical, mechanical or infectious irritation
Signs are:
1. Pain along path of cannula 2. Redness around site and swelling 3. Palpable venous cord 4. Pyrexia 5. Swelling
5. Edema (press over the lower medial third of the tibial shin for 30 seconds), other sites the medial side of the ankle and dorsum of the foot.
6. Possible sign of DVT 1. Inspection: skin color ,loss of hair ,swelling varicose vein 2. Palpation: hotness, tenderness, pulsation 3. Measurement of diameter
SYSTEMIC EXAMINATION
• Cardiovascular system • Respiratory system • Central nervous system
Abdominal examination:
Inspection:
1. The contour of the abdomen for any distension as pregnancy 2. Assess the shape of the uterus and note any asymmetry 3. Obvious fetal movements 4. Movement with respiration(if absent indicates peritonism) 5. Hair distribution 6. Umbilicus 7. dilated veins 8. striae gravidarum and albicans or linea nigra(the faint
brown line running from the umbilicus to the symphysis pubis)
9. The patient is asked to cough or raise her head for any herniae , divarication of the rectus muscles
10. Surgical scars: (suprapubic {pfannenstiel scar }=caesarean
section,Laprotomy for ectopic pregnancy or ovarian masses),
(sub-umbilical scars =Laparoscopy) right upper quadrant(cholycystectomy)
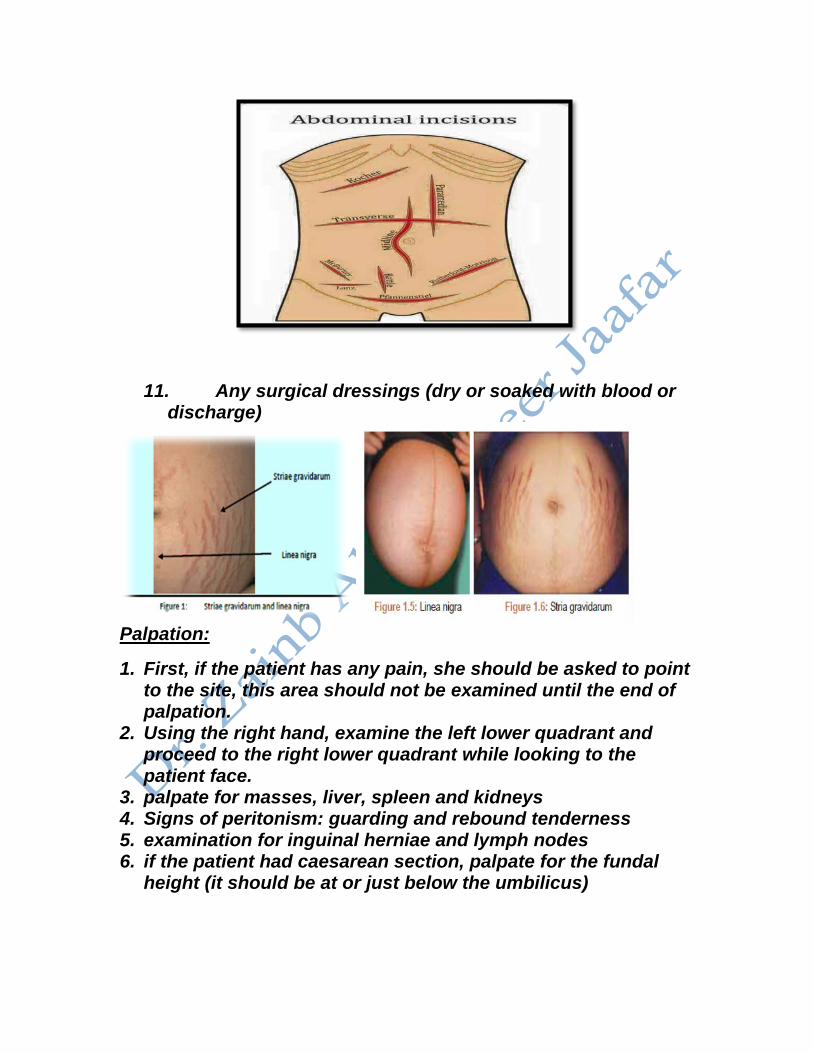
11. Any surgical dressings (dry or soaked with blood or discharge)
Palpation:
1. First, if the patient has any pain, she should be asked to point to the site, this area should not be examined until the end of palpation.
2. Using the right hand, examine the left lower quadrant and proceed to the right lower quadrant while looking to the patient face.
3. palpate for masses, liver, spleen and kidneys 4. Signs of peritonism: guarding and rebound tenderness 5. examination for inguinal herniae and lymph nodes 6. if the patient had caesarean section, palpate for the fundal
height (it should be at or just below the umbilicus)
Obstetric maneuvers:
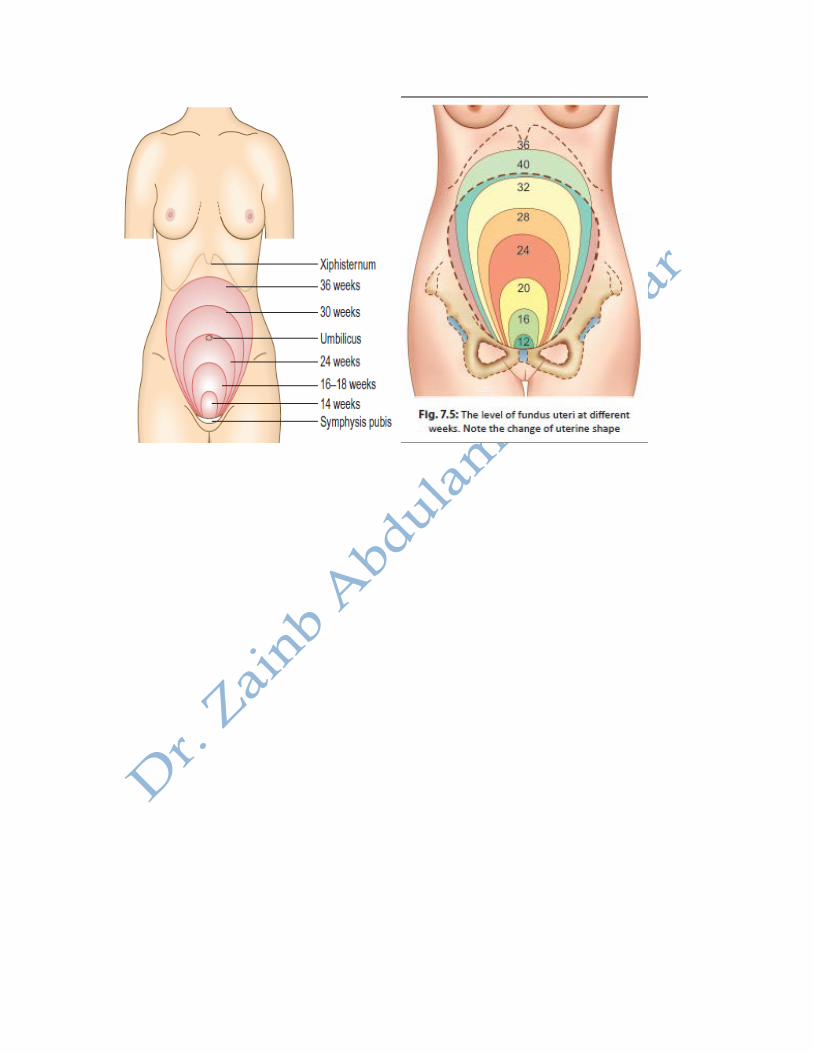
1. Fundal height:
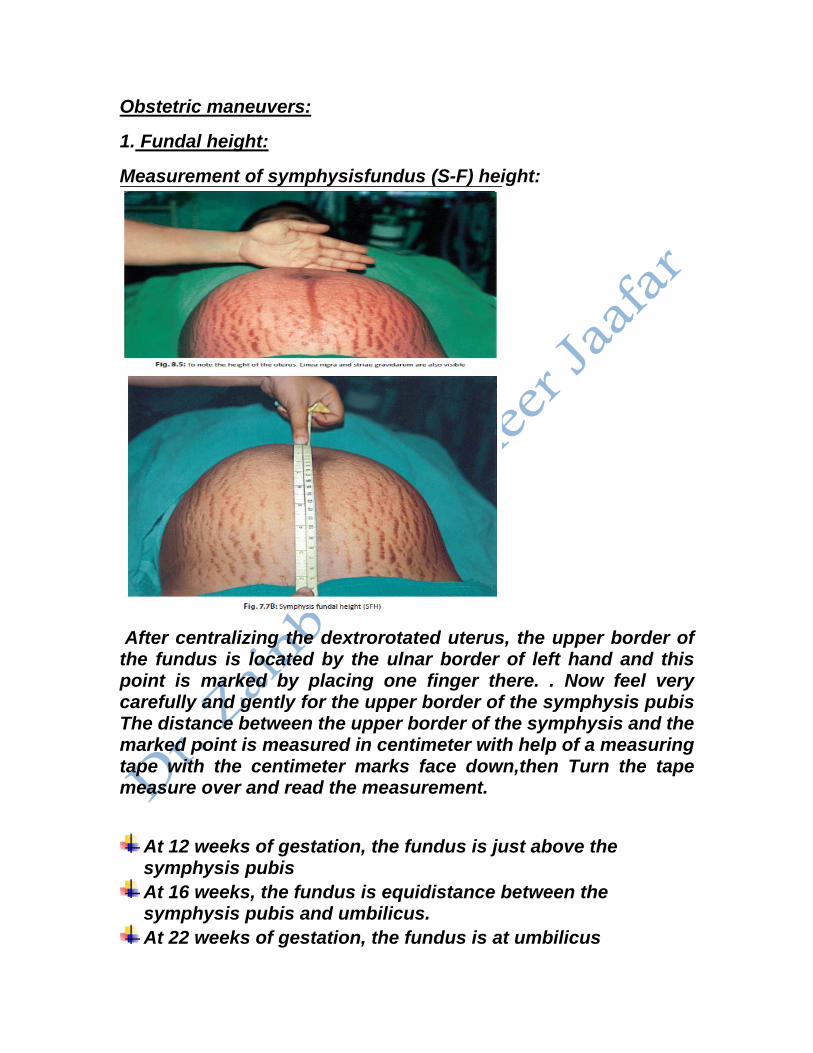
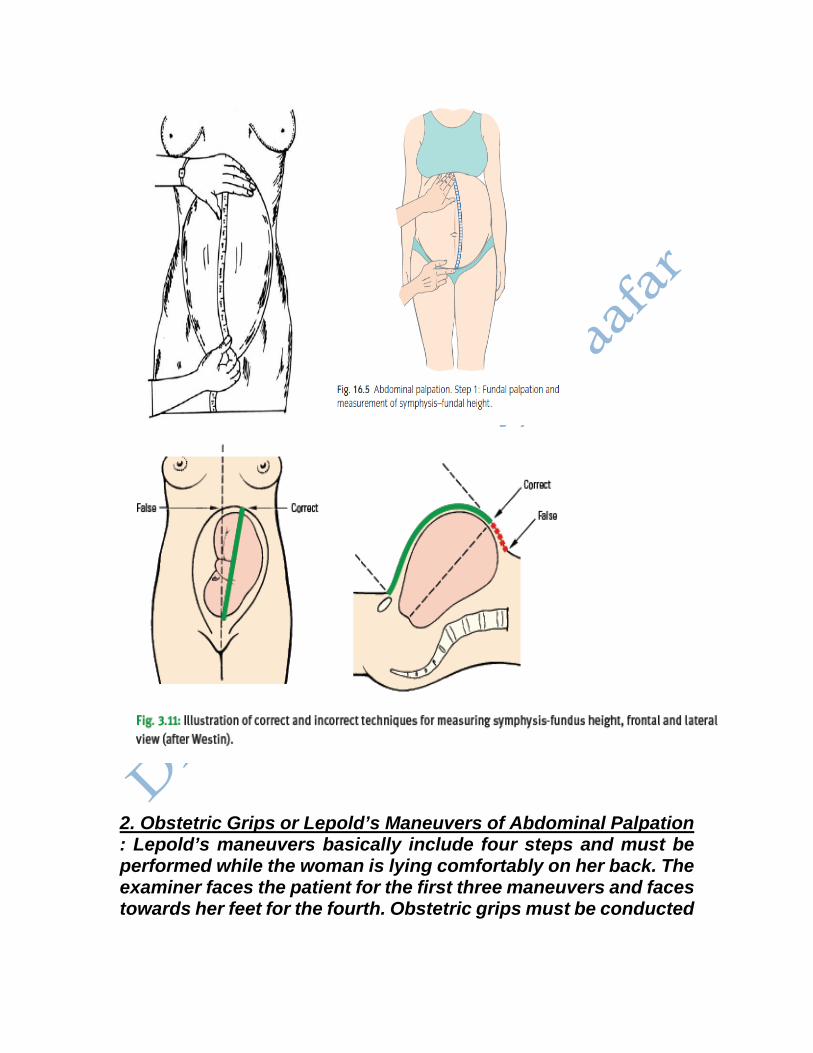
Measurement of symphysisfundus (S-F) height:
After centralizing the dextrorotated uterus, the upper border of the fundus is located by the ulnar border of left hand and this point is marked by placing one finger there. . Now feel very carefully and gently for the upper border of the symphysis pubis The distance between the upper border of the symphysis and the marked point is measured in centimeter with help of a measuring tape with the centimeter marks face down,then Turn the tape measure over and read the measurement.
At 12 weeks of gestation, the fundus is just above the symphysis pubis At 16 weeks, the fundus is equidistance between the symphysis pubis and umbilicus. At 22 weeks of gestation, the fundus is at umbilicus
After 24 weeks, the S-F height, measured in centimeters corresponds to the period of gestation up to 36 weeks. Though a variation of 2 cm (more or less) is regarded as normal At 30 weeks, the fundus is equidistance between the xiphisternum and umbilicus. At 36 weeks, the fundus is at xiphisternum, depending on the level of presenting part whether it descends into the pelvis. Late third trimester the fundal height is usually approximately 2 cm less than the number of weeks.
There are conditions where the height of the uterus may not correspond with the period of amenorrhea. The conditions where the height of the uterus is more than the period of amenorrhea are:
1. mistaken date of the last menstrual period 2. twins 3. polyhydramnios 4. big baby(macrosomia) 5. pelvic tumors—ovarian or fibroid 6. hydatidiform mole 7. concealed accidental hemorrhage. 8. Rarely, a twin is missed on ultrasound!
The condition where the height of the uterus is less than the period of amenorrhea are:
1. mistaken date of the last menstrual period 2. Oligohydramnios 3. fetal growth retardation (FGR) 4. intrauterine fetal death.
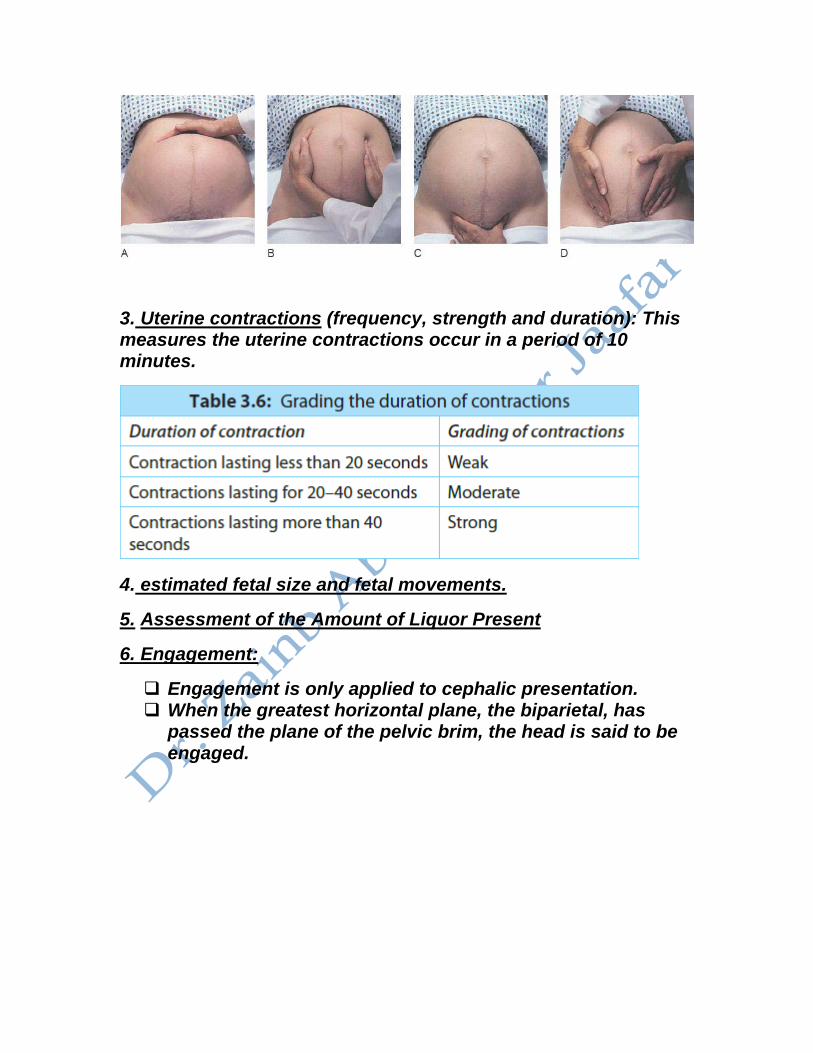
2. Obstetric Grips or Lepold’s Maneuvers of Abdominal Palpation : Lepold’s maneuvers basically include four steps and must be performed while the woman is lying comfortably on her back. The examiner faces the patient for the first three maneuvers and faces towards her feet for the fourth. Obstetric grips must be conducted
when the uterus is relaxed and not when the woman is experiencing contractions.
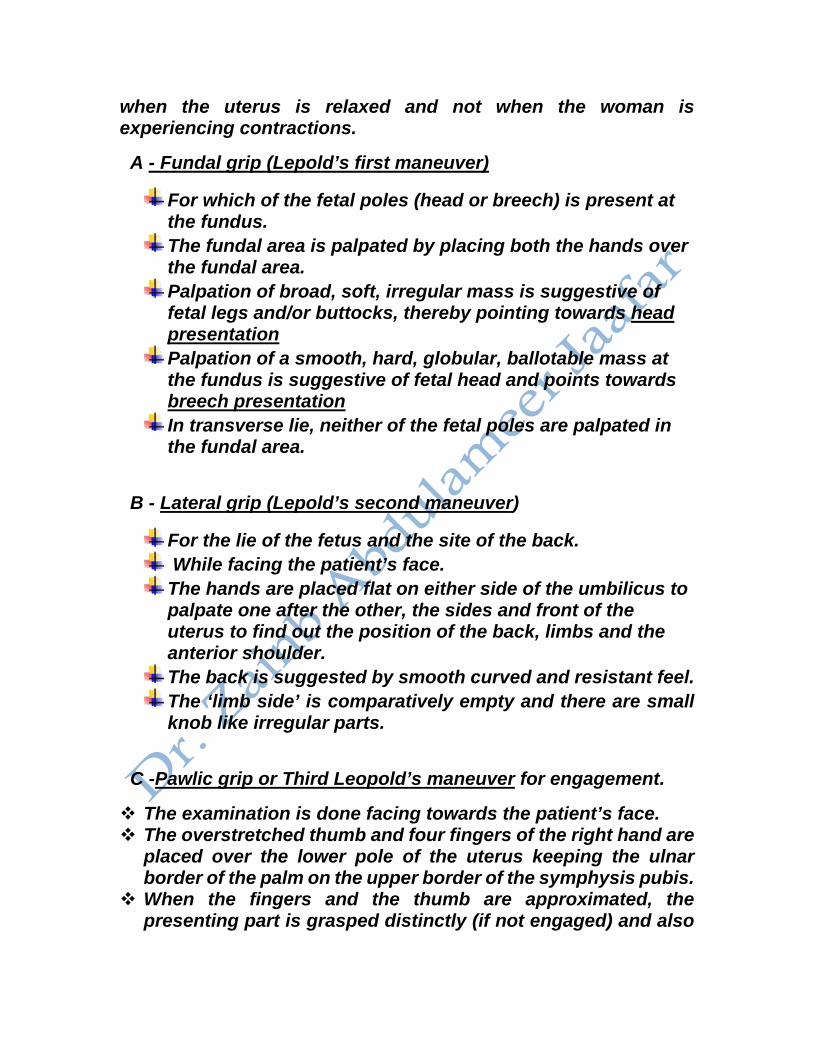
A - Fundal grip (Lepold’s first maneuver)
For which of the fetal poles (head or breech) is present at the fundus. The fundal area is palpated by placing both the hands over the fundal area. Palpation of broad, soft, irregular mass is suggestive of fetal legs and/or buttocks, thereby pointing towards head presentation Palpation of a smooth, hard, globular, ballotable mass at the fundus is suggestive of fetal head and points towards breech presentation In transverse lie, neither of the fetal poles are palpated in the fundal area.
B - Lateral grip (Lepold’s second maneuver)
For the lie of the fetus and the site of the back. While facing the patient’s face. The hands are placed flat on either side of the umbilicus to palpate one after the other, the sides and front of the uterus to find out the position of the back, limbs and the anterior shoulder. The back is suggested by smooth curved and resistant feel. The ‘limb side’ is comparatively empty and there are small knob like irregular parts.
C -Pawlic grip or Third Leopold’s maneuver for engagement.
The examination is done facing towards the patient’s face. The overstretched thumb and four fingers of the right hand are
placed over the lower pole of the uterus keeping the ulnar border of the palm on the upper border of the symphysis pubis.
When the fingers and the thumb are approximated, the presenting part is grasped distinctly (if not engaged) and also
the mobility from side to side is tested. In transverse lie, Pawlik’s grip is empty
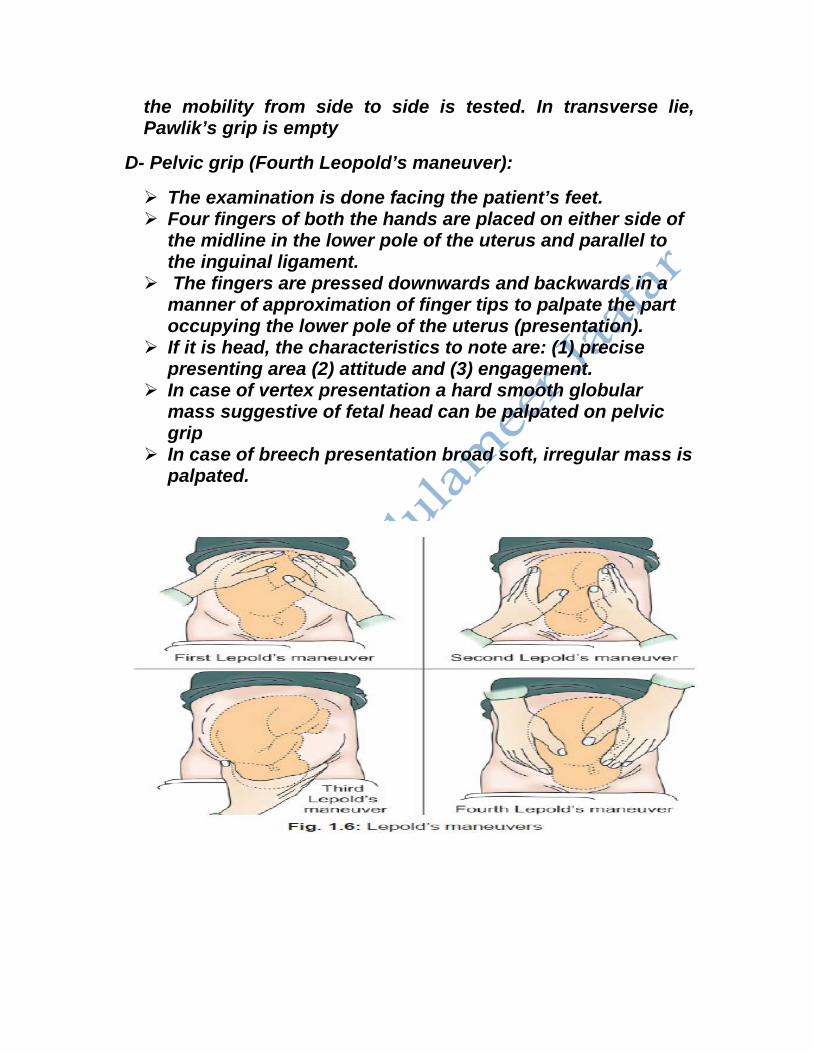
D- Pelvic grip (Fourth Leopold’s maneuver):
The examination is done facing the patient’s feet. Four fingers of both the hands are placed on either side of
the midline in the lower pole of the uterus and parallel to the inguinal ligament.
The fingers are pressed downwards and backwards in a manner of approximation of finger tips to palpate the part occupying the lower pole of the uterus (presentation).
If it is head, the characteristics to note are: (1) precise presenting area (2) attitude and (3) engagement.
In case of vertex presentation a hard smooth globular mass suggestive of fetal head can be palpated on pelvic grip
In case of breech presentation broad soft, irregular mass is palpated.
3. Uterine contractions (frequency, strength and duration): This measures the uterine contractions occur in a period of 10 minutes.
4. estimated fetal size and fetal movements.
5. Assessment of the Amount of Liquor Present
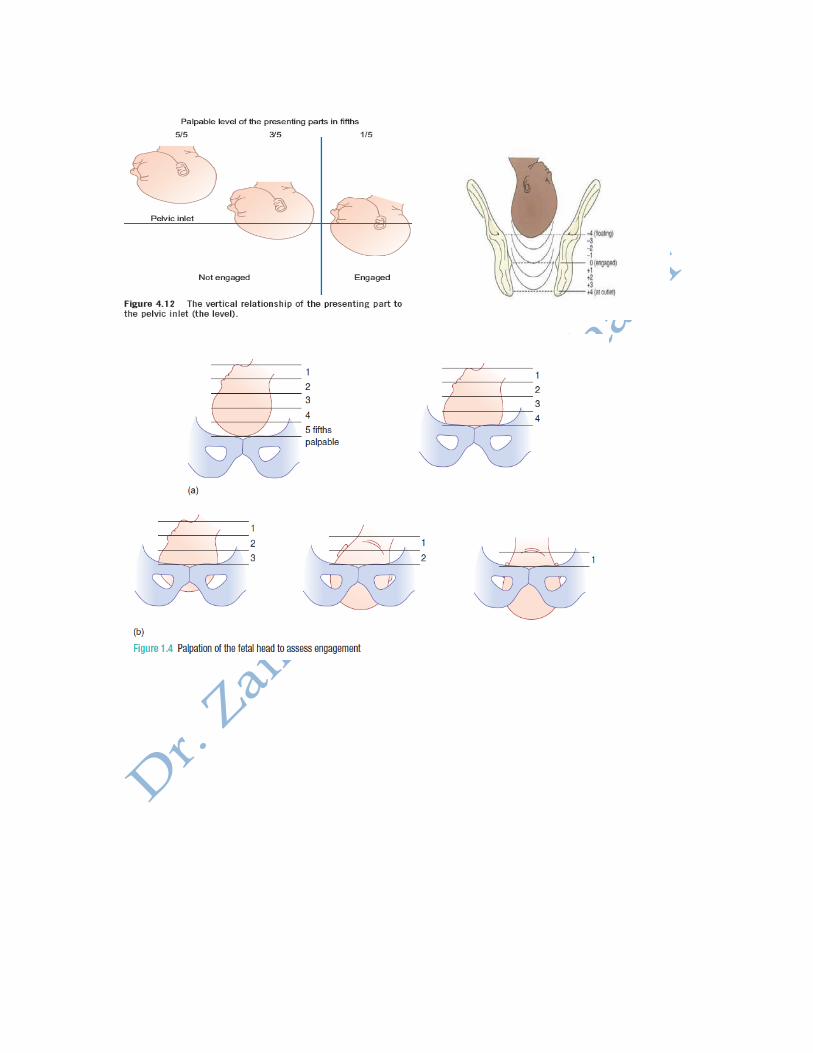
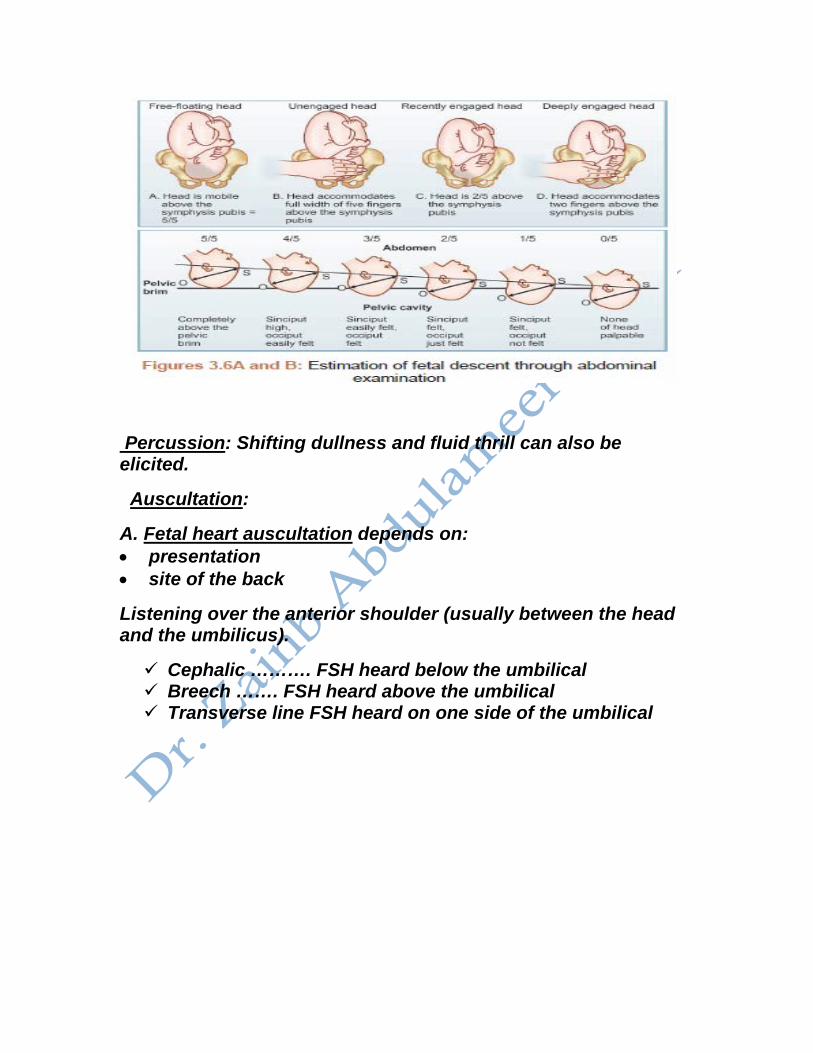
6. Engagement:
Engagement is only applied to cephalic presentation. When the greatest horizontal plane, the biparietal, has
passed the plane of the pelvic brim, the head is said to be engaged.
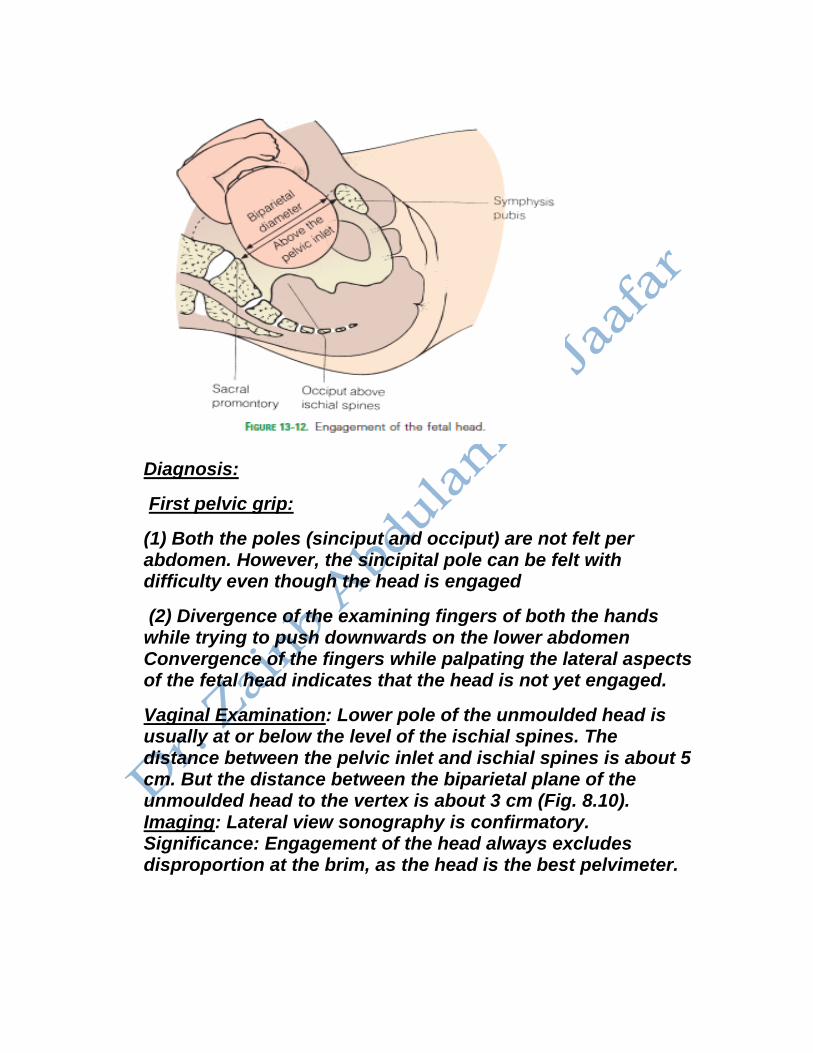
Diagnosis:
First pelvic grip:
(1) Both the poles (sinciput and occiput) are not felt per abdomen. However, the sincipital pole can be felt with difficulty even though the head is engaged
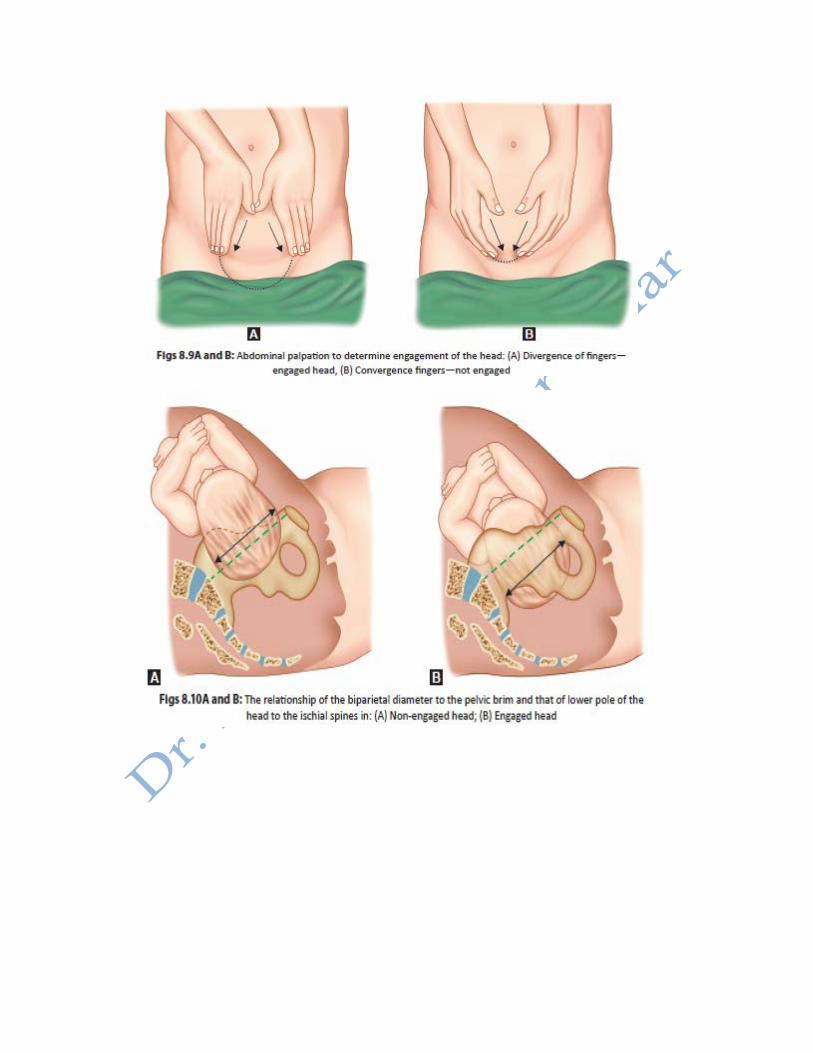
(2) Divergence of the examining fingers of both the hands while trying to push downwards on the lower abdomen Convergence of the fingers while palpating the lateral aspects of the fetal head indicates that the head is not yet engaged.
Vaginal Examination: Lower pole of the unmoulded head is usually at or below the level of the ischial spines. The distance between the pelvic inlet and ischial spines is about 5 cm. But the distance between the biparietal plane of the unmoulded head to the vertex is about 3 cm (Fig. 8.10). Imaging: Lateral view sonography is confirmatory. Significance: Engagement of the head always excludes disproportion at the brim, as the head is the best pelvimeter.
Percussion: Shifting dullness and fluid thrill can also be elicited.
Auscultation:
A. Fetal heart auscultation depends on: • presentation • site of the back
Listening over the anterior shoulder (usually between the head and the umbilicus).
Cephalic ………. FSH heard below the umbilical Breech ……. FSH heard above the umbilical Transverse line FSH heard on one side of the umbilical
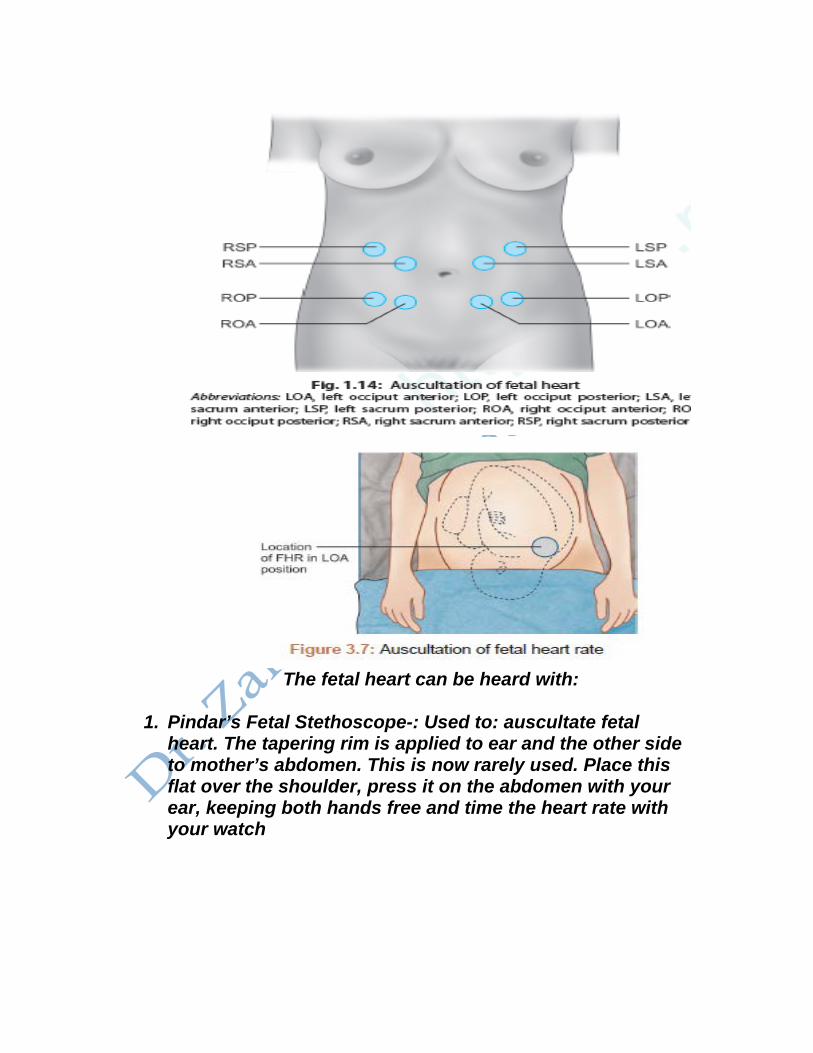
The fetal heart can be heard with:
1. Pindar’s Fetal Stethoscope-: Used to: auscultate fetal
heart. The tapering rim is applied to ear and the other side to mother’s abdomen. This is now rarely used. Place this flat over the shoulder, press it on the abdomen with your ear, keeping both hands free and time the heart rate with your watch
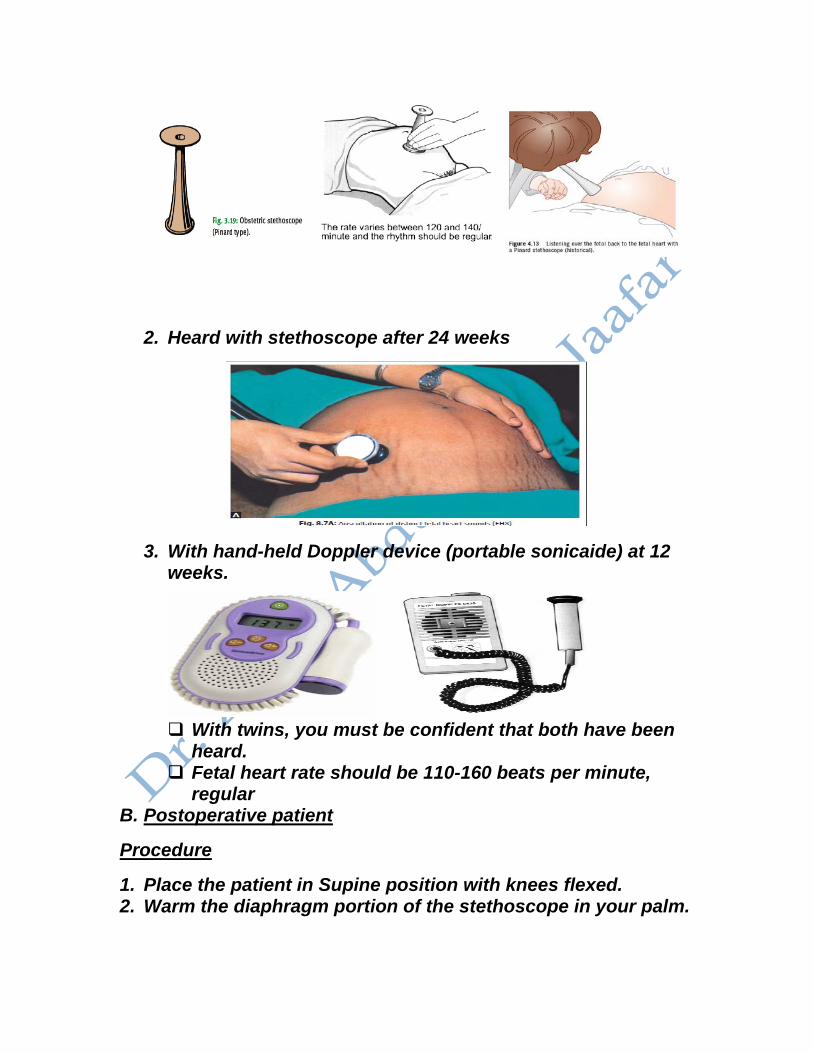
2. Heard with stethoscope after 24 weeks
3. With hand-held Doppler device (portable sonicaide) at 12
weeks.
With twins, you must be confident that both have been
heard. Fetal heart rate should be 110-160 beats per minute,
regular B. Postoperative patient
Procedure
1. Place the patient in Supine position with knees flexed. 2. Warm the diaphragm portion of the stethoscope in your palm.
3. Place it on the beginning quadrant. (The abdomen is divided mentally into four quadrants, you may start in the RLQ and proceed counter clockwise. See drawing. Or begin in any quadrant and listen to all four), best site at the Mc Burney's point (ileocecal valve at the junction of lateral third with medial two thirds of the line joining the umbilicus and ant. Sup. Iliac spine)
4. listen for 5 minutes to each quadrant before deciding that bowel sounds are absent (20 minutes is unrealistic to expect someone to stand and listen for bowel sounds so we often rely on the patient’s other signs
5. Document the presence or absence of sounds.( Note the character (high-pitched, gurgling, clicking, etc.) and frequency)
6. Normally the sounds occur intermittently at 5-15 times per minute. Judge if the sounds are normal, hypoactive or hyperactive.
Pelvic examination
Prerequisites for a Vaginal Examination
1. The patient must be carefully explained about the examination, prior to performing the examination.
2. Adequate permission must be taken from the patient. 3. There should be a valid reason for performing the
examination. A vaginal examination must always be preceded by an abdominal examination.
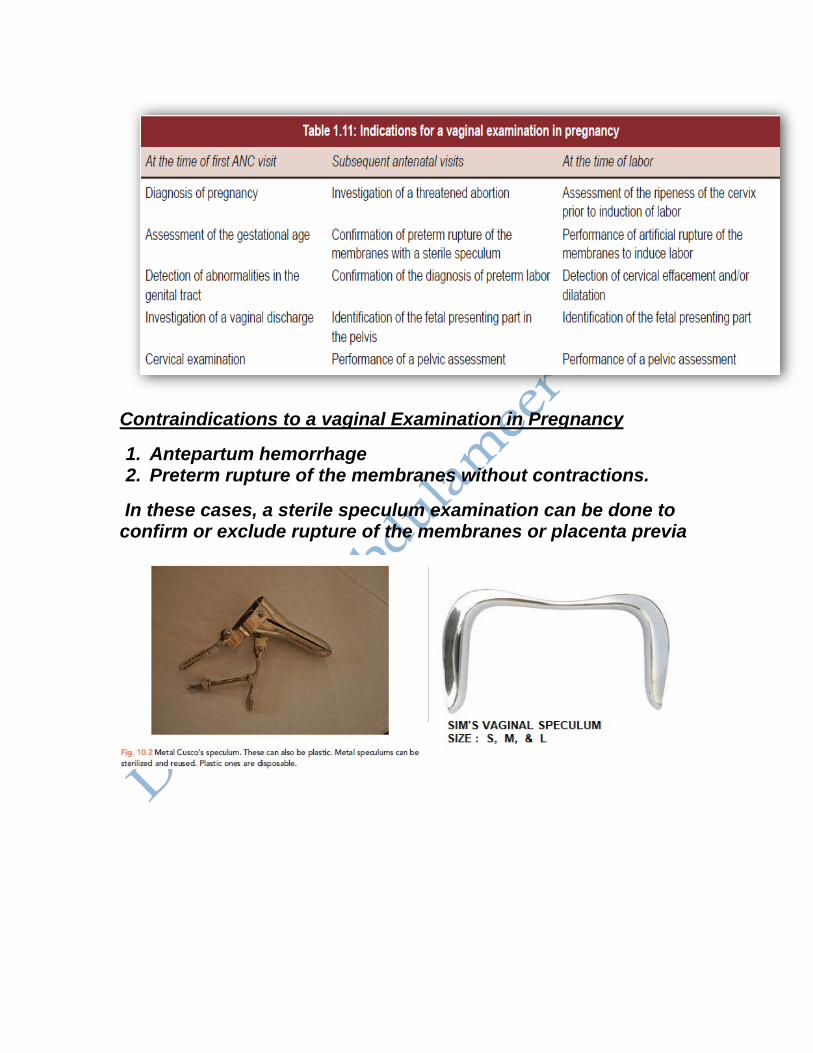
Contraindications to a vaginal Examination in Pregnancy
1. Antepartum hemorrhage 2. Preterm rupture of the membranes without contractions.
In these cases, a sterile speculum examination can be done to confirm or exclude rupture of the membranes or placenta previa






























