Embed Size (px)
Citation preview

The Old Man’s Friend No More:Disability & Cognitive Decline
After Acute Infection
Theodore J. Iwashyna, MD, PhDUniversity of Michigan
Ann Arbor VA Center for Clinical Management Research
5 December 2013 – DuPRI Seminar Series
Disclosures•Key Funding:
•U.S. NIH K08 HL091249 (TJI)•U.S. NIH U01 AG09740 (HRS)•U.S. VA HSR&D IIR 11-109 (TJI)
•This work does not necessarily represent the views of the U.S. Government or Department of Veterans Affairs
•I have no relevant financial conflicts of interest to disclose
•I thank the organizers for the opportunity to join you today
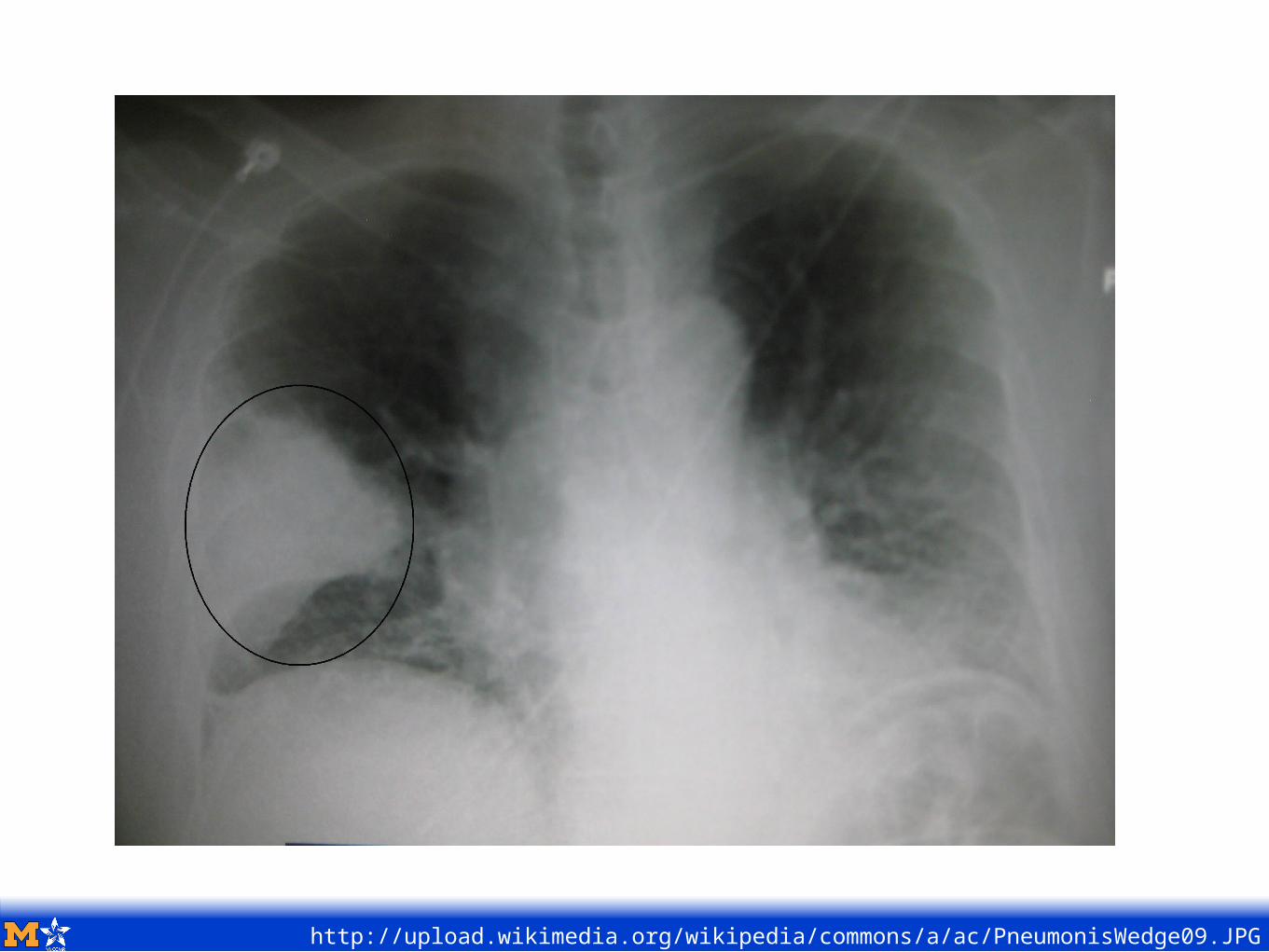
http://upload.wikimedia.org/wikipedia/commons/a/ac/PneumonisWedge09.JPG
http://upload.wikimedia.org/wikipedia/commons/a/ac/PneumonisWedge09.JPG
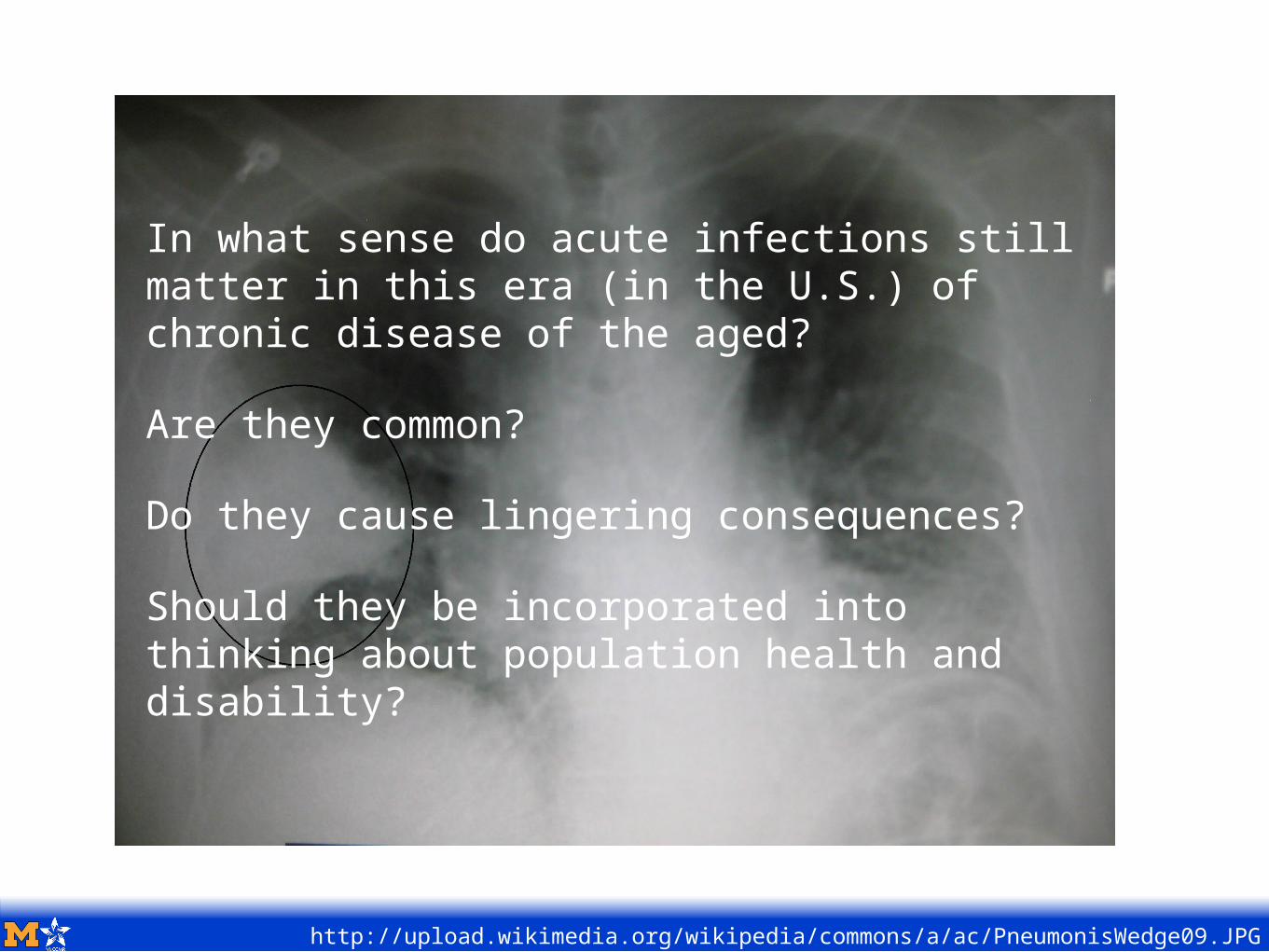
In what sense do acute infections still matter in this era (in the U.S.) of chronic disease of the aged?
Are they common?
Do they cause lingering consequences?
Should they be incorporated into thinking about population health and disability?
Today’s Agenda:
Prologue: When you die with heart disease, what do you die from?
Chapter 1: Sepsis Biology & Epidemiology 101
Chapter 2: Disability & Cognitive Dysfunction
Chapter 3: Life Course Matters
Chapter 4: Population Impact
Epilogue: Summary & What’s Next
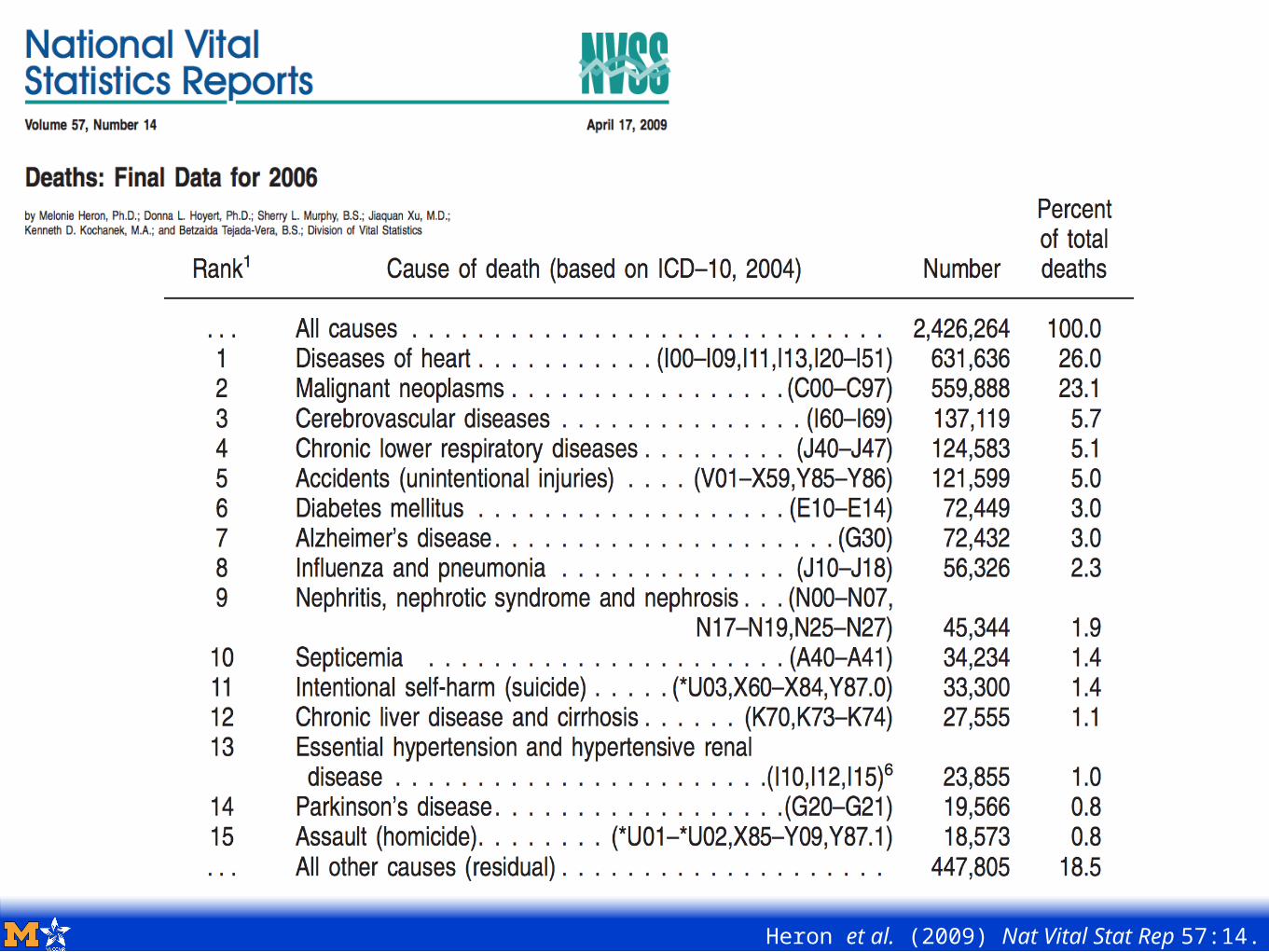
Heron et al. (2009) Nat Vital Stat Rep 57:14.
Death certificates are known to have substantial problems with accuracy compared to medical chart review, and there remains substantial uncertainty in how “underlying cause of death” is interpreted
A majority of older Americans die during an inpatient hospitalization
Hospitalization diagnoses are heavily audited for accuracy, with financial penalties for mistakes (unlike death certificates)
So we asked: for older Americans who die during an inpatient stay, how similar are the pictures that emerge from their hospitalization records and their death certificates?
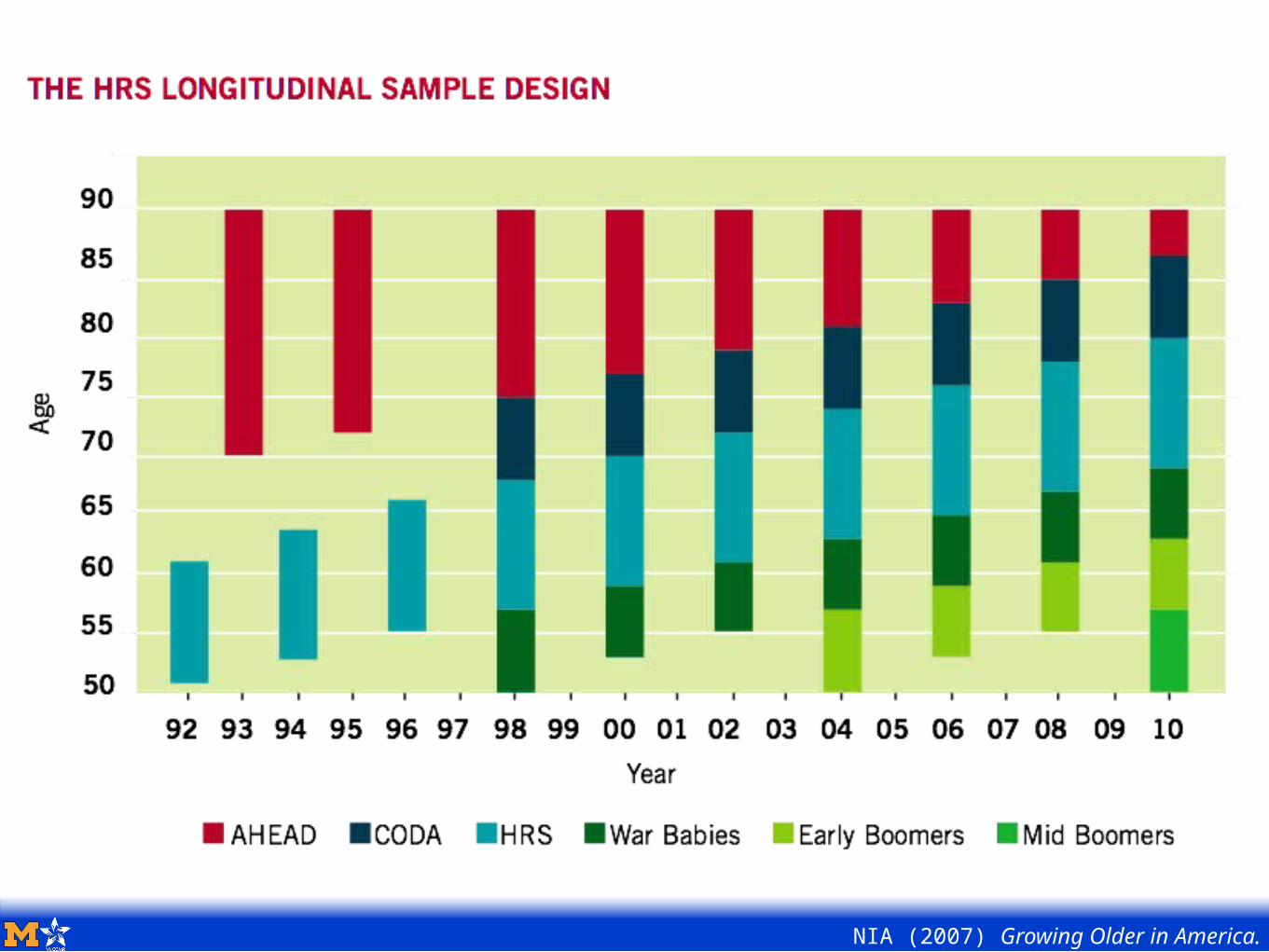
NIA (2007) Growing Older in America.
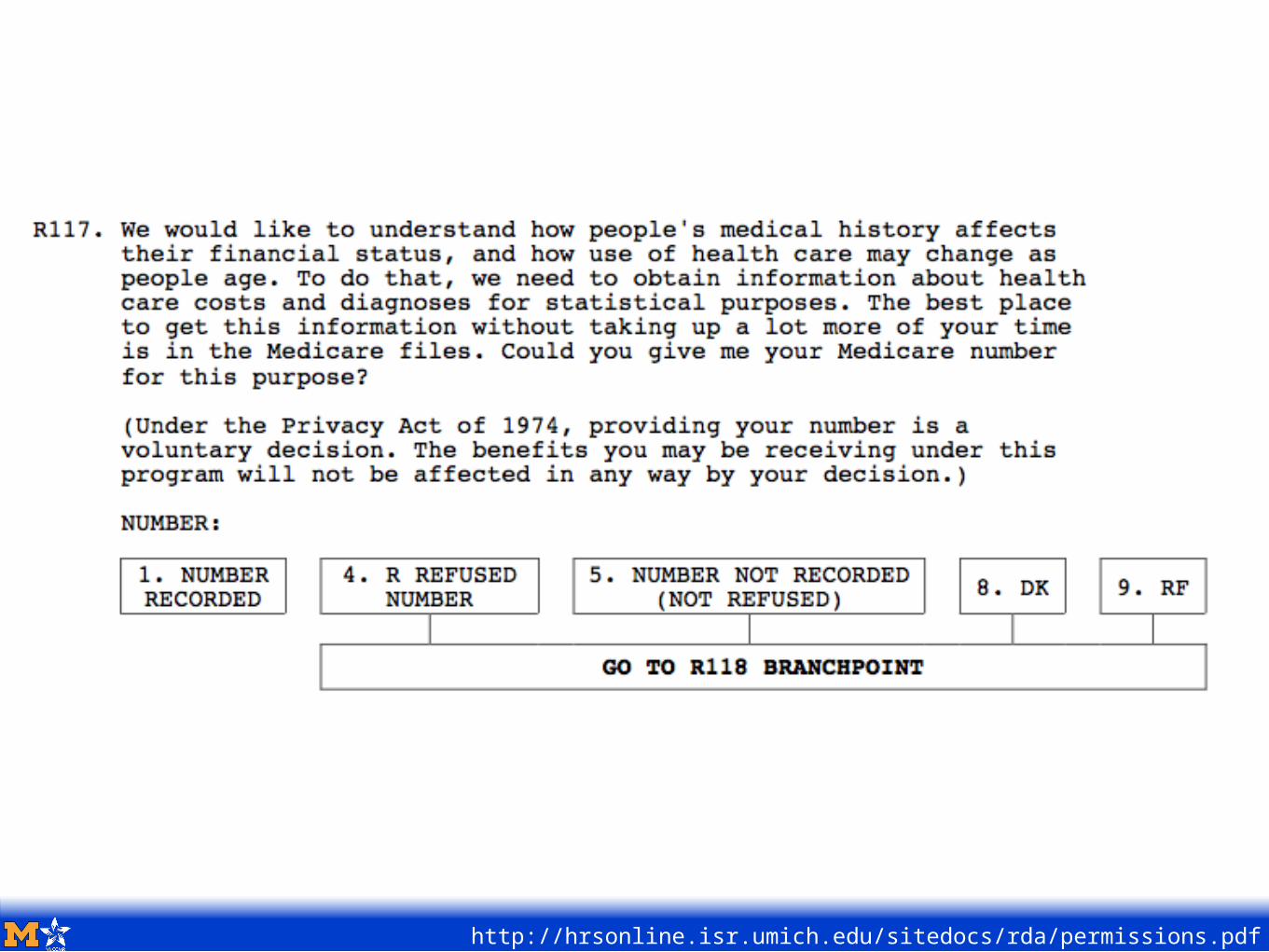
http://hrsonline.isr.umich.edu/sitedocs/rda/permissions.pdf
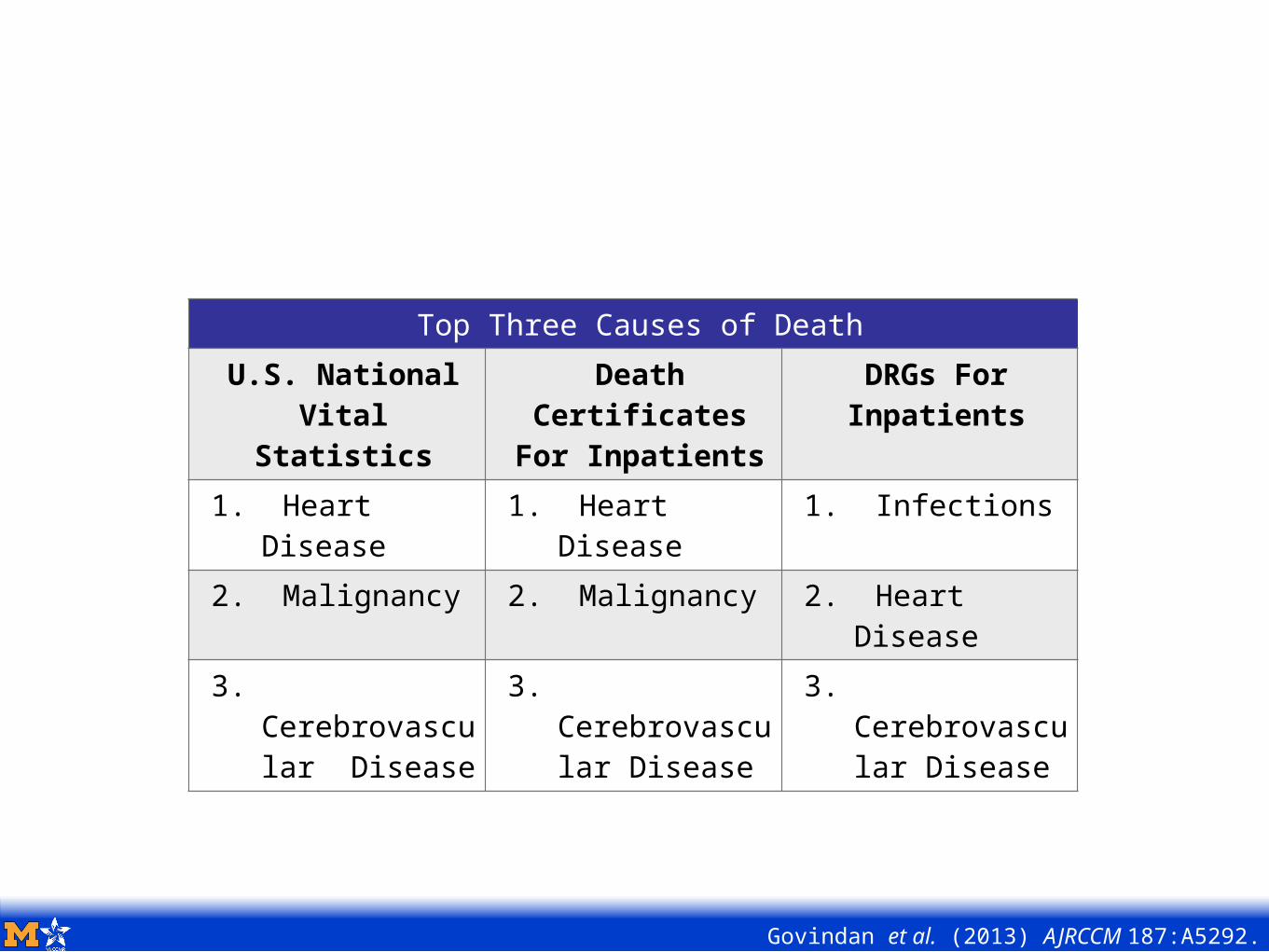
Govindan et al. (2013) AJRCCM 187:A5292.
For older Americans who die during an inpatient stay, how similar are the pictures that emerge from their hospitalization records and their death certificates?
Population: Death among HRS-Medicare Cohort where date of death was same as date of discharge from last hospitalization.
Causes of death abstracted from death certificates, then aggregated to National Center for Health Statistics List of 50 Rankable Causes of Death.
Reasons for hospitalization (CMS-DRGs) were manually aggregated into a parallel classification by blinded physician.
Influenza, pneumonia and sepsis combined into “Infections”
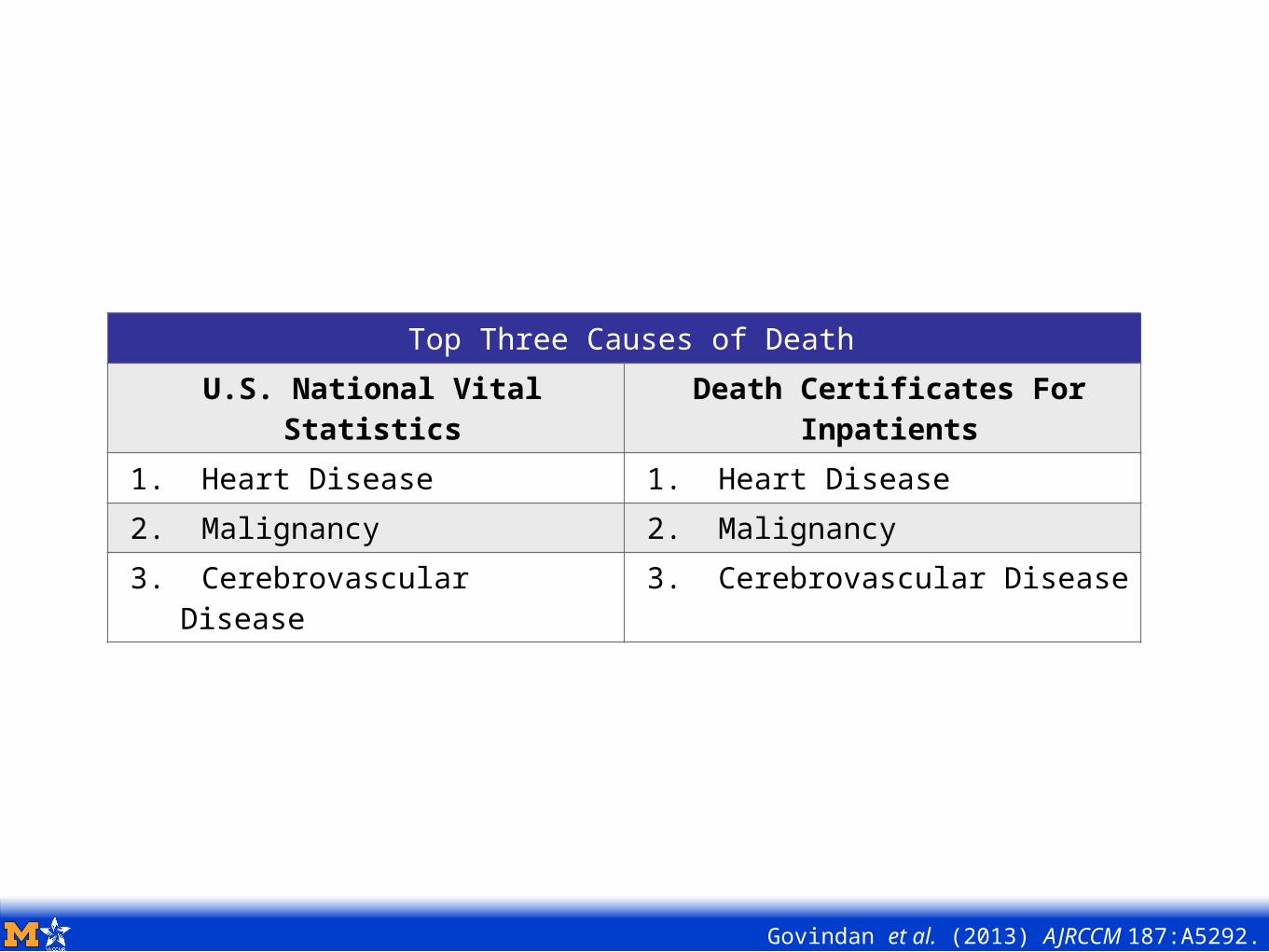
Top Three Causes of DeathU.S. National Vital
StatisticsDeath Certificates For
Inpatients1. Heart Disease 1. Heart Disease2. Malignancy 2. Malignancy3. Cerebrovascular
Disease3. Cerebrovascular Disease
Govindan et al. (2013) AJRCCM 187:A5292.
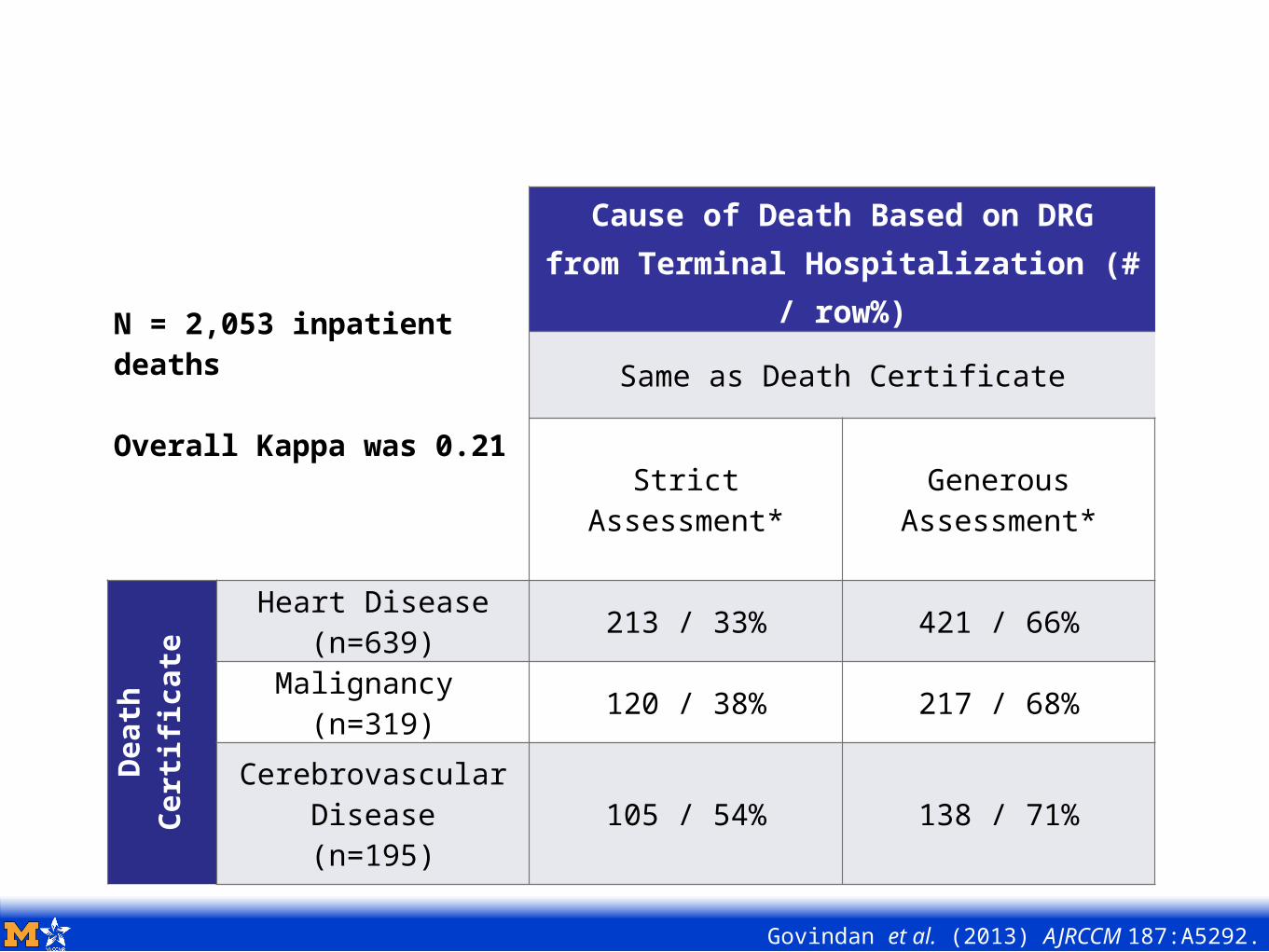
N = 2,053 inpatient deaths
Overall Kappa was 0.21
Cause of Death Based on DRGfrom Terminal Hospitalization (#
/ row%)
Same as Death Certificate
StrictAssessment*
Generous Assessment*
Death
Certificate
Heart Disease(n=639) 213 / 33% 421 / 66%
Malignancy (n=319) 120 / 38% 217 / 68%
Cerebrovascular Disease(n=195)
105 / 54% 138 / 71%
Govindan et al. (2013) AJRCCM 187:A5292.
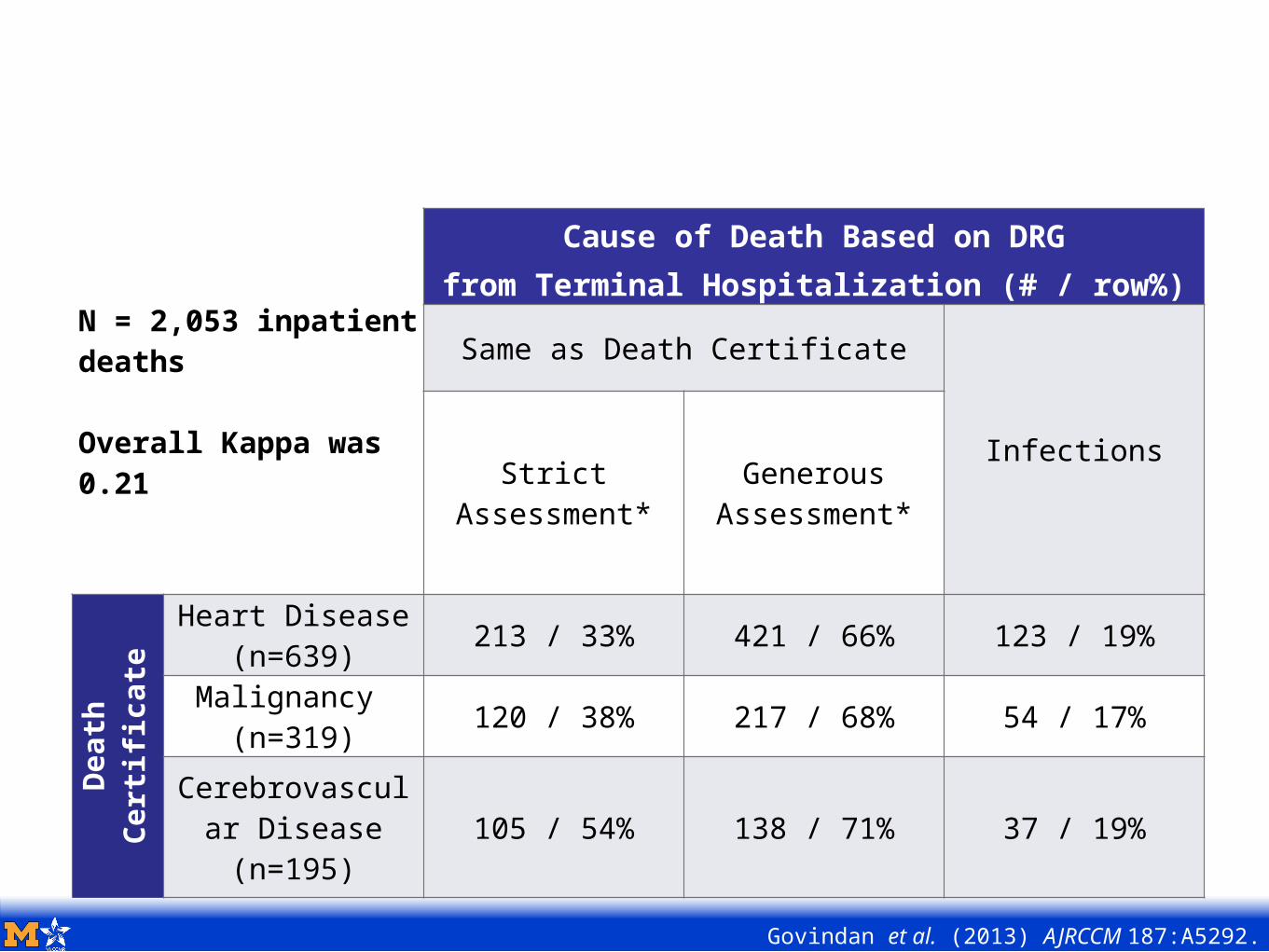
N = 2,053 inpatient deaths
Overall Kappa was 0.21
Cause of Death Based on DRGfrom Terminal Hospitalization (# / row%)
Same as Death Certificate
InfectionsStrictAssessment*
Generous Assessment*
Death
Certificate
Heart Disease(n=639) 213 / 33% 421 / 66% 123 / 19%
Malignancy (n=319) 120 / 38% 217 / 68% 54 / 17%
Cerebrovascular Disease(n=195)
105 / 54% 138 / 71% 37 / 19%
Govindan et al. (2013) AJRCCM 187:A5292.
Govindan et al. (2013) AJRCCM 187:A5292.
Top Three Causes of DeathU.S. National
Vital Statistics
Death CertificatesFor Inpatients
DRGs For Inpatients
1. Heart Disease
1. Heart Disease
1. Infections
2. Malignancy 2. Malignancy 2. Heart Disease
3. Cerebrovascular Disease
3. Cerebrovascular Disease
3. Cerebrovascular Disease
Today’s Agenda:
Prologue: When you die with heart disease, what do you die from?
Chapter 1: Sepsis Biology & Epidemiology 101
Chapter 2: Disability & Cognitive Dysfunction
Chapter 3: Life Course Matters
Chapter 4: Population Impact
Epilogue: Summary & What’s Next
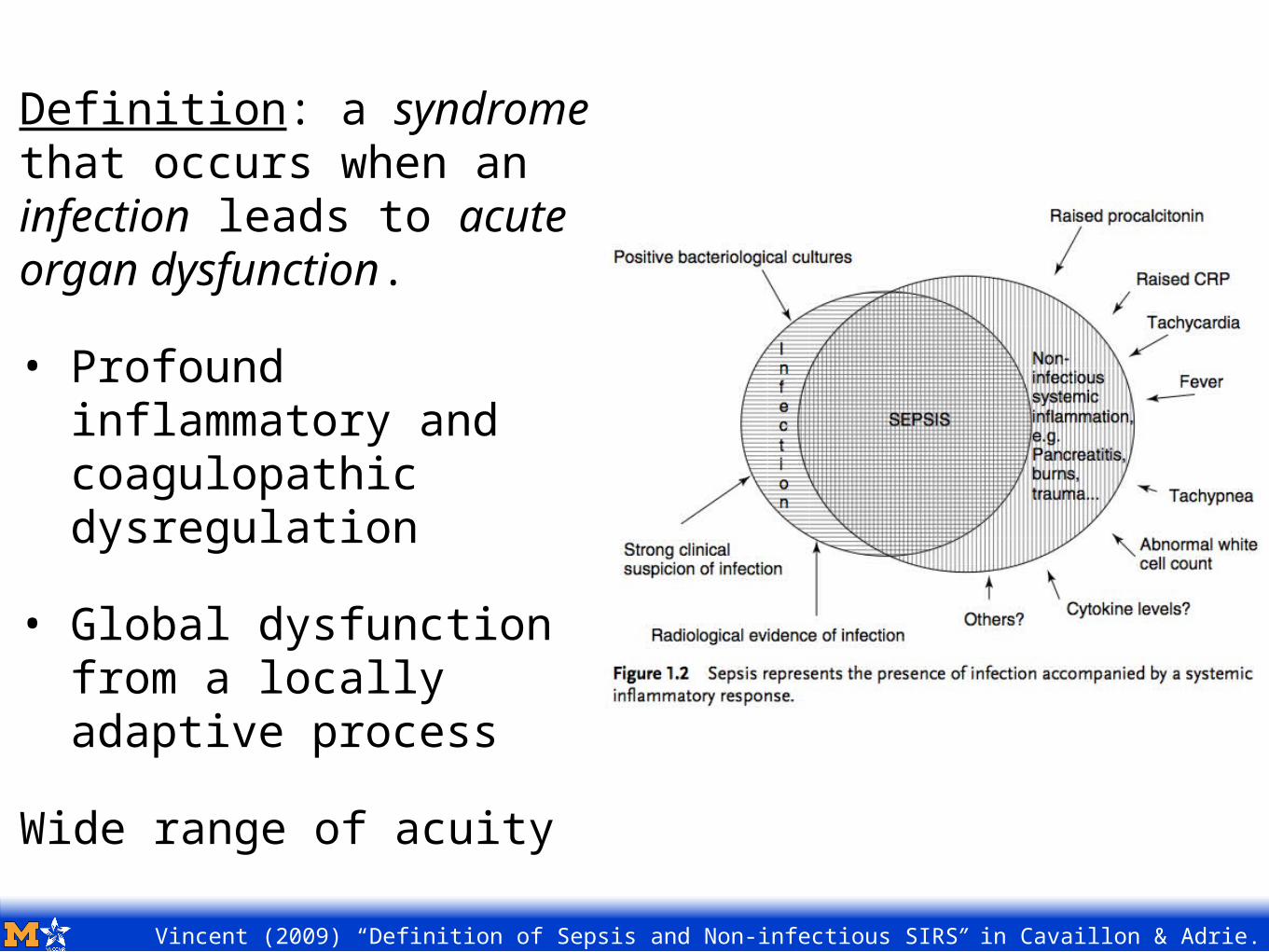
Vincent (2009) “Definition of Sepsis and Non-infectious SIRS” in Cavaillon & Adrie.
Definition: a syndrome that occurs when an infection leads to acute organ dysfunction.
• Profound inflammatory and coagulopathic dysregulation
• Global dysfunction from a locally adaptive process
Wide range of acuity
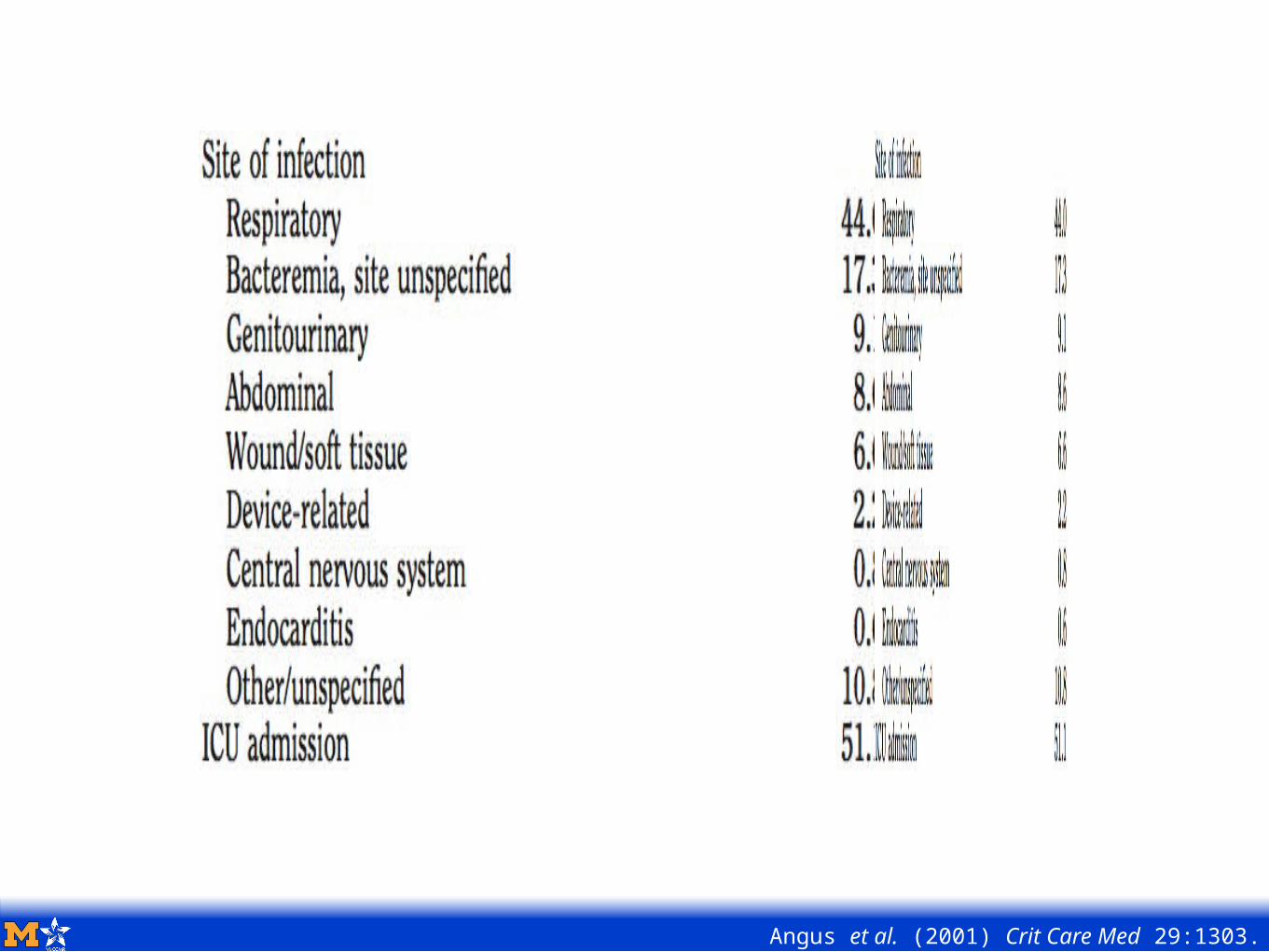
Angus et al. (2001) Crit Care Med 29:1303.
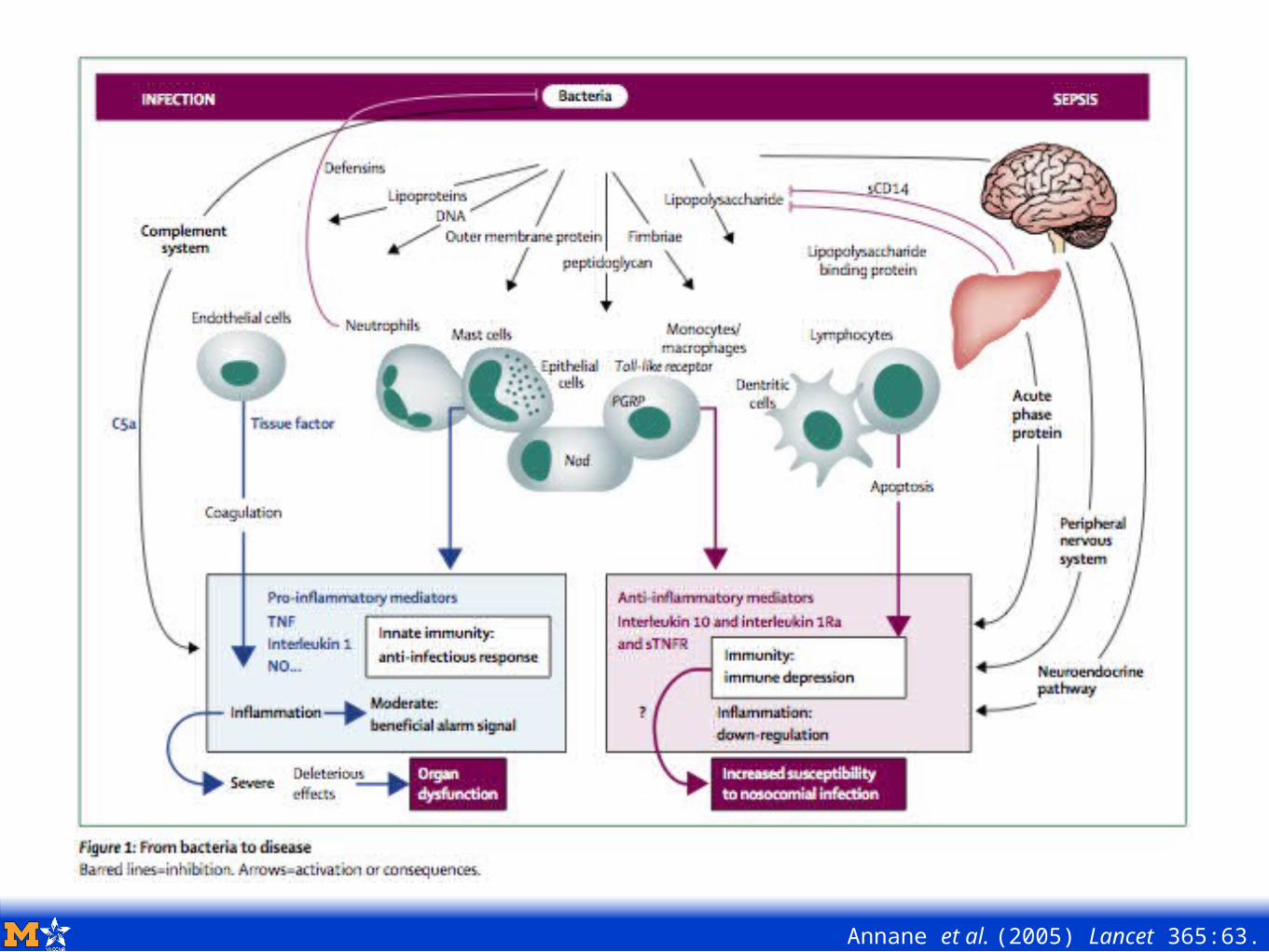
Annane et al. (2005) Lancet 365:63.

Sepsis as we were taught:• Hospital-Acquired• Procedure-Associated• An ICU Disease• Uniformly Acutely Devastating

The New Data:• Community-Acquired• Common• A Spectrum of Disease
• Most Survive• Dramatic Opportunities for Improvement
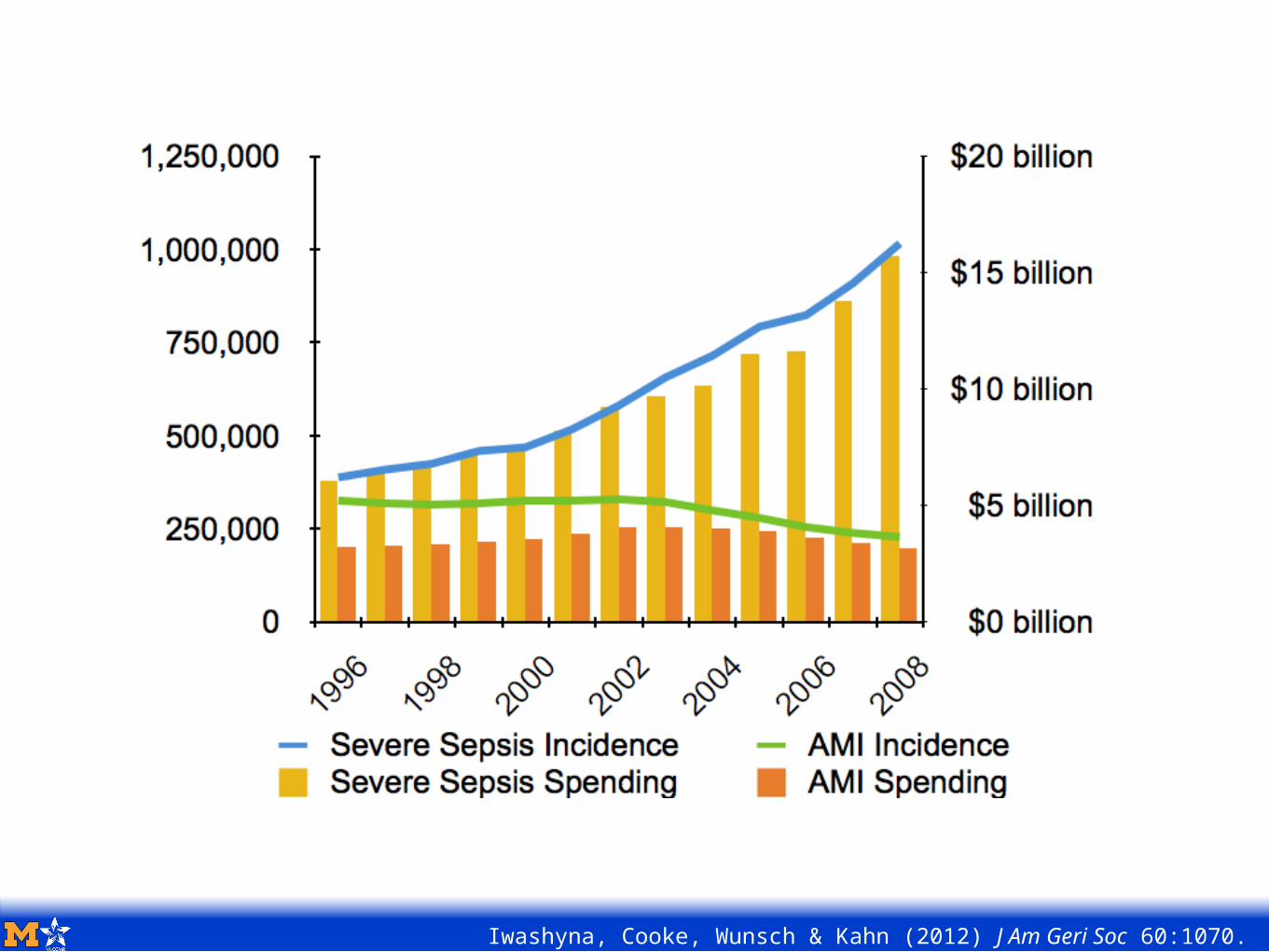
Iwashyna, Cooke, Wunsch & Kahn (2012) J Am Geri Soc 60:1070.
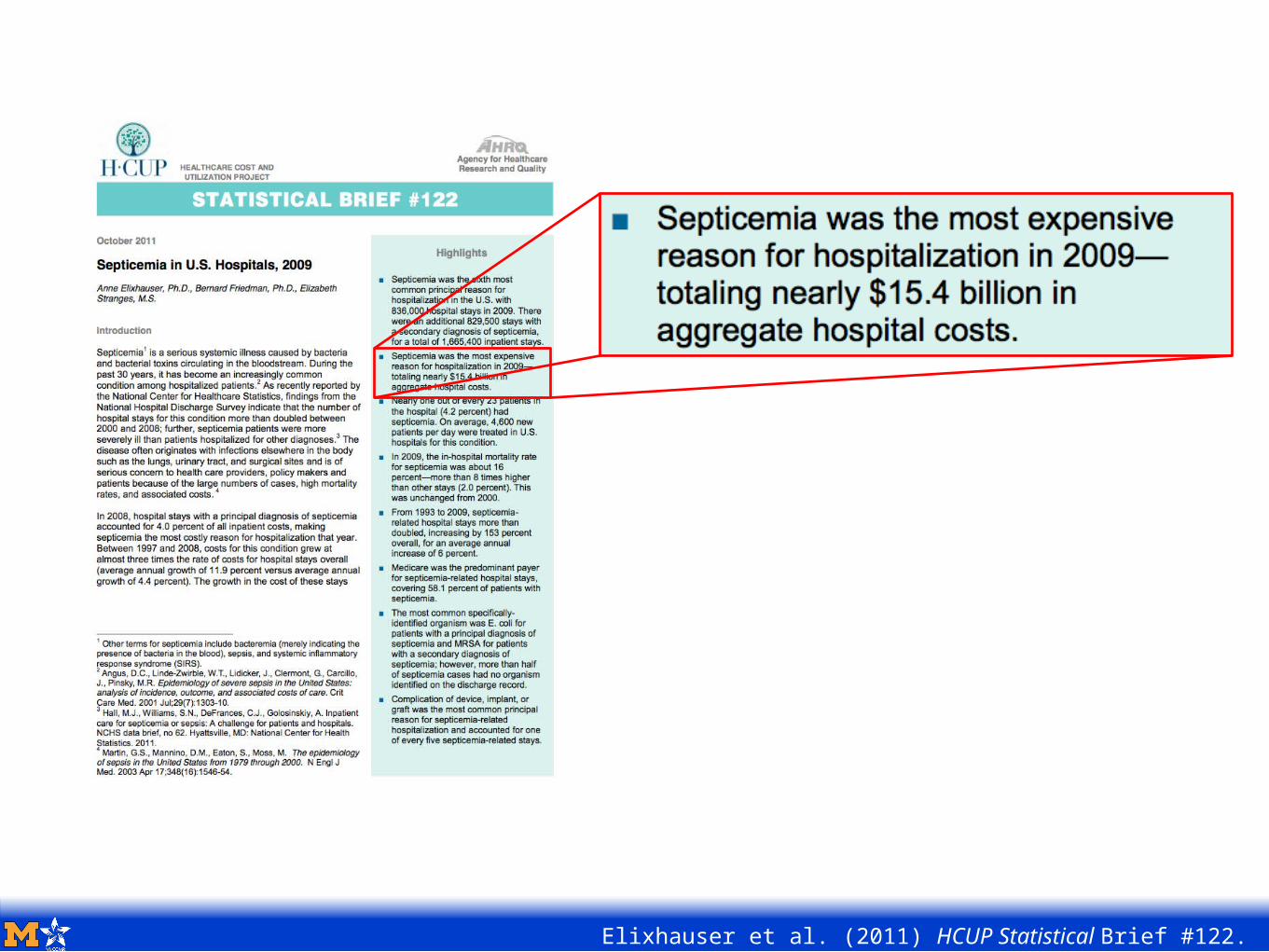
Elixhauser et al. (2011) HCUP Statistical Brief #122.
Today’s Agenda:
Prologue: When you die with heart disease, what do you die from?
Chapter 1: Sepsis Biology & Epidemiology 101
Chapter 2: Disability & Cognitive Dysfunction
Chapter 3: Life Course Matters
Chapter 4: Population Impact
Epilogue: Summary & What’s Next
Q: Is there a residue in sepsis survivors who have had multi-organ failures or dysfunctions?
A: Most people return to normal or near-normal lives even if they have had severe organ failures. … [Persistent problems are] rare. Most surviving patients come back to being normal.
2004 interview with Gordon Bernard, Assistant Vice-Chancellor for Research, Melinda Owen Bass Professor of Medicine and Director, Division of Allergy, Pulmonary and Critical Care Medicine, Vanderbilt University Medical Center.
Frontline (2004) Vol:21 Iss:20 URL: http://www.flonnet.com/fl2120/stories/20041008001708600.htm
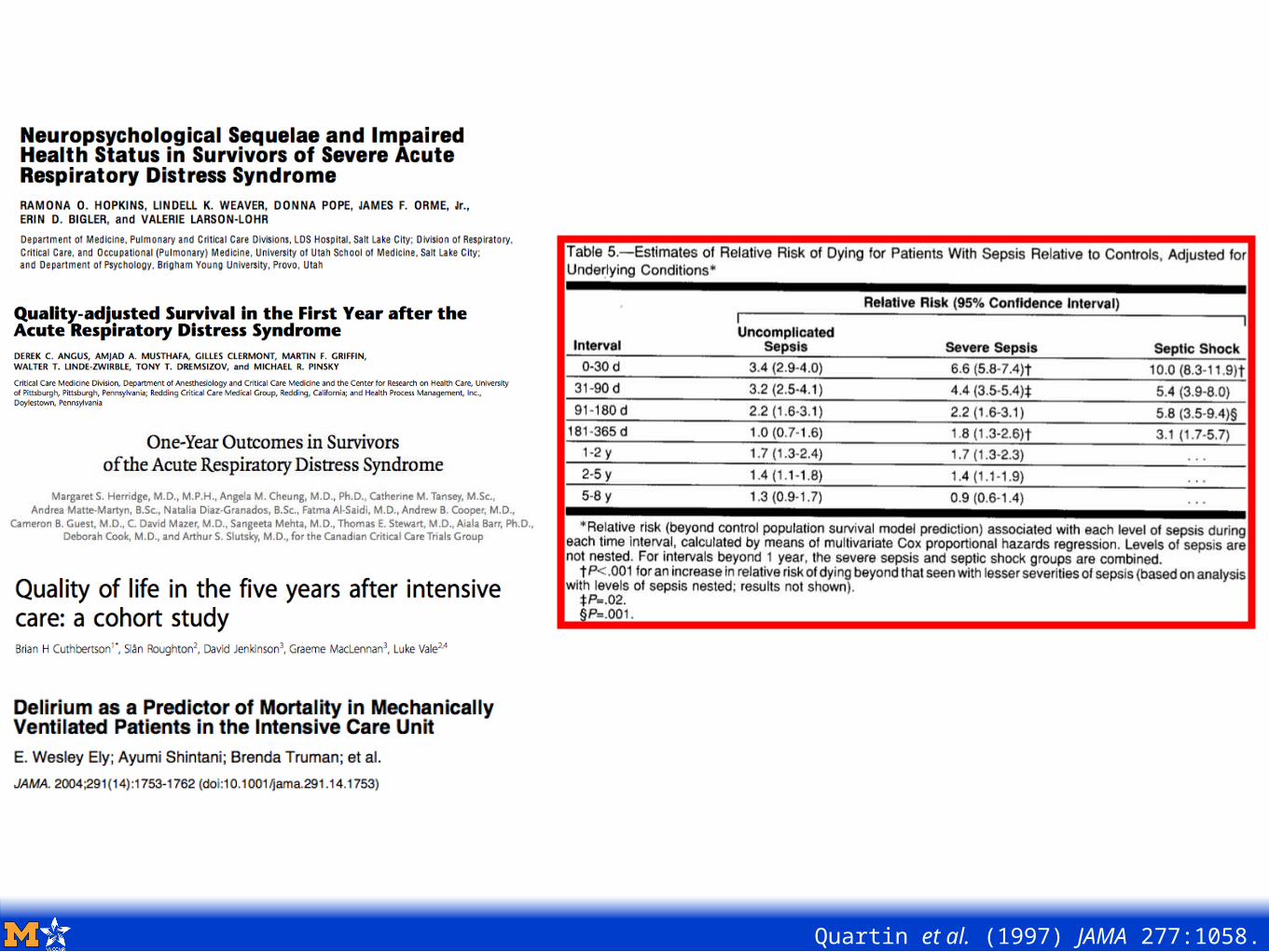
Quartin et al. (1997) JAMA 277:1058.
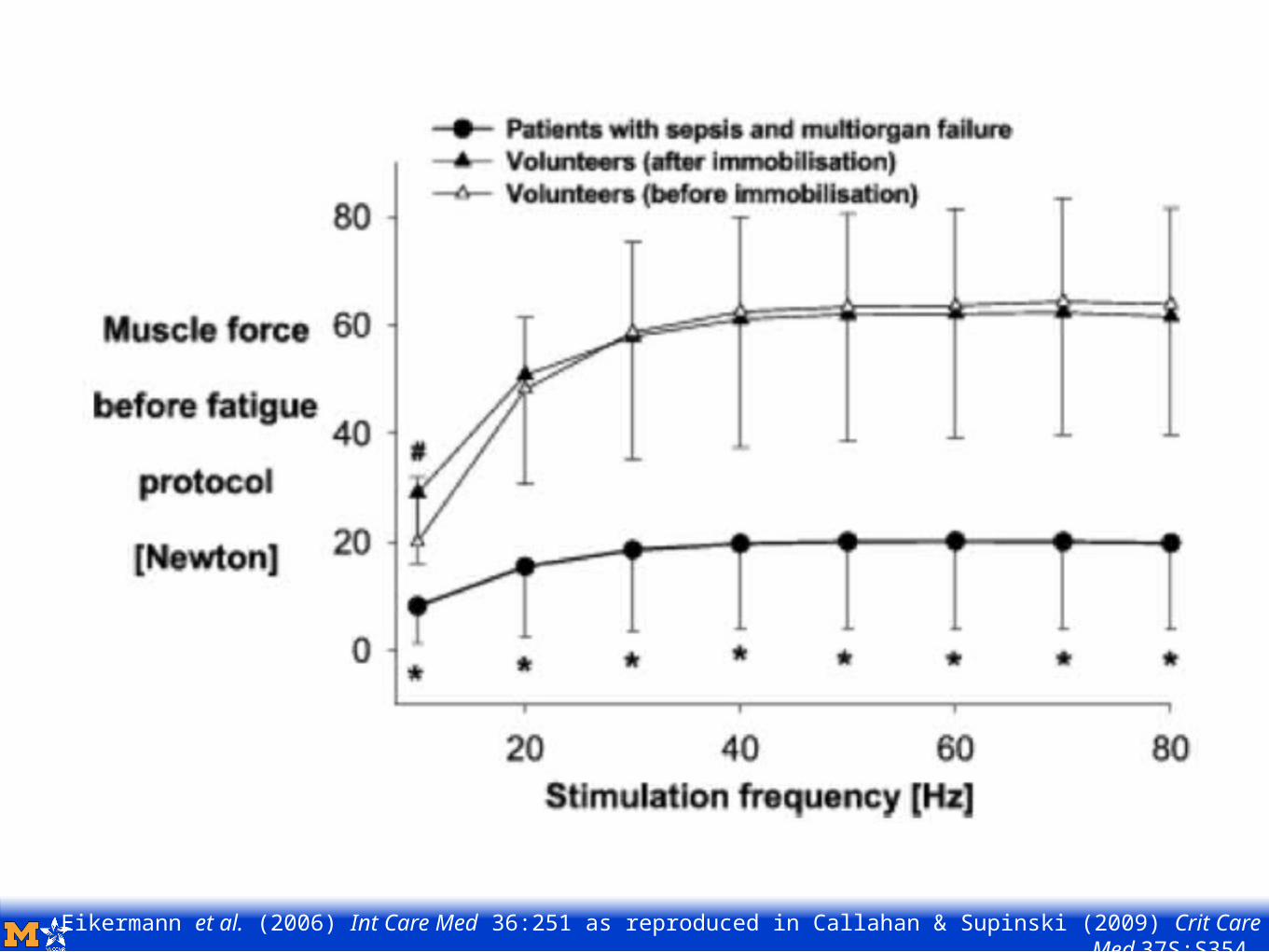
Eikermann et al. (2006) Int Care Med 36:251 as reproduced in Callahan & Supinski (2009) Crit Care Med 37S:S354.
“That which does not kill you, makes you weaker”.
- Christopher Hitchens in Vanity Fair, January, 2012
1998
2000
2002
2004
2006
Worsen
ing
Disabi
lity
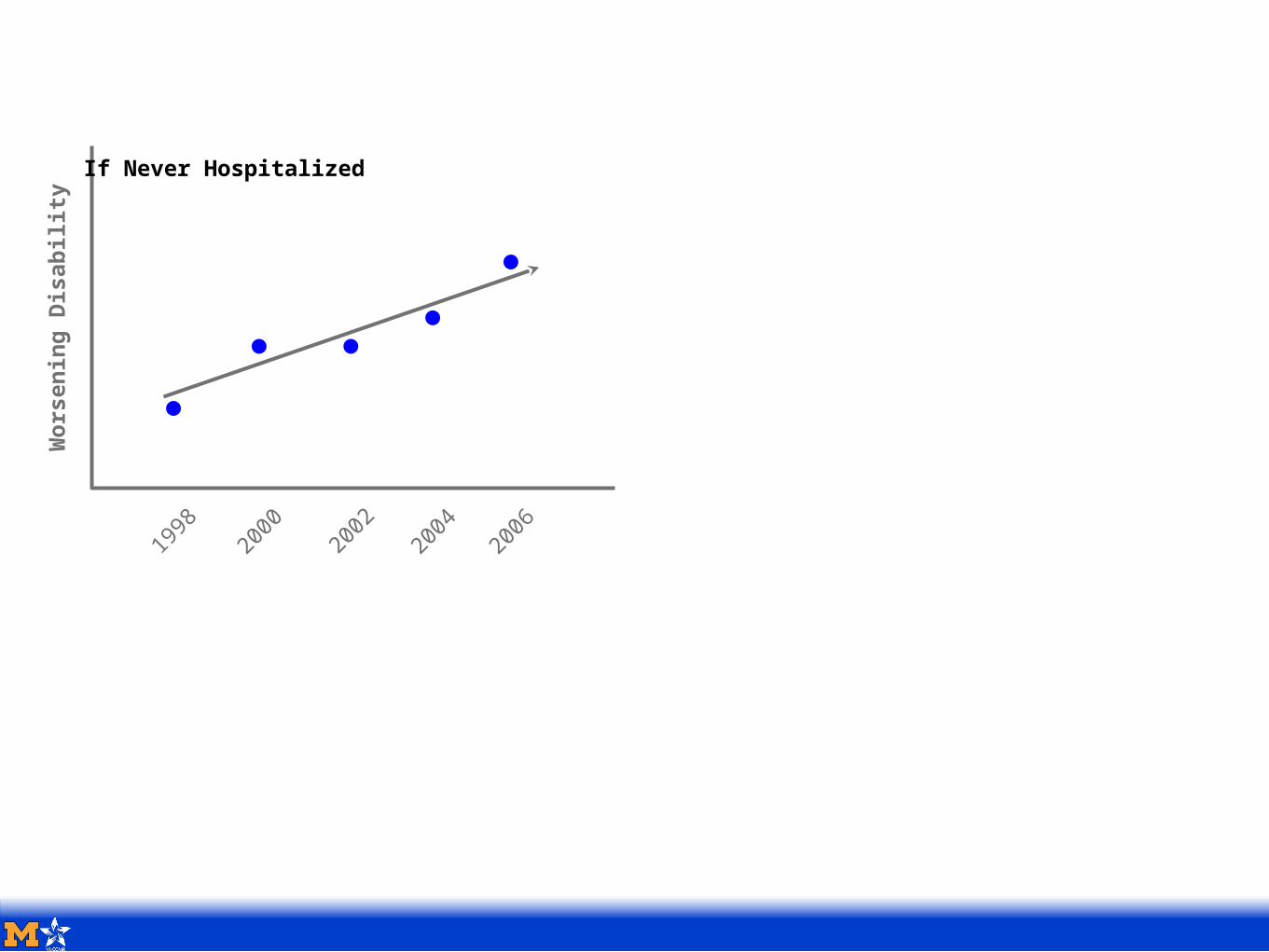
If Never Hospitalized
1998
2000
2002
2004
2006
Worsen
ing
Disabi
lity
If Never Hospitalized
1998 20
002002
2004
2006
Wors
enin
g Di
sabili
ty
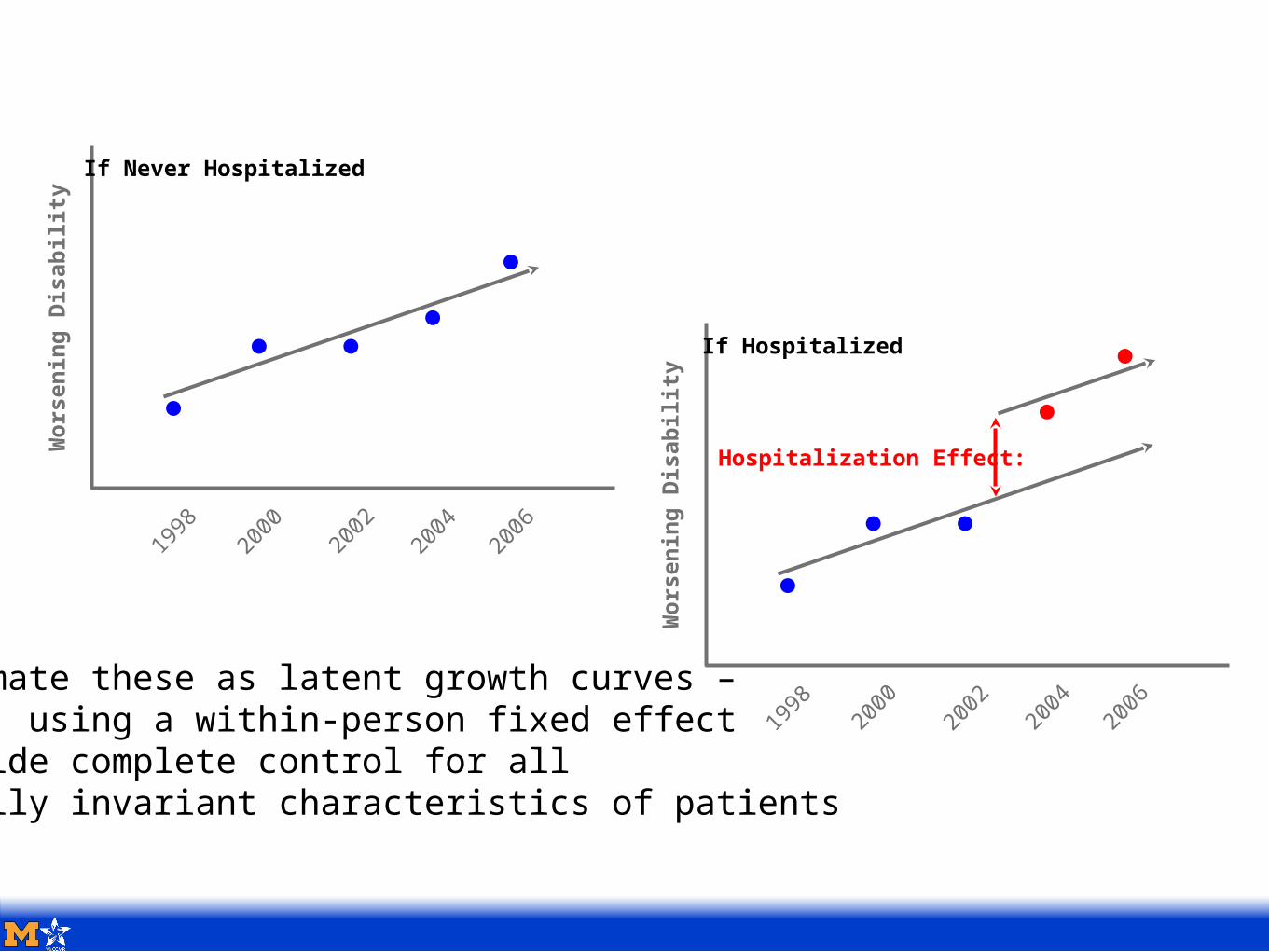
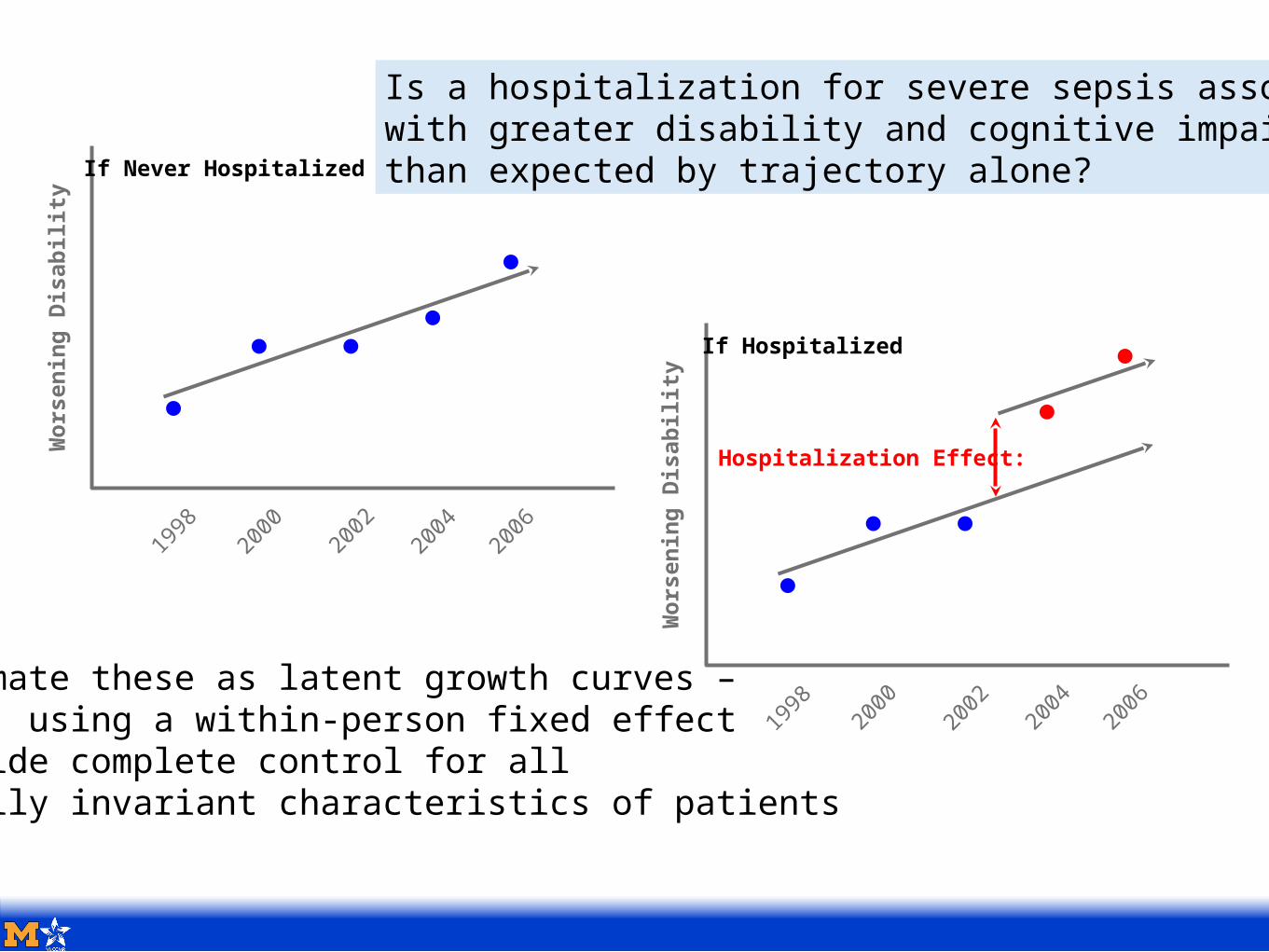
If Hospitalized
Hospitalization Effect:
We estimate these as latent growth curves – that is, using a within-person fixed effectto provide complete control for alltemporally invariant characteristics of patients
1998
2000
2002
2004
2006
Worsen
ing
Disabi
lity
If Never Hospitalized
1998 20
002002
2004
2006
Wors
enin
g Di
sabili
ty
If Hospitalized
Hospitalization Effect:
We estimate these as latent growth curves – that is, using a within-person fixed effectto provide complete control for alltemporally invariant characteristics of patients
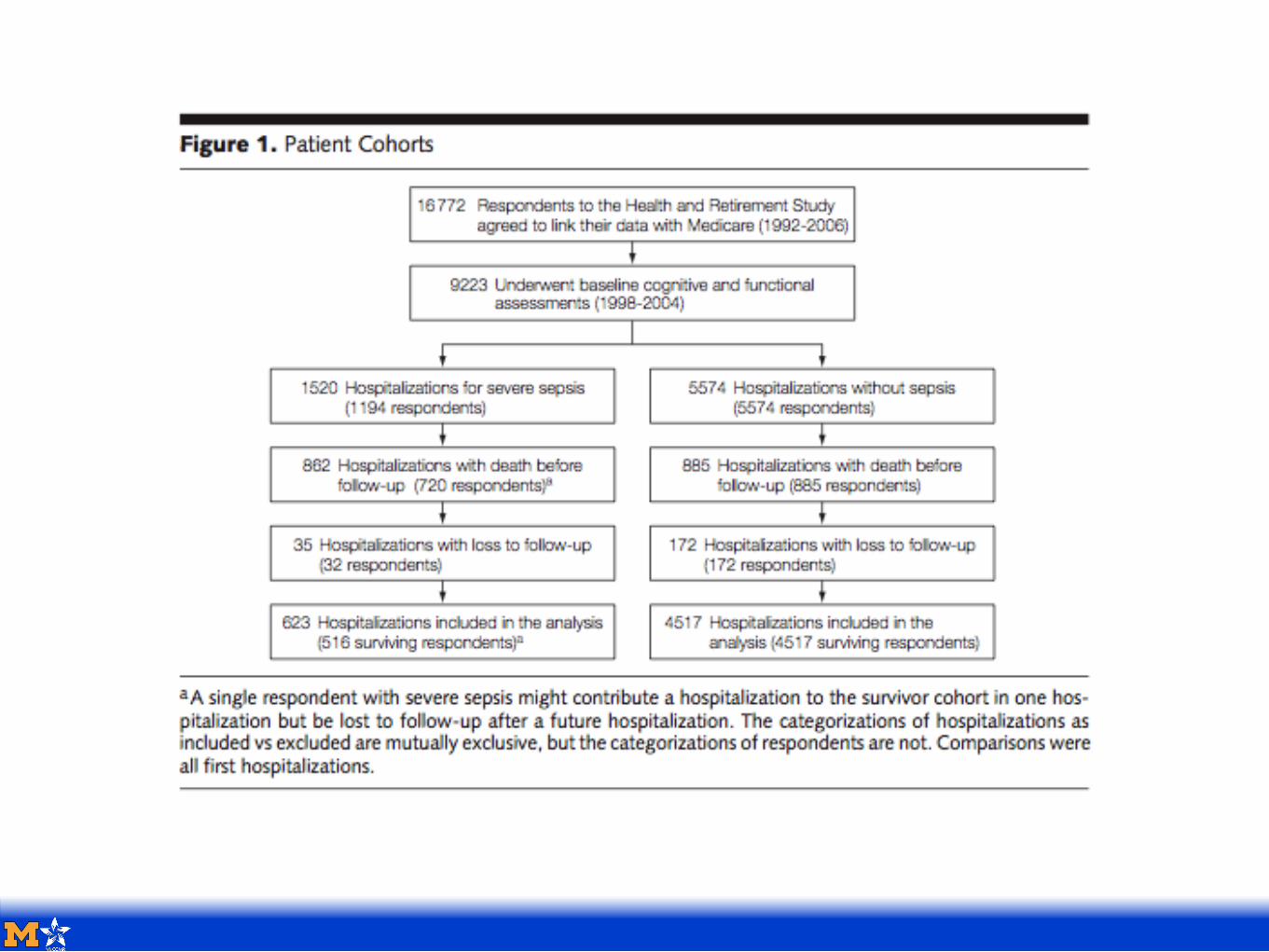
Is a hospitalization for severe sepsis associatedwith greater disability and cognitive impairmentthan expected by trajectory alone?
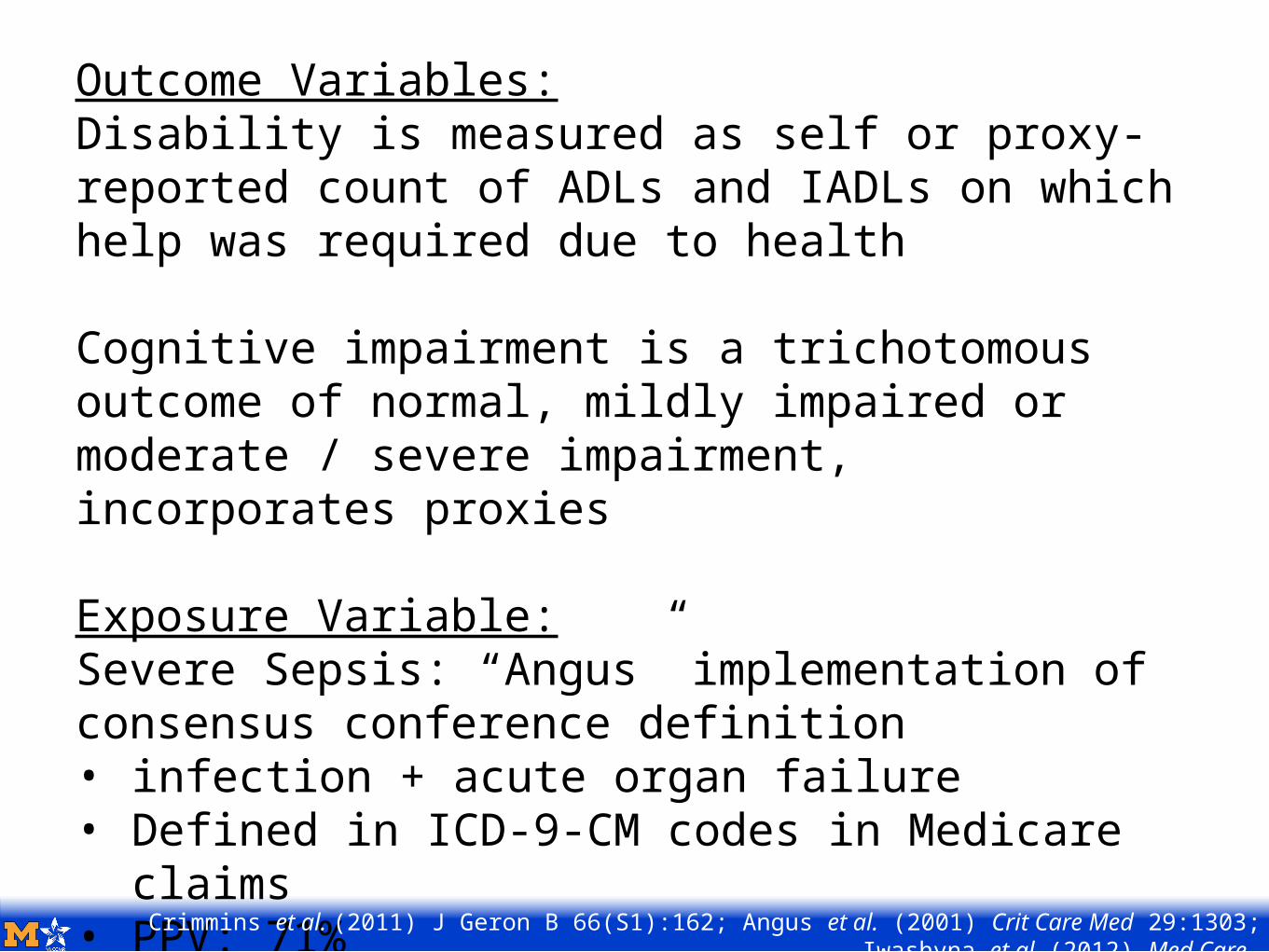
Outcome Variables:Disability is measured as self or proxy-reported count of ADLs and IADLs on which help was required due to health
Cognitive impairment is a trichotomous outcome of normal, mildly impaired or moderate / severe impairment, incorporates proxies
Exposure Variable:Severe Sepsis: “Angus” implementation of consensus conference definition• infection + acute organ failure• Defined in ICD-9-CM codes in Medicare
claims• PPV: 71%Crimmins et al. (2011) J Geron B 66(S1):162; Angus et al. (2001) Crit Care Med 29:1303;
Iwashyna et al (2012) Med Care.
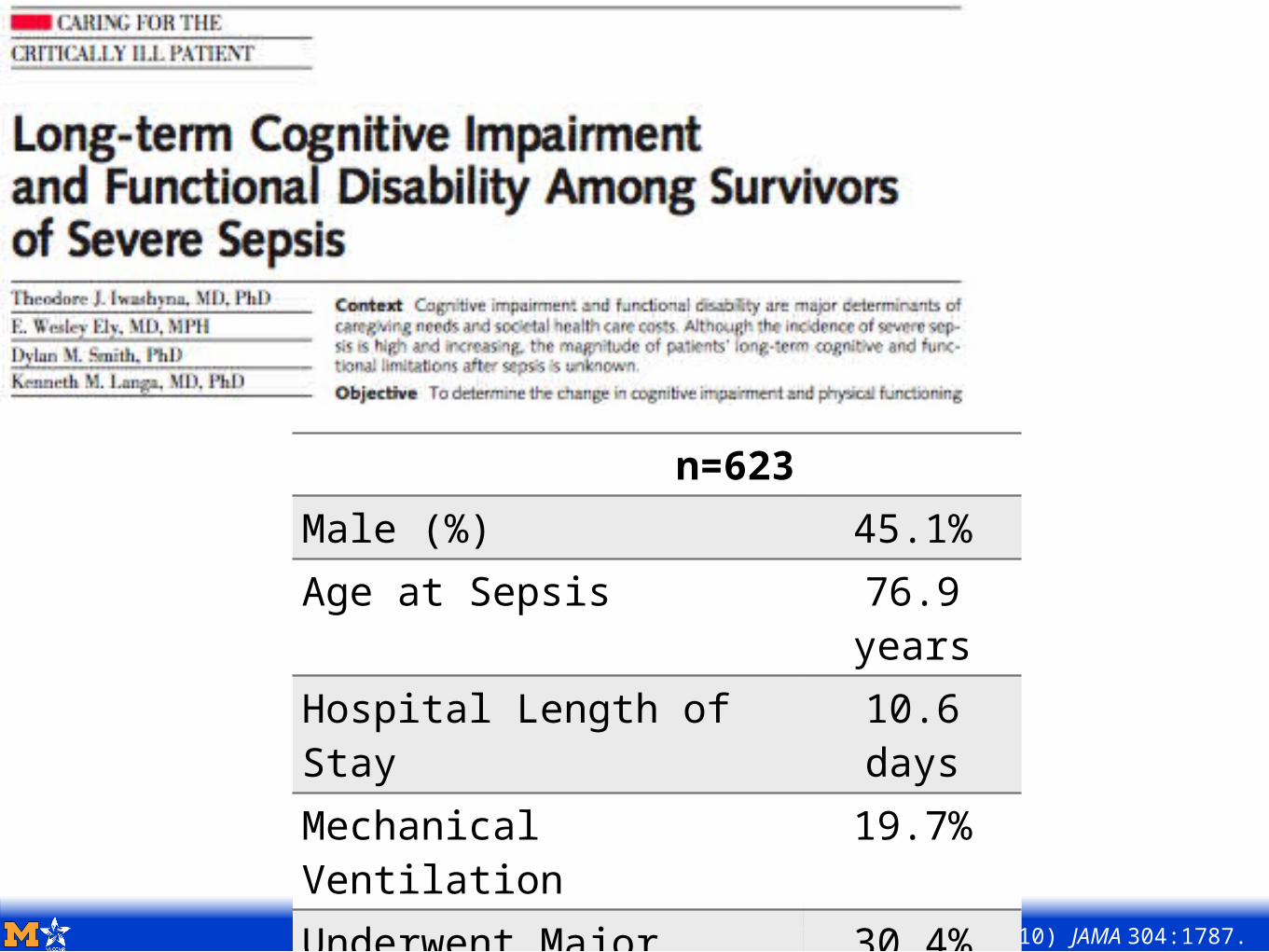
Iwashyna et al. (2010) JAMA 304:1787.
n=623Male (%) 45.1%Age at Sepsis 76.9
yearsHospital Length of Stay
10.6 days
Mechanical Ventilation
19.7%
Underwent Major Surgery
30.4%
Used Critical Care 43.2%Organ Dysfunction Score
1.1
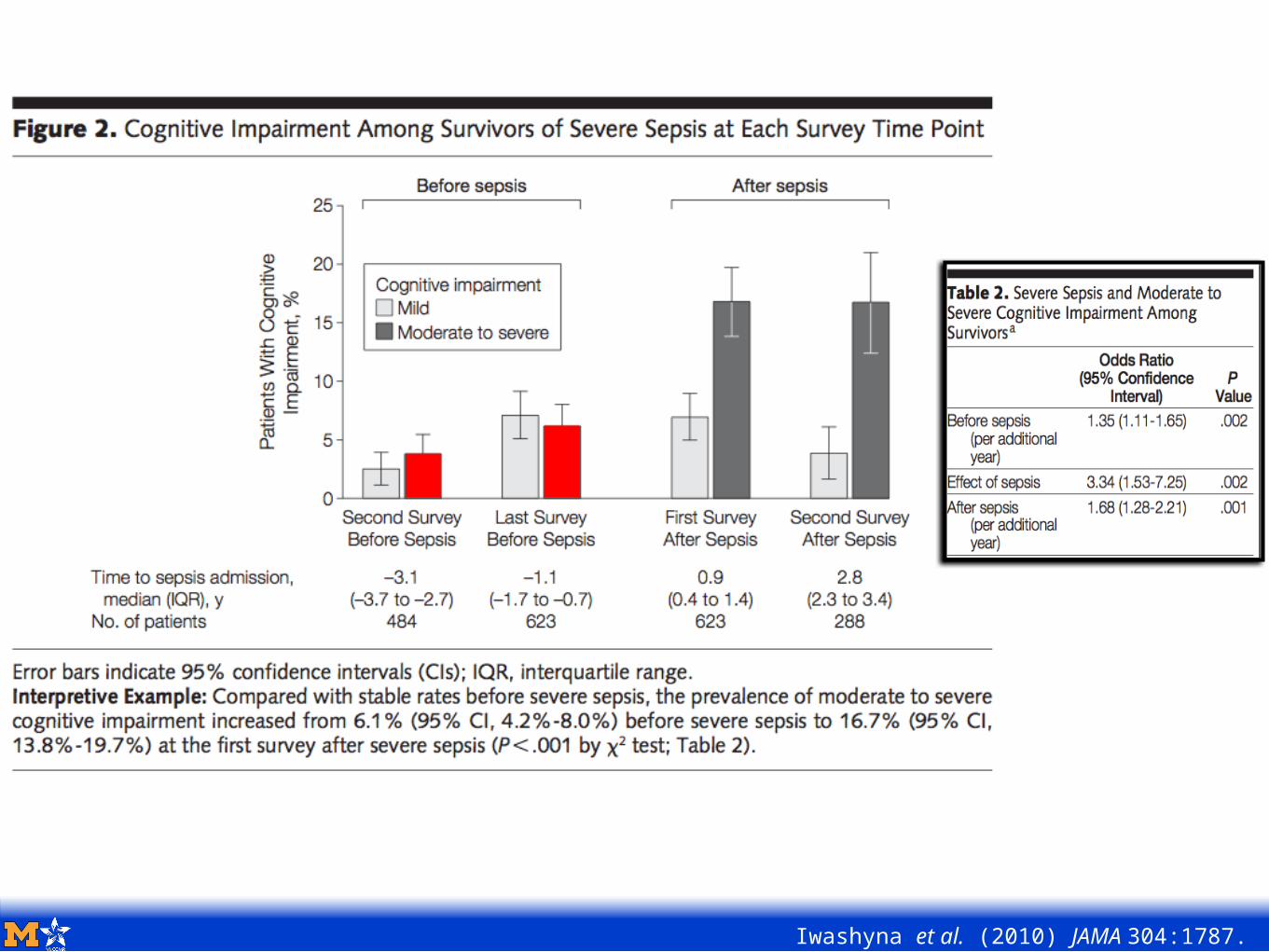
Iwashyna et al. (2010) JAMA 304:1787.
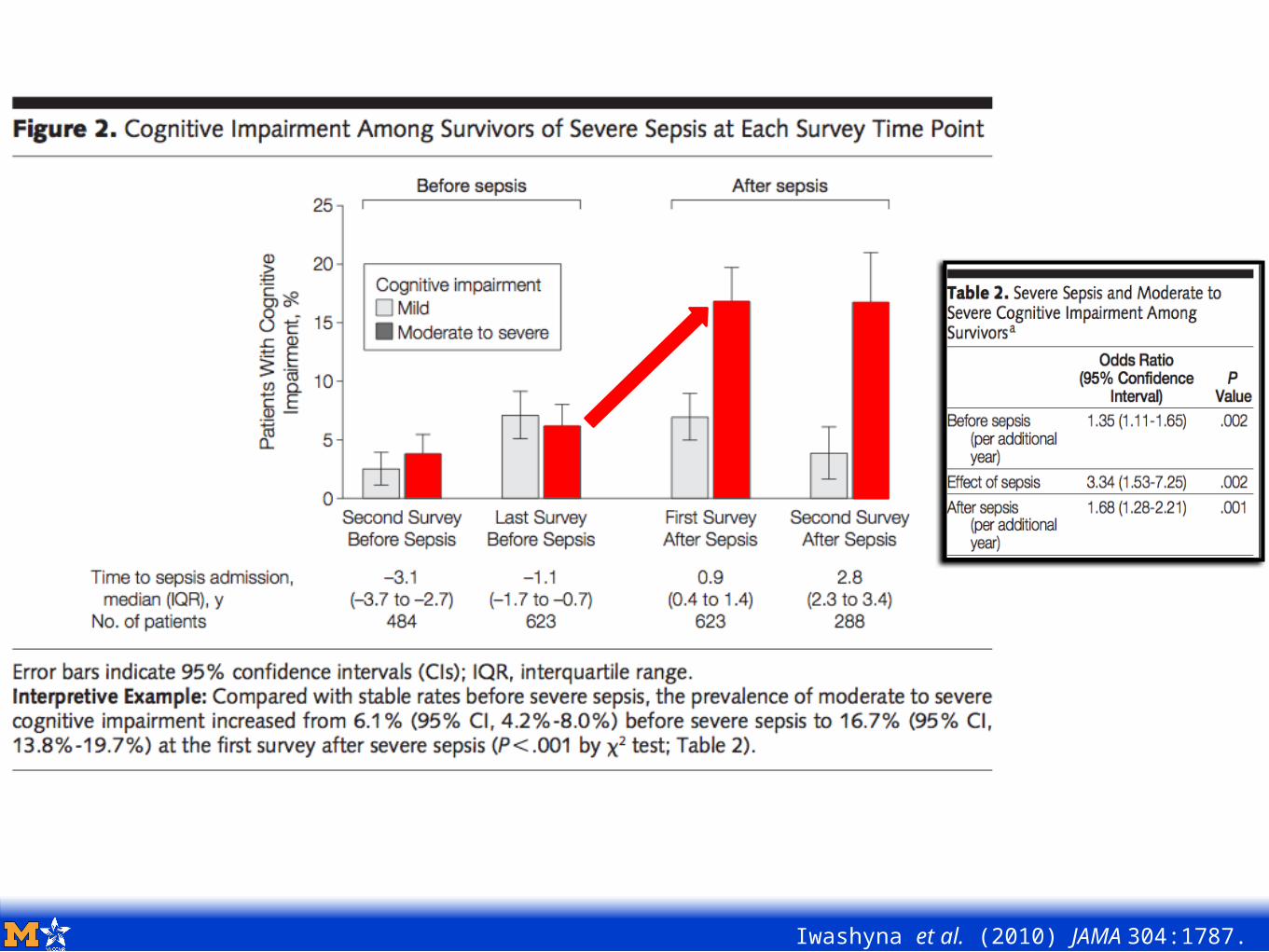
Iwashyna et al. (2010) JAMA 304:1787.
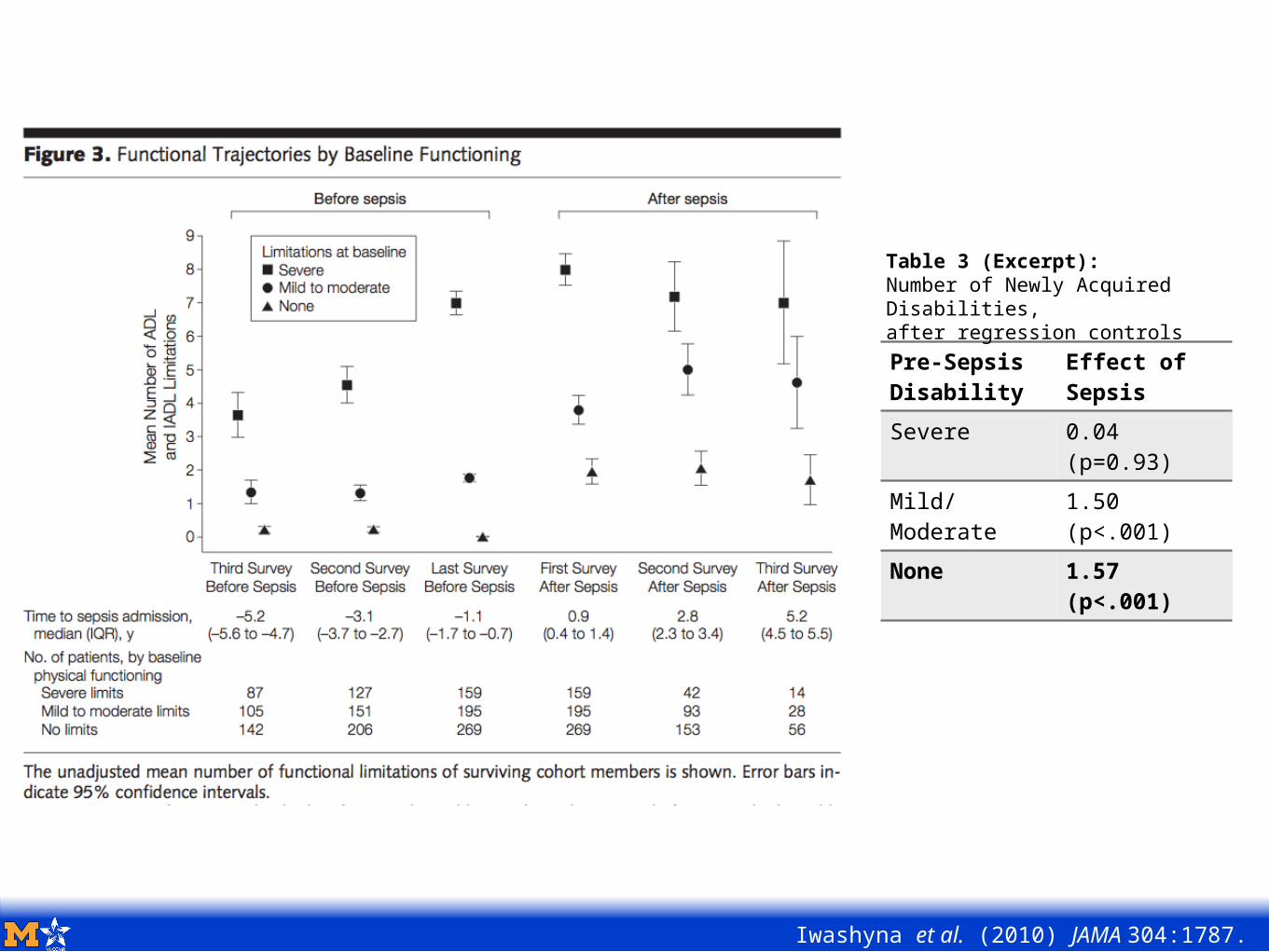
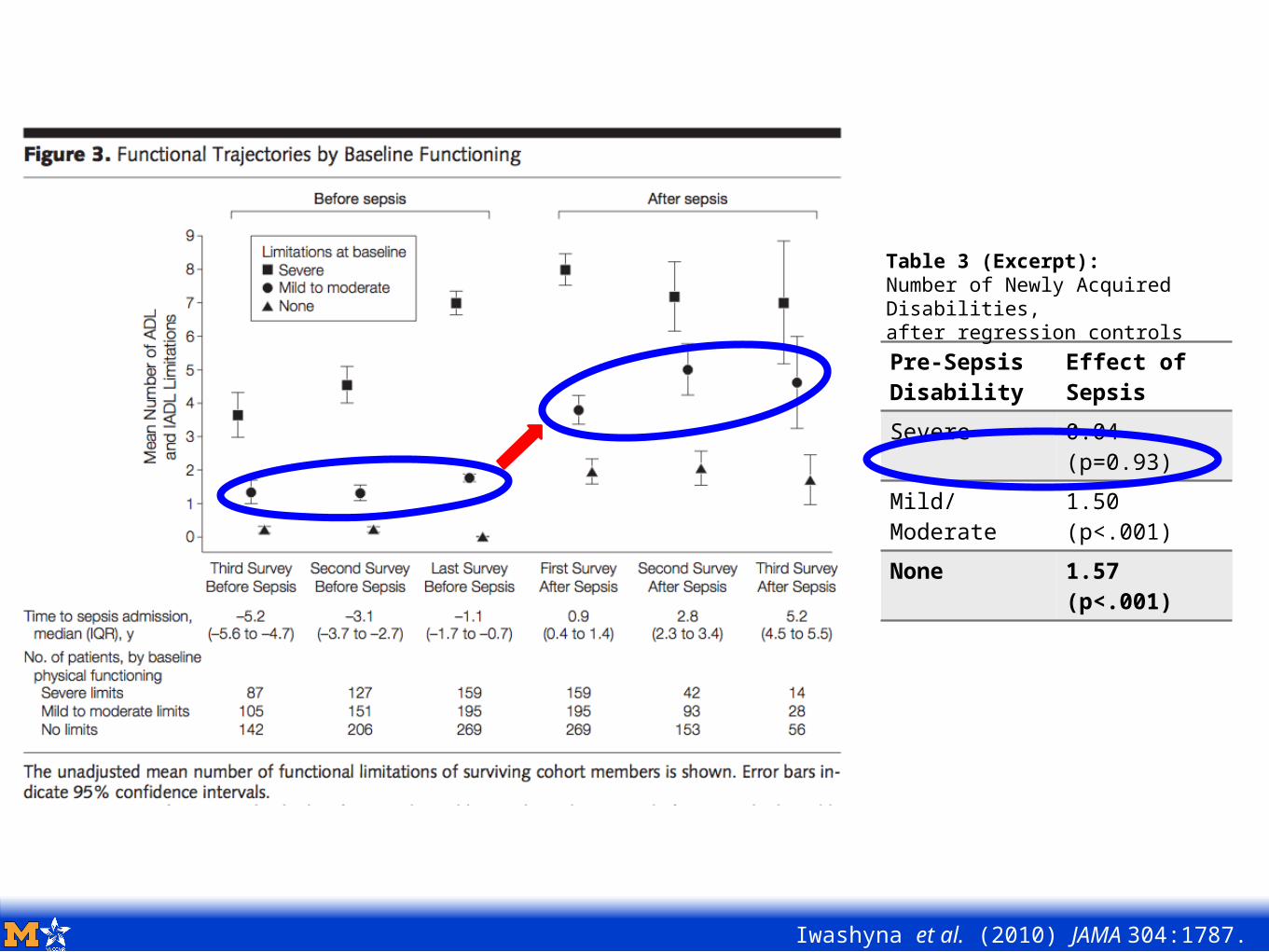
Enduring Long-Term Morbidity
Iwashyna et al. (2010) JAMA 304:1787.
Pre-SepsisDisability
Effect of Sepsis
Severe 0.04 (p=0.93)
Mild/Moderate
1.50 (p<.001)
None 1.57 (p<.001)
Table 3 (Excerpt):Number of Newly Acquired Disabilities,after regression controls
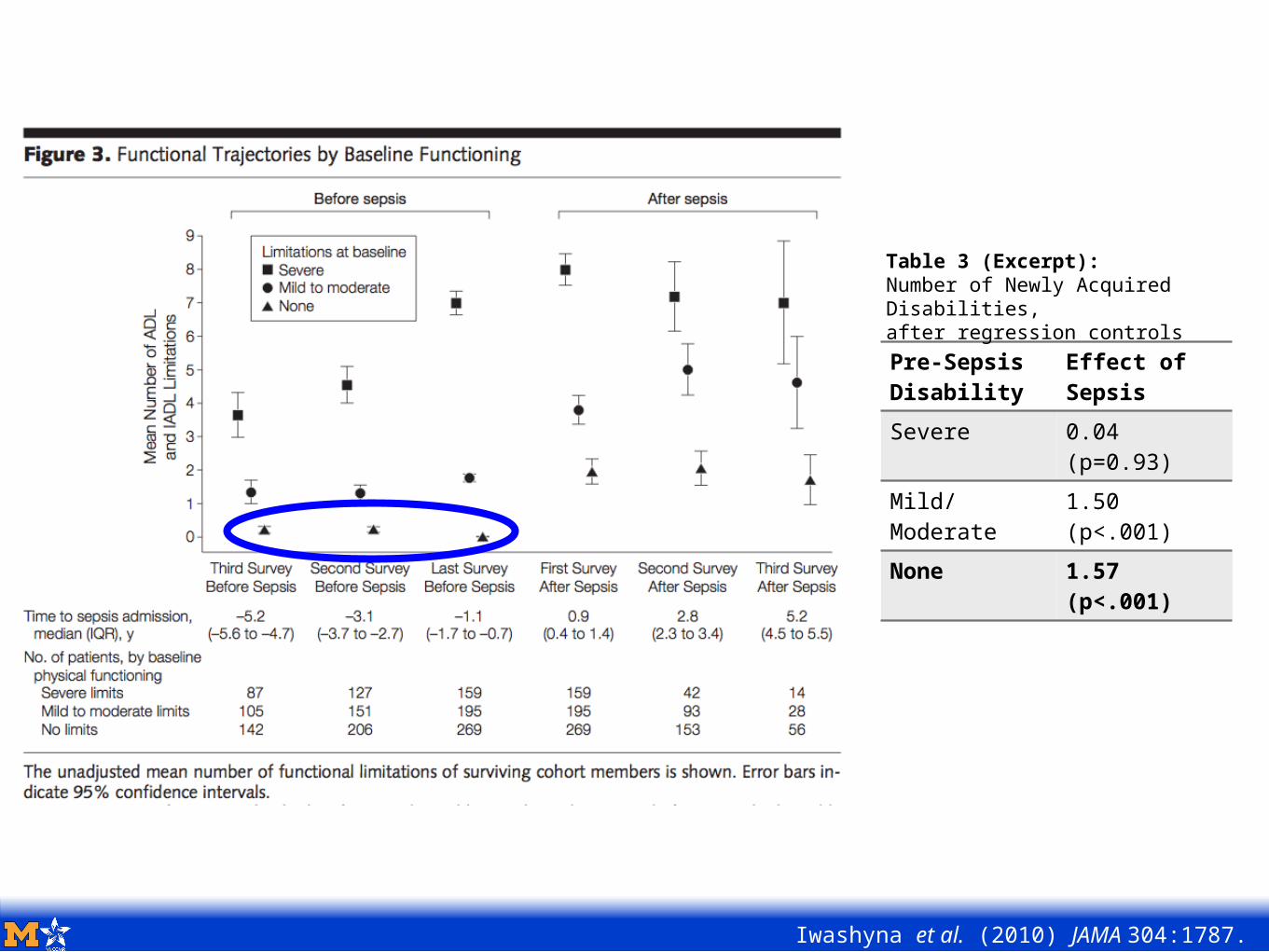
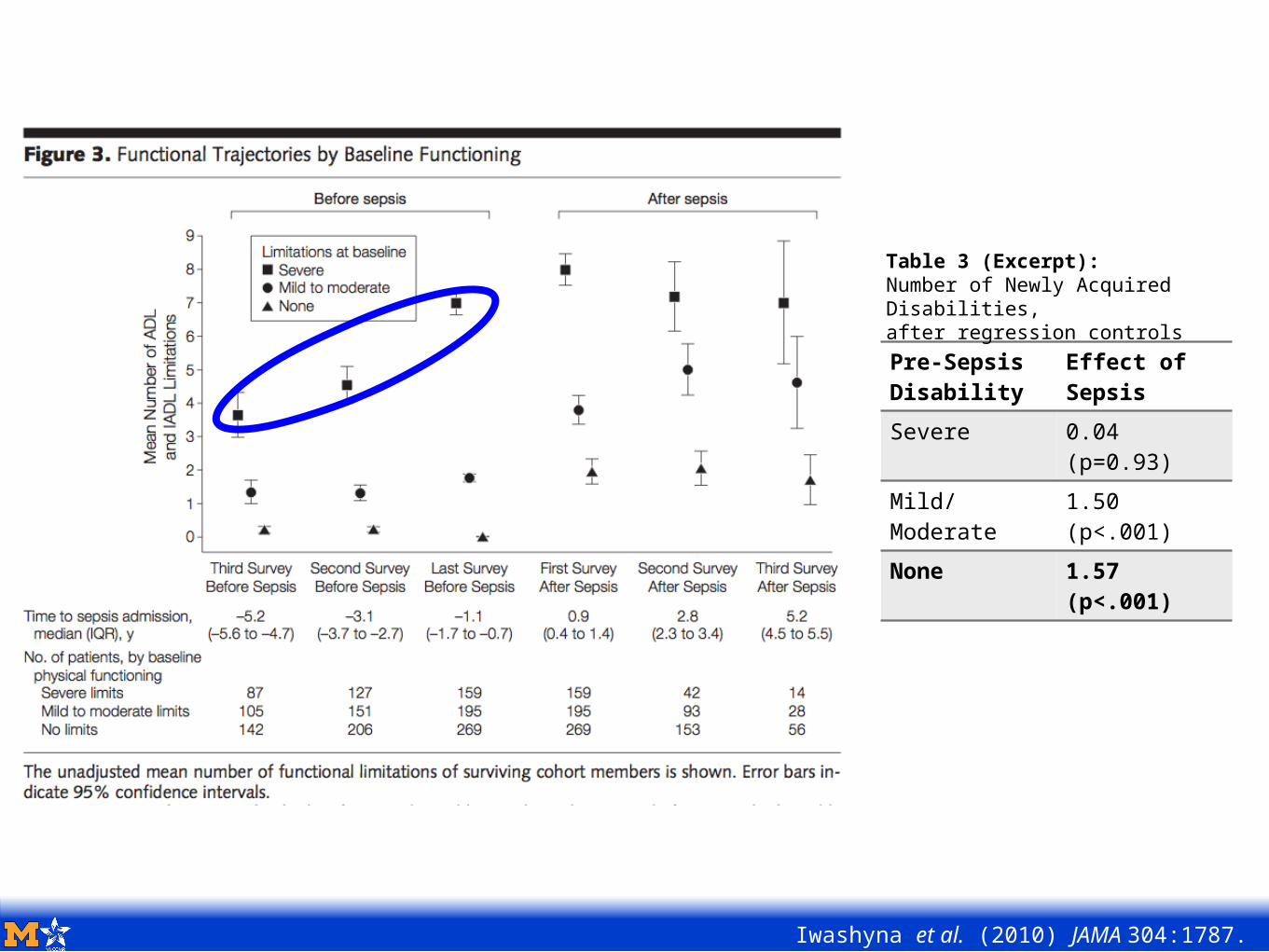
Enduring Long-Term Morbidity
Iwashyna et al. (2010) JAMA 304:1787.
Pre-SepsisDisability
Effect of Sepsis
Severe 0.04 (p=0.93)
Mild/Moderate
1.50 (p<.001)
None 1.57 (p<.001)
Table 3 (Excerpt):Number of Newly Acquired Disabilities,after regression controls
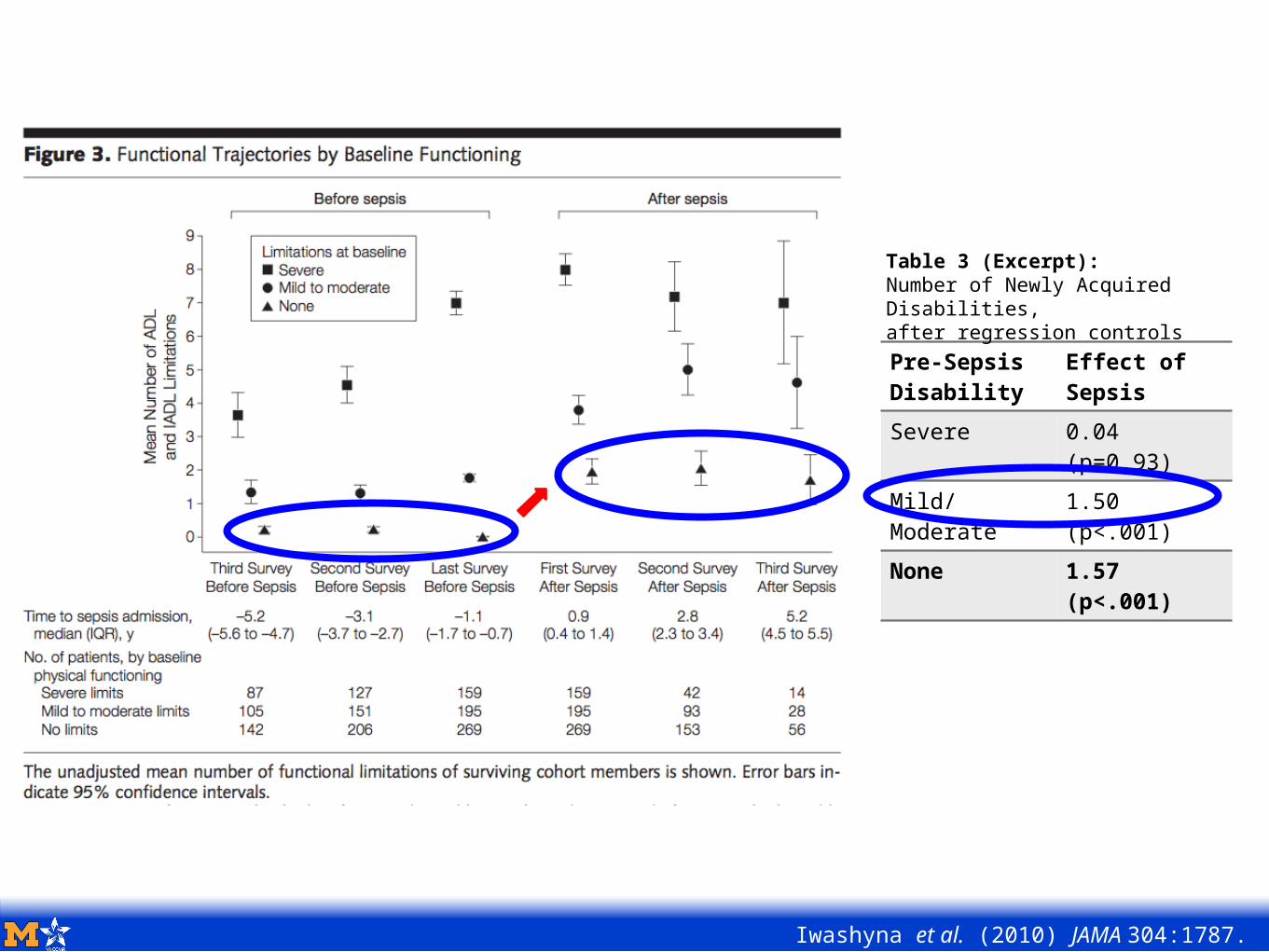
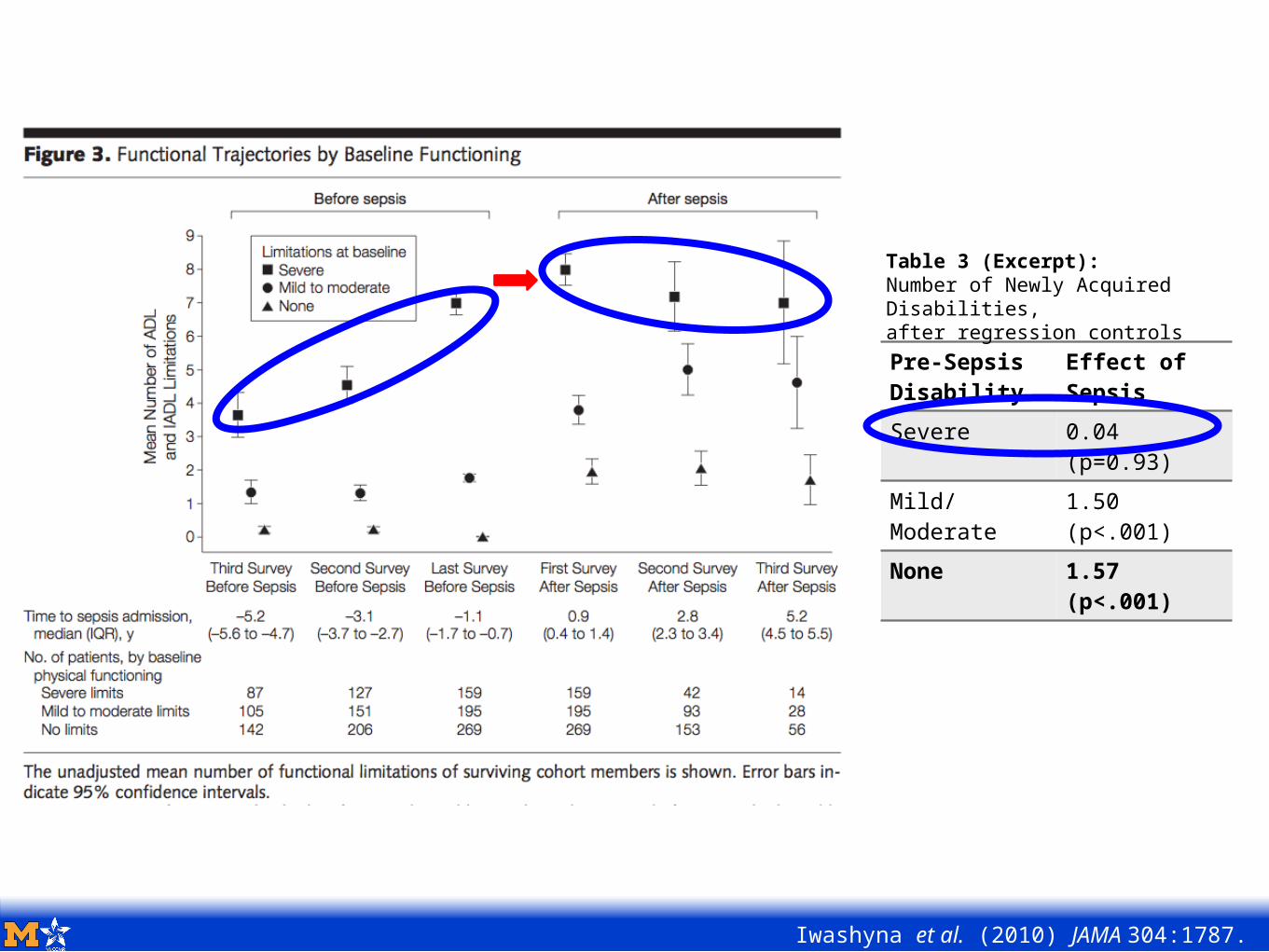
Enduring Long-Term Morbidity
Iwashyna et al. (2010) JAMA 304:1787.
Pre-SepsisDisability
Effect of Sepsis
Severe 0.04 (p=0.93)
Mild/Moderate
1.50 (p<.001)
None 1.57 (p<.001)
Table 3 (Excerpt):Number of Newly Acquired Disabilities,after regression controls
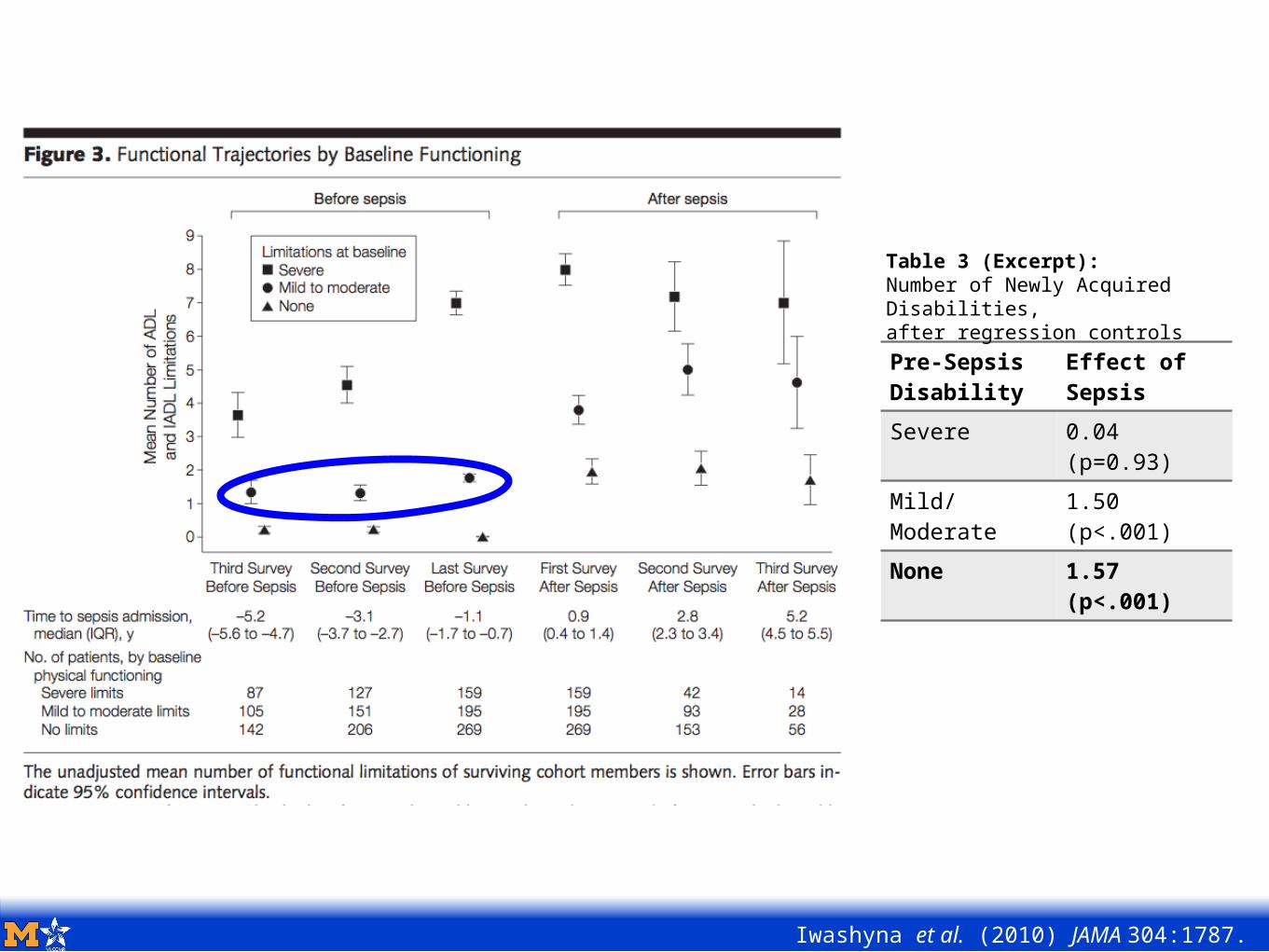
Enduring Long-Term Morbidity
Iwashyna et al. (2010) JAMA 304:1787.
Pre-SepsisDisability
Effect of Sepsis
Severe 0.04 (p=0.93)
Mild/Moderate
1.50 (p<.001)
None 1.57 (p<.001)
Table 3 (Excerpt):Number of Newly Acquired Disabilities,after regression controls
Enduring Long-Term Morbidity
Iwashyna et al. (2010) JAMA 304:1787.
Pre-SepsisDisability
Effect of Sepsis
Severe 0.04 (p=0.93)
Mild/Moderate
1.50 (p<.001)
None 1.57 (p<.001)
Table 3 (Excerpt):Number of Newly Acquired Disabilities,after regression controls
Enduring Long-Term Morbidity
Iwashyna et al. (2010) JAMA 304:1787.
Pre-SepsisDisability
Effect of Sepsis
Severe 0.04 (p=0.93)
Mild/Moderate
1.50 (p<.001)
None 1.57 (p<.001)
Table 3 (Excerpt):Number of Newly Acquired Disabilities,after regression controls
Enduring Long-Term Morbidity
Iwashyna et al. (2010) JAMA 304:1787.
Pre-SepsisDisability
Effect of Sepsis
Severe 0.04 (p=0.93)
Mild/Moderate
1.50 (p<.001)
None 1.57 (p<.001)
Table 3 (Excerpt):Number of Newly Acquired Disabilities,after regression controls
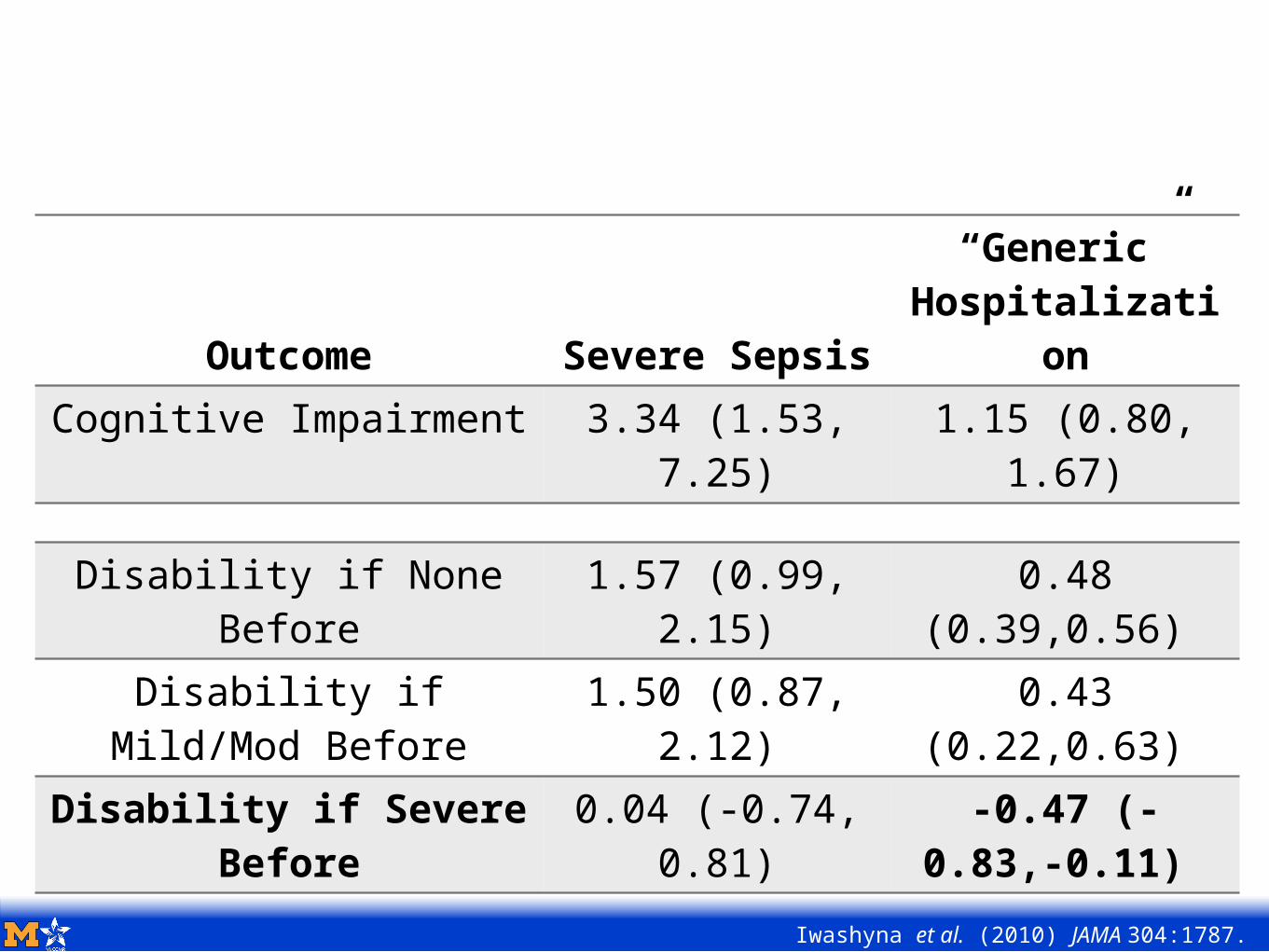
Enduring Long-Term Morbidity
Iwashyna et al. (2010) JAMA 304:1787.
Outcome Severe Sepsis
“Generic” Hospitalizati
onCognitive Impairment 3.34 (1.53,
7.25)1.15 (0.80,
1.67)
Disability if None Before
1.57 (0.99, 2.15)
0.48 (0.39,0.56)
Disability if Mild/Mod Before
1.50 (0.87, 2.12)
0.43 (0.22,0.63)
Disability if Severe Before
0.04 (-0.74, 0.81)
-0.47 (-0.83,-0.11)
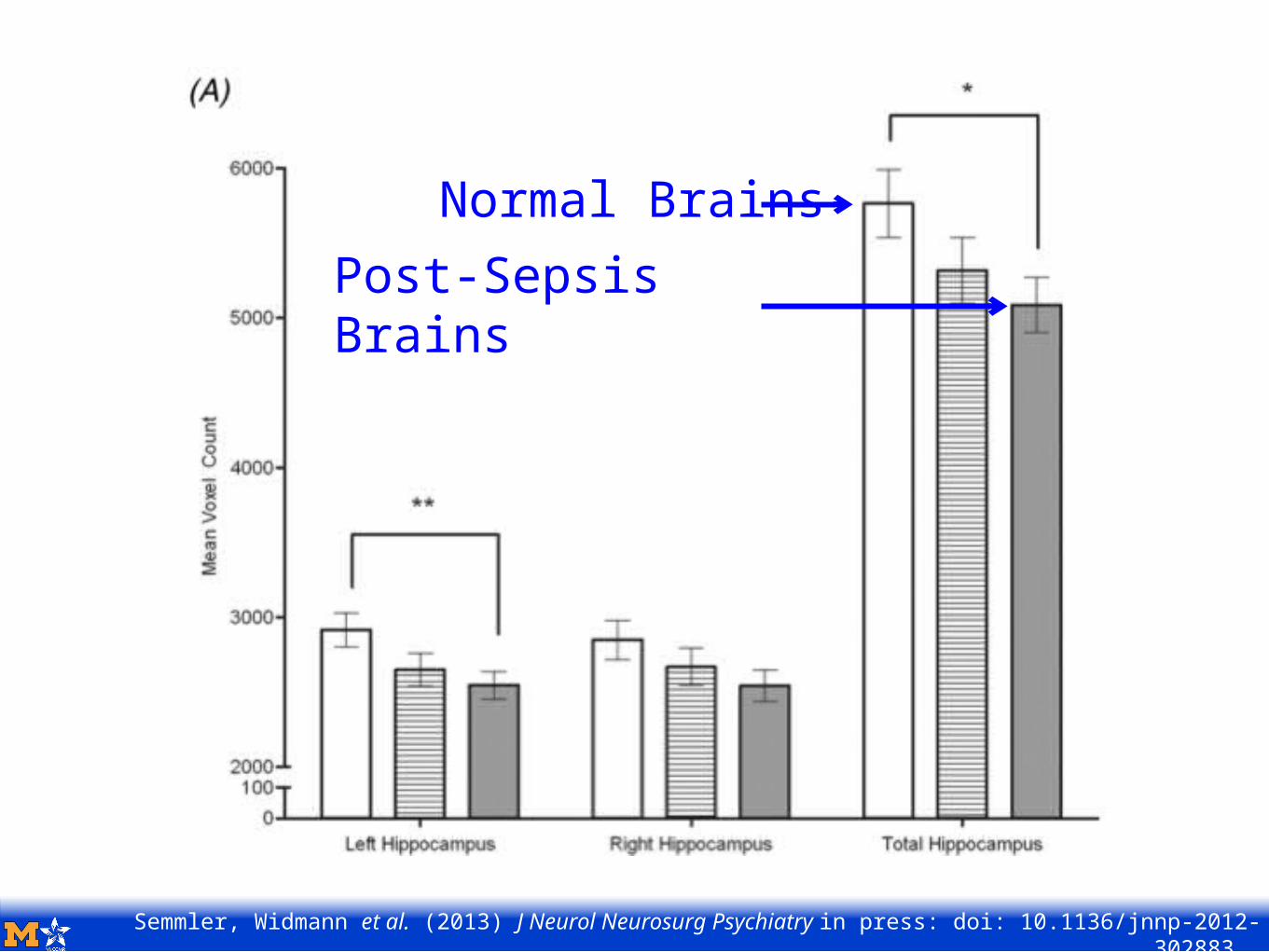
Semmler, Widmann et al. (2013) J Neurol Neurosurg Psychiatry in press: doi: 10.1136/jnnp-2012-302883.
Normal BrainsPost-Sepsis Brains
Disclosures
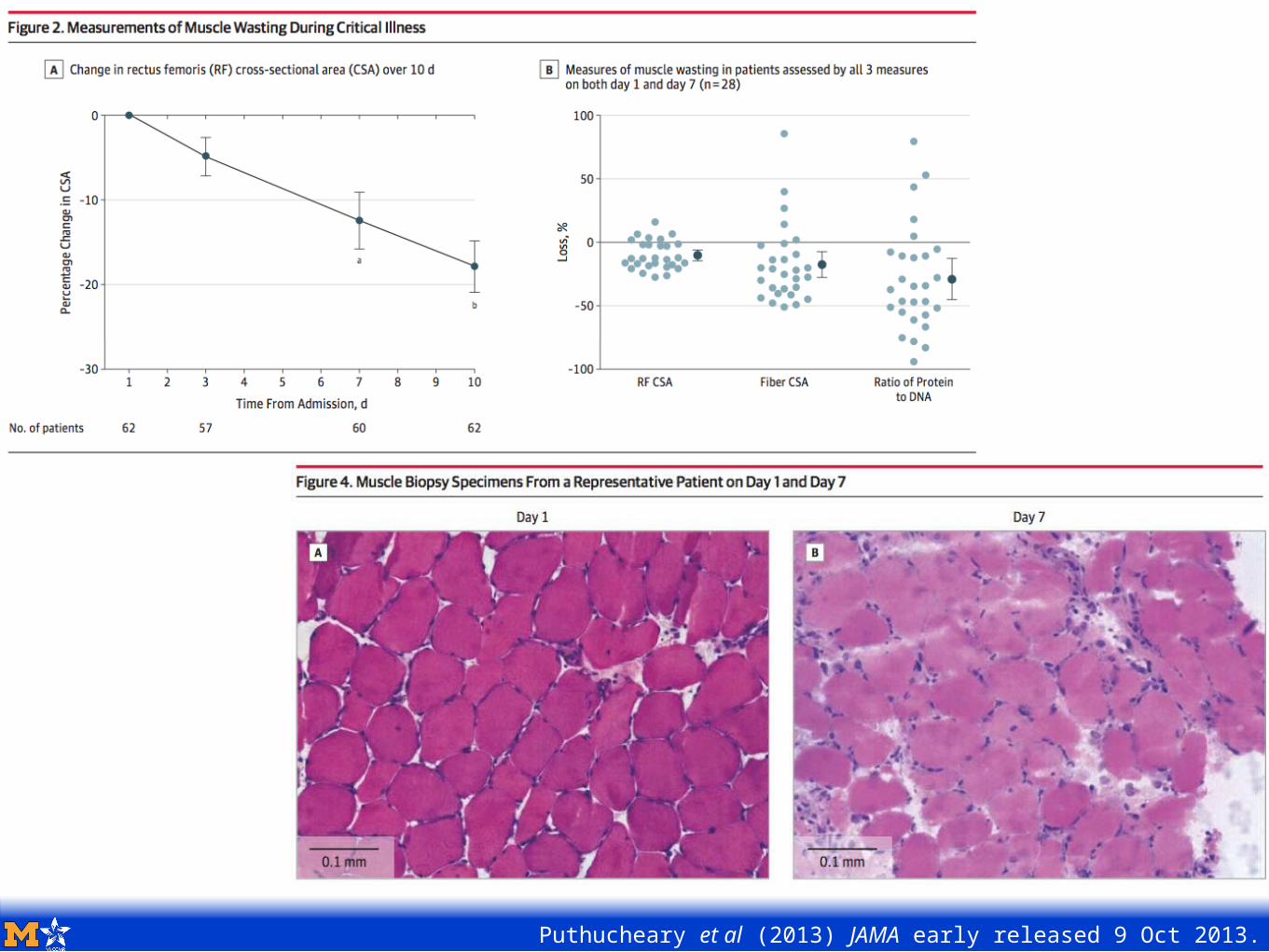
Puthucheary et al (2013) JAMA early released 9 Oct 2013.
Today’s Agenda:
Prologue: When you die with heart disease, what do you die from?
Chapter 1: Sepsis Biology & Epidemiology 101
Chapter 2: Disability & Cognitive Dysfunction
Chapter 3: Life Course Matters
Chapter 4: Population Impact
Epilogue: Summary & What’s Next
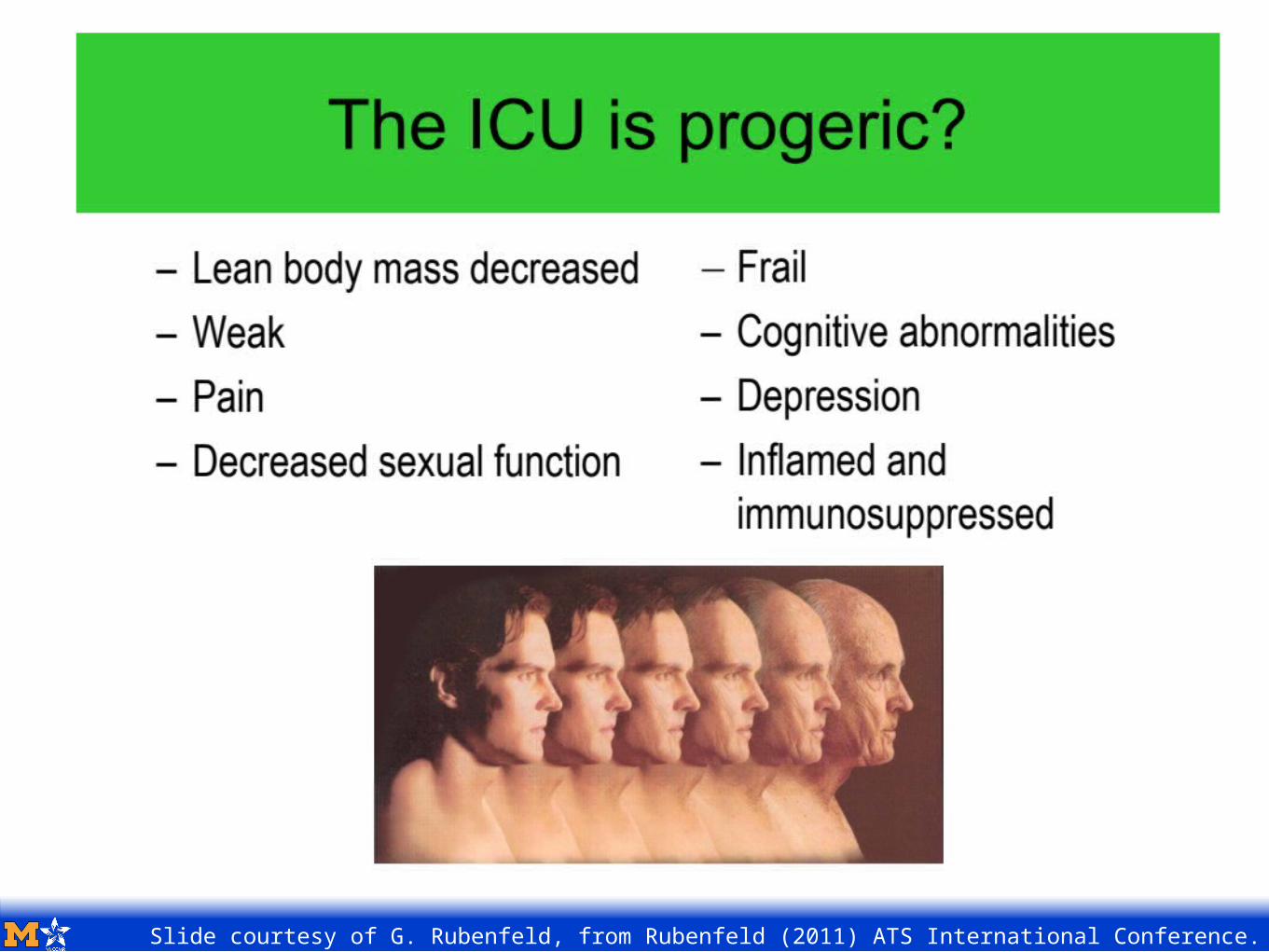
Slide courtesy of G. Rubenfeld, from Rubenfeld (2011) ATS International Conference.
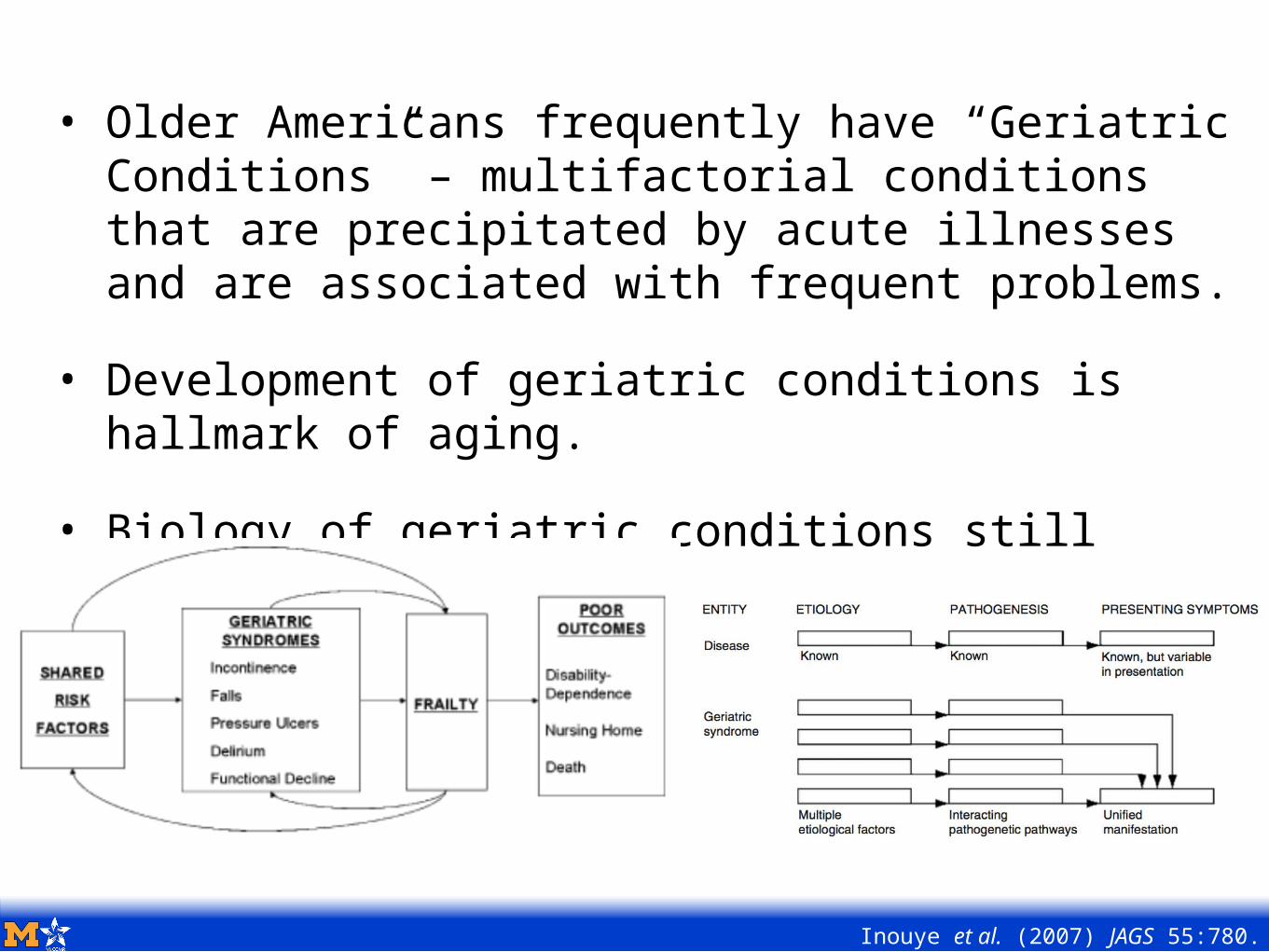
• Older Americans frequently have “Geriatric Conditions” – multifactorial conditions that are precipitated by acute illnesses and are associated with frequent problems.
• Development of geriatric conditions is hallmark of aging.
• Biology of geriatric conditions still actively researched.
Inouye et al. (2007) JAGS 55:780.
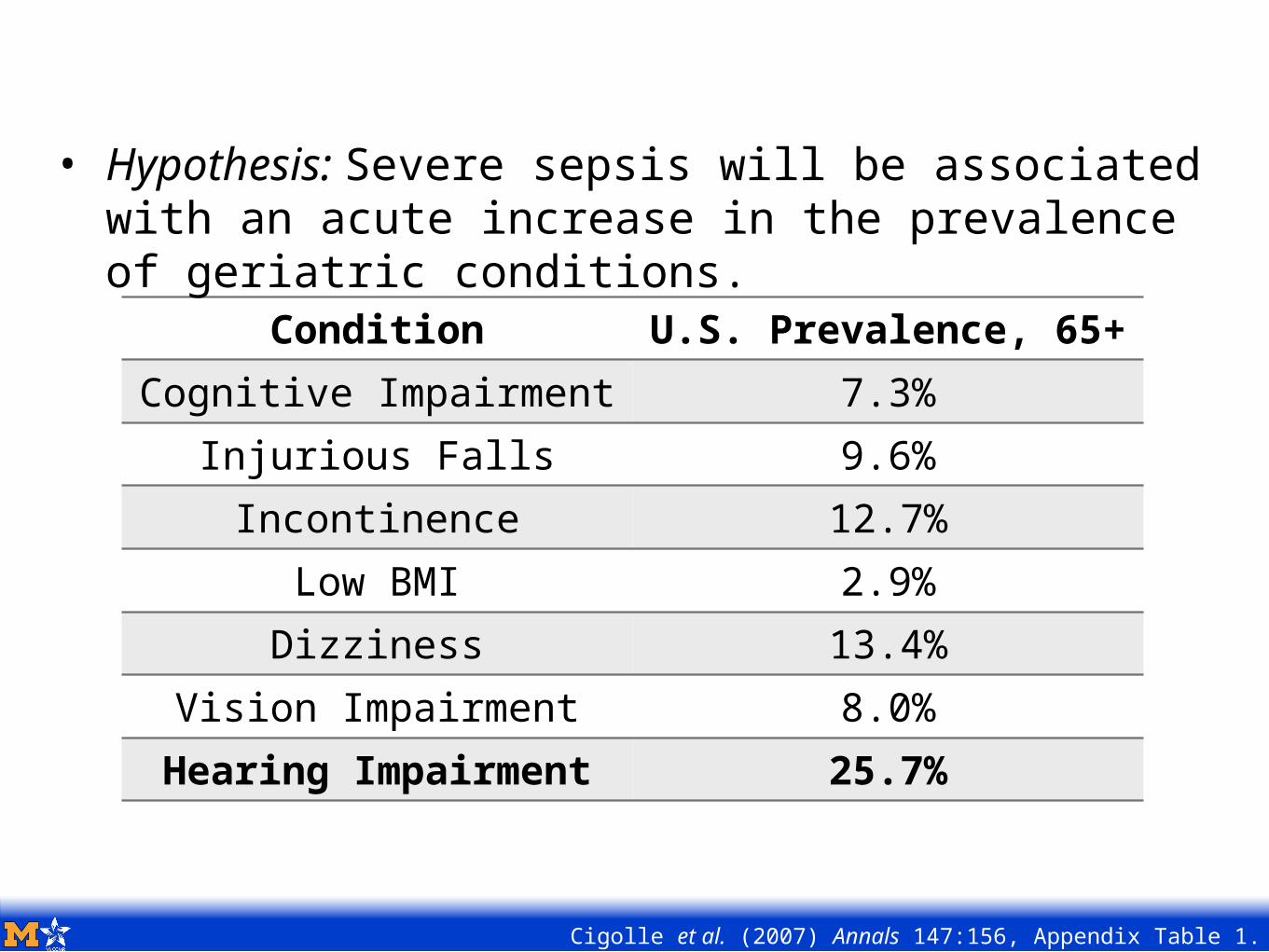
Condition U.S. Prevalence, 65+Cognitive Impairment 7.3%
Injurious Falls 9.6%Incontinence 12.7%
Low BMI 2.9%Dizziness 13.4%
Vision Impairment 8.0%Hearing Impairment 25.7%
Cigolle et al. (2007) Annals 147:156, Appendix Table 1.
• Hypothesis: Severe sepsis will be associated with an acute increase in the prevalence of geriatric conditions.
Outcomes were self-report using standard language across multiple survey waves of HRS.• augmented with proxies where necessary
Falls: resulting in injuring
Incontinence: requiring pads or diapers
Vision Impairment: despite corrective lenses
Hearing Impairment: despite use of hearing aids
Research Questions (II)Hypothesis: Severe sepsis will be associated with an acute increase in the prevalence of geriatric conditions.
Will the apparent association be similar across 3 alternative study designs?• Prospective cohort vs. age-matched population controls
• Prospective cohort vs. own pre-sepsis baseline
• Prospective longitudinal cohort with extensive pre-sepsis prospective data
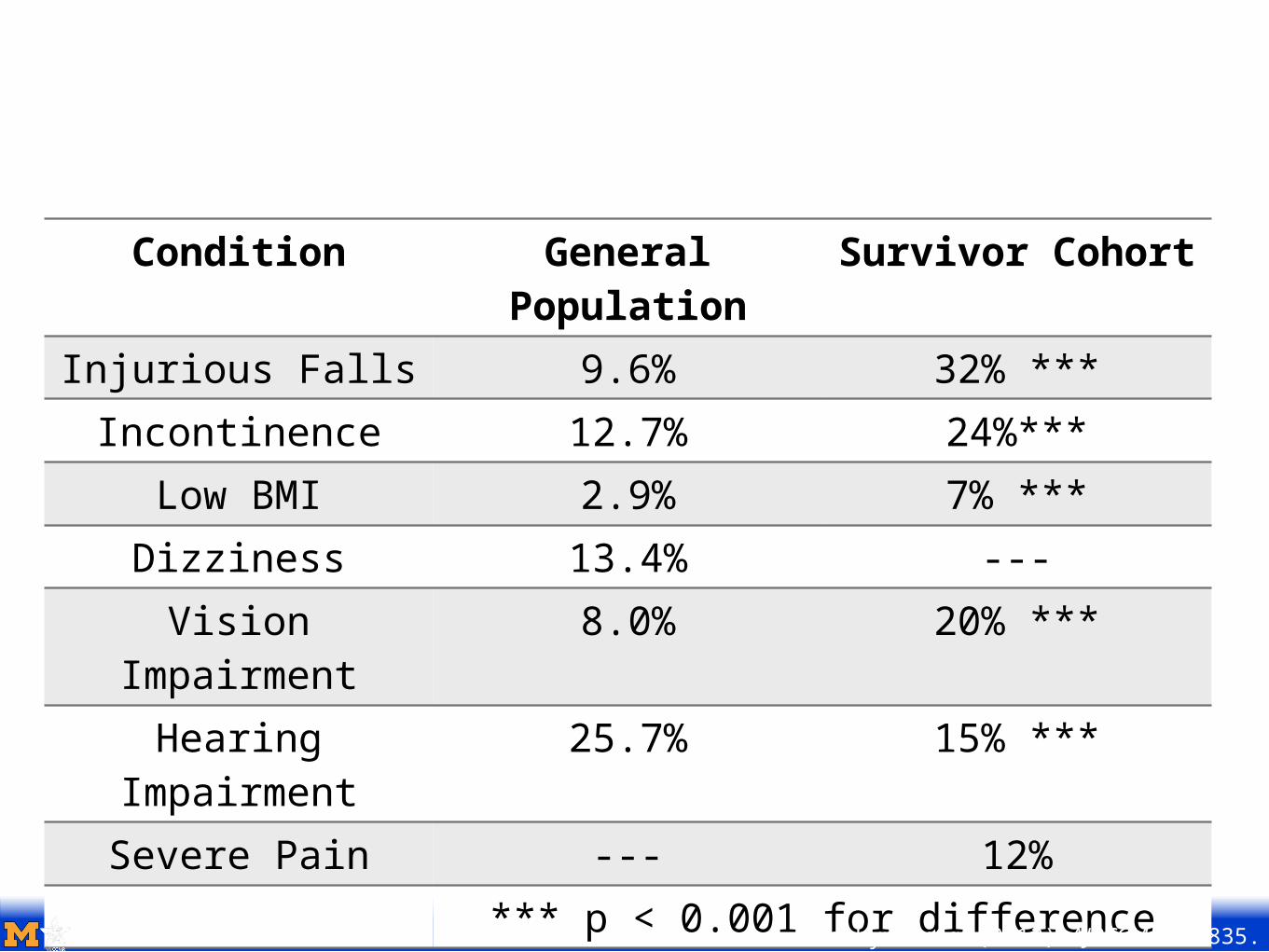
Condition General Population
Survivor Cohort
Injurious Falls 9.6% 32% ***Incontinence 12.7% 24%***
Low BMI 2.9% 7% ***Dizziness 13.4% ---Vision
Impairment8.0% 20% ***
Hearing Impairment
25.7% 15% ***
Severe Pain --- 12%*** p < 0.001 for differenceIwashyna et al. (2012) AJRCCM 185:835.
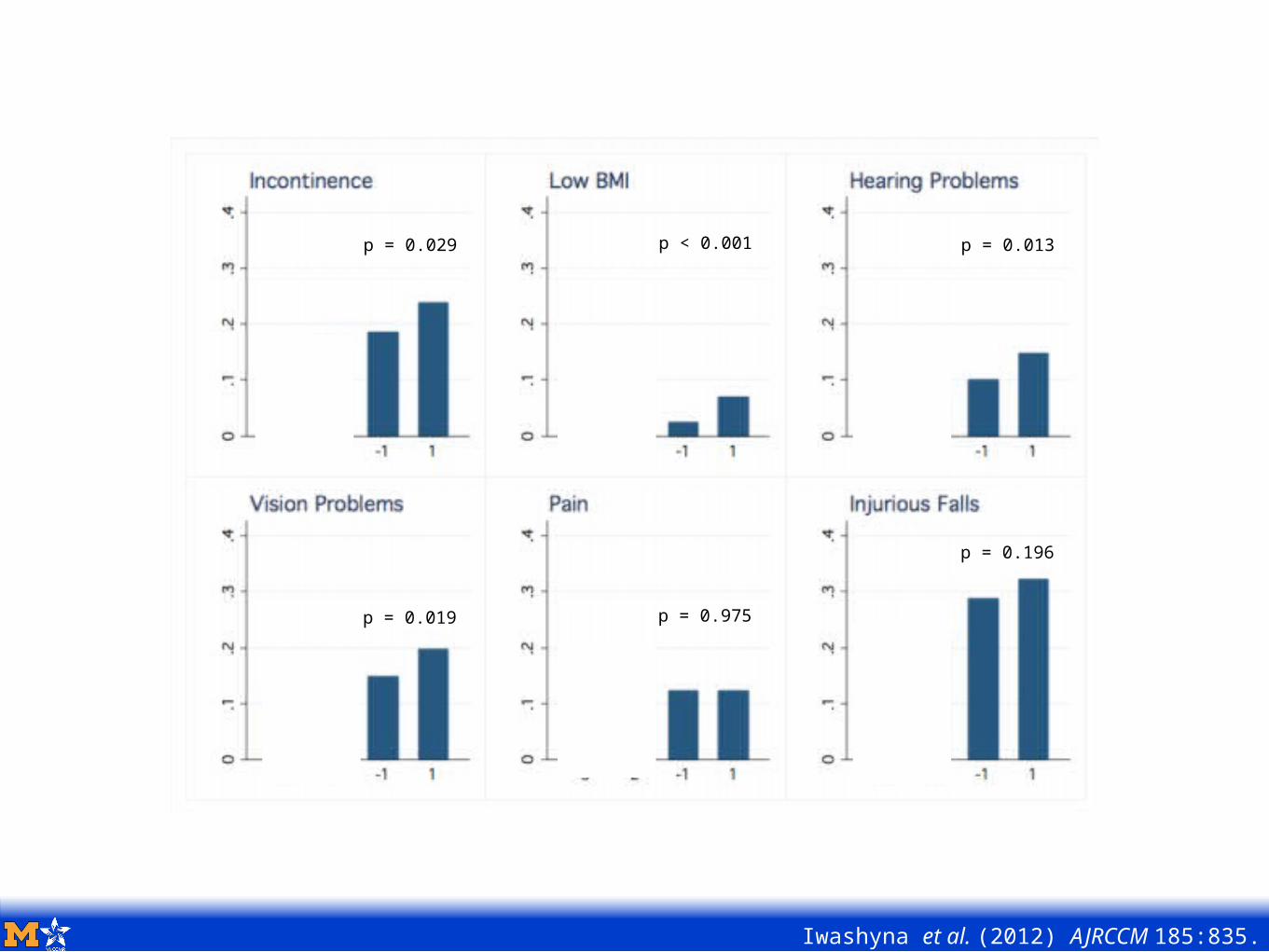
p = 0.029
p = 0.019
p < 0.001
p = 0.975
p = 0.013
p = 0.196
Iwashyna et al. (2012) AJRCCM 185:835.
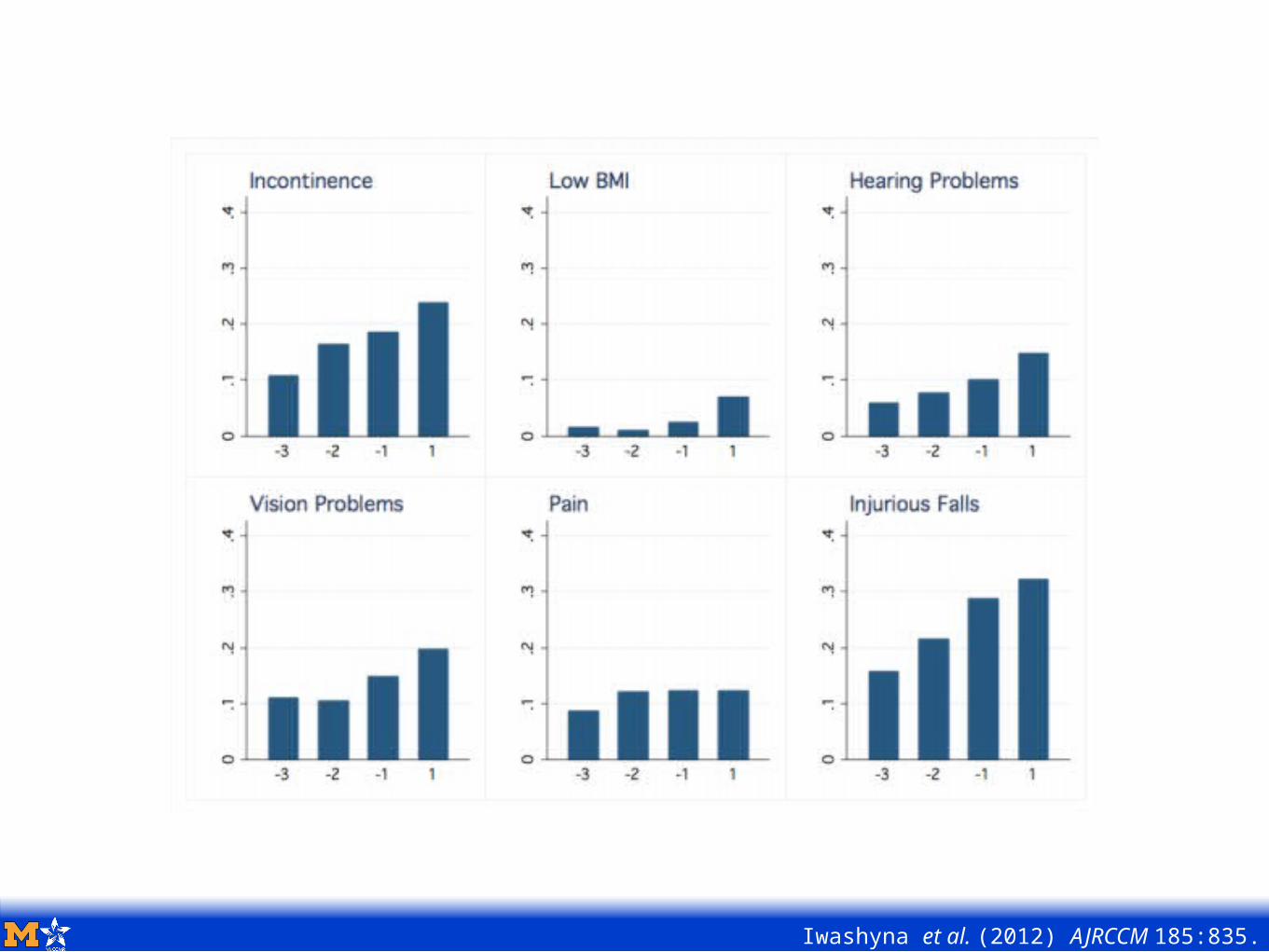
Iwashyna et al. (2012) AJRCCM 185:835.
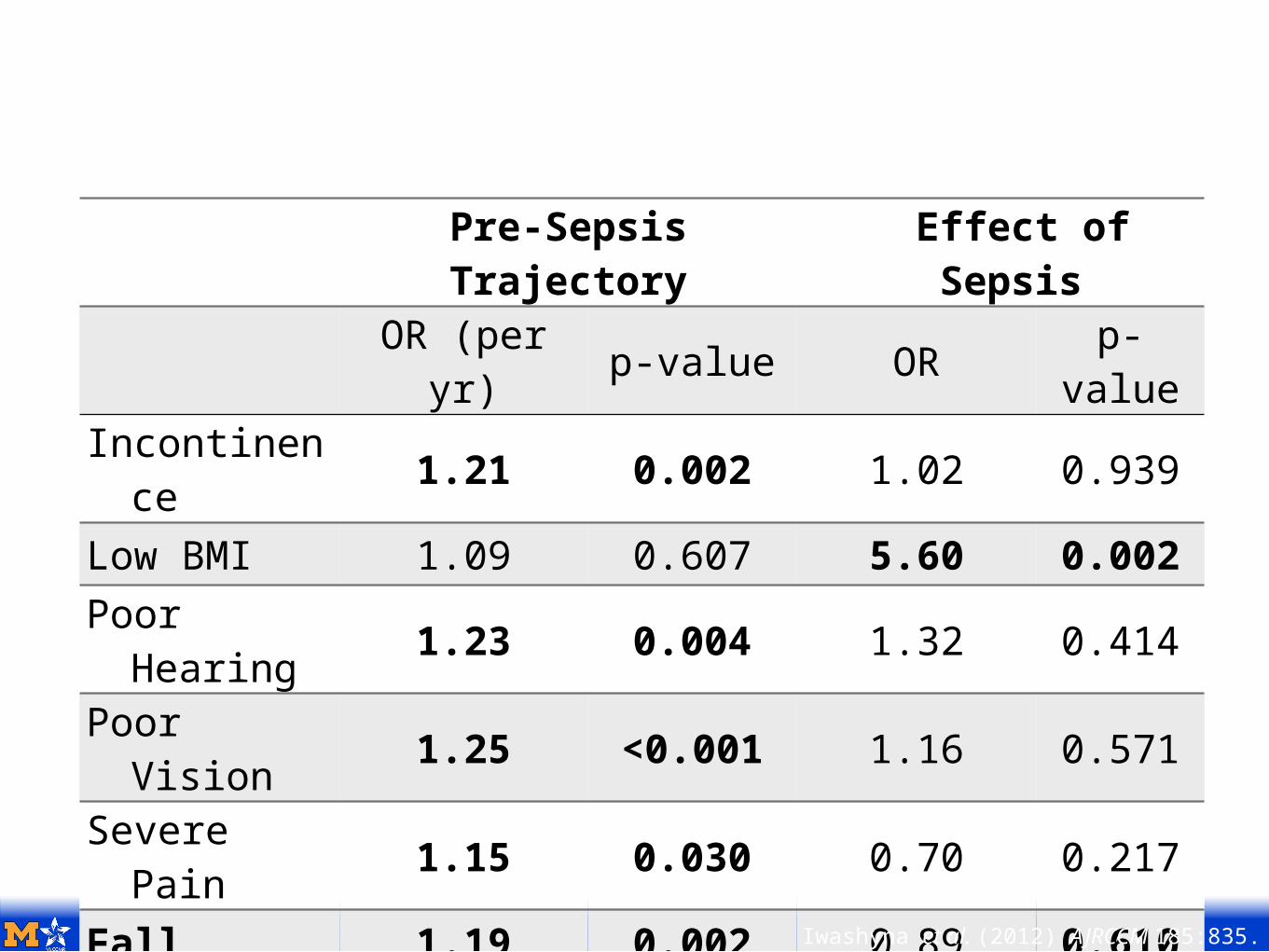
Pre-Sepsis Trajectory
Effect of Sepsis
OR (per yr) p-value OR p-
valueIncontinence 1.21 0.002 1.02 0.939
Low BMI 1.09 0.607 5.60 0.002Poor Hearing 1.23 0.004 1.32 0.414
Poor Vision 1.25 <0.001 1.16 0.571
Severe Pain 1.15 0.030 0.70 0.217
Fall 1.19 0.002 0.89 0.610Iwashyna et al. (2012) AJRCCM 185:835.
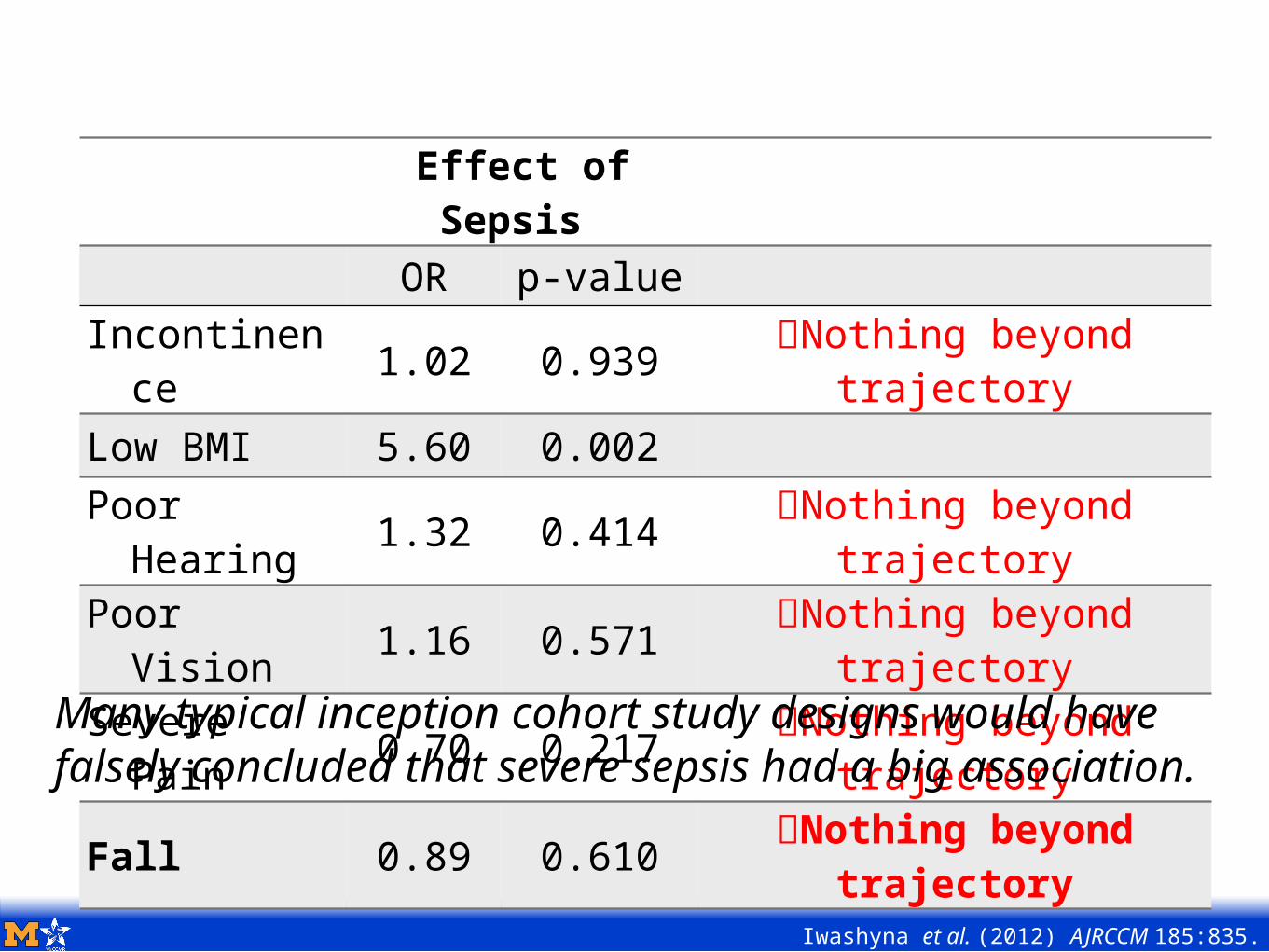
At Risk of Beating A Dead HorseEffect of
Sepsis OR p-value
Incontinence 1.02 0.939 Nothing beyond
trajectoryLow BMI 5.60 0.002Poor Hearing 1.32 0.414 Nothing beyond
trajectoryPoor Vision 1.16 0.571 Nothing beyond
trajectorySevere Pain 0.70 0.217 Nothing beyond
trajectory
Fall 0.89 0.610 Nothing beyond trajectory
Iwashyna et al. (2012) AJRCCM 185:835.
Many typical inception cohort study designs would have falsely concluded that severe sepsis had a big association.
Today’s Agenda:
Prologue: When you die with heart disease, what do you die from?
Chapter 1: Sepsis Biology & Epidemiology 101
Chapter 2: Disability & Cognitive Dysfunction
Chapter 3: Life Course Matters
Chapter 4: Population Impact
Epilogue: Summary & What’s Next
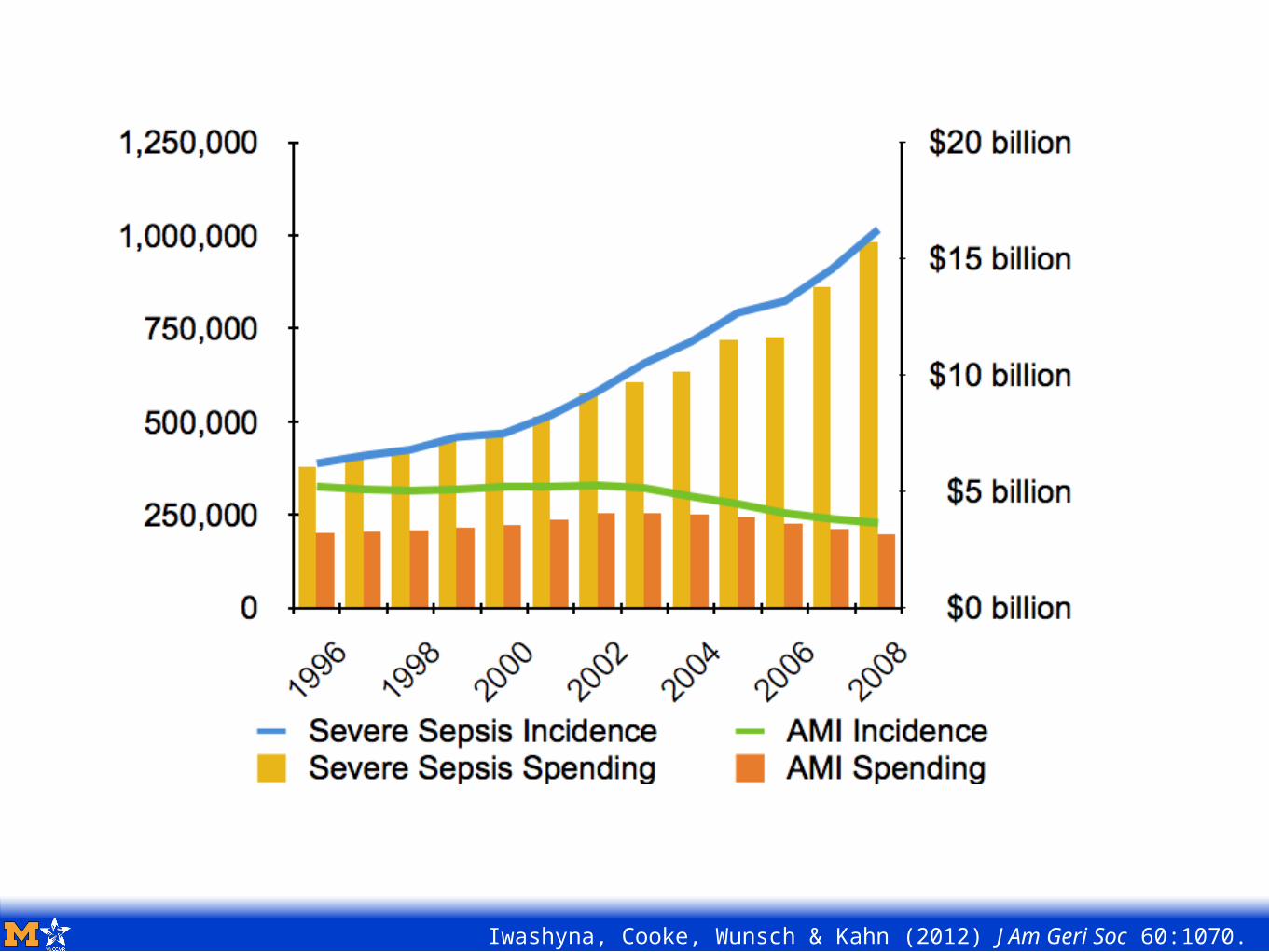
Iwashyna, Cooke, Wunsch & Kahn (2012) J Am Geri Soc 60:1070.
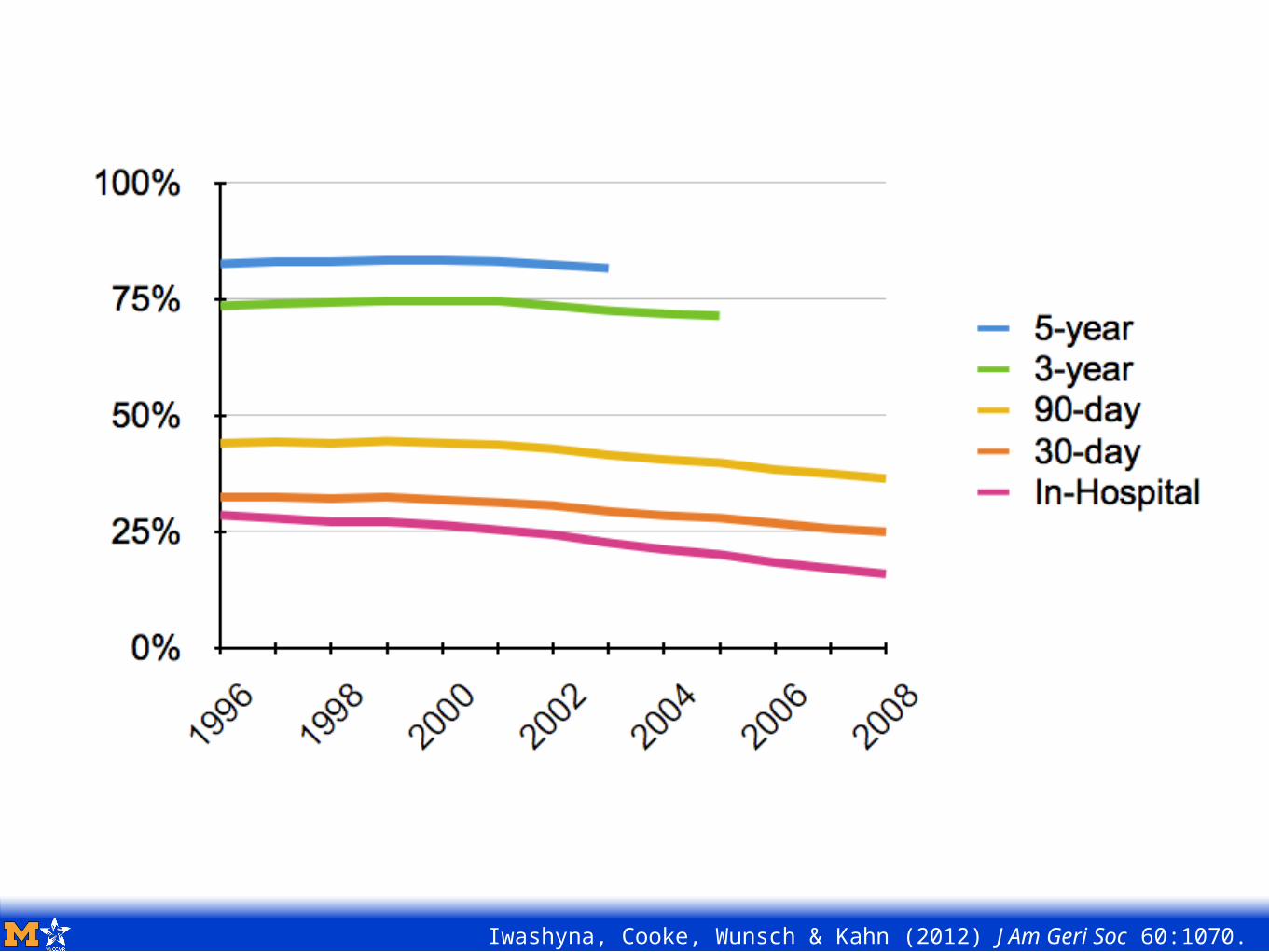
Little Change in Case-Fatality Rate
Iwashyna, Cooke, Wunsch & Kahn (2012) J Am Geri Soc 60:1070.
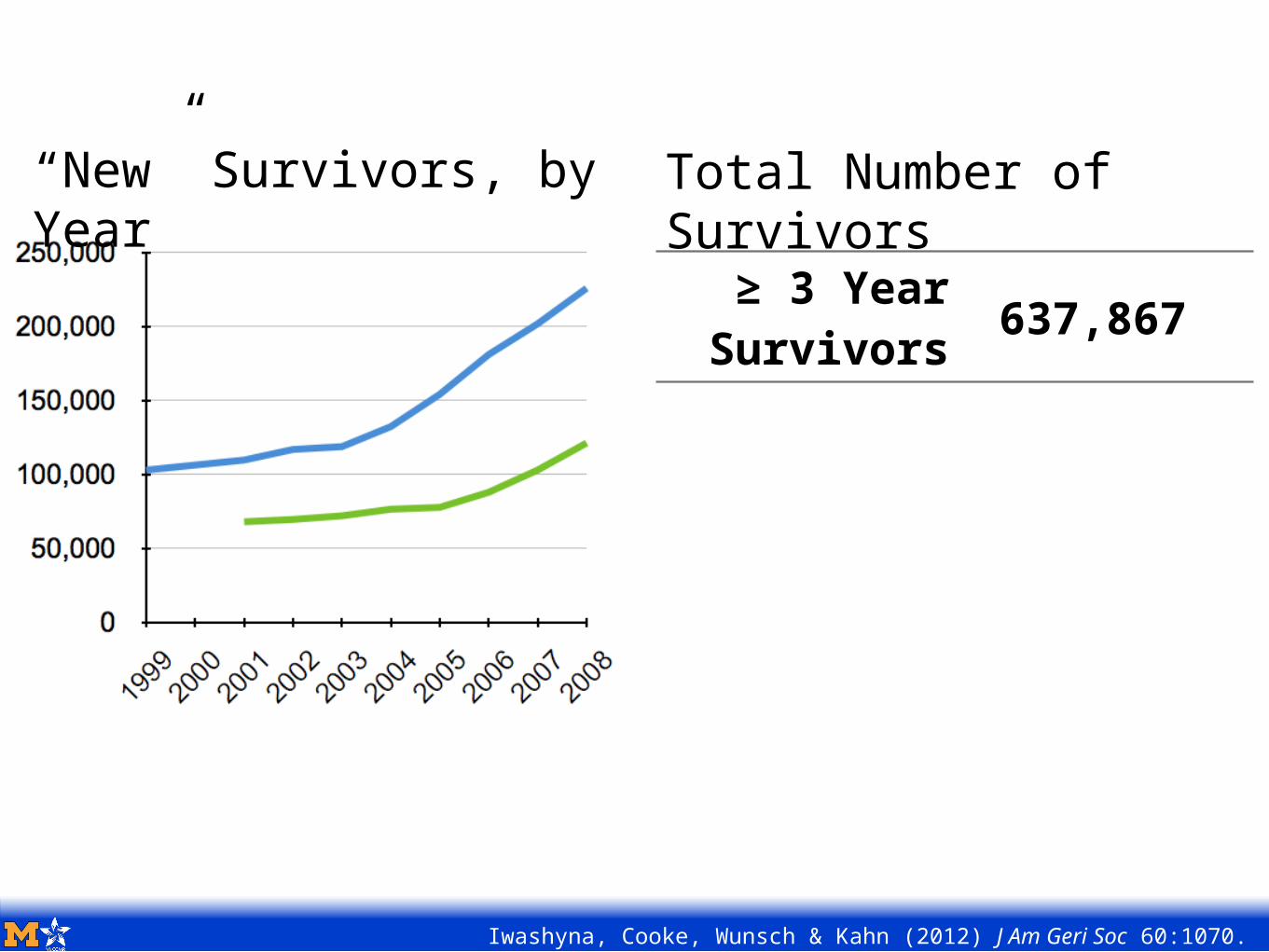
≥ 3 Year Survivors 637,867
Total Number of Survivors
“New” Survivors, by Year
Iwashyna, Cooke, Wunsch & Kahn (2012) J Am Geri Soc 60:1070.
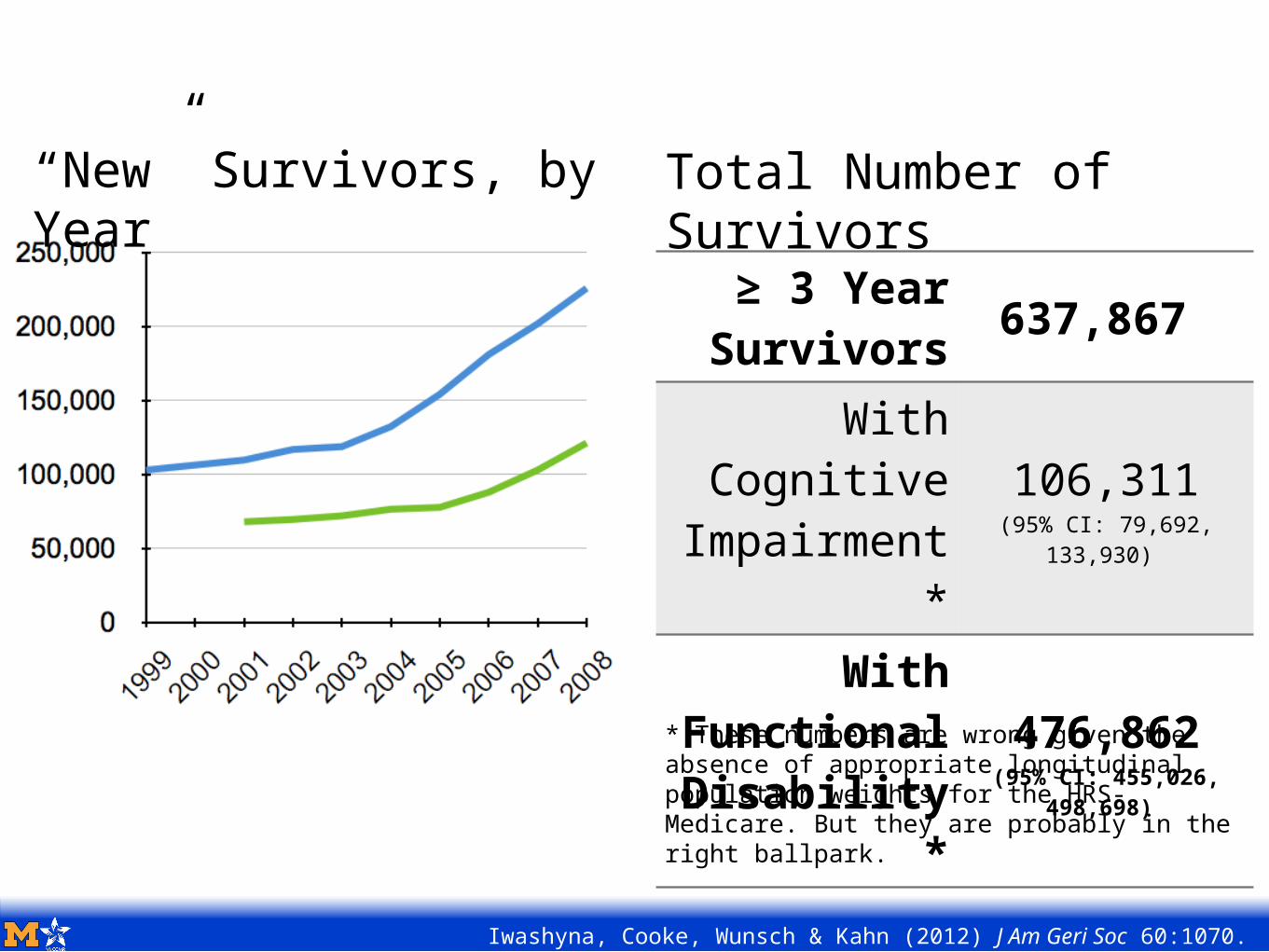
≥ 3 Year Survivors 637,867
With Cognitive Impairment
*
106,311(95% CI: 79,692,
133,930)
With Functional Disability
*
476,862(95% CI: 455,026,
498,698)
Total Number of Survivors
“New” Survivors, by Year
Iwashyna, Cooke, Wunsch & Kahn (2012) J Am Geri Soc 60:1070.
* These numbers are wrong given the absence of appropriate longitudinal population weights for the HRS-Medicare. But they are probably in the right ballpark.
Today’s Agenda:
Prologue: When you die with heart disease, what do you die from?
Chapter 1: Sepsis Biology & Epidemiology 101
Chapter 2: Disability & Cognitive Dysfunction
Chapter 3: Life Course Matters
Chapter 4: Population Impact
Epilogue: Summary & What’s Next
In what sense do acute infections still matter in this era (in the U.S.) of chronic disease of the aged?Acute infections are not just acutely life-threatening, but also often life-altering.
Are they common?Yes, both absolutely and as proximal causes of death across diverse underlying causes of death.
Do they cause lingering consequences?Yes, particularly for brains and muscles.
Should they be incorporated into thinking about population health and disability?Probably. There are a lot of survivors out there.
What drives recovery?• Heterogeneity in trajectories within disease
• Effect modifiers (particularly social, organizational and contextual) and positive deviants
• Heterogeneity across acute illnesses
To what extent are apparently continuous “growth curves” for many aging processes really the results of aggregated discontinuous hits?
How important would blunting these acute hits be for long-term morbidity and mortality?• Less bad sepsis vs. rarer sepsis?
The Old Man’s Friend No More:Disability & Cognitive Decline
After Acute Infection
Theodore J. Iwashyna, MD, PhDtiwashyn @ umich . edu
5 December 2013 – DuPRI Seminar Series
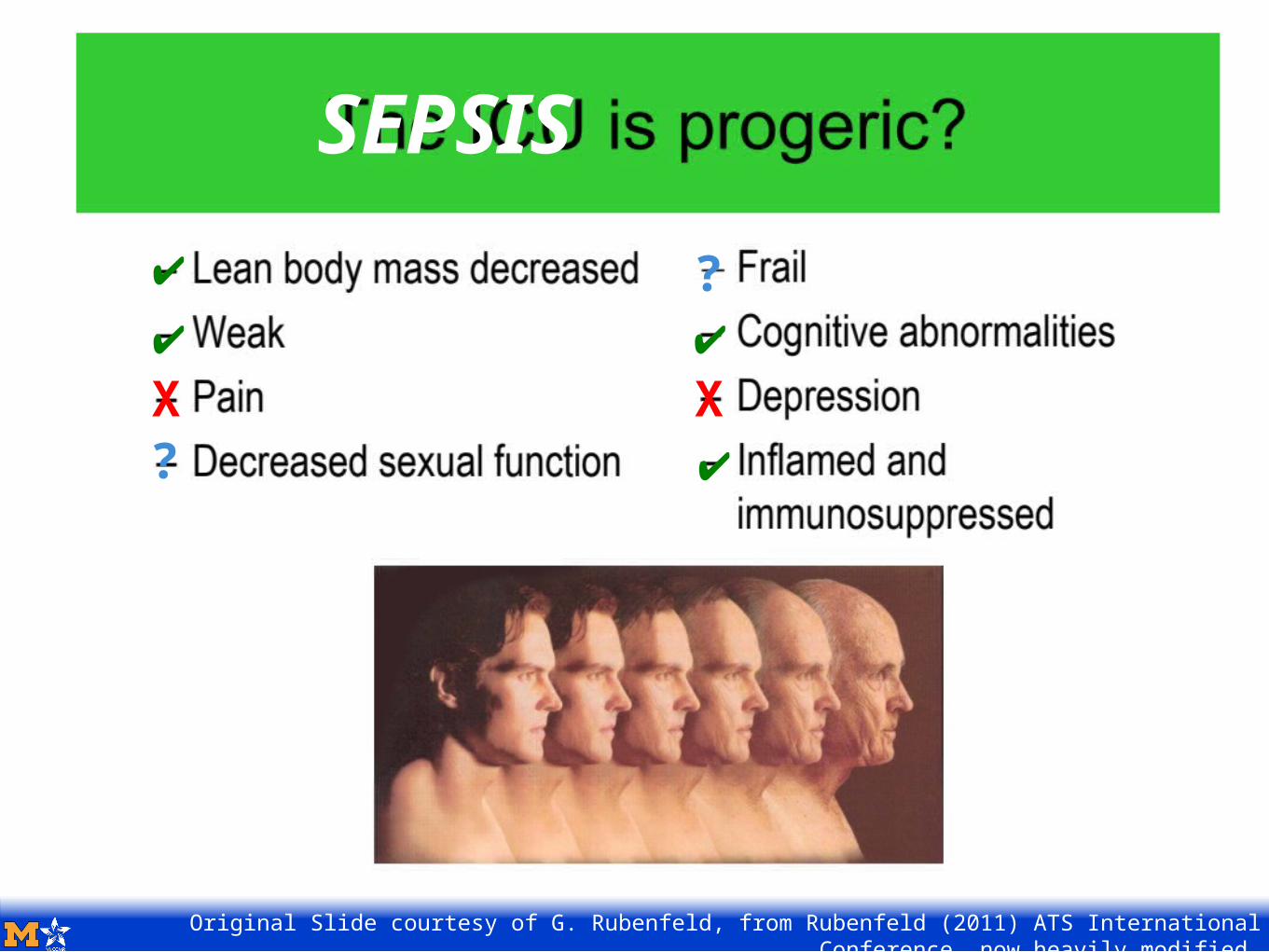
Original Slide courtesy of G. Rubenfeld, from Rubenfeld (2011) ATS International Conference, now heavily modified.
X X?
✔✔
✔
✔
?
SEPSIS





























