Embed Size (px)
Citation preview
benefits employee
guide
2021-2022
Page | 1
NOTES
Page | 2
Table of Contents NOTES ............................................................................................................................................................. 1 Table of Contents ........................................................................................................................................... 2 Benefits Resource List .................................................................................................................................. 3 Qualifying Life Events .................................................................................................................................... 4 What Constitutes a Qualifying Life Event? ................................................................................................... 5 Monthly Contributions Medical, Dental, & Vision ........................................................................................ 6 Tobacco Surcharge Affidavit ......................................................................................................................... 7 Spousal Surcharge Affidavit .......................................................................................................................... 8 Medical Benefits ............................................................................................................................................ 9 Baylor Scott & White Wellness ................................................................................................................... 10 MDLive ......................................................................................................................................................... 11 MDLive (continued) .................................................................................................................................... 12 Health Savings Account (HSA) ................................................................................................................... 14 Medical Eligible Expenses for HSA or FSA ................................................................................................ 15 Dental Benefits ........................................................................................................................................... 16 Voluntary Vision Benefits ........................................................................................................................... 17 Basic Life & AD&D Benefits ....................................................................................................................... 18 Voluntary Life & AD&D Benefits ................................................................................................................. 19 Voluntary Short-Term Disability Benefits ................................................................................................... 20 Long-Term Disability Benefits .................................................................................................................... 21 Employee Assistance Program (EAP) ......................................................................................................... 22 Employee Assistance Program (EAP) (continued)..................................................................................... 23 First Responder Resiliency Program ......................................................................................................... 24 Flexible Spending Account ......................................................................................................................... 25 Flexible Spending Account (continued) ..................................................................................................... 26 Limited Flexible Spending Account ............................................................................................................ 27 Holidays ....................................................................................................................................................... 28 Summary of Benefits Coverage Notice ..................................................................................................... 29 Glossary of Health Coverage & Medical Terms ........................................................................................ 30 Glossary of Health Coverage & Medical Terms (continued) .................................................................... 31 Glossary of Health Coverage & Medical Terms (continued) .................................................................... 32 Glossary of Health Coverage & Medical Terms (continued) .................................................................... 33
Page | 3
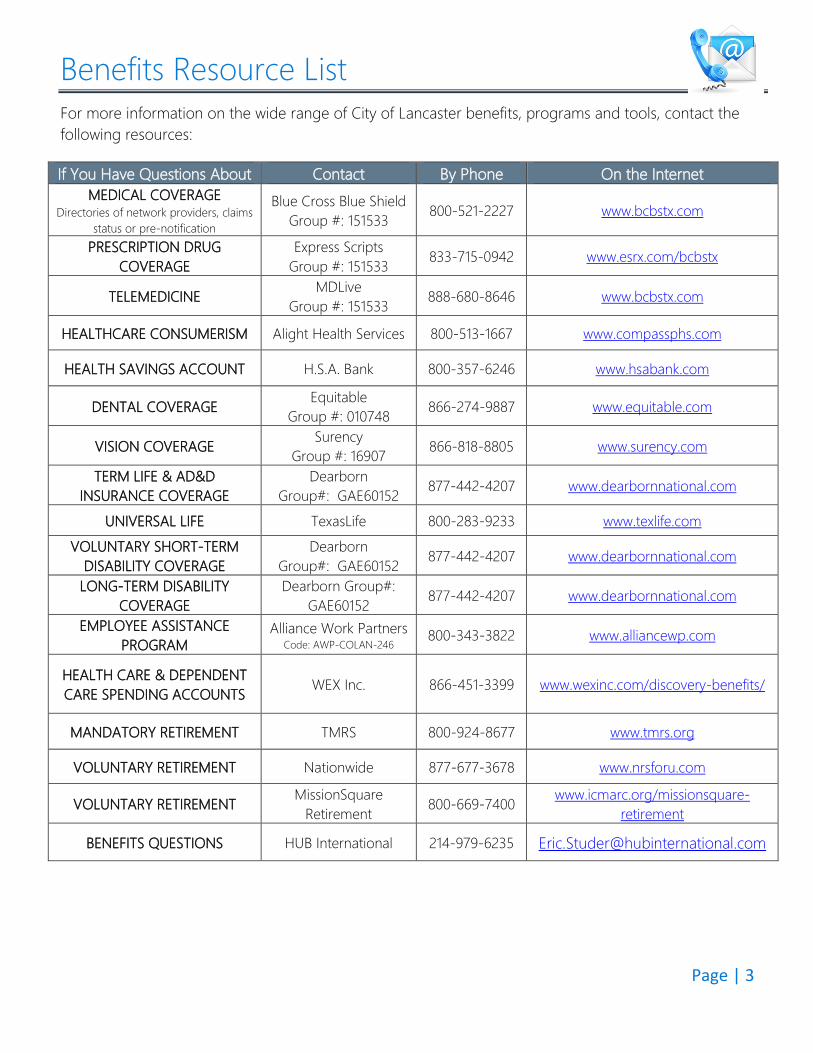
Benefits Resource List For more information on the wide range of City of Lancaster benefits, programs and tools, contact the following resources: If You Have Questions About Contact By Phone On the Internet
MEDICAL COVERAGE Directories of network providers, claims
status or pre-notification
Blue Cross Blue Shield Group #: 151533 800-521-2227 www.bcbstx.com
PRESCRIPTION DRUG COVERAGE
Express Scripts Group #: 151533 833-715-0942 www.esrx.com/bcbstx
TELEMEDICINE MDLive Group #: 151533 888-680-8646 www.bcbstx.com
HEALTHCARE CONSUMERISM Alight Health Services 800-513-1667 www.compassphs.com
HEALTH SAVINGS ACCOUNT H.S.A. Bank 800-357-6246 www.hsabank.com
DENTAL COVERAGE Equitable Group #: 010748 866-274-9887 www.equitable.com
VISION COVERAGE Surency Group #: 16907 866-818-8805 www.surency.com
TERM LIFE & AD&D INSURANCE COVERAGE
Dearborn Group#: GAE60152 877-442-4207 www.dearbornnational.com
UNIVERSAL LIFE TexasLife 800-283-9233 www.texlife.com VOLUNTARY SHORT-TERM
DISABILITY COVERAGE Dearborn
Group#: GAE60152 877-442-4207 www.dearbornnational.com
LONG-TERM DISABILITY COVERAGE
Dearborn Group#: GAE60152 877-442-4207 www.dearbornnational.com
EMPLOYEE ASSISTANCE PROGRAM
Alliance Work Partners Code: AWP-COLAN-246
800-343-3822 www.alliancewp.com
HEALTH CARE & DEPENDENT CARE SPENDING ACCOUNTS
WEX Inc.
866-451-3399 www.wexinc.com/discovery-benefits/
MANDATORY RETIREMENT TMRS 800-924-8677 www.tmrs.org
VOLUNTARY RETIREMENT Nationwide 877-677-3678 www.nrsforu.com
VOLUNTARY RETIREMENT MissionSquare Retirement 800-669-7400 www.icmarc.org/missionsquare-
retirement
BENEFITS QUESTIONS HUB International 214-979-6235 [email protected]
Page | 4
Qualifying Life Events
Changing Your Elections
In general, your annual pre-tax benefit elections are irrevocable for the plan year, October 1, 2021 through September 30, 2022.
However, if you experience a Change in Status or special enrollment event that directly affects your eligibility for coverage; you may change your election within
31 days of the event.
Under limited circumstances, an election change based solely on a Change in Status must be consistent with your Change in Status (i.e. if a child is born to you,
you add coverage for that child).
In general: Change in Status events provide more opportunities for you to make an election
change than do special enrollment rights.
If your event could be considered both a Change in Status event and a special enrollment right, you may make any change allowed by either a Change in Status
or special enrollment right.
Page | 5
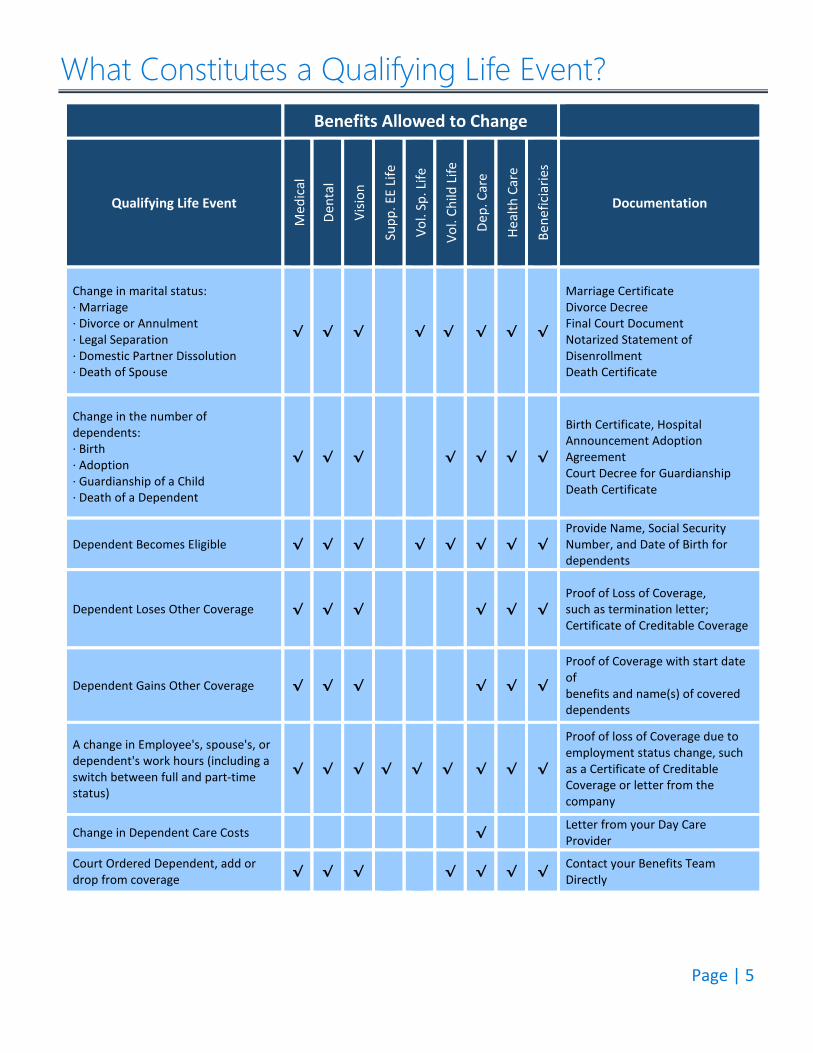
What Constitutes a Qualifying Life Event? Benefits Allowed to Change
Qualifying Life Event
Med
ical
Dent
al
Visio
n
Supp
. EE
Life
Vol.
Sp. L
ife
Vol.
Child
Life
Dep.
Car
e
Heal
th C
are
Bene
ficia
ries
Documentation
Change in marital status: ∙ Marriage∙ Divorce or Annulment∙ Legal Separation∙ Domestic Partner Dissolution∙ Death of Spouse
√ √ √ √ √ √ √ √
Marriage Certificate Divorce Decree Final Court Document Notarized Statement of Disenrollment Death Certificate
Change in the number of dependents: ∙ Birth∙ Adoption∙ Guardianship of a Child∙ Death of a Dependent
√ √ √ √ √ √ √
Birth Certificate, Hospital Announcement Adoption Agreement Court Decree for Guardianship Death Certificate
Dependent Becomes Eligible √ √ √ √ √ √ √ √ Provide Name, Social Security Number, and Date of Birth for dependents
Dependent Loses Other Coverage √ √ √ √ √ √ Proof of Loss of Coverage, such as termination letter; Certificate of Creditable Coverage
Dependent Gains Other Coverage √ √ √ √ √ √
Proof of Coverage with start date of benefits and name(s) of covered dependents
A change in Employee's, spouse's, or dependent's work hours (including a switch between full and part-time status)
√ √ √ √ √ √ √ √ √
Proof of loss of Coverage due to employment status change, such as a Certificate of Creditable Coverage or letter from the company
Change in Dependent Care Costs √ Letter from your Day Care Provider
Court Ordered Dependent, add or drop from coverage √ √ √ √ √ √ √ Contact your Benefits Team
Directly
Page | 6
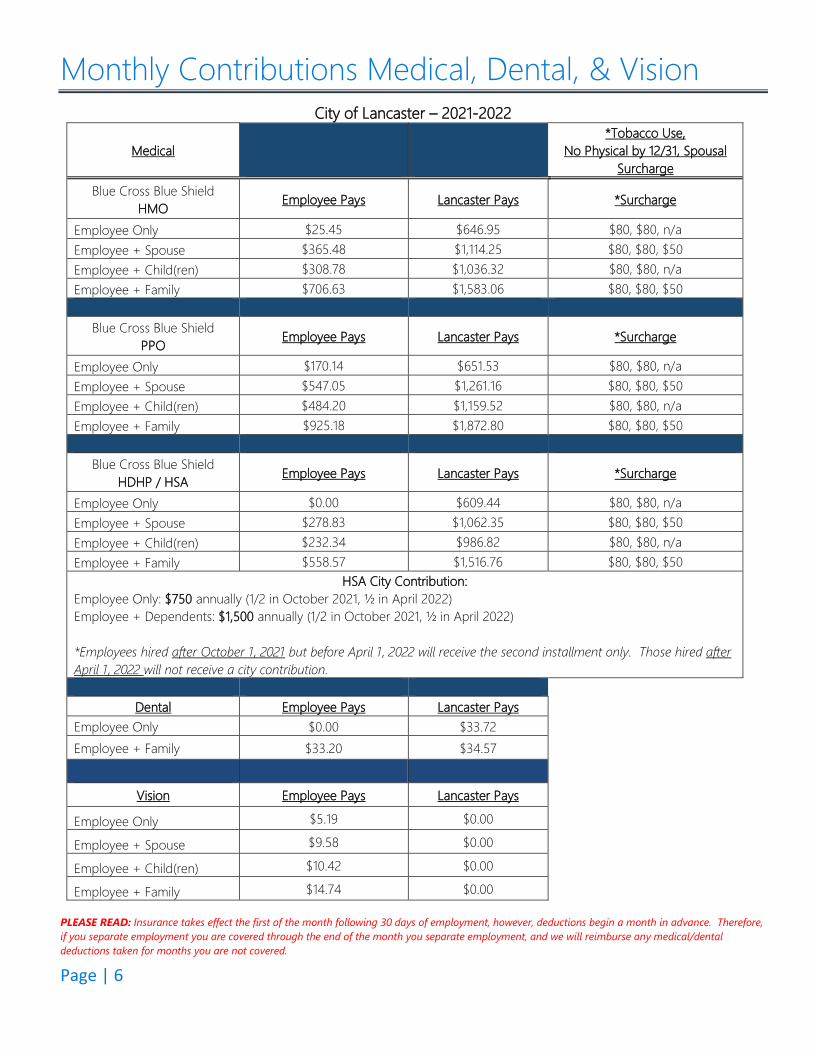
Monthly Contributions Medical, Dental, & Vision City of Lancaster – 2021-2022
Medical *Tobacco Use,
No Physical by 12/31, Spousal Surcharge
Blue Cross Blue Shield HMO Employee Pays Lancaster Pays *Surcharge
Employee Only $25.45 $646.95 $80, $80, n/a Employee + Spouse $365.48 $1,114.25 $80, $80, $50 Employee + Child(ren) $308.78 $1,036.32 $80, $80, n/a Employee + Family $706.63 $1,583.06 $80, $80, $50
Blue Cross Blue Shield PPO Employee Pays Lancaster Pays *Surcharge
Employee Only $170.14 $651.53 $80, $80, n/a Employee + Spouse $547.05 $1,261.16 $80, $80, $50 Employee + Child(ren) $484.20 $1,159.52 $80, $80, n/a Employee + Family $925.18 $1,872.80 $80, $80, $50
Blue Cross Blue Shield HDHP / HSA Employee Pays Lancaster Pays *Surcharge
Employee Only $0.00 $609.44 $80, $80, n/a Employee + Spouse $278.83 $1,062.35 $80, $80, $50 Employee + Child(ren) $232.34 $986.82 $80, $80, n/a Employee + Family $558.57 $1,516.76 $80, $80, $50
HSA City Contribution: Employee Only: $750 annually (1/2 in October 2021, ½ in April 2022) Employee + Dependents: $1,500 annually (1/2 in October 2021, ½ in April 2022)
*Employees hired after October 1, 2021 but before April 1, 2022 will receive the second installment only. Those hired afterApril 1, 2022 will not receive a city contribution.
Dental Employee Pays Lancaster Pays Employee Only $0.00 $33.72 Employee + Family $33.20 $34.57
Vision Employee Pays Lancaster Pays
Employee Only $5.19 $0.00
Employee + Spouse $9.58 $0.00
Employee + Child(ren) $10.42 $0.00
Employee + Family $14.74 $0.00
PLEASE READ: Insurance takes effect the first of the month following 30 days of employment, however, deductions begin a month in advance. Therefore, if you separate employment you are covered through the end of the month you separate employment, and we will reimburse any medical/dental deductions taken for months you are not covered.
Lancaster
Human Resources Department
P.O. Box 940 | Lancaster | Texas | 75146 | 972.275.1790 | www.lancaster-tx.com
City of Lancaster Tobacco Use Surcharge
To avoid the Tobacco Use Surcharge this form must be completed by you and
returned to the Human Resources Department by December 31, 2021.
EMPLOYEES WHO USE TOBACCO PRODUCTS AND DO NOT PROVIDE PROOF OF COMPLETION OF A TOBACCO CESSATION PROGRAM BY
12-31-2021 WILL PAY A $80 PER MONTH SURCHARGE UNTIL 9-30-2022.
City of Lancaster Employee Assistance Program offers a FREE Tobacco Cessation Program for employees.
You may sign up by calling 1-800-343-3822 or visit alliancewp.com I certify under penalty of perjury that this information is true and correct. When a person no longer meets the definition of tobacco free, the employee agrees to notify the Human Resources of any change in status within (30) days of the change. I acknowledge supervisors may confirm tobacco use form status with Human Resources to help enforce the program. I, the undersigned employee, understand that willful falsification of information on this affidavit may lead to disciplinary action, up to and including termination from employment. _____________________________________________________________ Tobacco Use Verification (to be completed by employee) Choose one of the following: I certify that I, _______________________________ do NOT use tobacco products. I certify that I, _______________________________ do use tobacco products and acknowledge a tobacco surcharge will be deducted from my paycheck. I certify that I, _______________________________ do use tobacco products, however, I wish to enroll in the tobacco cessation program (number above) offered by the City of Lancaster. I understand that failure to provide proof of enrollment by December 31, 2021 will activate the tobacco surcharge. Signature: __________________________ Date: ___________________________
(MEDICAL PLAN PARTICIPANTS ONLY)
Lancaster
Human Resources Department
P.O. Box 940 | Lancaster | Texas | 75146 | 972.275.1790 | www.lancaster-tx.com
City of Lancaster Spousal Surcharge Affidavit
To avoid the Spousal Surcharge of $50 monthly until 9-30-2022 this form must be
completed by you and returned to the Human Resources Department by December 31, 2021.
I, ____________________________ certify that ________________________ Employee Name (Print) Spouse Name (Print) does not have access to health care coverage outside the plan offerings through the City of Lancaster. I understand that this information is considered confidential and is subject to disclosure only as required by law. I certify under penalty of perjury that this information is true and correct. When a person no longer meets the definition of a covered spouse, I understand that person no longer qualifies as a Dependent. The employee agrees to notify Human Resources of any change in status within (30) days of the change. I, the undersigned employee, understand that willful falsification of information on this affidavit may lead to disciplinary action, up to and including termination from employment. Employee Signature: ____________________________________________ Date: ________________________________________________________
EMPLOYEE + SPOUSE & EMPLOYEE + FAMILY
MEDICAL PLAN PARTICIPANTS ONLY
Page | 9
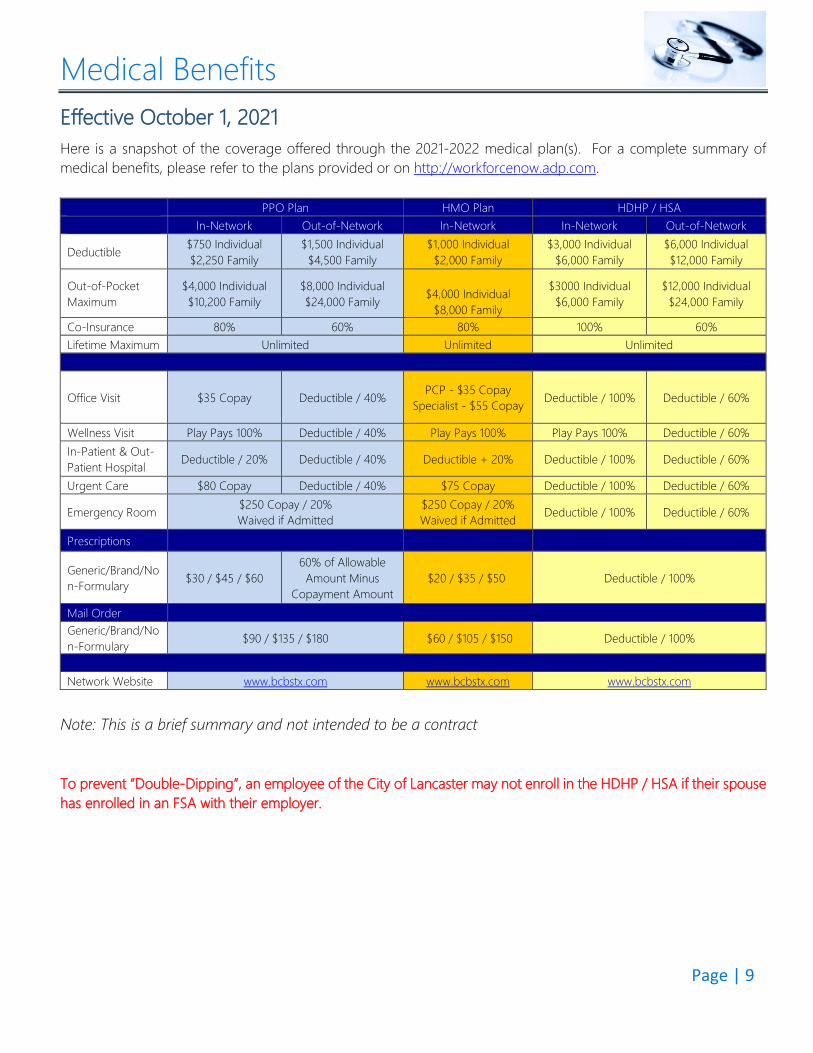
Medical Benefits Effective October 1, 2021 Here is a snapshot of the coverage offered through the 2021-2022 medical plan(s). For a complete summary of medical benefits, please refer to the plans provided or on http://workforcenow.adp.com.
PPO Plan HMO Plan HDHP / HSA In-Network Out-of-Network In-Network In-Network Out-of-Network
Deductible $750 Individual $2,250 Family
$1,500 Individual $4,500 Family
$1,000 Individual $2,000 Family
$3,000 Individual $6,000 Family
$6,000 Individual $12,000 Family
Out-of-Pocket Maximum
$4,000 Individual $10,200 Family
$8,000 Individual $24,000 Family
$4,000 Individual
$8,000 Family
$3000 Individual $6,000 Family
$12,000 Individual $24,000 Family
Co-Insurance 80% 60% 80% 100% 60% Lifetime Maximum Unlimited Unlimited Unlimited
Office Visit $35 Copay Deductible / 40% PCP - $35 Copay Specialist - $55 Copay Deductible / 100% Deductible / 60%
Wellness Visit Play Pays 100% Deductible / 40% Play Pays 100% Play Pays 100% Deductible / 60% In-Patient & Out-Patient Hospital Deductible / 20% Deductible / 40% Deductible + 20% Deductible / 100% Deductible / 60%
Urgent Care $80 Copay Deductible / 40% $75 Copay Deductible / 100% Deductible / 60%
Emergency Room $250 Copay / 20% Waived if Admitted
$250 Copay / 20% Waived if Admitted Deductible / 100% Deductible / 60%
Prescriptions
Generic/Brand/Non-Formulary $30 / $45 / $60
60% of Allowable Amount Minus
Copayment Amount $20 / $35 / $50 Deductible / 100%
Mail Order Generic/Brand/Non-Formulary $90 / $135 / $180 $60 / $105 / $150 Deductible / 100%
Network Website www.bcbstx.com www.bcbstx.com www.bcbstx.com
Note: This is a brief summary and not intended to be a contract To prevent “Double-Dipping”, an employee of the City of Lancaster may not enroll in the HDHP / HSA if their spouse has enrolled in an FSA with their employer.
Page | 10
Baylor Scott & White Wellness We are thrilled to continue offering our employees a comprehensive well-being program through our wellness program partner Baylor Scott and White Health (BSWH). Throughout the coming year BSWH will be providing engaging wellness resources and hosting wellness events through virtual and onsite options. All wellness events and resources revolve around one simple idea — to provide you the health and wellness tools and support needed to live well. Your BSWH wellness team is eager to get started on another great year! Below is a list of wellness programs to look forward to:
• Wellness Calendar with City-Wide Participation Opportunities • Collaborative Onsite and Virtual Wellness Events • Wellness Champions Opportunities • Biometric Intake and Tracking • Updated Wellness Portal with Health Screening Completion Confirmation • A Multitude of Online Wellness Resources
More information will be emailed to employees and posted on the city’s intranet as these programs are scheduled and the portal is updated.
Wellness Program Minimum Requirements
• Complete a Wellness Physical by December 31, 2021 EMPLOYEES WHO DO NOT PROVIDE PROOF OF A WELLNESS PHYSICAL BY 12-31-2021 WILL PAY AN $80 PER MONTH SURCHARGE UNTIL 9-30-2022. FORMS WILL NOT BE ACCEPTED AFTER 12-31-2021. Keep in mind; wellness will be paid at 100% on all three health plan options with no co-pay applied. It’s important to know, a wellness exam includes a routine exam by a Family or General Practitioner/Internist OR a well man or well woman exam by either of these providers OR a well woman exam by an Ob-Gyn. To ensure your wellness benefit is applied to wellness at 100%, make sure the claim coding is correct upon check-out on the date of your visit. Because wellness visits are covered 100% without a co pay, the City will not be reimbursing office visit co pays for the 2021-2022 benefit plan year. If you have already completed your annual health screening within the date ranges listed above: Simply provide the health screening form to your physician’s office to complete. This form will be emailed to you in the coming weeks. The physician’s office must fax the completed form directly to 214-820-8773 or scan and email the form to [email protected] Privacy Statement: Data collected on this form is considered Protected Health Information (PHI). This PHI is provided directly to Baylor Scott & White Health and not the City of Lancaster. Baylor Scott & White Health will provide high level summary data to the City of Lancaster once per year about the overall employee population, but the City does not receive any individual person’s data collected on this form. For more information about the City’s Privacy Policy, contact the City of Lancaster Human Resources office. If you have any questions, please email [email protected]
Page | 11
MDLive
Page | 12
MDLive (continued)

Page | 13
Page | 14
Health Savings Account (HSA) A Health Savings Account is an alternative to traditional health insurance; it is a savings product that offers a different way for consumers to pay for their health care. HSAs enable you to pay for current health expenses and save for future qualified medical retiree health expenses on a tax-free basis. You must be covered by a High Deductible Health Plan (HDHP) to be able to take advantage of the HSA. A HDHP generally costs less than what traditional health care coverage costs, so the money that you save on insurance premiums can therefore be put into the Health Savings Account. You own and you control the money in your HSA. Decisions on how to spend the money are made by you without relying on a third party or a health insurer. You can also (after a certain balance is reached) decide what types of investments to make with the money in the account in order to make it grow.
How does the HSA plan work? 1. Contributions to your HSA will be made by the City of Lancaster. The City of Lancaster’s 2021 / 2022 contribution is $750 for single coverage for the year and $1,500 for Employee & Spouse/Child(ren) or Family, deposited bi-annually on October 1st, and April 1st. You can also elect at Open Enrollment to make your own additional contribution to the HSA which would be taken out of your paycheck on a pre-tax basis. That money is available to pay for the qualifying medical expenses throughout the year. 2. When you need medical care and visit the doctor, emergency room or hospital, you will be responsible for the full cost of the visit (minus any network discounts). You can use the HSA account funds to pay for that visit at the time of the service, you can reimburse yourself at the end of the year or you can choose to pay for the visit out of pocket and let the HSA funds grow. 3. You may also use your HSA funds for dependent health care costs even if your dependent is not on the City’s plan.
HSA Advantages Choosing a High Deductible Health Plan with the Health Savings Account may help you save money: 1. The monthly premium on this plan is less expensive than the monthly premium for the buy-up PPO or the HMO plans. 2. Contributions to an HSA are made by the City of Lancaster and additional contributions may be made by the employee on a pre-tax basis up to the annual limits listed above. 3. Unused HSA contributions carry over from year to year and remain in the HSA for the following year’s medical expenses. 4. At age 65, the unused contributions and earned interest can be used to supplement retirement needs.
2021 Annual Contribution Limits ♦ The maximum annual HSA contribution for an eligible individual with self-only coverage is $3,600 or $7,200 for family
coverage. ♦ Catch up contribution for individuals who are between ages 55 to 65 is $1,000.
Page | 15
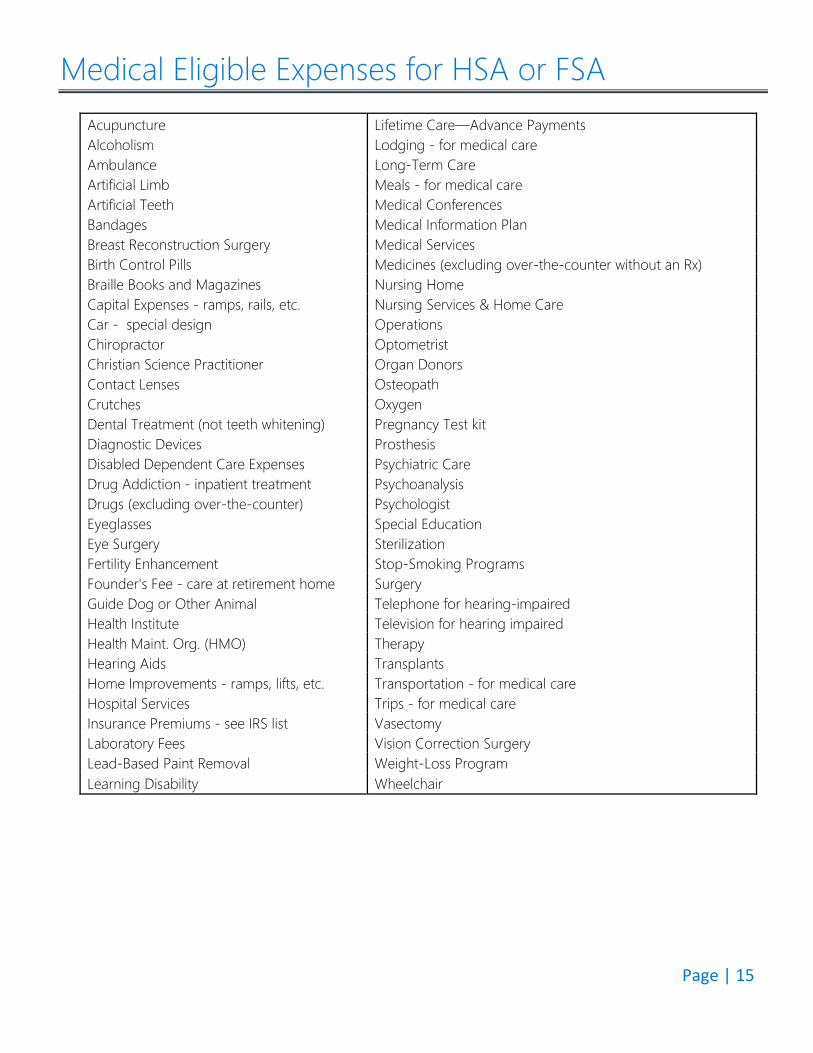
Medical Eligible Expenses for HSA or FSA Acupuncture Lifetime Care—Advance Payments Alcoholism Lodging - for medical care Ambulance Long-Term Care Artificial Limb Meals - for medical care Artificial Teeth Medical Conferences Bandages Medical Information Plan Breast Reconstruction Surgery Medical Services Birth Control Pills Medicines (excluding over-the-counter without an Rx) Braille Books and Magazines Nursing Home Capital Expenses - ramps, rails, etc. Nursing Services & Home Care Car - special design Operations Chiropractor Optometrist Christian Science Practitioner Organ Donors Contact Lenses Osteopath Crutches Oxygen Dental Treatment (not teeth whitening) Pregnancy Test kit Diagnostic Devices Prosthesis Disabled Dependent Care Expenses Psychiatric Care Drug Addiction - inpatient treatment Psychoanalysis Drugs (excluding over-the-counter) Psychologist Eyeglasses Special Education Eye Surgery Sterilization Fertility Enhancement Stop-Smoking Programs Founder's Fee - care at retirement home Surgery Guide Dog or Other Animal Telephone for hearing-impaired Health Institute Television for hearing impaired Health Maint. Org. (HMO) Therapy Hearing Aids Transplants Home Improvements - ramps, lifts, etc. Transportation - for medical care Hospital Services Trips - for medical care Insurance Premiums - see IRS list Vasectomy Laboratory Fees Vision Correction Surgery Lead-Based Paint Removal Weight-Loss Program Learning Disability Wheelchair
Page | 16
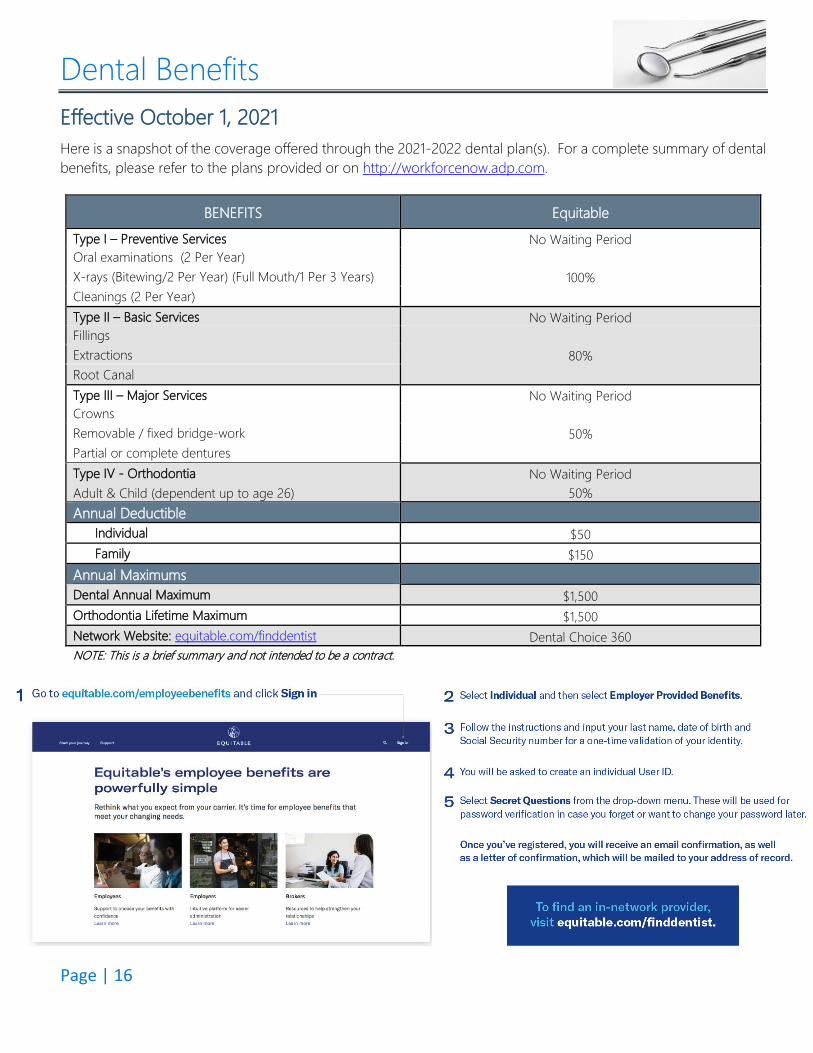
Dental Benefits Effective October 1, 2021 Here is a snapshot of the coverage offered through the 2021-2022 dental plan(s). For a complete summary of dental benefits, please refer to the plans provided or on http://workforcenow.adp.com.
BENEFITS Equitable Type I – Preventive Services No Waiting Period Oral examinations (2 Per Year)
100% X-rays (Bitewing/2 Per Year) (Full Mouth/1 Per 3 Years)Cleanings (2 Per Year)Type II – Basic Services No Waiting Period Fillings
80% Extractions Root Canal Type III – Major Services No Waiting Period Crowns
50% Removable / fixed bridge-work Partial or complete dentures Type IV - Orthodontia No Waiting Period Adult & Child (dependent up to age 26) 50% Annual Deductible Individual $50 Family $150 Annual Maximums Dental Annual Maximum $1,500 Orthodontia Lifetime Maximum $1,500 Network Website: equitable.com/finddentist Dental Choice 360 NOTE: This is a brief summary and not intended to be a contract.
Page | 17
Voluntary Vision Benefits Effective October 1, 2021 Here is a snapshot of the coverage offered through the 2021-2022 vision plan(s). For a complete summary of vision benefits, please refer to the plans provided or on www.surency.com
BENEFITS Surency
Eye Exam Network $10 Copay Non-Network Up to $35 Reimbursement Frames/ Lens Single Vision Network $20 Copay Non-Network Up to $25 Reimbursement Bifocal Lenses Network $20 Copay Non-Network Up to $40 Reimbursement Trifocal Lenses Network $20 Copay Non-Network Up to $55 Reimbursement Frames Network Up to $130 Allowance Non-Network Up to $65 Reimbursement Contacts *In Lieu of Glasses Network Medically Necessary $0 Copay/Covered in Full Elective Up to $130 Allowance Non-Network Medically Necessary Up to $200 Reimbursement Elective Up to $90 Reimbursement Exam Frequency 12 Months Lens Frequency 12 Months Frames Frequency 24 Months Network Website www.surency.com Surency Network of Providers NOTE: This is a brief summary and not intended to be a contract.
Page | 18
Basic Life & AD&D Benefits Effective October 1, 2021 City of Lancaster provides Basic Life and AD&D (Accidental Death and Dismemberment) insurance for you as a full-time employee at no additional cost. If you would like to purchase additional life insurance for yourself and/or your dependents, please see the Voluntary Life Insurance page for more information.
BENEFICIARY INFORMATION
Remember, it is important to designate beneficiaries for all of your insurance policies that require them. If you don’t, laws may cause death benefits to be distributed differently than you had planned resulting in additional taxes and may unnecessarily delay the process of finalizing payment to your loved ones. You should regularly review and, if necessary, update your beneficiary designations. You can update your beneficiary at any time by submitting a new beneficiary form to HR.
BASIC LIFE/AD&D BENEFITS Dearborn National Basic Life & AD&D Schedule 1X Basic Annual Earnings Guarantee Issue Amount $100,000 Maximum Amount $100,000
Employee Age Reduction Schedule
To 65% @ Age 70 To 45% @ Age 75 To 30% @ Age 80 To 15% @ Age 85
Waiver of Premium Included Accelerated Death Benefit Included Conversion Included Portability Not Included NOTE: This is a brief summary and not intended to be a contract.
For more information on the basic life plan(s), please visit http://workforcenow.adp.com.
Page | 19
Voluntary Life & AD&D Benefits Effective October 1, 2021
VOLUNTARY LIFE BENEFITS Dearborn National Employee Life Amount Increments of $10,000 Employee AD&D Amount Same as Life Employee Guarantee Issue Amount - New Hires Only
$150,000
Employee Maximum Amount $500,000 Employee Age Reduction Schedule To 65% @ Age 70
To 45% @ Age 75 To 30% @ Age 80 To 15% @ Age 85
Spouse Life Amount Increments of $5,000 to a maximum of $500,000 Spouse Guarantee Issue Amount $20,000 Spouse Maximum Amount May not exceed Employee Voluntary Life Benefit
Child Life Amount Birth to 6 months: $100
6 months to 26 years: $5,000 or $10,000 Child Maximum Amount $10,000 Waiver of Premium Included Conversion Included Suicide Clause Included – 1 Year
AGE RATED PREMIUMS (Rates based on Employee/Spouse)
Employee & Spouse (Rate Per $1,000)
AD&D Rate: (per $1,000) $0.045 Life Rate: Up to 24 $0.08 25-29 $0.08 30-34 $0.08 35-39 $0.12 40-44 $0.19 45-49 $0.28 50-54 $0.48 55-59 $1.29 60-64 $2.03
65-69 $3.23 70-74 $5.72 75-79 $5.72 Child Life Rate (Per $5,000) $1.00 NOTE: This is a brief summary and not intended to be a contract.
Guarantee issue Amounts listed are only available to new hires and their spouses. All other eligible employees and spouses will be required to submit Evidence of Insurability for any new coverage amount or increase in coverage amount, except as noted.
Page | 20
Voluntary Short-Term Disability Benefits
Effective October 1, 2021 If you are a full-time employee regularly scheduled to work at least 30 hours per week, Short-Term Disability benefits are available to you on a voluntary basis. In the event you become disabled from a non-work-related injury or sickness, disability income benefits are provided as a source of income.
SHORT TERM DISABILITY BENEFITS Dearborn National
Weekly Percentage 60% Weekly Maximum $1,000 Benefit Duration Up to 26 Weeks (1st week elimination period) Accident Benefit Begin 8th Day Sickness Benefit Begin 8th Day Pre-existing Condition 12/12
Rates per $10 Covered Benefit (Rates based as of October 1, 2019)
<20 $0.378 20-24 $0.380 25-29 $0.395 30-34 $0.370 35-39 $0.355 40-44 $0.379 45-49 $0.408 50-54 $0.506 55-59 $0.673 60-64 $0.848 65-69 $0.867 70+ $0.980
NOTE: This is a brief summary and not intended to be a contract. Should an employee leave employment or otherwise become ineligible to participate in the STD plan, coverage will end the day the employee becomes ineligible to participate.
Page | 21
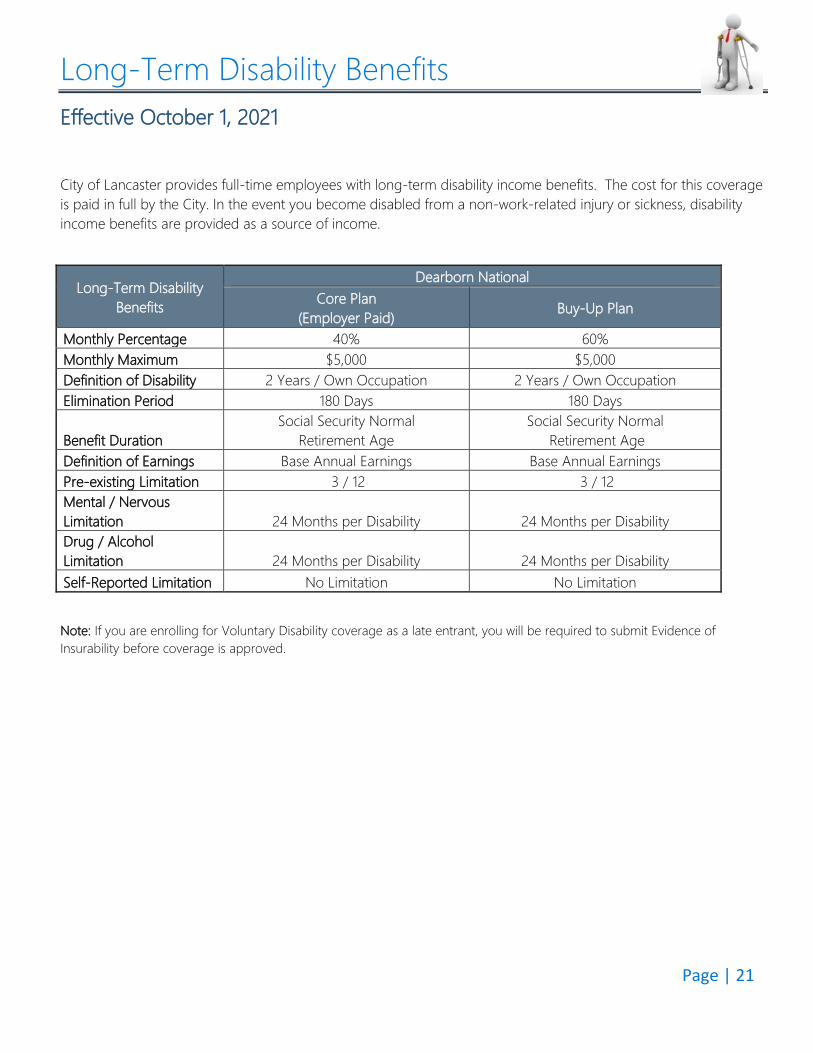
Long-Term Disability Benefits Effective October 1, 2021
City of Lancaster provides full-time employees with long-term disability income benefits. The cost for this coverage is paid in full by the City. In the event you become disabled from a non-work-related injury or sickness, disability income benefits are provided as a source of income.
Long-Term Disability Benefits
Dearborn National Core Plan
(Employer Paid) Buy-Up Plan
Monthly Percentage 40% 60% Monthly Maximum $5,000 $5,000 Definition of Disability 2 Years / Own Occupation 2 Years / Own Occupation Elimination Period 180 Days 180 Days
Benefit Duration Social Security Normal
Retirement Age Social Security Normal
Retirement Age Definition of Earnings Base Annual Earnings Base Annual Earnings Pre-existing Limitation 3 / 12 3 / 12 Mental / Nervous Limitation 24 Months per Disability 24 Months per Disability Drug / Alcohol Limitation 24 Months per Disability 24 Months per Disability Self-Reported Limitation No Limitation No Limitation
Note: If you are enrolling for Voluntary Disability coverage as a late entrant, you will be required to submit Evidence of Insurability before coverage is approved.
Page | 22
Employee Assistance Program (EAP) Effective October 1, 2021
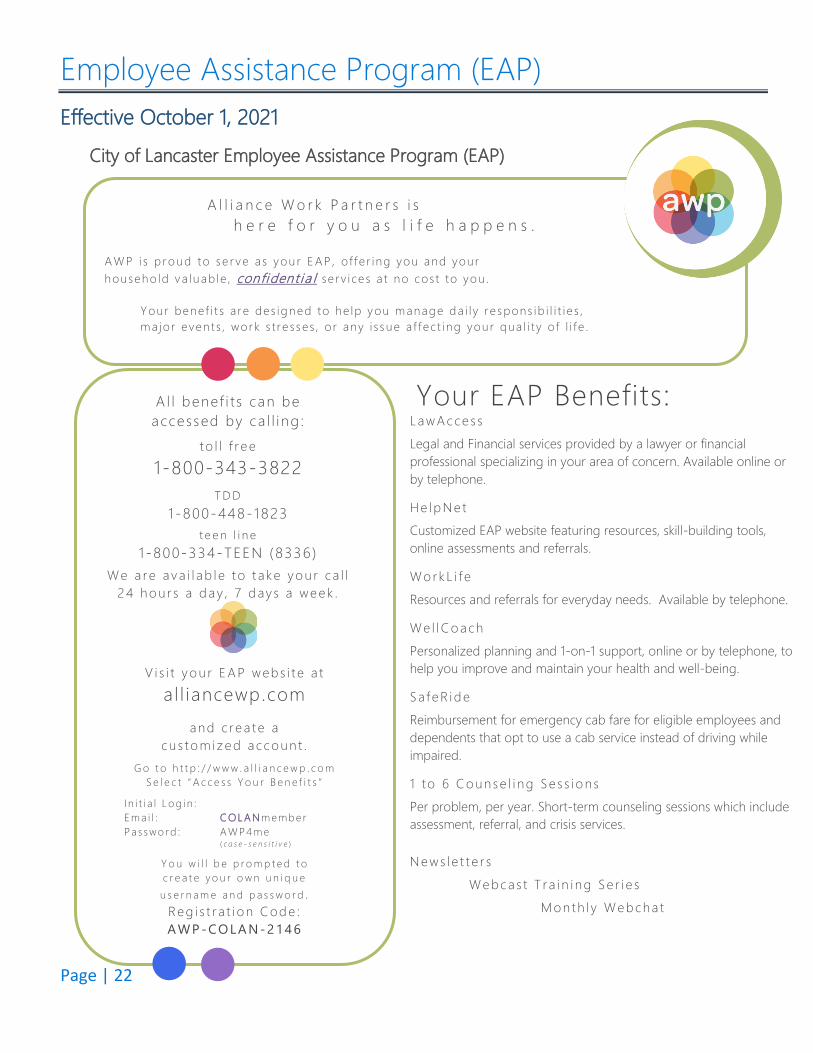
City of Lancaster Employee Assistance Program (EAP)
A l l i a n c e W o r k P a r t n e r s i s h e r e f o r y o u a s l i f e h a p p e n s .
AWP i s p roud to se r ve as you r E AP , o f f e r ing you and your househo ld va luab le , confident i a l se rv i ces a t no cos t to you .
Your bene f i t s a re des igned to he lp you manage da i l y re spons ib i l i t i e s , ma jo r event s , work s t re s ses , o r any i s sue a f f ec t ing your qua l i t y o f l i f e .
A l l benef i t s can be accessed by ca l l i ng :
t o l l f r ee
1-800-343-3822T D D
1 -800-448-1823t e e n l i n e
1 -800-334-TEEN (8336)We a re av a i l ab l e t o t ake y o u r c a l l
24 ho u r s a d ay , 7 d ay s a week .
Your EAP Benefits:LawAcce s s Legal and Financial services provided by a lawyer or financial professional specializing in your area of concern. Available online or by telephone.
He lp Ne t Customized EAP website featuring resources, skill-building tools, online assessments and referrals.
Wo rkL i f e Resources and referrals for everyday needs. Available by telephone.
We l lC o ach Personalized planning and 1-on-1 support, online or by telephone, to help you improve and maintain your health and well-being.
Sa f eR id e Reimbursement for emergency cab fare for eligible employees and dependents that opt to use a cab service instead of driving while impaired.
1 to 6 C o unse l i ng Se s s i o ns Per problem, per year. Short-term counseling sessions which include assessment, referral, and crisis services.
News l e t t e r s Web cas t T ra i n i ng Se r i e s
Mo n th l y Web cha t
V i s i t y o u r E AP web s i t e a t
a l l iancewp.com and c rea t e a
cu s to m iz ed ac co un t . G o t o h t t p : / / w w w . a l l i a n c e w p . c o m
S e l e c t “ A c c e s s Y o u r B e n e f i t s ”
I n i t i a l L o g i n : E ma i l : C OL AN memb e r Pa s swo rd : AWP4 me
( c a s e - s e n s i t i v e )
Y o u w i l l b e p r o m p t e d t o c r e a t e y o u r o w n u n i q u e u s e r n a m e a n d p a s s w o r d .
Reg i s t r a t i o n C od e : A W P -CO LA N-2146
Page | 23 Alliance Work Partners is a professional service of Workers Assistance Program, Inc. Copyright © 2014 Workers Assistance Program, Inc. Confidential and proprietary. All rights reserved.
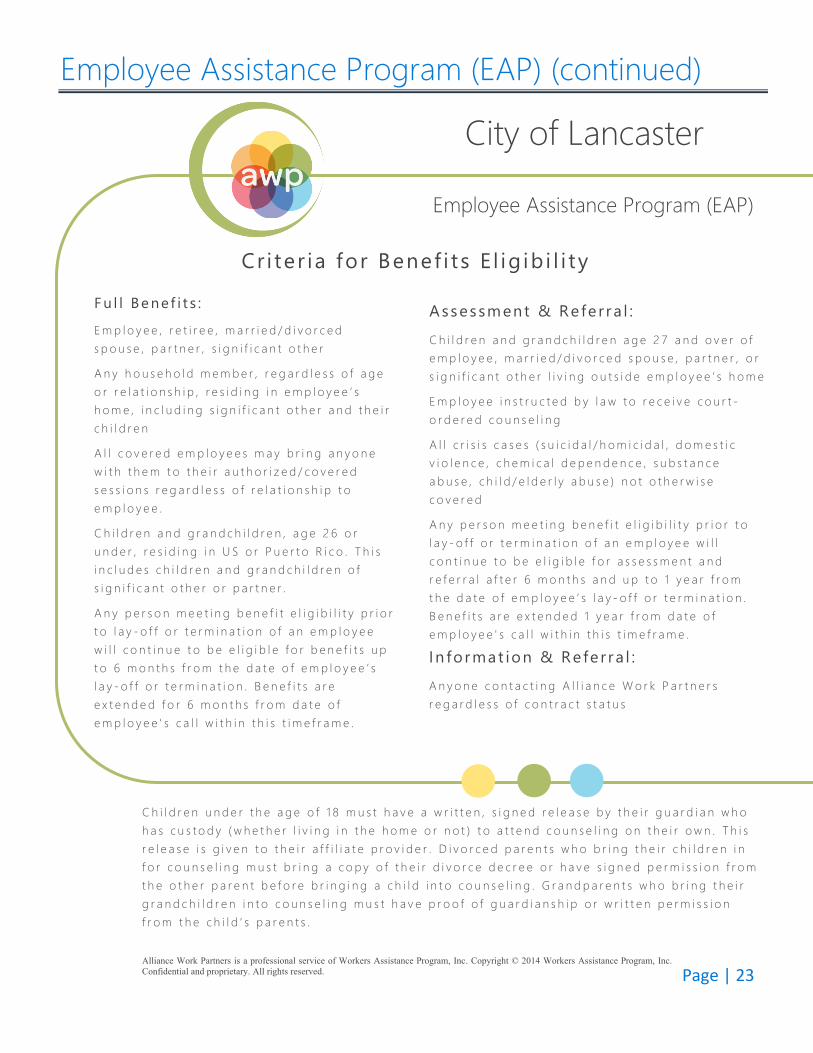
Employee Assistance Program (EAP) (continued) City of Lancaster
Employee Assistance Program (EAP)
Cr i ter ia for Benef i ts E l ig ib i l i ty
F u l l Be ne f i t s :
E m p l o y e e , r e t i r e e , m a r r i e d / d i v o r c e d s p o u s e , p a r t n e r , s i g n i f i c a n t o t h e r
A n y h o u s e h o l d m e m b e r , r e g a r d l e s s o f a g e o r r e l a t i o n s h i p , r e s i d i n g i n e m p l o y e e ’ s h o m e , i n c l u d i n g s i g n i f i c a n t o t h e r a n d t h e i r c h i l d r e n
A l l c o v e r e d e m p l o y e e s m a y b r i n g a n y o n e w i t h t h e m t o t h e i r a u t h o r i z e d / c o v e r e d s e s s i o n s r e g a r d l e s s o f r e l a t i o n s h i p t o e m p l o y e e .
C h i l d r e n a n d g r a n d c h i l d r e n , a g e 2 6 o r u n d e r , r e s i d i n g i n U S o r P u e r t o R i c o . T h i s i n c l u d e s c h i l d r e n a n d g r a n d c h i l d r e n o f s i g n i f i c a n t o t h e r o r p a r t n e r .
A n y p e r s o n m e e t i n g b e n e f i t e l i g i b i l i t y p r i o r t o l a y - o f f o r t e r m i n a t i o n o f a n e m p l o y e e w i l l c o n t i n u e t o b e e l i g i b l e f o r b e n e f i t s u p t o 6 m o n t h s f r o m t h e d a t e o f e m p l o y e e ’ s l a y - o f f o r t e r m i n a t i o n . B e n e f i t s a r e e x t e n d e d f o r 6 m o n t h s f r o m d a t e o f e m p l o y e e ' s c a l l w i t h i n t h i s t i m e f r a m e .
Assessment & Re fe r ra l : C h i l d r e n a n d g r a n d c h i l d r e n a g e 2 7 a n d o v e r o f e m p l o y e e , m a r r i e d / d i v o r c e d s p o u s e , p a r t n e r , o r s i g n i f i c a n t o t h e r l i v i n g o u t s i d e e m p l o y e e ’ s h o m e
E m p l o y e e i n s t r u c t e d b y l a w t o r e c e i v e c o u r t -o r d e r e d c o u n s e l i n g
A l l c r i s i s c a s e s ( s u i c i d a l / h o m i c i d a l , d o m e s t i c v i o l e n c e , c h e m i c a l d e p e n d e n c e , s u b s t a n c e a b u s e , c h i l d / e l d e r l y a b u s e ) n o t o t h e r w i s e c o v e r e d
A n y p e r s o n m e e t i n g b e n e f i t e l i g i b i l i t y p r i o r t o l a y - o f f o r t e r m i n a t i o n o f a n e m p l o y e e w i l l c o n t i n u e t o b e e l i g i b l e f o r a s s e s s m e n t a n d r e f e r r a l a f t e r 6 m o n t h s a n d u p t o 1 y e a r f r o m t h e d a t e o f e m p l o y e e ’ s l a y - o f f o r t e r m i n a t i o n . B e n e f i t s a r e e x t e n d e d 1 y e a r f r o m d a t e o f e m p l o y e e ' s c a l l w i t h i n t h i s t i m e f r a m e .
In fo rmat ion & Re fe r ra l : A n y o n e c o n t a c t i n g A l l i a n c e W o r k P a r t n e r s r e g a r d l e s s o f c o n t r a c t s t a t u s
C h i l d r e n u n d e r t h e a g e o f 1 8 m u s t h a v e a w r i t t e n , s i g n e d r e l e a s e b y t h e i r g u a r d i a n w h o h a s c u s t o d y ( w h e t h e r l i v i n g i n t h e h o m e o r n o t ) t o a t t e n d c o u n s e l i n g o n t h e i r o w n . T h i s r e l e a s e i s g i v e n t o t h e i r a f f i l i a t e p r o v i d e r . D i v o r c e d p a r e n t s w h o b r i n g t h e i r c h i l d r e n i n f o r c o u n s e l i n g m u s t b r i n g a c o p y o f t h e i r d i v o r c e d e c r e e o r h a v e s i g n e d p e r m i s s i o n f r o m t h e o t h e r p a r e n t b e f o r e b r i n g i n g a c h i l d i n t o c o u n s e l i n g . G r a n d p a r e n t s w h o b r i n g t h e i r g r a n d c h i l d r e n i n t o c o u n s e l i n g m u s t h a v e p r o o f o f g u a r d i a n s h i p o r w r i t t e n p e r m i s s i o n f r o m t h e c h i l d ’ s p a r e n t s .
Page | 24
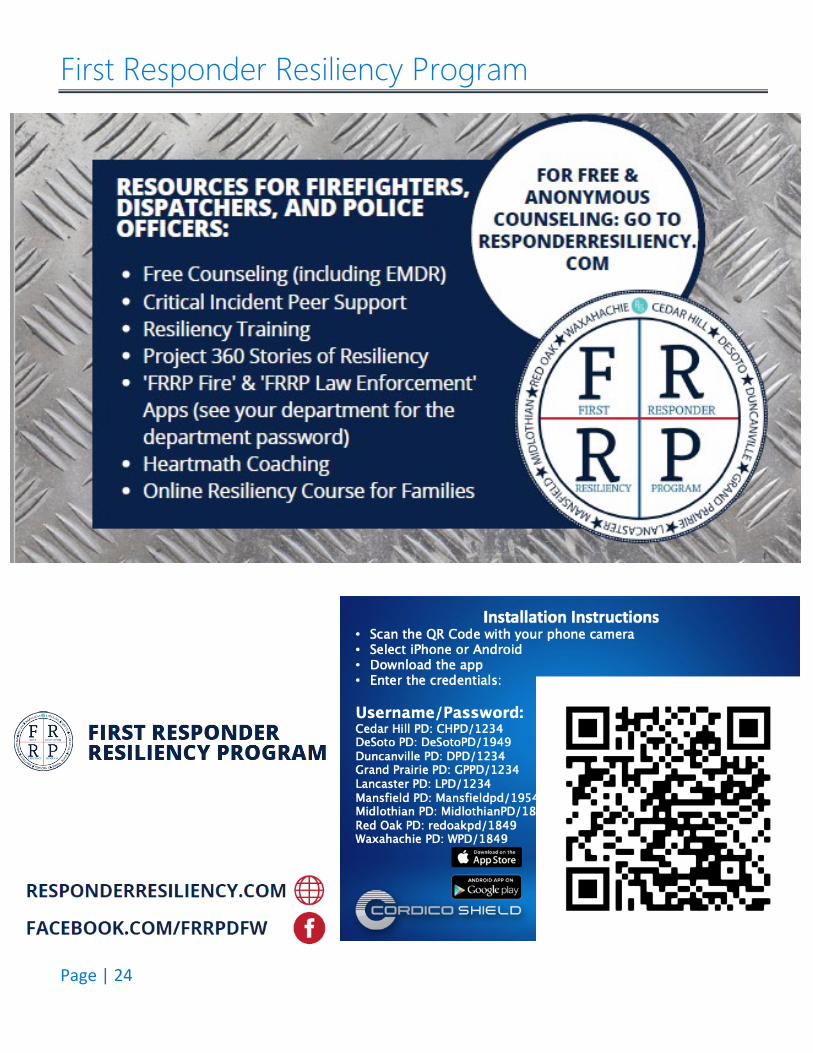
First Responder Resiliency Program
Page | 25
Flexible Spending Account Effective October 1, 2021
A Flexible Spending Account, or FSA, lets you set aside pre-tax money from your paychecks to spend on out-of-pocket healthcare expenses (i.e. co-pays, deductibles, over-the-counter items, etc.). Money that goes into an FSA is pre-tax, so by anticipating your family’s health care and dependent care costs for the next year, you can actually lower your taxable income.
Health Care Reimbursement FSA
This program lets employees pay for certain IRS-approved medical care expenses not covered by their insurance plan with pre-tax dollars. The annual maximum amount you may contribute to the Health Care Reimbursement FSA is $2,750. Some examples include:
Deductible, Prescriptions & Doctor Visit Co-Payments Over-the-Counter Medicines with a Prescription Vision services, including Lasik Eye Surgery, Glasses & Contacts Hearing services, including hearing aids and batteries Orthodontics, Dental deductibles and coinsurance Acupuncture
Dependent Care FSA
The Dependent Care FSA allows employees to use pre-tax dollars towards qualified dependent care for children under the age of age 13 or caring for elders. The annual maximum amount you may contribute to the Dependent Care FSA is $10,500 for 2021, (or $5,250 if married and filing separately).
Examples include:
The cost of child or adult dependent care The cost for an individual to provide care either in or out of your house Nursery schools and preschools (excluding kindergarten)
FSA Smart Tips
Cover any significant medical expenses early in the year using your FSA. You’ll spend the remainder of the year paying yourself back with the regular payroll deductions.
Save your receipts as proof of purchase in order to be reimbursed for your health care expenses from your FSA. So if you are making purchases that are eligible for reimbursement, you’ll want to keep them separate from other items.
Take advantage of the pre-tax savings and use your FSA dollars. Remember, unused money in an FSA at the end of the year is lost.
If enrolled in an HSA you cannot enroll in a traditional FSA program.
Page | 26
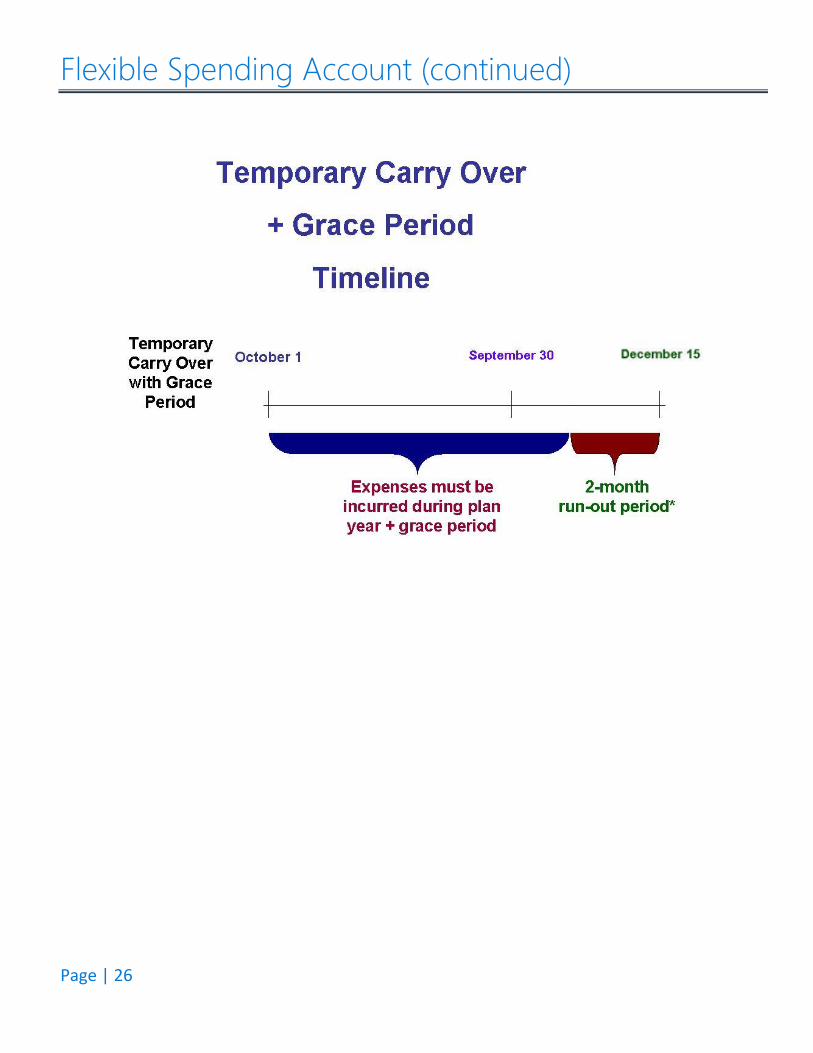
Flexible Spending Account (continued)
Page | 27
Limited Flexible Spending Account Effective October 1, 2021
*For those on the HDHP/HSA
Limited FSA
A Limited FSA is a cost-effective and easy way to help you manage expenses for dental and vision care. Like a traditional FSA, it allows you to use tax-free dollars to pay for expenses that are not covered, or only partially covered, by insurance. It’s known as a Limited FSA because the expenses you’ll pay from this account will be “limited” to what you spend on dental and vision care.
The best part of this FSA is that since you’re setting aside pre-tax dollars to cover these expenses, you’ll save money because less of your income is taxable. Expenses include:
• Dental and vision copayments, coinsurance amounts and deductibles• Dental and orthodontic services• Lasik eye surgery; and• Vision care products like eyeglasses and contact lenses
IRS Rules for Married Couples
Under IRS rules for married couples, an employee whose spouse has non-HDHP coverage, including a Health Flexible Spending Account (FSA), is not eligible for an HSA. For example, a wife may not contribute to an HSA if her husband has a health FSA through his employer; the reason being is that the Health FSA is considered “other coverage” and therefore, disqualifies the wife from contributing to the HSA.
There are very strict limits on the use of HSAs with FSAs – HSAs can be used with FSAs as long as there is no “Double-Dipping” – meaning that payments cannot be duplicated.
To prevent “Double-Dipping”, an employee of the City of Lancaster may not enroll in the HDHP / HSA if their spouse has enrolled in an FSA with their employer.
Page | 28
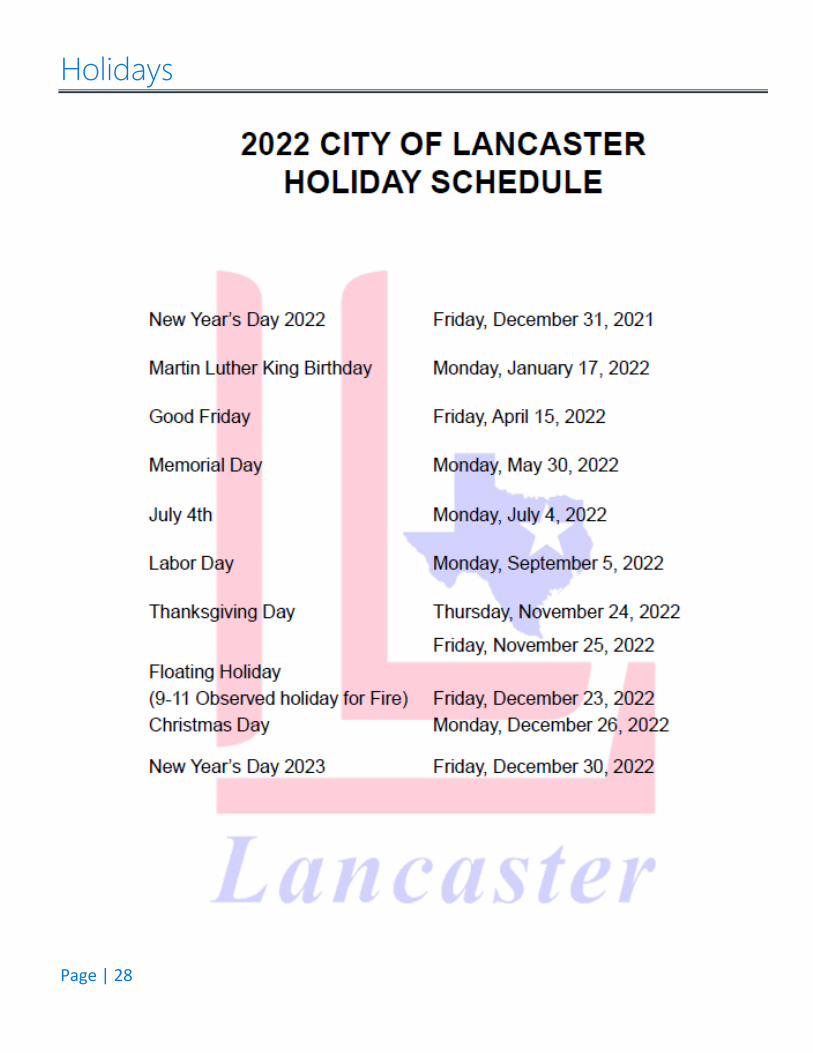
Holidays
Page | 29
Summary of Benefits Coverage Notice
Notice for Electronic Delivery of Applicable Documents, Including the Summary of Benefits and Coverage
Under the Affordable Care Act, the City of Lancaster group health plan is required to provide employees with a clear, consistent and comparable Summary of Benefits and Coverages (SBC) which contains information about your health plan benefits and coverage.
The City of Lancaster would like to provide you with important information regarding the availability of the plan’s summary of benefits.
Your voluntary consent is required for you to receive electronic documents such as the SBC. If you do not wish to consent to electronic distribution, please contact Dori Lee at [email protected]/972.275.1795. If you do not object to having electronic accessibility to such documents, and we do not hear otherwise from you within 14 (business days) from the date of this notice, no action is necessary and such information, such as the SBC, will be emailed or delivered to your work email address. If you do not have a work email address, or would like the City of Lancaster to electronically deliver applicable documents to another email address, please provide such email address Dori Lee at [email protected]/972.275.1795.
You may download and print the electronic versions of these documents at no charge or contact Dori Lee at [email protected]/972.275.1795 for a free copy to be mailed to you. Furthermore, any applicable documents, including the SBC, are available at ADP. If you have any trouble with the retrieval of such documents at www.adp.com, please contact [email protected]/972.275.1795.
Please note that it is your responsibility to update the City of Lancaster of any updated email address to which electronic documents are delivered. To do so, please contact [email protected]/972.275.1795.
Lastly, should you determine, at a later date, that you desire to receive a paper version of the Summary of Benefit Coverage (SBC) documents, or such other applicable documents, please notify Human Resources and such documents will be mailed to you free of charge.
Dori Lee Director of Human Resources / Civil Service The City of Lancaster [email protected] 972.275.1795
Michelle Evans Assistant Director of Human Resources The City of Lancaster [email protected] 972.275.1794
Page | 30
Glossary of Health Coverage & Medical Terms This glossary has many commonly used terms, but isn’t a full list. These glossary terms and definitions are intended to be educational and may be different from the terms and definitions in your plan. Some of these terms also might not have exactly the same meaning when used in your policy or plan, and in any such case, the policy or plan governs. (See your Summary of Benefits and Coverage for information on how to get a copy of your policy or plan document.)
Allowed Amount Maximum amount on which payment is based for covered health care services. This may be called “eligible expense,” “payment allowance" or "negotiated rate." If your provider charges more than the allowed amount, you may have to pay the difference. (See Balance Billing.)
AppealA request for your health insurer or plan to review a decision or a grievance again.
Balance BillingWhen a provider bills you for the difference between the provider’s charge and the allowed amount. For example, if the provider’s charge is $100 and the allowed amount is $70, the provider may bill you for the remaining $30. A preferred provider may not balance bill you for covered services.
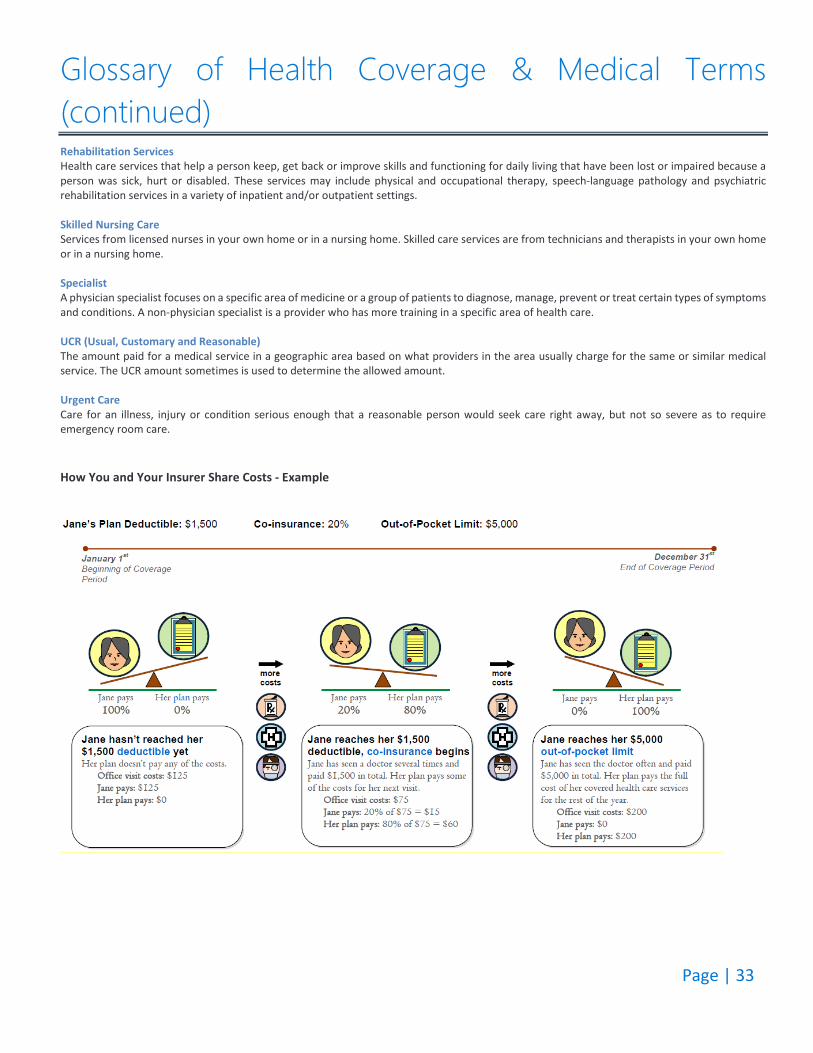
Co-insuranceYour share of the costs of a covered health care service, calculated as a percent (for example, 20%) of the allowed amount for the service. You pay co-insurance plus any deductibles you owe. For example, if the health insurance or plan’s allowed amount for an office visit is $100 and you’ve met your deductible, your co-insurance payment of 20% would be $20. The health insurance or plan pays the rest of the allowed amount.
Complications of Pregnancy Conditions due to pregnancy, labor and delivery that require medical care to prevent serious harm to the health of the mother or the fetus. Morning sickness and a non-emergency caesarean section aren’t complications of pregnancy.
Co-paymentA fixed amount (for example, $15) you pay for a covered health care service, usually when you receive the service. The amount can vary by the type of covered health care service.
DeductibleThe amount you owe for health care services your health insurance or plan covers before your health insurance or plan begins to pay. For example, if your deductible is $1000, your plan won’t pay anything until you’ve met your $1000 deductible for covered health care services subject to the deductible. The deductible may not apply to all services.
Durable Medical Equipment (DME) Equipment and supplies ordered by a health care provider for everyday or extended use. Coverage for DME may include: oxygen equipment, wheelchairs, crutches or blood testing strips for diabetics. Emergency Medical ConditionAn illness, injury, symptom or condition so serious that a reasonable person would seek care right away to avoid severe harm.
Emergency Medical TransportationAmbulance services for an emergency medical condition.
Emergency Room CareEmergency services you get in an emergency room.
Emergency ServicesEvaluation of an emergency medical condition and treatment to keep the condition from getting worse.
Page | 31
Glossary of Health Coverage & Medical Terms (continued) Excluded Services Health care services that your health insurance or plan doesn’t pay for or cover. Grievance A complaint that you communicate to your health insurer or plan. Habilitation Services Health care services that help a person keep, learn or improve skills and functioning for daily living. Examples include therapy for a child who isn’t walking or talking at the expected age. These services may include physical and occupational therapy, speech-language pathology and other services for people with disabilities in a variety of inpatient and/or outpatient settings. Health Insurance A contract that requires your health insurer to pay some or all of your health care costs in exchange for a premium. Home Health Care Health care services a person receives at home. Hospice Services Services to provide comfort and support for persons in the last stages of a terminal illness and their families. Hospitalization Care in a hospital that requires admission as an inpatient and usually requires an overnight stay. An overnight stay for observation could be outpatient care. Hospital Outpatient Care Care in a hospital that usually doesn’t require an overnight stay. In-network Co-insurance The percent (for example, 20%) you pay of the allowed amount for covered health care services to providers who contract with your health insurance or plan. In-network co-insurance usually costs you less than out-of-network co-insurance. In-network Co-payment A fixed amount (for example, $15) you pay for covered health care services to providers who contract with your health insurance or plan. In-network co-payments usually are less than out-of-network co-payments.
Medically Necessary Health care services or supplies needed to prevent, diagnose or treat an illness, injury, condition, disease or its symptoms and that meet accepted standards of medicine.
Network The facilities, providers and suppliers your health insurer or plan has contracted with to provide health care services. Non-Preferred Provider A provider who doesn’t have a contract with your health insurer or plan to provide services to you. You’ll pay more to see a non-preferred provider. Check your policy to see if you can go to all providers who have contracted with your health insurance or plan, or if your health insurance or plan has a “tiered” network and you must pay extra to see some providers.
Out-of-network Co-insurance The percent (for example, 40%) you pay of the allowed amount for covered health care services to providers who do not contract with your health insurance or plan. Out-of-network co-insurance usually costs you more than in-network co-insurance. Out-of-network Co-payment A fixed amount (for example, $30) you pay for covered health care services from providers who do not contract with your health insurance or plan. Out-of-network co-payments usually are more than in-network co-payments.
Page | 32
Glossary of Health Coverage & Medical Terms (continued) Out-of-Pocket LimitThe most you pay during a policy period (usually a year) before your health insurance or plan begins to pay 100% of the allowed amount. This limit never includes your premium, balance-billed charges or health care your health insurance or plan doesn’t cover. Some health insurance or plans don’t count all of your co-payments, deductibles, co-insurance payments, out-of-network payments or other expenses toward this limit.
Physician Services Health care services a licensed medical physician (M.D. – Medical Doctor or D.O. – Doctor of Osteopathic Medicine) provides or coordinates.
PlanA benefit your employer, union or other group sponsor provides to you to pay for your health care services.
PreauthorizationA decision by your health insurer or plan that a health care service, treatment plan, prescription drug or durable medical equipment is medically necessary. Sometimes called prior authorization, prior approval or precertification. Your health insurance or plan may require preauthorization for certain services before you receive them, except in an emergency. Preauthorization isn’t a promise your health insurance or plan will cover the cost.
Preferred ProviderA provider who has a contract with your health insurer or plan to provide services to you at a discount. Check your policy to see if you can see all preferred providers or if your health insurance or plan has a “tiered” network and you must pay extra to see some providers. Your health insurance or plan may have preferred providers who are also “participating” providers. Participating providers also contract with your health insurer or plan, but the discount may not be as great, and you may have to pay more.
PremiumThe amount that must be paid for your health insurance or plan. You and/or your employer usually pay it monthly, quarterly or yearly.
Prescription Drug CoverageHealth insurance or plan that helps pay for prescription drugs and medications.
Prescription DrugsDrugs and medications that by law require a prescription.
Primary Care PhysicianA physician (M.D. – Medical Doctor or D.O. – Doctor of Osteopathic Medicine) who directly provides or coordinates a range of health care services for a patient.
Primary Care ProviderA physician (M.D. – Medical Doctor or D.O. – Doctor of Osteopathic Medicine), nurse practitioner, clinical nurse specialist or physician assistant, as allowed under state law, who provides, coordinates or helps a patient access a range of health care services.
ProviderA physician (M.D. – Medical Doctor or D.O. – Doctor of Osteopathic Medicine), health care professional or health care facility licensed, certified or accredited as required by state law.
Reconstructive SurgerySurgery and follow-up treatment needed to correct or improve a part of the body because of birth defects, accidents, injuries or medical conditions.
Page | 33
Glossary of Health Coverage & Medical Terms (continued) Rehabilitation ServicesHealth care services that help a person keep, get back or improve skills and functioning for daily living that have been lost or impaired because a person was sick, hurt or disabled. These services may include physical and occupational therapy, speech-language pathology and psychiatric rehabilitation services in a variety of inpatient and/or outpatient settings.
Skilled Nursing CareServices from licensed nurses in your own home or in a nursing home. Skilled care services are from technicians and therapists in your own home or in a nursing home.
SpecialistA physician specialist focuses on a specific area of medicine or a group of patients to diagnose, manage, prevent or treat certain types of symptoms and conditions. A non-physician specialist is a provider who has more training in a specific area of health care.
UCR (Usual, Customary and Reasonable)The amount paid for a medical service in a geographic area based on what providers in the area usually charge for the same or similar medical service. The UCR amount sometimes is used to determine the allowed amount.
Urgent CareCare for an illness, injury or condition serious enough that a reasonable person would seek care right away, but not so severe as to require emergency room care.
How You and Your Insurer Share Costs - Example

Page | 34
Have questions? Please contact HUB International at (214) 979-6235.
Page | 35
211 N. Henry St. Lancaster, TX 75146
(972) 275-1794
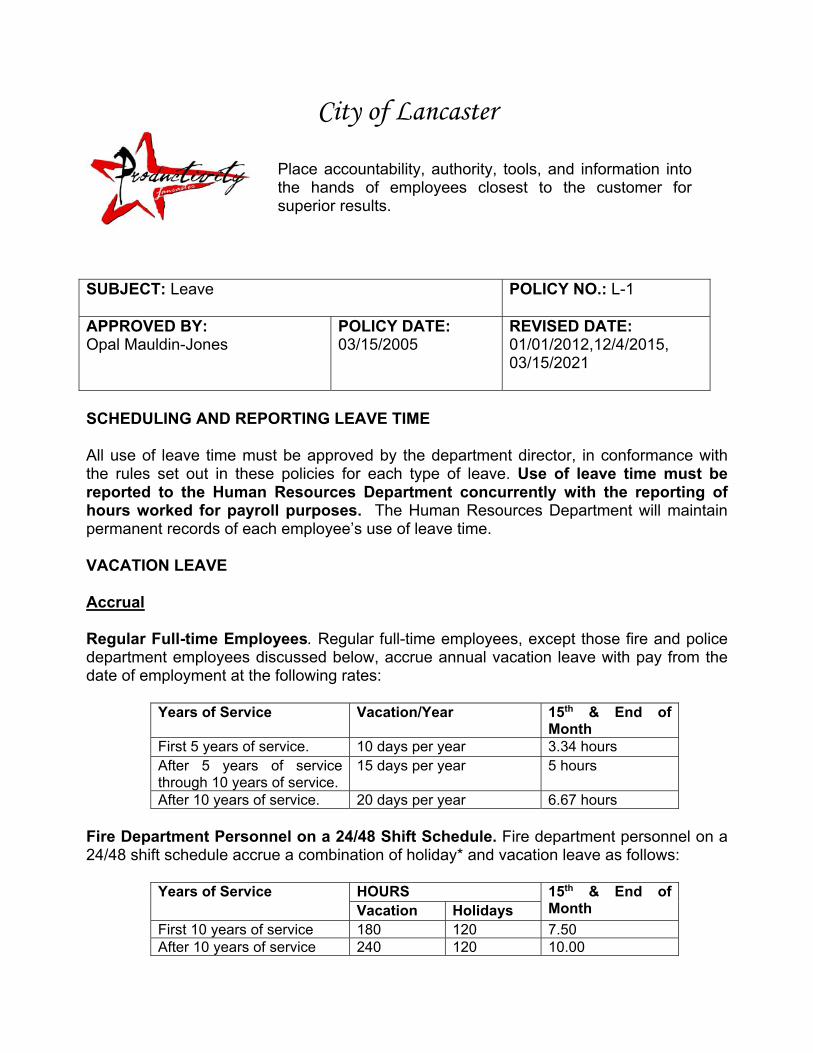
City of Lancaster
Place accountability, authority, tools, and information into the hands of employees closest to the customer for superior results.
SUBJECT: Leave POLICY NO.: L-1
APPROVED BY: Opal Mauldin-Jones
POLICY DATE: 03/15/2005
REVISED DATE: 01/01/2012,12/4/2015, 03/15/2021
SCHEDULING AND REPORTING LEAVE TIME All use of leave time must be approved by the department director, in conformance with the rules set out in these policies for each type of leave. Use of leave time must be reported to the Human Resources Department concurrently with the reporting of hours worked for payroll purposes. The Human Resources Department will maintain permanent records of each employee’s use of leave time. VACATION LEAVE Accrual Regular Full-time Employees. Regular full-time employees, except those fire and police department employees discussed below, accrue annual vacation leave with pay from the date of employment at the following rates:
Years of Service Vacation/Year 15th & End of Month
First 5 years of service. 10 days per year 3.34 hours After 5 years of service through 10 years of service.
15 days per year 5 hours
After 10 years of service. 20 days per year 6.67 hours Fire Department Personnel on a 24/48 Shift Schedule. Fire department personnel on a 24/48 shift schedule accrue a combination of holiday* and vacation leave as follows:
Years of Service HOURS 15th & End of Month Vacation Holidays
First 10 years of service 180 120 7.50 After 10 years of service 240 120 10.00
2
*Holiday hours are scheduled the same as vacation leave, but may not be carried over to the next calendar year. Police Department Personnel. Police department personnel on other than a forty (40) hour, Monday-through-Friday schedule accrue a combination of holiday and vacation leave as follows:
Years of Service Vacation 15th & End of Month
First 10 years of service 15 days 5 hours After 10 years of service 20 days 6.67 hours
Newly Hired Employees Accrual. Newly hired employees will begin accruing vacation leave with their first full pay period. Use of Vacation Leave. An employee may use vacation upon accrual, with the approval of the department director. Limit on Accumulation of Vacation Leave. In no case shall more than two (2) year's accumulation be carried over to the next calendar year according to each employee’s accrual schedule.
Vacation Carry Over Maximum Chart
General Government Under 5 years 160 hours Over 5 years and under 10 years 240 hours Over 10 years 320 hours Police Civil Service Under 10 years 240 hours Over 10 years 320 hours Fire Personnel on Shift Under 10 years 360 hours Over 10 years 480 hours
3
Scheduling of Vacation Leave Vacation leave may be taken at such times as to meet the operating requirements of the City and in so far as possible, the preference of the employee. Accrued vacation leave cannot be taken in less than one hour increments. Departments may expand minimum requirements. Deceased employees’ remaining accrued vacation leave will be paid to his/her beneficiary or estate in accordance with Texas Municipal Retirement System (TMRS) guidelines. A supervisor may grant vacation leave at a time during the year that will best serve public interest. Priority may be given to an employee based upon departmental policy. Payment Upon Separation From Employment. Upon separation, accrued, earned vacation hours are payable at the employee’s hourly rate at the time of separation. SICK LEAVE Purpose of Sick Leave. Allowances for sick leave with pay shall be granted to all regular full-time employees in case of personal injury or sickness; and for necessary medical, dental and optical examinations or treatments of the employee or a member of the employee’s immediate family (spouse, child or parent, or the child or parent of a spouse). Sick leave may also be used for bereavement leave, as defined in section 5.9.4. In addition, sick leave may be taken for the birth and care of the newborn child of the employee; for placement with the employee of a son or daughter for adoption or foster care; to care for an immediate family member with a serious health condition; or for the care of an individual with a serious health condition who resides with the employee and for whom the employee is the principal caretaker. Sick leave is meant to be a protection in case of need, and not a benefit to be used whenever wanted. All allowances of such leave shall be in conformance with this stated purpose. Accrual of Sick Leave. Every full-time employee accrues sick leave. All accrued sick leave is forfeited when employment is terminated except as provided for in state and local government law. Yearly sick leave accruals are as follows: All employees, except Civil Service employees of the fire department working a 24-
hour shift, will accrue sick leave at a rate of 6.67 hours per month (10 days per year).
Employees of the fire department on 24-hour shift will accrue sick leave at a rate of
one and one-fourth (1 ¼) working days for each month employed in a calendar year, totaling a maximum of fifteen (15) working days to an employee’s credit for each twelve months in accordance with Section 143.045 of the Civil Service Law.
4
Maximum Accrual. Sick leave may be accumulated in accordance with the following: All regular employees except civil service classified personnel may accrue a maximum of 2080 hours. Civil Service Personnel may accumulate sick leave without limit. Leave Time Deficits. It is the standard practice of the City of Lancaster that City employees not be allowed to accrue leave time deficits. Departments may not allow an employee to have a leave deficit by any informal practice, such as failing to report leave time when actually taken. Holidays. If an official holiday occurs during a period of illness, an employee will be charged for the holiday instead of sick leave. Vacation. If an employee becomes ill while taking vacation leave, the period of illness may be charged as sick leave, and the charge against vacation leave will be reduced accordingly. A written request for this substitution must be made within three (3) days after the employee has returned to work and must be supported by a medical statement from a health care professional. Restrictions on Use Minimum Use. Accrued sick leave absences may be taken in no smaller than one (1) hour increments. Physician’s Certification. A physician’s certificate is a report from a licensed health care professional that verifies that an employee has been seen by the physician. This certificate should also state whether the employee is or is not able to perform their duties, as well as an estimate of the duration of the illness. A physician’s certificate is required if an employee is off-duty due to illness or injury for more than three (3) days. The original of this report is submitted to the supervisor. A doctor’s certificate is required for every sick leave use if an employee has reported five (5) incidents of illness/injury in the past twelve (12) months, or has a negative sick leave review in the past six (6) months. In the event an employee is admitted to a hospital as a result of injury/illness, that period of sick leave usage will be excluded from the five (5) incident provision above. The supervisor may require a doctor’s certificate for any employee whose sick leave usage indicates a chronic illness or excessive usage pattern. Doctor’s Release. A doctor’s release authorizing the employee to return to work is required: When an employee is off work for an illness or non-work related injury for three (3)
days or longer. When an employee has been hospitalized with a major medical occurrence. When an employee is returning to regular work from an on-the-job injury.
5
At the request of the department director or Human Resources Director to ascertain the employee’s ability to perform his or her duties.
Sick Leave Review. All sick leave usage will be reviewed. Employees having five (5) incidents of sick leave during the previous twelve 12-month period will have their record scrutinized, and may be scheduled for an interview to discuss their sick leave usage. (Note: An “incident” of sick leave is any consecutive loss of time, either one-day or multiple days.) Upon review if it determined that there have been a negative review it will generate counseling and/or disciplinary action as appropriate, and will require the employee to submit a doctor’s certificate for every absence until the 5/12 record no longer applies. If an employee has a recurring health problem, every effort will be made to assist that employee in recovering from the illness. Follow-up in these cases will be tailored to the needs of the individual situation. Items than can result in a negative sick leave review may include, but are not limited to: Patterns of absenteeism. Evidence of outside occupation during a sick leave period. Recent denial of vacation or holiday leave or a substitution request that coincides
with the sick leave period. Evidence that indicates an abuse of sick leave.
Summary. It is the intent of this policy to provide for the health and well being of all employees, while assuring compliance with reasonable standards of work attendance, state and federal laws. Sick leave is not a free day off – it is a form of insurance against income loss for ill or injured employees or other members of the family as defined in the policy. Inappropriate use of sick leave will be subject to disciplinary action. Payment Upon Separation From Employment. Except as outlined in state and local government law, an employee will not be reimbursed for accrued sick leave upon separation from employment. JURY DUTY An employee will be granted leave with pay when required to be absent from work for jury duty. An employee required to serve on jury duty shall notify his or her department director as soon as practicable of the requirement to serve, and the projected length of time the employee’s attendance will be required. Appearance as a Witness. An employee will be granted leave with pay when required to be absent from work to appear as a witness in a court proceeding to testify on behalf of the City or to appear as a City employee to testify as to a matter related to his or her employment with the City in a case in which the City is not a party. When the employee is required to appear as a witness or party in any other court proceeding, the employee may
6
use accumulated vacation time or compensatory time for court appearances. Under court order an employee may appear without pay. The employee shall provide his or her department director with a copy of the subpoena or other record requiring the employee’s appearance in court. Voting. Employees have three consecutive hours available to vote in any election in which the employee is registered to vote and the three consecutive hours can take into account hours that the employee is not scheduled to work. City employees will be allowed three consecutive hours off in order to vote, subject to the following restrictions: The time available from the time polls open until the beginning of the employee’s shift, or from the time the employee’s shift ends until the time the polls close will be considered as part of the time the employee has available to vote. Employees must use the time taken for the purpose of voting. Employees must be at work during all regularly scheduled hours that are not actually used to vote. Employees may not engage in other activities during time when they have been released from work to vote. Scheduling of the time off for voting must be approved by the employee’s supervisor. BEREAVEMENT LEAVE Paid Leave. Upon the approval of the department director and the City Manager, an employee may be granted emergency leave with pay for up to three (3) days per fiscal year, to attend the funeral, or to deal with other matters relating to the death of an immediate family member. For purposes of this provision, immediate family member shall mean the employee’s spouse; and the children, parents, siblings, aunts, uncles, nieces, nephews, grandchildren and grandparents of the employee or the employee’s spouse and members of the employee’s household, whether or not related by blood or marriage. Use of Other Leave Time. An employee may use accumulated leave time, including sick leave, for the purpose of attending a funeral or to deal with other matters relating to the death of an immediate family member or household member, as defined above, when bereavement leave is exhausted. Leave Without Pay. Upon approval of the department director and the City Manager, an additional forty (40) hours of leave without pay may be granted to employees who have exhausted bereavement leave and all other paid leave time to deal with matters relating to the death of an immediate family or household member. Other than immediate family. Death of a relative or other person not included in the immediate family may be considered on an individual basis as approved by City Manager or his/her designee and time off granted as the circumstances warrant.
7
DISCRETIONARY LEAVE OF ABSENCE Full time employees with five (5) years of service who have exhausted Family and Medical Leave (FML) or who seek leave for reasons other than family and medical leave, may apply for a discretionary leave of absence. Such leaves are totally within the discretion of the City and will be granted only if the City Manager believes the employee’s time away from the job would be in the best interests of both the employee and the City. If such a leave is approved, it will be for such length of time and on such other terms and conditions as the City approves, up to 180 days. The City reserves the right to fill such positions and may not be able to hold an employee’s job open while the employee is on discretionary leave. Thus, an employee on such leave cannot be guaranteed reinstatement at the conclusion of such a leave. UNPAID LEAVE OF ABSENCE Employees who are on a statutory or approved discretionary leave of absence and have exhausted available benefit time will transition to an unpaid leave of absence for the duration of the statutory leave. Non statutory unpaid leave of absence requests may be granted once per fiscal year for up to one week by the Department Director. Extensions or additional time for non-statutory unpaid leaves are not authorized and will subject the employee to disciplinary action for failure to report to work. This policy will be administered consistently with the City’s obligations under the Americans with Disabilities Act. An unpaid leave of absence will not be authorized unless there is a reasonable expectation that the employee will return to employment with the City at the end of the approved leave period. Under no circumstances may an employee on an authorized unpaid leave of absence with or without pay work another job, whether for pay, as a volunteer or as self-employment, unless expressly authorized in writing by the Department Director and the Director of Human Resources on the outside employment authorization form. Employees returning from an unpaid leave of absence will be reinstated to their same position or one of similar pay and status, provided the City’s circumstances have not changed to the extent that it would be impossible or unreasonable to provide reinstatement. If the same job or one of similar pay and status is not available, reinstatement may, at the City’s discretion, be deferred until a position is available. Usually, an employee who fails to return to work at the conclusion of an approved an unpaid leave of absence will be considered to have voluntarily resigned employment with the City.
8
During an unpaid leave of absence, vacation, sick leave, holiday pay, and other benefits do not accrue. Employees who have group health or any other kind of insurance through the City continue to be responsible for paying their portion of the premiums while on an unpaid leave of absence. An employee’s failure to pay the employee’s portion of insurance premiums during an unpaid leave of absence may result in cancellation of coverage. The City Manager may revoke authorized leave without pay at any time. Failure to return to work after the expiration of an authorized unpaid leave of absence or failure to provide required medical status reports, physician's statements, or to contact the City per the required schedule will likely result in revocation of the leave and/or disciplinary action up to and including dismissal. TERMINATION If an employee’s absence while on leave will impair the functions of the City, the employee may be replaced after all family and medical leave is exhausted. If the previous position is not available the employee may apply for another position within the City if they are able to perform the essential functions of that job with or without reasonable accommodation. However, the employee may be considered terminated upon missing a 180 days of work due to injury or illness, and it is medically shown that because of chronic physical injury, ailment or condition: The employee is unable to return to his/her position and perform the essential
functions of the job, with or without reasonable accommodations. The employee is unable to transfer to another position within the City and perform
the essential functions of that job with or without reasonable accommodation.
City of Lancaster
Dedication: Each person finishes their role in the process and completes the work with passion. Loyalty and commitment to the success of others through our professionalism and willingness to embrace new colleagues.
SUBJECT: Longevity POLICY NO.: L-3
APPROVED BY: Opal Mauldin Robertson
POLICY DATE: 03/15/2005
REVISED DATE: 01/01/2012
LONGEVITY Regular Full-Time employees will be compensated at a rate of $4.00 per month for each year of service after one year of continuous service. In addition to longevity pay, employees will earn one-time lump sum compensation in accordance with the following schedule:
Years of Service Amount 5 $ 50.00 10 $100.00 15 $200.00 20 $300.00 25 $500.00 30 $700.00 35 $900.00 40 $1,100.00
City of Lancaster
Excellence: Working together to win trust, capitalize on our creative talents, acknowledging and sharing ideas, to create a high performing organization.
SUBJECT: Retirement POLICY NO.: R-4
APPROVED BY: Opal Mauldin Robertson
POLICY DATE: 03/15/2005
REVISED DATE: 01/01/2012, 06/09/2012
Texas Municipal Retirement System (TMRS). The City provides a retirement benefit for employees through TMRS. The plan is administered in accordance with the Texas Municipal Retirement Act (Texas Government Code, Title 8, and Subtitle G) and is governed by a Board of Trustees appointed by the Governor. A brief outline of the plan is as follows: Participation in the program is mandatory. Municipal matching ratio is two to one. Service retirement eligibilities - 5 yrs/age 60, 20 yrs/any age. Vesting requirement is five years.
Deferred Compensation Plans. Deferred compensation plans allow both part-time and full-time employees to contribute to a retirement savings plan with pre-tax dollars through payroll deduction. Any money the employee contributes to the plan will be deducted from the employee’s salary before taxes are calculated, reducing the employee’s taxable income and the amount of taxes paid by the employee. Employees are encouraged to contact the Director of Human Resources for information on the deferred compensation plans currently available to employees.
City of Lancaster
Excellence: Working together to win trust, capitalize on our creative talents, acknowledging and sharing ideas, to create a high performing organization.
SUBJECT: Tuition Reimbursement POLICY NO.: T-5
APPROVED BY: Opal Mauldin Robertson
POLICY DATE: 03/15/2005
REVISED DATE: 01/01/2012
Purpose. In recognition of the long-range contribution that additional job-related education can make to the City of Lancaster, it is the policy of the City of Lancaster to provide educational assistance to its employees in accordance with the guidelines described in this policy. Eligibility. To be eligible for educational assistance, employees must have regular full-time status. Procedures. Eligible employees who want educational assistance must have approval of the City Manager or his/her designee before enrollment. Eligible employees may be reimbursed only for courses of study and book expenses which the City determines are directly related to the employee’s potential for advancement to a position within the City and to which the employee has a reasonable expectation of advancing. Required certification and continuing education courses shall be reimbursed through department budget as a training and education expenditure. Reimbursement will be paid only for courses offered by accredited institutions. Employee must fill out a request form, indicating the name of course, school, hours attending, reason for taking course (pursuing degree, etc.). The employee’s supervisor will review the request to insure that the class schedule will not conflict with his/her job schedule. The supervisor may grant an alternative work schedule that will not adversely impact City operations but is not required.
2
The City Manager, or his/her representative and supervisors, will consider the following factors in evaluating requests for educational assistance: The nature and purpose of the course of study; The benefits to be derived by the employee and the City; and The estimated cost.
Classes must not be scheduled during normal work hours, except as may be approved by the City Manager. Reimbursement Schedule. Employee reimbursement for eligible educational assistance will be based upon the grade received for the course, as follows: For a grade of “A” (90-100), 85% of tuition & books; For a grade of “B” (80-89), 70% of tuition & books;
For a grade of “C” (70-79), 60% of tuition & books;
No reimbursement will be made for a grade lower than “C” (69 or less) or if the
employee does not pass a pass-fail course. A “pass-fail” course will be reimbursed at 60% of tuition.
The maximum annual educational assistance per employee is $1,000.00. Certification. Employees seeking reimbursement for educational expenses must submit to the City Manager or his/her representative a certified transcript of their grades, and receipts for the expense incurred. Records of all education programs completed by each employee will be maintained by the Human Resources Department.
City of Lancaster
Dedication: Each person finishes their role in the process and completes the work with passion. Loyalty and commitment to the success of others through our professionalism and willingness to embrace new colleagues.
SUBJECT: Well Pay POLICY NO.: W-4
APPROVED BY: Opal Mauldin Robertson
POLICY DATE: 03/15/2005
REVISED DATE: 01/01/2012
Purpose. Well pay is an incentive plan to encourage employee’s to minimize the use of sick leave. Well pay shall be compensated in accordance with the following schedule:
General Government Police Officers on alternate work schedule of 9 or 12 hour shifts
Fire Personnel on 24-hour shift
ABSENCES (hours)
HOURS OF PAY ABSENCES
(hours) HOURS OF PAY
Ex. A Ex. B Ex. A Ex. B
ABSENCES (hours)
HOURS OF PAY
0-7 24 0-8 0-11 27 36 0-11 36 8-15 16 9-17 12-23 18 24 12-23 24 16-23 8 18-27 24-35 9 12 24-35 12
Implementation. Supervisors are responsible for approving time off requests from employees. Use of vacation time to avoid disciplinary action for unfavorable sick leave usage is not permitted. Vacation or comp time that is scheduled in advance and approved could be used for doctor’s appointments or other medical appointments. Leaves of absence due to illness (defined as more than five days off work) or unscheduled time for illness (i.e., calling in sick, leaving work early due to sickness) are to be taken as sick days. Once the sick time balance has been depleted then vacation leave or comp time may be taken.
2
It would be expected that an employee would no longer be eligible for well pay as they are using their sick leave before using their vacation leave or comp time. Once time off for illness has been requested an employee or supervisor may not change the request to vacation leave. At no time can sick leave be approved for use as vacation leave. Definition of well pay year: The well pay year starts October 1st of each year and ends September 30 of the following year. In order to be eligible for well pay, one must be hired prior to the beginning of the prior fiscal year. If at the end of the year a review of sick time taken for well pay payments reveals no sick time taken for someone known to have taken a medical leave of absence, then the well pay payment will be withheld according to the published schedule in the personnel policy manual. Employees who have donated sick time to other employees during the year will not have the donated sick time counted as hours taken for well pay payments. Employee whose sick leave use is taken in conjunction with an approved FMLA or worker’s compensation leave will not have the sick hours count as hours taken for well pay payments.
City of Lancaster Employee Benefits Notices and Forms Annual, New Hire, and Other Notices and Forms
Please note: While HUB is providing these notices as a courtesy to its clients, HUB does not provide legal or tax advice. HUB makes no representation or warranty as to the accuracy or completeness of these documents and is not obligated to update them. Consult your attorney and/or professional advisor as to your organization’s specific circumstances and legal, tax or other requirements.
A Note about COVID-19: The content of the HIPAA special enrollment notice and the COBRA Initial Notice in this packet may be affected by disaster relief guidance issued in response to the COVID-19 pandemic (see our article on hubinternational.com on these issues).
The notice templates provided by HUB do not reflect that relief for a couple of reasons. First, the relief may apply differently depending on how you and/or your vendors have chosen to apply the guidance. Second, we assume you have already communicated about the COVID-19 relief with your employees. However, as a best practice, HUB recommends you include information about the COVID-19 relief with your enrollment communications, even if you have communicated it previously.
Medicare Part D Creditable Coverage Notice
Important Notice from City of Lancaster About Your Prescription Drug Coverage and Medicare
Please read this notice carefully and keep it where you can find it. This notice has information about your current prescription drug coverage with City of Lancaster (the “Plan Sponsor”) and about your options under Medicare’s prescription drug coverage. This information can help you decide whether or not you want to join a Medicare drug plan. If you are considering joining, you should compare your current coverage, including which drugs are covered at what cost, with the coverage and costs of the plans offering Medicare prescription drug coverage in your area. Information about where you can get help to make decisions about your prescription drug coverage is at the end of this notice.
There are two important things you need to know about your current coverage and Medicare’s prescription drug coverage:
(1) Medicare prescription drug coverage became available in 2006to everyone with Medicare. You can get this coverage if youjoin a Medicare Prescription Drug Plan or join a MedicareAdvantage Plan (like an HMO or PPO) that offers prescriptiondrug coverage. All Medicare drug plans provide at least astandard level of coverage set by Medicare. Some plans mayalso offer more coverage for a higher monthly premium.
(2) The Plan Sponsor has determined that the prescription drugcoverage offered by the City of Lancaster’s Group Health Planis, on average for all plan participants, expected to pay out asmuch as standard Medicare prescription drug coverage paysand is therefore considered Creditable Coverage. Becauseyour existing coverage is Creditable Coverage, you can keep
this coverage and not pay a higher premium (a penalty) if you later decide to join a Medicare drug plan.
When Can You Join A Medicare Drug Plan? You can join a Medicare drug plan when you first become eligible for Medicare and each year from October 15th to December 7th.
However, if you lose your current creditable prescription drug coverage, through no fault of your own, you will also be eligible for a two (2) month Special Enrollment Period (SEP) to join a Medicare drug plan.
What Happens To Your Current Coverage If You Decide to Join A Medicare Drug Plan? If you decide to join a Medicare drug plan, your current Plan Sponsor coverage may be affected. Moreover, if you do decide to join a Medicare drug plan and drop your current Plan Sponsor coverage, be aware that you and your dependents may not be able to get this coverage back.
Please contact the person listed at the end of this notice for more information about what happens to your coverage if you enroll in a Medicare Part D prescription Drug Plan.
When Will You Pay A Higher Premium (Penalty) To Join A Medicare Drug Plan? You should also know that if you drop or lose your current coverage with the Plan Sponsor and don’t join a Medicare drug plan within 63 continuous days after your current coverage ends, you may pay a higher premium (a penalty) to join a Medicare drug plan later.
If you go 63 continuous days or longer without creditable prescription drug coverage, your monthly premium may go up by at least 1% of the Medicare base beneficiary premium per month for every month
that you did not have that coverage. For example, if you go nineteen months without creditable coverage, your premium may consistently be at least 19% higher than the Medicare base beneficiary premium. You may have to pay this higher premium (a penalty) as long as you have Medicare prescription drug coverage. In addition, you may have to wait until the following October to join.
For More Information about This Notice or Your Current Prescription Drug Coverage… Contact the person listed below for further information. NOTE: You’ll get this notice each year. You will also get it before the next period you can join a Medicare drug plan, and if this coverage through the Plan Sponsor changes. You also may request a copy of this notice at any time.
For More Information about Your Options under Medicare Prescription Drug Coverage… More detailed information about Medicare plans that offer prescription drug coverage is in the “Medicare & You” handbook. You’ll get a copy of the handbook in the mail every year from Medicare. You may also be contacted directly by Medicare drug plans.
For more information about Medicare prescription drug coverage: o Visit www.medicare.gov.o Call your State Health Insurance Assistance Program (see the
inside back cover of your copy of the “Medicare & You”handbook for their telephone number) for personalized helpCall 1-800-MEDICARE (1-800-633-4227). TTY users shouldcall 1-877-486-2048.
If you have limited income and resources, extra help paying for Medicare prescription drug coverage is available. For information about this extra help, visit Social Security on the web at www.socialsecurity.gov or call them at 1-800-772-1213 (TTY 1-800-325-0778).
Remember: Keep this Creditable Coverage notice. If you decide to join one of the Medicare drug plans, you may be required to provide a copy of this notice when you join to show whether or not you have maintained creditable coverage and, therefore, whether or not you are required to pay a higher premium (a penalty).
Date: 10/1/2021 Name of Entity/Sender: City of Lancaster Contact-Position/Office: HR Manager Address: 211 North Henry Street,
Lancaster, TX, 75146 Phone Number: 972-275-1794
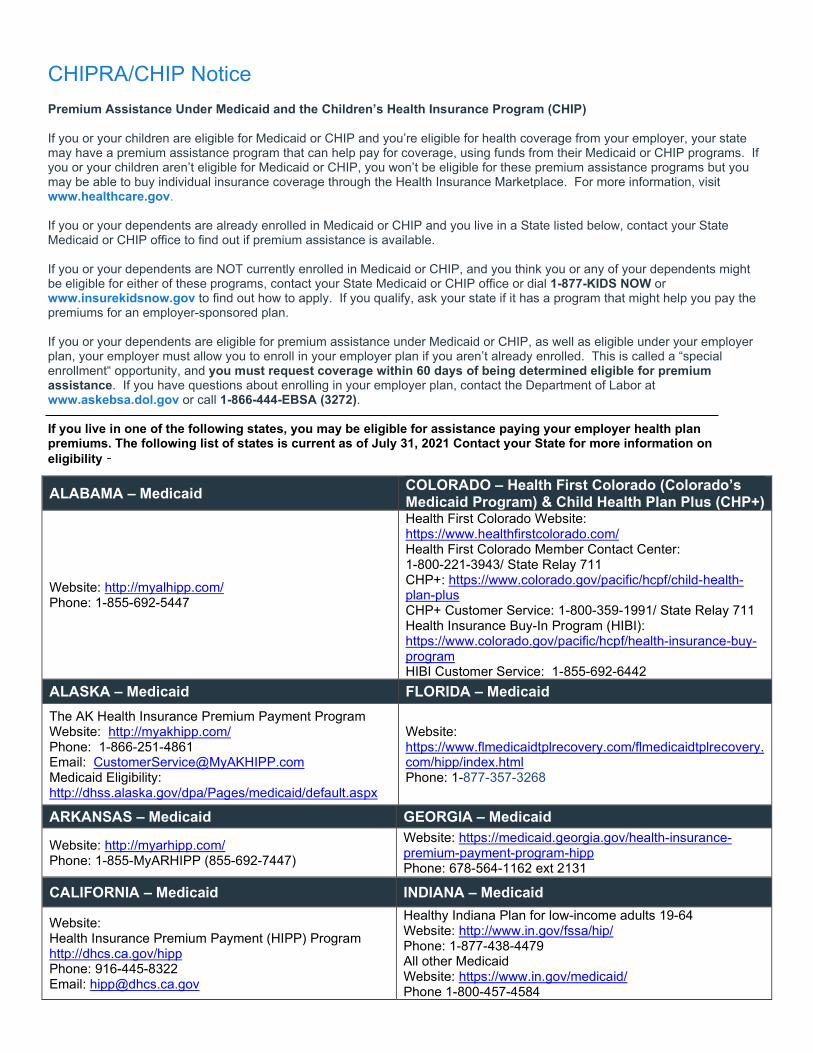
CHIPRA/CHIP Notice Premium Assistance Under Medicaid and the Children’s Health Insurance Program (CHIP)
If you or your children are eligible for Medicaid or CHIP and you’re eligible for health coverage from your employer, your state may have a premium assistance program that can help pay for coverage, using funds from their Medicaid or CHIP programs. If you or your children aren’t eligible for Medicaid or CHIP, you won’t be eligible for these premium assistance programs but you may be able to buy individual insurance coverage through the Health Insurance Marketplace. For more information, visit www.healthcare.gov.
If you or your dependents are already enrolled in Medicaid or CHIP and you live in a State listed below, contact your State Medicaid or CHIP office to find out if premium assistance is available. If you or your dependents are NOT currently enrolled in Medicaid or CHIP, and you think you or any of your dependents might be eligible for either of these programs, contact your State Medicaid or CHIP office or dial 1-877-KIDS NOW or www.insurekidsnow.gov to find out how to apply. If you qualify, ask your state if it has a program that might help you pay the premiums for an employer-sponsored plan. If you or your dependents are eligible for premium assistance under Medicaid or CHIP, as well as eligible under your employer plan, your employer must allow you to enroll in your employer plan if you aren’t already enrolled. This is called a “special enrollment“ opportunity, and you must request coverage within 60 days of being determined eligible for premium assistance. If you have questions about enrolling in your employer plan, contact the Department of Labor at www.askebsa.dol.gov or call 1-866-444-EBSA (3272). If you live in one of the following states, you may be eligible for assistance paying your employer health plan premiums. The following list of states is current as of July 31, 2021 Contact your State for more information on eligibility –
ALABAMA – Medicaid COLORADO – Health First Colorado (Colorado’s Medicaid Program) & Child Health Plan Plus (CHP+)
Website: http://myalhipp.com/ Phone: 1-855-692-5447
Health First Colorado Website: https://www.healthfirstcolorado.com/ Health First Colorado Member Contact Center: 1-800-221-3943/ State Relay 711 CHP+: https://www.colorado.gov/pacific/hcpf/child-health-plan-plus CHP+ Customer Service: 1-800-359-1991/ State Relay 711 Health Insurance Buy-In Program (HIBI): https://www.colorado.gov/pacific/hcpf/health-insurance-buy-program HIBI Customer Service: 1-855-692-6442
ALASKA – Medicaid FLORIDA – Medicaid The AK Health Insurance Premium Payment Program Website: http://myakhipp.com/ Phone: 1-866-251-4861 Email: [email protected] Medicaid Eligibility: http://dhss.alaska.gov/dpa/Pages/medicaid/default.aspx
Website: https://www.flmedicaidtplrecovery.com/flmedicaidtplrecovery.com/hipp/index.html Phone: 1-877-357-3268
ARKANSAS – Medicaid GEORGIA – Medicaid
Website: http://myarhipp.com/ Phone: 1-855-MyARHIPP (855-692-7447)
Website: https://medicaid.georgia.gov/health-insurance-premium-payment-program-hipp Phone: 678-564-1162 ext 2131
CALIFORNIA – Medicaid INDIANA – Medicaid
Website: Health Insurance Premium Payment (HIPP) Program http://dhcs.ca.gov/hipp Phone: 916-445-8322 Email: [email protected]
Healthy Indiana Plan for low-income adults 19-64 Website: http://www.in.gov/fssa/hip/ Phone: 1-877-438-4479 All other Medicaid Website: https://www.in.gov/medicaid/ Phone 1-800-457-4584
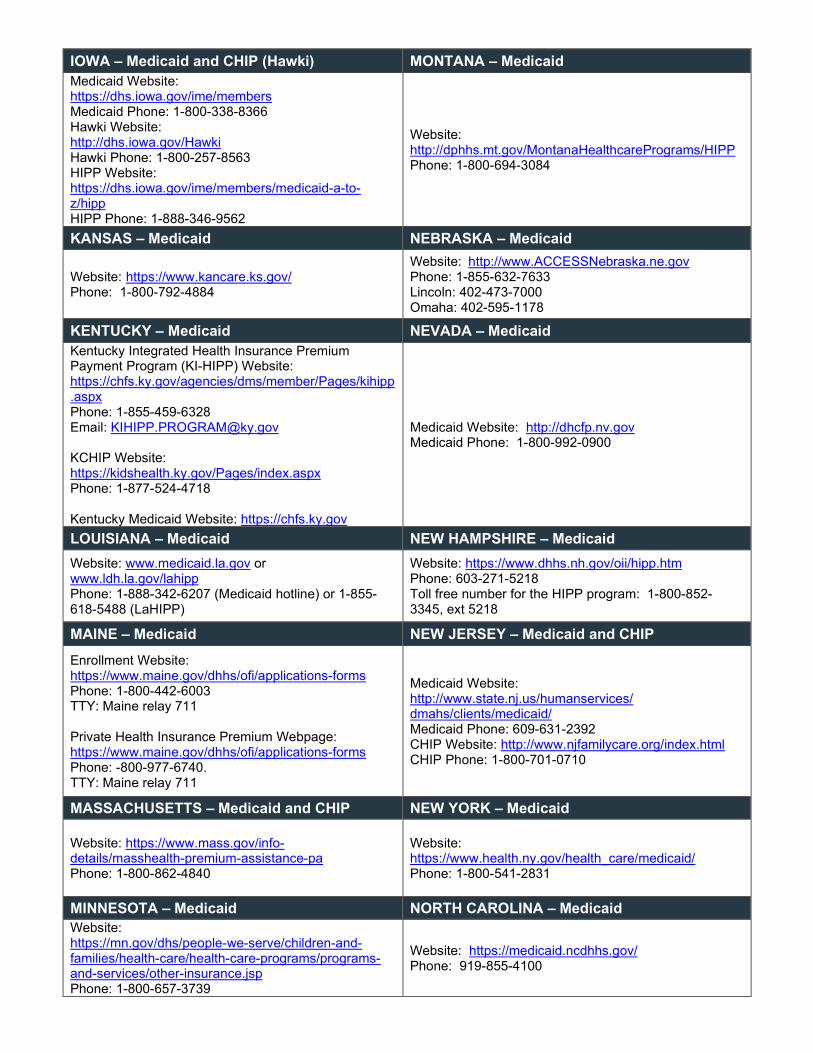
IOWA – Medicaid and CHIP (Hawki) MONTANA – Medicaid Medicaid Website: https://dhs.iowa.gov/ime/members Medicaid Phone: 1-800-338-8366 Hawki Website: http://dhs.iowa.gov/Hawki Hawki Phone: 1-800-257-8563 HIPP Website: https://dhs.iowa.gov/ime/members/medicaid-a-to-z/hipp HIPP Phone: 1-888-346-9562
Website: http://dphhs.mt.gov/MontanaHealthcarePrograms/HIPP Phone: 1-800-694-3084
KANSAS – Medicaid NEBRASKA – Medicaid
Website: https://www.kancare.ks.gov/ Phone: 1-800-792-4884
Website: http://www.ACCESSNebraska.ne.gov Phone: 1-855-632-7633 Lincoln: 402-473-7000 Omaha: 402-595-1178
KENTUCKY – Medicaid NEVADA – Medicaid Kentucky Integrated Health Insurance Premium Payment Program (KI-HIPP) Website: https://chfs.ky.gov/agencies/dms/member/Pages/kihipp.aspx Phone: 1-855-459-6328 Email: [email protected]
KCHIP Website: https://kidshealth.ky.gov/Pages/index.aspx Phone: 1-877-524-4718
Kentucky Medicaid Website: https://chfs.ky.gov
Medicaid Website: http://dhcfp.nv.gov Medicaid Phone: 1-800-992-0900
LOUISIANA – Medicaid NEW HAMPSHIRE – Medicaid Website: www.medicaid.la.gov or www.ldh.la.gov/lahipp Phone: 1-888-342-6207 (Medicaid hotline) or 1-855-618-5488 (LaHIPP)
Website: https://www.dhhs.nh.gov/oii/hipp.htm Phone: 603-271-5218 Toll free number for the HIPP program: 1-800-852-3345, ext 5218
MAINE – Medicaid NEW JERSEY – Medicaid and CHIP Enrollment Website: https://www.maine.gov/dhhs/ofi/applications-forms Phone: 1-800-442-6003 TTY: Maine relay 711
Private Health Insurance Premium Webpage: https://www.maine.gov/dhhs/ofi/applications-forms Phone: -800-977-6740. TTY: Maine relay 711
Medicaid Website: http://www.state.nj.us/humanservices/ dmahs/clients/medicaid/ Medicaid Phone: 609-631-2392 CHIP Website: http://www.njfamilycare.org/index.html CHIP Phone: 1-800-701-0710
MASSACHUSETTS – Medicaid and CHIP NEW YORK – Medicaid
Website: https://www.mass.gov/info-details/masshealth-premium-assistance-pa Phone: 1-800-862-4840
Website: https://www.health.ny.gov/health_care/medicaid/ Phone: 1-800-541-2831
MINNESOTA – Medicaid NORTH CAROLINA – Medicaid Website: https://mn.gov/dhs/people-we-serve/children-and-families/health-care/health-care-programs/programs-and-services/other-insurance.jsp Phone: 1-800-657-3739
Website: https://medicaid.ncdhhs.gov/ Phone: 919-855-4100
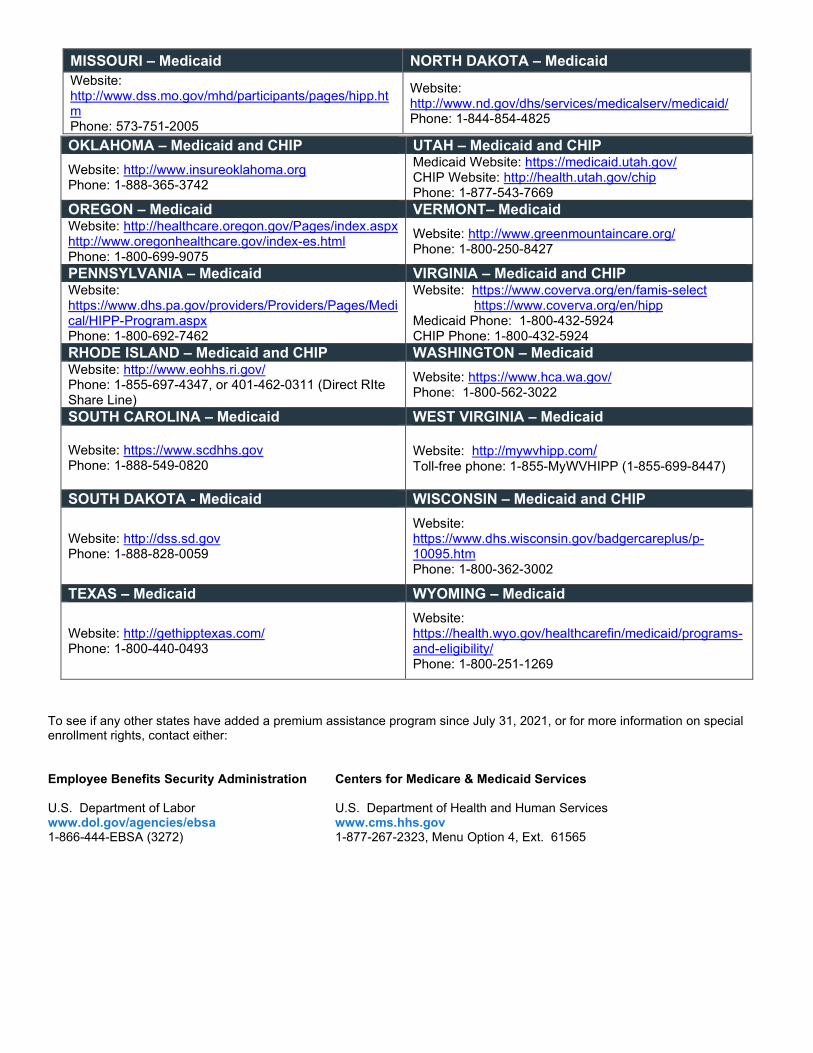
MISSOURI – Medicaid NORTH DAKOTA – Medicaid Website: http://www.dss.mo.gov/mhd/participants/pages/hipp.htm Phone: 573-751-2005
Website: http://www.nd.gov/dhs/services/medicalserv/medicaid/ Phone: 1-844-854-4825
To see if any other states have added a premium assistance program since July 31, 2021, or for more information on special enrollment rights, contact either:
Employee Benefits Security Administration Centers for Medicare & Medicaid Services
U.S. Department of Labor U.S. Department of Health and Human Services www.dol.gov/agencies/ebsa www.cms.hhs.gov 1-866-444-EBSA (3272) 1-877-267-2323, Menu Option 4, Ext. 61565
OKLAHOMA – Medicaid and CHIP UTAH – Medicaid and CHIP Website: http://www.insureoklahoma.org Phone: 1-888-365-3742
Medicaid Website: https://medicaid.utah.gov/ CHIP Website: http://health.utah.gov/chip Phone: 1-877-543-7669
OREGON – Medicaid VERMONT– Medicaid Website: http://healthcare.oregon.gov/Pages/index.aspx http://www.oregonhealthcare.gov/index-es.html Phone: 1-800-699-9075
Website: http://www.greenmountaincare.org/ Phone: 1-800-250-8427
PENNSYLVANIA – Medicaid VIRGINIA – Medicaid and CHIP Website: https://www.dhs.pa.gov/providers/Providers/Pages/Medical/HIPP-Program.aspx Phone: 1-800-692-7462
Website: https://www.coverva.org/en/famis-select https://www.coverva.org/en/hipp
Medicaid Phone: 1-800-432-5924 CHIP Phone: 1-800-432-5924
RHODE ISLAND – Medicaid and CHIP WASHINGTON – Medicaid Website: http://www.eohhs.ri.gov/ Phone: 1-855-697-4347, or 401-462-0311 (Direct RIte Share Line)
Website: https://www.hca.wa.gov/ Phone: 1-800-562-3022
SOUTH CAROLINA – Medicaid WEST VIRGINIA – Medicaid
Website: https://www.scdhhs.gov Phone: 1-888-549-0820
Website: http://mywvhipp.com/ Toll-free phone: 1-855-MyWVHIPP (1-855-699-8447)
SOUTH DAKOTA - Medicaid WISCONSIN – Medicaid and CHIP
Website: http://dss.sd.gov Phone: 1-888-828-0059
Website: https://www.dhs.wisconsin.gov/badgercareplus/p-10095.htm Phone: 1-800-362-3002
TEXAS – Medicaid WYOMING – Medicaid
Website: http://gethipptexas.com/ Phone: 1-800-440-0493
Website: https://health.wyo.gov/healthcarefin/medicaid/programs-and-eligibility/ Phone: 1-800-251-1269
Annual Notice of Women’s Health and Cancer Rights Act
Do you know that your plan, as required by the Women’s Health and Cancer Right Act of 1998, provides benefits for mastectomy-related services, including all stages of reconstruction and surgery to achieve symmetry between the breasts, prostheses and treatment for complications resulting from a mastectomy, including lymphedema? Call your plan administrator at 972-275-1794 for more information.
Notice of Availability of HIPAA Notice of Privacy Practices
City of Lancaster 211 North Henry Street, Lancaster, TX, 75146 10/1/2021
To: Participants in the Major Medical, HSA/FSA, Dental, Vision, Basic & Term Life, Short-Term and Long-Term Disability
From: Michelle Evans, HR Manager
Re: Availability of Notice of Privacy Practices
The Major Medical, HSA/FSA, Dental, Vision, Basic & Term Life, Short-Term and Long-Term Disability (each a “Plan”) maintains a Notice of Privacy Practices that provides information to individuals whose protected health information (PHI) will be used or maintained by the Plan. If you would like a copy of the Plan's Notice of Privacy Practices, please contact Michelle Evans, HR Manager at [email protected].
Patient Protection Disclosures City of Lancaster’s Group Health Plan generally requires the designation of a primary care provider. You have the right to designate any primary care provider who participates in our network and who is available to accept you or your family members. Until you make this designation, City of Lancaster’s Group Health Plan designates one for you. For information on how to select a primary care provider, and for a list of the participating primary care providers, contact the Michelle Evans, HR Manager at 211 North Henry Street, Lancaster, TX, 75146, 972-275-1794, [email protected].
For children, you may designate a pediatrician as the primary care provider.
You do not need prior authorization from City of Lancaster’s Group Health Plan or from any other person (including a primary care provider) in order to obtain access to obstetrical or gynecological care from a health care professional in our network who specializes in obstetrics or gynecology. The health care professional, however, may be required to comply with certain procedures, including obtaining prior authorization for certain services, following a pre-approved treatment plan, or procedures for making referrals. For a list of participating health care professionals who specialize in obstetrics or gynecology, contact the Michelle Evans, HR Manager at 211 North Henry Street, Lancaster, TX, 75146, 972-275-1794, [email protected].
Wellness Program Disclosure
HIPAA Wellness Notice
Your health plan is committed to helping you achieve your best health. Rewards for participating in a wellness program are available to all participants. If you think you might be unable to meet a standard for a reward under this wellness program, you might qualify for an opportunity to earn the same reward by different means. Contact Michelle Evans, HR Manager, at 211 North Henry Street, Lancaster, TX, 75146, 972-275-1794, [email protected] and we will work with you (and, if you wish, with your doctor) tofind a wellness program with the same reward that is right for you in light of your health status, if you areeligible for an alternate standard.
EEOC Wellness Notice
Baylor Scott and White Health Wellness Program is a voluntary wellness program available to all employees. The program is administered according to federal rules permitting employer-sponsored wellness programs that seek to improve employee health or prevent disease, including the Americans with Disabilities Act of 1990, the Genetic Information Nondiscrimination Act of 2008, and the Health Insurance Portability and Accountability Act, as applicable, among others. If you choose to participate in the wellness program you will be asked to complete a voluntary health risk assessment or “HRA” that asks a series of questions about your health-related activities and behaviors and whether you have or had certain medical conditions (e.g., cancer, diabetes, or heart disease). You are not required to complete the HRA.
If you choose to participate in the wellness program, you will be asked to complete a biometric screening, which will include a blood test for diabetes, high cholesterol, blood clotting, immune strength, HIV/AIDS, organ productivity. You are not required to participate in the blood test or other medical examinations.
However, employees who choose to participate in the wellness program will avoid an Incomplete Physical and Tobacco Use Surcharge for complete health risk assessment by December 31st. Although you are not required to participate, only employees who do so will avoid the surcharge.
Your results will be used to provide you with information to help you understand your current health and potential risks, and may also be used to offer you services through the wellness program, such as diabetes education/prevention, disease management, nutrition counseling. You also are encouraged to share your results or concerns with your own doctor.
Protections from Disclosure of Medical Information
We are required by law to maintain the privacy and security of your personally identifiable health information. Although the wellness program and City of Lancaster may use aggregate information it collects to design a program based on identified health risks in the workplace, Baylor Scott and White Health Wellness Program will never disclose any of your personal information either publicly or to the employer, except as necessary to respond to a request from you for a reasonable accommodation needed to participate in the wellness program, or as expressly permitted by law. Medical information that personally identifies you that is provided in connection with the wellness program will not be provided to your supervisors or managers and may never be used to make decisions regarding your employment.
Your health information will not be sold, exchanged, transferred, or otherwise disclosed except to the extent permitted by law to carry out specific activities related to the wellness program, and you will not be asked or required to waive the confidentiality of your health information as a condition of participating in the wellness program or receiving an incentive. Anyone who receives your information for purposes of providing you services as part of the wellness program will abide by the same confidentiality requirements. The only individual(s) who will receive your personally identifiable health information is (are) registered nurses and health coaches in order to provide you with services under the wellness program.
In addition, all medical information obtained through the wellness program will be maintained separate from your personnel records, information stored electronically will be encrypted, and no information you provide as part of the wellness program will be used in making any employment decision. Surveys will be anonymous. Participants names and other PHI will not be disclosed to the City of Lancaster. Appropriate precautions will be taken to avoid any data breach, and in the event a data breach occurs involving information you provide in connection with the wellness program, we will notify you immediately.
You may not be discriminated against in employment because of the medical information you provide as part of participating in the wellness program, nor may you be subjected to retaliation if you choose not to participate.
If you have questions or concerns regarding this notice, or about protections against discrimination and retaliation, please contact Michelle Evans, HR Manager at 211 North Henry Street, Lancaster, TX, 75146, 972-275-1794, [email protected].
Notice of Marketplace Coverage Options
PART A: General Information When key parts of the health care law take effect in 2014, there will be a new way to buy health insurance: the Health Insurance Marketplace. To assist you as you evaluate options for you and your family, this notice provides some basic information about the new Marketplace and employment-based health coverage offered by your employer.
What is the Health Insurance Marketplace? The Marketplace is designed to help you find health insurance that meets your needs and fits your budget. The Marketplace offers "one-stop shopping" to find and compare private health insurance options. You may also be eligible for a new kind of tax credit that lowers your monthly premium right away. Open enrollment for health insurance coverage through the Marketplace begins November 1, 2021 for coverage starting January 1, 2022.
Can I Save Money on my Health Insurance Premiums in the Marketplace? You may qualify to save money and lower your monthly premium, but only if your employer does not offer coverage, or offers coverage that doesn't meet certain standards. The savings on your premium that you're eligible for depends on your household income.
Does Employer Health Coverage Affect Eligibility for Premium Savings through the Marketplace? Yes. If you have an offer of health coverage from your employer that meets certain standards, you will not be eligible for a tax credit through the Marketplace and may wish to enroll in your employer's health plan. However, you may be eligible for a tax credit that lowers your monthly premium, or a reduction in certain cost-sharing if your employer does not offer coverage to you at all or does not offer coverage that meets certain standards. If the cost of a plan from your employer that would cover you (and not any other members of your family) is more than 9.5% (as adjusted annually) of your household income for the year, or if the coverage your employer provides does not meet the "minimum value" standard set by the Affordable Care Act, you may be eligible for a tax credit.1
Note: If you purchase a health plan through the Marketplace instead of accepting health coverage offered by your employer, then you may lose the employer contribution (if any) to the employer-offered coverage. Also, this employer contribution -as well as your employee contribution to employer-offered coverage- is often excluded from income for Federal and State income tax purposes. Your payments for coverage through the Marketplace are made on an after-tax basis.
How Can I Get More Information? For more information about your coverage offered by your employer, please check your summary plan description or contact. Michelle Evans, HR Manager at 211 North Henry Street, Lancaster, TX, 75146, 972-275-1794, [email protected].
The Marketplace can help you evaluate your coverage options, including your eligibility for coverage through the Marketplace and its cost. Please visit HealthCare.gov for more information, including an online application for health insurance coverage and contact information for a Health Insurance Marketplace in your area.
1 An employer-sponsored health plan meets the “minimum value standard” if the plan’s share of the total allowed benefit costs
covered by the plan is no less than 60 percent of such costs.
New Health Insurance Marketplace Coverage Options and Your Health Coverage
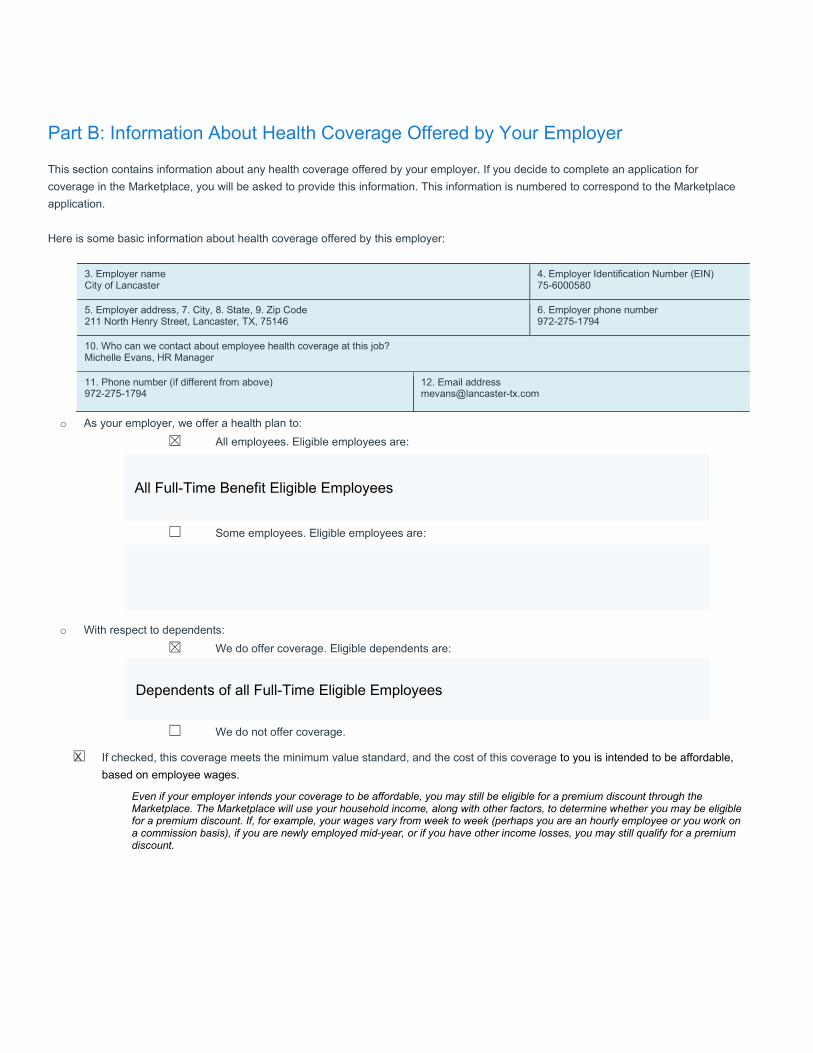
Part B: Information About Health Coverage Offered by Your Employer
This section contains information about any health coverage offered by your employer. If you decide to complete an application for coverage in the Marketplace, you will be asked to provide this information. This information is numbered to correspond to the Marketplace application.
Here is some basic information about health coverage offered by this employer:
o As your employer, we offer a health plan to:☒ All employees. Eligible employees are:
☐ Some employees. Eligible employees are:
o With respect to dependents:☒ We do offer coverage. Eligible dependents are:
☐ We do not offer coverage.
☐ If checked, this coverage meets the minimum value standard, and the cost of this coverage to you is intended to be affordable,based on employee wages.
Even if your employer intends your coverage to be affordable, you may still be eligible for a premium discount through the Marketplace. The Marketplace will use your household income, along with other factors, to determine whether you may be eligible for a premium discount. If, for example, your wages vary from week to week (perhaps you are an hourly employee or you work on a commission basis), if you are newly employed mid-year, or if you have other income losses, you may still qualify for a premium discount.
3. Employer name City of Lancaster
4. Employer Identification Number (EIN) 75-6000580
5. Employer address, 7. City, 8. State, 9. Zip Code 211 North Henry Street, Lancaster, TX, 75146
6. Employer phone number 972-275-1794
10. Who can we contact about employee health coverage at this job? Michelle Evans, HR Manager
11. Phone number (if different from above) 972-275-1794
12. Email [email protected]
All Full-Time Benefit Eligible Employees
Dependents of all Full-Time Eligible Employees
X
Notice of Special Enrollment Rights
If you are declining enrollment for yourself or your dependents (including your spouse) because of other health insurance or group health plan coverage, you may be able to enroll yourself and your dependents in this plan if you or your dependents lose eligibility for that other coverage (or if the employer stops contributing toward your or your dependents’ other coverage). However, you must request enrollment no later than 30 days after your or your dependents’ other coverage ends (or after the employer stops contributing toward the other coverage).
In addition, if you have a new dependent as a result of marriage, birth, adoption, or placement for adoption, you may be able to enroll yourself and your dependents. However, you must request enrollment no later than 30 days after the marriage, birth, adoption, or placement for adoption.
Effective April 1, 2009, if either of the following two events occur, you will have 60 Days after the date of the event to request enrollment in your employer’s plan:
o Your dependents lose Medicaid or CHIP coverage because they are no longer eligible.o Your dependents become eligible for a state’s premium assistance program.
To take advantage of special enrollment rights, you must experience a qualifying event and provide the employer plan with timely notice of the event and your enrollment request. .
To request special enrollment or obtain more information, contact City of Lancaster, Human Resource Dept. at 972-275-1794.





























